EATING DISORDERS. models-meet-criteria-for-anorexia-size-6-is-plus-size- magazine 1)On a scale of.
25
EATING DISORDERS
-
Upload
donald-washington -
Category
Documents
-
view
214 -
download
0
Transcript of EATING DISORDERS. models-meet-criteria-for-anorexia-size-6-is-plus-size- magazine 1)On a scale of.

EATING DISORDERS
http://abcnews.go.com/blogs/headlines/2012/01/most-models-meet-criteria-for-anorexia-size-6-is-plus-size-magazine1)On a scale of 1 to 10 – how much pressure are University of Dayton women under to conform to an ideal body type?
2) On a scale of 1 to 10 – how much pressure are University of Dayton men under to conform to an ideal body type?
3) What are the sources of these messages?
4) Do you think that eating disorders are a significant problem at University of Dayton?
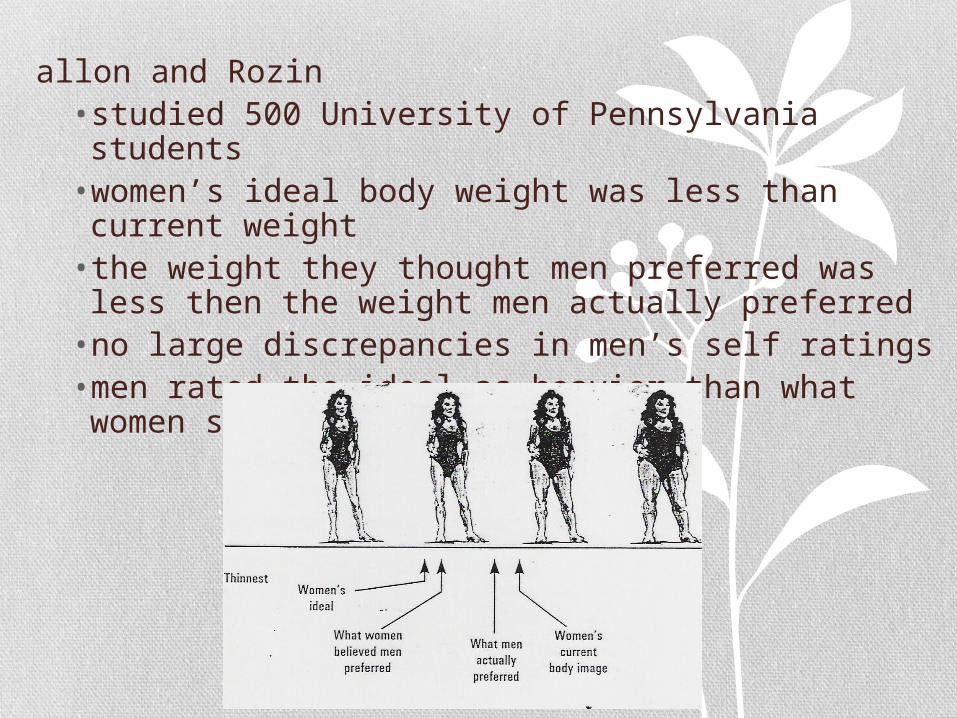
•Fallon and Rozin • studied 500 University of Pennsylvania students•women’s ideal body weight was less than current weight • the weight they thought men preferred was less then the weight men actually preferred• no large discrepancies in men’s self ratings•men rated the ideal as heavier than what women said was most attractive
Anorexia Nervosa
A) Refusal to maintain body weight at a normal weight for age and height (less than 85% of expected)
B) Intense fear of gaining weight or becoming fat even though underweight
C) Disturbance in body image
AnorexiaPossible Medical Complications
•amenorrhea
•sensitivity to cold temperatures
•lanugo – downy hair on the lips and cheeks
•bradycardia
•arrhythmia
•hypotension
•osteoporosis
•hair loss

Biological Factors
•relatives of patients with eating disorders are 4-5 times more likely to have eating disorders
•Ventromedial hypothalamus – lesion – overeat (hyperphagia)
•Lateral hypothalamus – lesion – don’t eat at all (aphagia)
•Non-specific risk factors
•Cultural imperative for thinness
• Ideal body size standards
• Ethnicity
•Data from experimental and cross-cultural research
•Family influences
Social Factors
•Low sense of personal control•Low self-confidence•Perfectionistic attitudes•Distorted body image•Preoccupation with food and appearance•Negative mood intolerance
Psychological Dimensions
Treatment of Anorexia
1) First goal is to gain weight so at least in low normal range
2) If 70% below average – inpatient treatment may be needed
3) Treat underlying thought patterns about eating
4) Family therapy may be effective
Bulimia Nervosa A) Recurrent episode of binge eating.
B) Inappropriate behaviors to prevent weight gain
C) Binge and compensatory behavior
D) Overly concerned about body image
•Anxiety
•Mood disorders
•Substance abuse
Bulimia Nervosa:Associated Psychological Disorders
BulimiaPossible Medical Consequences
•salivary gland enlargement•erosion of dental enamel•electolyte imbalance (e.g., sodium and potassium)•cardiac arrhythmia•kidney failure• intestinal problems
Treatment of Bulimia1) teach the patient the physical consequences
of binge eating and purging and the ineffectiveness of purging for weight loss
2) eat small amounts of food 5-6 times a day with no more than 3 hour intervals between planned meals and snacks
3) cognitive therapy focused on altering thoughts about eating
4) exposure with response prevention.

Binge-Eating Disorder
A.Recurrent episodes of binge eating
B. Binge episodes associated with at least 3 of following:
1) rapid eating2) eat until uncomfortably full3) eat large amounts when not hungry4) eating alone – embarrassed by how much eat5) feeling disgusted with oneself
C. Distress regarding binges
D. Absence of compensatory behaviors

SLEEP DISORDERS

Stages of Sleep
1) brain waves become smaller - drifting to edge of consciousness. (theta waves)
2) sleep spindles: short bursts of rapid, high – peaking waves. (theta waves)
3) delta waves: slow, regular brain waves characteristic of stage 3 and stage 4 sleep.
4) delta waves have almost completely taken over - deep sleep.
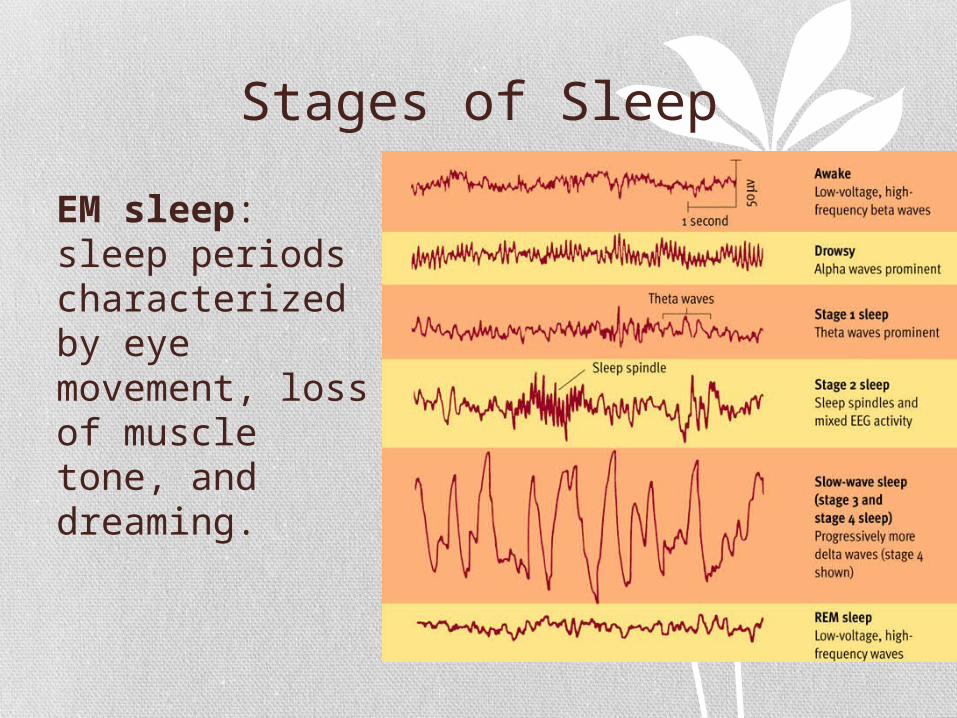
Stages of Sleep•R
EM sleep: sleep periods characterized by eye movement, loss of muscle tone, and dreaming.
Sleep Disorders•P
arasomnias• Abnormal behaviors such as nightmares or sleepwalking that occur during sleep
•Dyssomnias• Problems in getting to sleep or in obtaining sufficient quality sleep
Parasomnias
•Sleepwalking Disorder• occurs during stage IV sleep• nocturnal eating syndrome• people eat while asleep
• http://www.standoutessay.com/blog/2011/08/22/adorable-kid-tries-to-finish-his-ice-cream-while-falling-asleep/

Parasomnias
•Sleep Terror Disorder• Recurrent episodes of abrupt awakening•Usually during first third of sleep•Often beings with a scream
Dyssomnia
•Primary Insomnia•Difficulty initiating / maintaining sleep or nonrestorative sleep• Lasts at least one month•Not related to other medical or psychological problems

Fatal Familial Insomnia
•Extremely rare (about 50 families worldwide)
•Insomnia is fatal (death 7 to 36 months from onset)
•gene mutation leads to plaque in thalamus

Treatment of Insomnia•s
timulus control• only use bed for sleep and sex
•progressive relaxation
•improve sleep hygiene• regularity, temperature, noise, stimulants, cover clock
•sleep restriction
•paradoxical intention

Dyssomnias•N
arcolepsy• sudden and irreversible sleep attacks (treated with stimulant medication)• cataplexy (treated with SSRI)
•Sleep apnea• brief periods when breathing ceases (treated with CPAP machine and/or meds)

Dyssomnias
•Circadian rhythm sleep disorder• brain cannot synchronize sleep with day/night• suprachiasmatic nucleus (in hypothalamus)
•Primary hypersomnia• excessive daytime sleepiness not caused by insomnia or sleep apnea