Earthquake forcasting

of 29
-
Upload
mohit-bajaj -
Category
Documents
-
view
221 -
download
0
Transcript of Earthquake forcasting
-
8/12/2019 Earthquake forcasting
1/29
Group-7
Development of Hospital Operations for
Regional Disaster Relief
1.IntroductionThe project deals with the development and actual planning and management of them at
the time of disaster, which also extends from planning of routing of patients from the
disaster location to the nearest medical facility to after disaster relief.
1.1ScopeThe scope of the project includes the development of the meta-model which will be useful
for efficient working of hospital in the regional disaster conditions.
This includes on-site examination of patients and triaging of the patients and routing them
to the appropriate medical facility by taking the severity,prehospital transport time,facility
available and capacity of the hospital and various other factors like traffic,weather,etc.
Also,this includes the surveying of various medical facilities(government or private) in the
disaster-prone region ,their capacity and type of facilities and infrastructural development
of these facilities by funding government facilities or subsidising private facilities and other
training programmes.This will also include after disaster medical attention and Counselling to provide moral
support to patients.
1.2Purpose
When a disaster occurs, the number ofpatients who require treatment in EDs may increase
35 times the normal which easily could overwhelm the hospitals resources.
Thus,the main purpose of the system is to essentially reduce the mortality due to inefficient
hospital management and incapability of the services available at such medical facilities at
the time of disaster.Also to decrease the discomfort ,pain ,trouble in the process of disaster relief work by
implementing an efficient algorithmic model for routing of patients.
-
8/12/2019 Earthquake forcasting
2/29
1.3System Overview
The overall view about whole system can be given as :
1.To estimate capacity of the hospial for various patient-mix and severities casulities &
development according to it.2.Classification of victims according to the severity of injuries/illnesses, and assigning
priorities based on survivability time so that every victim gets optimum resources and
treatment.
3.Routing of the patients depending upon the difference between the the survibility time
and waiting time ,i.e,on the basis of maximum allowable waiting time.
4.After relief work and movement of patients and other related work(such as informing the
patients relative).
5.study of the patients waiting time on their survibility and thus suggesting changes in the
present routing algorithm.the further detailed overviews about each subsystem are given in the each subsystems
description.
2.References:
1.http://www.urban.org/UploadedPDF/411348_katrinahospitals.pdf
Bradford H Gray and Katy Hebert.
2.Transient Modeling in Simulation of Hospital Operations for Emergency Response -
Jomon Aliyas Paul, PhD Santhosh K. George, MS Pengfei Yi, PhD Li Lin, PhD.
http://www.mendeley.com/catalog/transient-modeling-simulation-hospital-o
perations-emergency-response/
3.www.gliffy.com/
Gliffy: Online Diagram Software and Flowchart Software
4.http://1.bp.blogspot.com/-oPlDxwyqoLM/Tya9ZjH1vlI/AAAAAAAAAN4/PDnwYfVx5Fg/s1600/Hos
pitalManagementSystem-usecaseDiagram.bmp
5.https://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&ved=0CDkQFjAB&u
rl=http%3A%2F%2Fapicssoutheast.org%2FChattanooga%2FHealthCareManagement.pps&ei=lI
0wUffqHZHKrAfM04CIBw&usg=AFQjCNFFmdXPIcKV8nBlj-UHsi7vi7bnYw&sig2=Syc4EaQtV9Z
WuU1gjAIuIw&bvm=bv.43148975,d.bmk
https://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&ved=0CDkQFjAB&url=http%3A%2F%2Fapicssoutheast.org%2FChattanooga%2FHealthCareManagement.pps&ei=lI0wUffqHZHKrAfM04CIBw&usg=AFQjCNFFmdXPIcKV8nBlj-UHsi7vi7bnYw&sig2=Syc4EaQtV9ZWuU1gjAIuIw&bvm=bv.43148975,d.bmkhttps://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&ved=0CDkQFjAB&url=http%3A%2F%2Fapicssoutheast.org%2FChattanooga%2FHealthCareManagement.pps&ei=lI0wUffqHZHKrAfM04CIBw&usg=AFQjCNFFmdXPIcKV8nBlj-UHsi7vi7bnYw&sig2=Syc4EaQtV9ZWuU1gjAIuIw&bvm=bv.43148975,d.bmkhttps://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&ved=0CDkQFjAB&url=http%3A%2F%2Fapicssoutheast.org%2FChattanooga%2FHealthCareManagement.pps&ei=lI0wUffqHZHKrAfM04CIBw&usg=AFQjCNFFmdXPIcKV8nBlj-UHsi7vi7bnYw&sig2=Syc4EaQtV9ZWuU1gjAIuIw&bvm=bv.43148975,d.bmkhttps://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&ved=0CDkQFjAB&url=http%3A%2F%2Fapicssoutheast.org%2FChattanooga%2FHealthCareManagement.pps&ei=lI0wUffqHZHKrAfM04CIBw&usg=AFQjCNFFmdXPIcKV8nBlj-UHsi7vi7bnYw&sig2=Syc4EaQtV9ZWuU1gjAIuIw&bvm=bv.43148975,d.bmkhttp://www.google.com/url?q=http%3A%2F%2F1.bp.blogspot.com%2F-oPlDxwyqoLM%2FTya9ZjH1vlI%2FAAAAAAAAAN4%2FPDnwYfVx5Fg%2Fs1600%2FHospitalManagementSystem-usecaseDiagram.bmp&sa=D&sntz=1&usg=AFQjCNHE_CR945Z5_jv2K485P8mY9fQtmghttp://www.google.com/url?q=http%3A%2F%2F1.bp.blogspot.com%2F-oPlDxwyqoLM%2FTya9ZjH1vlI%2FAAAAAAAAAN4%2FPDnwYfVx5Fg%2Fs1600%2FHospitalManagementSystem-usecaseDiagram.bmp&sa=D&sntz=1&usg=AFQjCNHE_CR945Z5_jv2K485P8mY9fQtmghttp://www.google.com/url?q=http%3A%2F%2Fwww.gliffy.com%2F&sa=D&sntz=1&usg=AFQjCNGLddiMcA4BwEKOU0yUg_73WuXNWwhttp://www.google.com/url?q=http%3A%2F%2Fwww.gliffy.com%2F&sa=D&sntz=1&usg=AFQjCNGLddiMcA4BwEKOU0yUg_73WuXNWwhttp://www.google.com/url?q=http%3A%2F%2Fwww.mendeley.com%2Fcatalog%2Ftransient-modeling-simulation-hospital-operations-emergency-response%2F&sa=D&sntz=1&usg=AFQjCNEaghP3yk-Yn_dWEK-iFSTtGuWxkQhttp://www.google.com/url?q=http%3A%2F%2Fwww.mendeley.com%2Fcatalog%2Ftransient-modeling-simulation-hospital-operations-emergency-response%2F&sa=D&sntz=1&usg=AFQjCNEaghP3yk-Yn_dWEK-iFSTtGuWxkQhttp://www.google.com/url?q=http%3A%2F%2Fwww.urban.org%2FUploadedPDF%2F411348_katrinahospitals.pdf&sa=D&sntz=1&usg=AFQjCNGx7JNwWkvUU8caOl2Xgj5Rw_1SxQ -
8/12/2019 Earthquake forcasting
3/29
6.https://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&cad=rja&sqi=2&ved
=0CE0QFjAB&url=http%3A%2F%2Fwww.ahrq.gov%2Fqual%2Fhroadvice%2Fhroadvice.pdf&ei
=6o0wUbPQMMWGrAes1IHwAg&usg=AFQjCNHntGHPpfIadUni2MdGj292iRYIOw&sig2=WfqZ_
HIyXnixXztZaaOMmQ&bvm=bv.43148975,d.bmk
3.0 REQUIREMENTS3.1 Operational Performance Characteristics
3.1.2 System Mission(s)
1]To focus on a region, number of hospitals in the region and conduct survey in each
hospital and develop an integrated report.
2]To give greater priority to severely injured patients,to effectively and efficiently use the
hospital resources by diverting the resources and to effectively predict the patientsurvivability time for any patient mix, and thereby route the patients accordingly.
3] To study the effects of injury/illness severities and a priority-based, routing system of
patients on their waiting times.
4] Continuous assessment of severity of patients and shifting them to other speciality
hospital in case severity level increases or to local hospitals,theatres or school in case
severity level decreases.
5] To ensure a patients complete recovery post treatment both physically as well as
emotionally.
7] To make suggestions to the local government on resource utilization to enable thecommunity to be better prepared in case disaster strikes again.
3.1.3 Phases of Operation:-
Our mission is divided into 5 Subsystem depending upon different types of work required
for management of hospital operations for regional disaster relief work.Work has been
divided among the different subsystems for proper maintainability and sustainability of the
system.
Phases of operations will be as follows:-
1] Initially there would be survey regarding the number of speciality doctors availiable in aparticular hospital,Operating Rooms,beds,hospitals in a particular area.In case a large
number of patients arrives,Some patients of less severity has to be shifted to temporary
hospitals.An integrated report containing all the database of a hospitals related to a
particluar area is made so that during emergency routing can be done properly and proper
recommendation can be proovided to the related authoritires regarding improvemnet in
available facilities.
https://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&cad=rja&sqi=2&ved=0CE0QFjAB&url=http%3A%2F%2Fwww.ahrq.gov%2Fqual%2Fhroadvice%2Fhroadvice.pdf&ei=6o0wUbPQMMWGrAes1IHwAg&usg=AFQjCNHntGHPpfIadUni2MdGj292iRYIOw&sig2=WfqZ_HIyXnixXztZaaOMmQ&bvm=bv.43148975,d.bmkhttps://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&cad=rja&sqi=2&ved=0CE0QFjAB&url=http%3A%2F%2Fwww.ahrq.gov%2Fqual%2Fhroadvice%2Fhroadvice.pdf&ei=6o0wUbPQMMWGrAes1IHwAg&usg=AFQjCNHntGHPpfIadUni2MdGj292iRYIOw&sig2=WfqZ_HIyXnixXztZaaOMmQ&bvm=bv.43148975,d.bmkhttps://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&cad=rja&sqi=2&ved=0CE0QFjAB&url=http%3A%2F%2Fwww.ahrq.gov%2Fqual%2Fhroadvice%2Fhroadvice.pdf&ei=6o0wUbPQMMWGrAes1IHwAg&usg=AFQjCNHntGHPpfIadUni2MdGj292iRYIOw&sig2=WfqZ_HIyXnixXztZaaOMmQ&bvm=bv.43148975,d.bmkhttps://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&cad=rja&sqi=2&ved=0CE0QFjAB&url=http%3A%2F%2Fwww.ahrq.gov%2Fqual%2Fhroadvice%2Fhroadvice.pdf&ei=6o0wUbPQMMWGrAes1IHwAg&usg=AFQjCNHntGHPpfIadUni2MdGj292iRYIOw&sig2=WfqZ_HIyXnixXztZaaOMmQ&bvm=bv.43148975,d.bmk -
8/12/2019 Earthquake forcasting
4/29
2] As soon as the disaster occurs there will be a team of severity analyst onsite who will
check the severity of the patients.Severity will be marked on a scale of three.According to
the level of severity of patients and database of the nearby hospitals and other
information,routing system will run a algorithm and willdecide on where this patients need
be translocated.
3] Routing system takes care of measures like change in the severity of patients during
routing,ambulance facilities depending on the information of severity analyst team and
survey team which gives the database regarding the available hospitals and roads leading
to it,etc
4] Once the patients reaches a particular hospital and he is operated he/she is kept under
constant evaluation of his/her severity levels.This is taken care by post disaster relief work
team.If there is a change in the severity levels of the patients he/she is redirected or
translocated to different speciality hospital or temporary hospitals.System also takes care
of moral support to the patients by informing patients relatives.It also take care of the back
up plans.
3.1.3.1 Pre-Mission Phase Operational Capabilities
Our system first surveys the existing conditions.We survey the operating environment.
Understand the functioning of hospitals and their capability to handle disasters. Survey the
increase in number of patients and the hospitals preparedness to handle them.Emergency
preparedness helps hospitals cope with this sudden surge of patients by making temporary
room and utilizing resources from other hospital departments.The hospital capacity information
can be used to make patient/ambulance routing decisions and resource allocations.
3.1.3.2 Mission Phase Operational
At the event of Disaster,Our Mission is stated as follows:
The On-Site Severity team rushes as fast as possible to the site.They make an
approximation of the number of casualties and calculate the severity levels of the patients
on the basis of various parameters , then on the basis of these severity and the database
already prepared by the Pre Mission Survey Team, They run the routing Algorithm and find
the nearest hospitals and since all transportation modes were already on standby ( like.,
Public/Private Ambulances , 108 etc) as the Disaster Occurred. And The same information
is been told to the hospital Staff about number of casualties to be brought there. then
without any delay patients are sent to the Hospital and the patient is under guidance of
severity team , so that if his severity changes again in between and accordingly his waiting
time decreases then are there any other measures to be taken like informing the hospital
about getting ready and receive the patient and shift him/her to the OR immediately.
3.1.3.3 Post-Mission Phase Operational Capabilities
-
8/12/2019 Earthquake forcasting
5/29
Post mission capabilities include work regarding taking proper care and provide
convenience and comfort to the patients.
1] Our system is capable of handling emergency shortages and failures like power,
communication, food shortage failures.
2] Hospital staff and relatives of patients are prepared for emergency evacuation
procedures incase the hospital itself is damaged due to the disaster.
3] The relatives of patients are trained to perform simple medical procedures so that the
staff can take care of more pressing issues.
4] System ensures complete physical and mental healing of the patient.
5] System also provides the guidelines to local authorities.
6]In case of severity of the patients changes he/she is shifted to other hospitals,thereby
increasing the efficacy of the whole system.
3.1.4 Mission Reliability
We have taken into consideration pre disaster management as well post disaster
management which make our system reliable.A proper survey is done regarding the
number of hospitals,facilities in a particular hospital,road to the particular hospital.This
survey is done very often to keep the database regarding the facilities updated.moreover
the algorithm we are going to implement is based on the real time data and proper
simulation.As health is so uncertain,there might be a sudden change in severity of the
patient.Considering this also there is a proper and continuous evaluation related to the
severity levels and if there is a change actions are take n accordingly.Attention has beengiven for giving moral support to patients which is very much necessary.We have also
taken into considerations the situations when hospital itself is affected by the disaster.For
this a proper back up plans has been prepared in case such situations arise.
3.1.5 System Maintainability
Though our system is a most crucial for the perspective of the nation,it has been divided
into proper subsystems.Work has been properly distributed depending upon the phases of
operations.A proper dependency and coordination between subsystem has resulted in amaintainable system as a whole.A continuous evaluation of the patients,updating the
database,etc has made our algorithm for routing more efficient.With each subsystem
working excellently well in their own domain provides its output to other subsystem which
thereby take actions accordingly.Due to proper distribution of work amongst the
subsystems and great coordination has resulted in maintainable system.
-
8/12/2019 Earthquake forcasting
6/29
Below each subsystem is described in detail:-
SubSystem 1 : Survey & Development
1.INTRODUCTION :During a disaster, the role of hospital becomes even more critical. It is vital to provide timely
treatment to patients injured in the disaster in order to minimize the fatalities. When a disaster
occurs, the number of patients who require treatment may increase 35 times the normal
volume. Rapid estimates of hospital capacity after a disaster can assist relief operations greatly.
Emergency preparedness helps hospitals cope with this sudden surge of patients by making
temporary room and utilizing resources from other hospital departments. The hospital capacity
information can be used to make patient/ambulance routing decisions and resource allocations.
1.1SCOPE:
Study the dependence of waiting time with incoming patient volume,patient mix and efficiency of
the hospital. Preparedness helps to cope with the sudden surge of patients with the limited
available resources. Timely treatment of injured victims helps to decrease the mortality rate.
1.2PURPOSE:
The purpose of the system is to survey about hospitals operational capabilities before any
disaster occurs. It is important to estimate hospital capacity as it can assist disaster mitigation
efforts to provide timely treatment to the injured and the ill. The hospital capacity information can
be used to make patients /ambulance routing decisions and resource allocations. The survey
covers all the factors which affects the hospital operations during disaster and focusses on
suggesting the development to the concerned authorities.
-
8/12/2019 Earthquake forcasting
7/29
These factors include survey of number of operating rooms,arrival of patients,availability of
doctors, severity of patients and their timely treatment, number of hospitals in the areas which
are disaster prone
2.References:
1.http://1.bp.blogspot.com/-oPlDxwyqoLM/Tya9ZjH1vlI/AAAAAAAAAN4/PDnwYfVx5Fg/s1600/HospitalManagementSystem-usecaseDiagram.bmp
2.https://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&ved=0CDkQFjAB&u
rl=http%3A%2F%2Fapicssoutheast.org%2FChattanooga%2FHealthCareManagement.pps&ei=lI
0wUffqHZHKrAfM04CIBw&usg=AFQjCNFFmdXPIcKV8nBlj-UHsi7vi7bnYw&sig2=Syc4EaQtV9Z
WuU1gjAIuIw&bvm=bv.43148975,d.bmk
3.https://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&cad=rja&sqi=2&ved
=0CE0QFjAB&url=http%3A%2F%2Fwww.ahrq.gov%2Fqual%2Fhroadvice%2Fhroadvice.pdf&ei
=6o0wUbPQMMWGrAes1IHwAg&usg=AFQjCNHntGHPpfIadUni2MdGj292iRYIOw&sig2=WfqZ_HIyXnixXztZaaOMmQ&bvm=bv.43148975,d.bmk
3.1OPERATIONAL PERFORMANCE CAPABILITIES
3.1.1.Latency:
Treatment in hospital usually requires a referral from a physician during a disaster .So if a
patient is referred to some other hospital in case of severe injury patient requires specialised
treatment .So he would be referred to another physician but we are conducting a pre disaster
survey which shows us the capacity of a physician to handle number of patients.If physician
cannot treat more than a specific number of patients then we have to automatically send a
message from the physician that he can't treat more patients and hence patients have to be
diverted to another hospital.
This is how latency can be minimised otherwise if physician does not send a message that he
can't treat more patients, then patients keep waiting endlessly and hence after having waited a
long time are shifted to another hospital.
Inspite of facing this situation they are diverted before hand.
3.1.2.SYSTEM MISSION AND PERFORMANCE:
3.1.2.1System Entities
Team of people involved in this survey form an important entity of the system. Other entities
are, on whom the survey is conducted physicians,patients,housekeeping persons,ward
incharge,nurses. System entities also constitute of the number of beds,operating rooms,
Emergency departments, operating equipments.
3.2.2 Mission :
https://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&cad=rja&sqi=2&ved=0CE0QFjAB&url=http%3A%2F%2Fwww.ahrq.gov%2Fqual%2Fhroadvice%2Fhroadvice.pdf&ei=6o0wUbPQMMWGrAes1IHwAg&usg=AFQjCNHntGHPpfIadUni2MdGj292iRYIOw&sig2=WfqZ_HIyXnixXztZaaOMmQ&bvm=bv.43148975,d.bmkhttps://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&cad=rja&sqi=2&ved=0CE0QFjAB&url=http%3A%2F%2Fwww.ahrq.gov%2Fqual%2Fhroadvice%2Fhroadvice.pdf&ei=6o0wUbPQMMWGrAes1IHwAg&usg=AFQjCNHntGHPpfIadUni2MdGj292iRYIOw&sig2=WfqZ_HIyXnixXztZaaOMmQ&bvm=bv.43148975,d.bmkhttps://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&cad=rja&sqi=2&ved=0CE0QFjAB&url=http%3A%2F%2Fwww.ahrq.gov%2Fqual%2Fhroadvice%2Fhroadvice.pdf&ei=6o0wUbPQMMWGrAes1IHwAg&usg=AFQjCNHntGHPpfIadUni2MdGj292iRYIOw&sig2=WfqZ_HIyXnixXztZaaOMmQ&bvm=bv.43148975,d.bmkhttps://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&cad=rja&sqi=2&ved=0CE0QFjAB&url=http%3A%2F%2Fwww.ahrq.gov%2Fqual%2Fhroadvice%2Fhroadvice.pdf&ei=6o0wUbPQMMWGrAes1IHwAg&usg=AFQjCNHntGHPpfIadUni2MdGj292iRYIOw&sig2=WfqZ_HIyXnixXztZaaOMmQ&bvm=bv.43148975,d.bmkhttps://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&ved=0CDkQFjAB&url=http%3A%2F%2Fapicssoutheast.org%2FChattanooga%2FHealthCareManagement.pps&ei=lI0wUffqHZHKrAfM04CIBw&usg=AFQjCNFFmdXPIcKV8nBlj-UHsi7vi7bnYw&sig2=Syc4EaQtV9ZWuU1gjAIuIw&bvm=bv.43148975,d.bmkhttps://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&ved=0CDkQFjAB&url=http%3A%2F%2Fapicssoutheast.org%2FChattanooga%2FHealthCareManagement.pps&ei=lI0wUffqHZHKrAfM04CIBw&usg=AFQjCNFFmdXPIcKV8nBlj-UHsi7vi7bnYw&sig2=Syc4EaQtV9ZWuU1gjAIuIw&bvm=bv.43148975,d.bmkhttps://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&ved=0CDkQFjAB&url=http%3A%2F%2Fapicssoutheast.org%2FChattanooga%2FHealthCareManagement.pps&ei=lI0wUffqHZHKrAfM04CIBw&usg=AFQjCNFFmdXPIcKV8nBlj-UHsi7vi7bnYw&sig2=Syc4EaQtV9ZWuU1gjAIuIw&bvm=bv.43148975,d.bmkhttps://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&ved=0CDkQFjAB&url=http%3A%2F%2Fapicssoutheast.org%2FChattanooga%2FHealthCareManagement.pps&ei=lI0wUffqHZHKrAfM04CIBw&usg=AFQjCNFFmdXPIcKV8nBlj-UHsi7vi7bnYw&sig2=Syc4EaQtV9ZWuU1gjAIuIw&bvm=bv.43148975,d.bmkhttp://www.google.com/url?q=http%3A%2F%2F1.bp.blogspot.com%2F-oPlDxwyqoLM%2FTya9ZjH1vlI%2FAAAAAAAAAN4%2FPDnwYfVx5Fg%2Fs1600%2FHospitalManagementSystem-usecaseDiagram.bmp&sa=D&sntz=1&usg=AFQjCNHE_CR945Z5_jv2K485P8mY9fQtmghttp://www.google.com/url?q=http%3A%2F%2F1.bp.blogspot.com%2F-oPlDxwyqoLM%2FTya9ZjH1vlI%2FAAAAAAAAAN4%2FPDnwYfVx5Fg%2Fs1600%2FHospitalManagementSystem-usecaseDiagram.bmp&sa=D&sntz=1&usg=AFQjCNHE_CR945Z5_jv2K485P8mY9fQtmg -
8/12/2019 Earthquake forcasting
8/29
To focus on a region, number of hospitals in the region and conduct survey in each hospital
and develop an integrated report.
System performance depends on how well the survey is conducted and how much reliable is
it.
3.3 Phases of operation:
Pre-Mission Operations : It is required that a trained group of people are selected who can
conduct a survey and give a detailed report.
Its important to arrange funds before the survey is conducted. Its either the government or an
Non government organisation who can provide the funds.
Also transport facilities must be available for this operation.
Mission Phase Operations : Talking to hospital staff , doctors , patients and make a record of
availability time of doctors, number of patients each can handle, if number and type of
equipments are sufficient enough, number of bedrooms in the hospital, operating roomefficiency. In case of increase in number of patients arrangements have to be made to source
supplies from other places and ensure their quick delivery. Nearby doctors can be located to
immediately reach the hospital.
Post Mission Operations: To Create an integrated report of the survey and suggesting the
concerned authorities to take actions and make changes in their operational capabilities
accordingly.
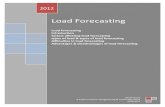
4.USE CASE DIAGRAM:
-
8/12/2019 Earthquake forcasting
9/29
5.1.SYSTEM AVAILABILITY:
1. Health service and hospitals are not available in many regions affected by disasters. It is
difficult to reach them even if they are close by sometimes. In this situation locations for make
shift hospitals are to be located in several areas.
2. Also till the time being these suggestions for make shift hospitals are forwarded to
government, we will be locating public places which can serve us for relief operations after a
disaster when availability of hospital is not there and also the patient is severely injured.
5.2.SYSTEM RELIABILITY:
We aim at performing surveys after every 6 months that whether the hospitals still have
-
8/12/2019 Earthquake forcasting
10/29
the same facilities or they have come up with some new technologies or new facilities for
patients and we will be tracking that in our records so that these things can be utilised during a
disaster.
We also aim to verify that hospitals are operating efficiently. To ensure that they are following the
standards expected of them. The supplies they use should be of high quality. To ensure they arenot indulging in unfair trade practices.
5.3.SYSTEM MAINTAINABILITY:
It is important that the functioning of the system is maintained over time ,i.e we overlook
our survey policies. Review if we have required number of officials to conduct a proper survey, if
the funding provided is efficiently utilised to pay the officials , take care of transport facilities etc.
There also has to be a check on the time intervals after which survey has to be conducted, and
proper coordination and communication with the government regarding this survey is also to bedone at regular intervals.
SUBSYSTEM 2:
To study the effects of injury/illness severity:
1.0 Introduction
1.1 System scope:At the time of a disaster there are victims on-site with different injury levels. Patients
with different severities of injuries have different survivability times. Not just that,
classifying the victims on the basis of severity of injury allows for judicious use of
hospital resources(imperative during disaster situation). Therefore, patients must be
classified according to the severity of injuries/illnesses, and priorities assigned based
on survivability time so that every victim gets optimum resources and treatment. The
scope of our system is confined to examining victim and assigning them severity
levels and survivability times. The patient is continuously examined to check for any
changes in severity level until he is operated on in Operating Room(OR). The
collected data is sent to the routing team.
Stakeholders:
Disaster victims
Health personnels
Data loggers
Patient's family
-
8/12/2019 Earthquake forcasting
11/29
1.2 PURPOSE:Patients with different severities of injuries have different survivability times.
Therefore, the purpose of this subsystem is to classify the patients according to the
severity of their injuries/illnesses. Higher priorities are assigned to the patients withlower survivability time so as to dedicate optimum resources to needy patients a the
right time.
1.3 System overview: Medical teams are deployed in disaster site with necessary tools.
The victims are examined/diagnosed.
Survivability times are assigned based on severity level and other data obtained
through examination.
Based on examination of patients three different levels of severities are
considered. Severity 1 class patients are patients with minor injuries, e.g.,lacerations, cuts, wounds, minor respiratory problems, fractures, who do not
require surgery. Severity 2 patients are patients who arrive with comparatively
more severe problems, and might not require surgery. Severity 3 patients are
the highest severity patients, arriving with major issues, e.g., burns, head
injuries, fractures, which require surgery. Since Severity 1 patients do not
require surgery, only Severity 2 and Severity 3 patients are considered in the
queue before entering the Operating Room(OR).
Each ambulance contains a personnel who is constantly monitoring the victim
and reassessing his severity level. The reasons for doing so follow:
(i) The patient's severity may remain the same as it was before
transportation, but the survivability time may decreased
(ii) The patient's severity type may change during transportation and
decrease survivability time as a result.
2.0 Referenced DocumentsTransient Modeling in Simulation of Hospital Operations for Emergency Response -
Jomon Aliyas Paul, PhD Santhosh K. George, MS Pengfei Yi, PhD Li Lin, PhD.
3.0 Requirements Teams of well trained health assistants and doctors are required to examine the
patients on site, in ambulance and in hospital right until they are operated on.
Different examination and diagnostic tools are required based on the kind of
disaster.
3.1 Operational performance characteristics: Minimize latency by rapidly deploying the response team with adequate
-
8/12/2019 Earthquake forcasting
12/29
personnel to handle the disaster situation.
Availability of advanced tools and techniques for diagnosis and examination of
victims.
Performance of deployed personnel based on the accuracy of assigned severity
and usefulness of the model as a whole in improving operational efficiency and
effectiveness. Performance of the team as a whole can be increased bydeploying experienced personnels and experts in a given disaster situation.
3.1.1 System missions: To give greater priority to severely injured patients thereby reducing the total
patient waiting time by considering the patient survivability times.
To effectively and efficiently use the hospital resources by diverting the
resources to the needy patients during disaster situation.
To effectively predict the patient survivability times for any patient mix, and
thereby, the routing of patients in order to provide medical attention as soon as
possible.
3.1.2 Phases of operation:
3.1.2.1 Pre-Mission Phase Operational Capabilities Training of health personnels preparing them for disaster situations using
simulations.
Availability of health personnels prior to disaster.
Availability of equipments necessary for diagnosing and examining the victims
in disaster zones.
Expert knowledge of injuries during different types of disasters and skills to
operate different tools during the same.
3.1.2.2 Mission Phase Operational Capabilities Trained personnel who can examine the patients and provide reliable
data/output based on which routing team can take appropriate action.
A personnel to examine the patient during transportation and waiting(until the
patient is operated on) to monitor the change in his injury/illness severity if
any.
Data logging equipments to log data on patients' condition.
3.1.2.3 Post-Mission Phase Operational Capabilities Analyze the effectiveness of system of assigning severity levels and
survivability time to different patients.
-
8/12/2019 Earthquake forcasting
13/29
Upgrade the equipments based on the success of equipments deployed.
3.1.3 System Reliability Quickly respond to any disaster alert.
Using state-of-the-art tools and techniques for diagnosis and examination.
Ensuring that health personnels are motivated to face the on-site situation.
Retrain the health personnels in regular interval of time(3-6 months) and test
them to ensure that their work remains effective through and through.
3.1.4 System Maintainability Assess the shortcomings in the model(dividing victims on the basis of severity
of illness and assigning priorities) through trial and error and make changes to
the model if need be.
Work towards making the model more effective such that more patients are
diagnosed, analyzed and examined quickly and more effectively.
Ensure that the model is equally effective in any kind of disaster(earthquake,
tsunami, fire et cetera).
3.1.5 System Availability The team should be prepped to be deployed at any period of time.
All the diagnostic tools(for any kind of disaster) should be available for on-site
deployment at all times.
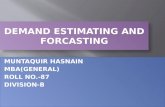
Use case diagrams:
-
8/12/2019 Earthquake forcasting
14/29
-
8/12/2019 Earthquake forcasting
15/29
SUBSYSTEM - 3 Routing system
1. Introduction1.1. ScopeRouting of the patients depending on the severity and types of injuries, along with
pre-acquired knowledge and information about the hospitals and similar facilities , taking
patient Mix and pre-hospital time into consideration.
1.2. Purpose
To reduce the patients waiting time and providing them appropriate medication byimplementing efficient priority based routing algorithm depending upon the data of nearby
hospitals and similar facilities which will be collected by survey subsystem. Thereby,
reducing severity and discomfort caused to victims of disaster. Also the purpose is to
develop a metamodel which provides best available medical facilities to the victims,
therefore, reducing mortality rate in the event of any disaster or an emergency.
1.3. Subsystem Overview
SubSystem includes following components:1] Database containing information about hospitals, clinics and the places where
emergency medical services can be provided and it will also include information about the
patients according to severity, survivability time feeded as output by Severity Analysis
Subsystem.
2] Algorithms designed for transient modeling, factorial modeling, generic modeling and
offline simulations.
3] Hospital Routing Managing and Assisting team.
4] Well Equipped Ambulance and Other Transportation Vehicle System.
5] As the survey subsystem updates the database, that coordinates with various
government agencies and private clinics, physicians to utilise all the available resources.
2. Referenced Documents :
Transient modeling in simulation of hospital operations for emergency
response.
-
8/12/2019 Earthquake forcasting
16/29
By : Jomon Aliyas Paul, PhD Santhosh K. George, MS Pengfei Yi, PhD Li Lin, PhD
http://www.mendeley.com/catalog/transient-modeling-simulation-hospital-o
perations-emergency-response/
3. Requirements :
3.1 Operational Performance Characteristics :
3.1.1. System Definition:
Analysis of the effects of priority based routing of patients within the hospitals and affects
on the patient waiting times determined using various patient mixes. THe system guides
the patients based on the severity of injuries and queues the patients requiring critical care
depending upon their remaining survivability time.
3.1.2 System Missions:
1] A real time simulation model that will take input the priority queue and return the routing
structure, which will help us to route causalities on the basis of their sustainability time.
2] To study the effects of injury/illness severities and a priority-based, routing system of
patients on their
waiting times.
3] System should be able to cater the changes in severity levels and type of injuries.
4] To make the routing system more efficient and reliable by studying the effects of patient
mix of various severities using offline simulation.
3.1.3 System Phases of Operation:
1] Taking Input from the severity analyst present at the location of disaster.
2] Running the routing algorithm on the data provided by severity analyst and survey
subsystem and also the continuous evaluation team which continuously evaluates the
current status of hospital, weather conditions,traffic, etc
3] Routing according to priority queue and the data from above point and available
transportation modes.
4] Coordinating with hospital staff and adjust the patient in the queue of OR (Operating
Room) on the basis of remaining allowable waiting time.
5] Allocation of wards to the patient after operation.
6] For Severity 1 making temporary rooms and utilising resources from other hospital
departments.
http://www.google.com/url?q=http%3A%2F%2Fwww.mendeley.com%2Fcatalog%2Ftransient-modeling-simulation-hospital-operations-emergency-response%2F&sa=D&sntz=1&usg=AFQjCNEaghP3yk-Yn_dWEK-iFSTtGuWxkQhttp://www.google.com/url?q=http%3A%2F%2Fwww.mendeley.com%2Fcatalog%2Ftransient-modeling-simulation-hospital-operations-emergency-response%2F&sa=D&sntz=1&usg=AFQjCNEaghP3yk-Yn_dWEK-iFSTtGuWxkQ -
8/12/2019 Earthquake forcasting
17/29
3.2 System Capabilities:
1] Our system will be capable of providing real time simulation of hospitals capacity andresources available in that disaster prone area.
2] It will also be capable of routing the patient from the disaster prone area to hospital and
also from hospital to the OR(operating room) with the capability of routing the patient to
correct place and within the
required time as per the survivability time of the patient.
3.3 System Feasibility:
1] Our system feasibility depends on two broader aspects one is costand another is value
to be attained.
2] Our system will be more feasibleif our real time simulation requires less resources in
terms of cost
and gives the best routing plan in required time for the particular disaster which has
occurred.
3] Our system feasibility will be affected by many factors such as : Traffic during routing ,
facility damage in hospital due to disaster, Shortage of Resources due to sudden surge of
patients in hospital, Dynamics of Hospital etc.
4] Our System will become more feasible if we are capable of changes in our routing plan
and generating new routing plan on the basis of the current circumstances.
3.4 System Reliability:
The design of simulation experiments using factorials and off-line simulation runs, a
generic simulation model has been developed that can represent any hospital with various
ED patient volumes, hospital size, and operating efficiency. Parametric response surface
model thus represents the steady-state behavior of the system. By further combining the
transient behavior with this generic hospital model, a meta-model is prepared to capture
the temporal behavior of hospitals during a disaster. Thus our meta-model can handle
various worst case conditions. Our system can handle sudden surge of patients as ourmeta-model can route patients to private clinics as well.
3.4.1. Cost of Performance: The cost of performance of our system is affordable.
Algorithms design and implemetation of various models are one time investment. And its
very convinient and cheap to run offline simulations which will improve system performance.
-
8/12/2019 Earthquake forcasting
18/29
3.5 System Maintainability:
Maintainability means characteristic of design and installation which determines the
probability that a failed equipment, machine, or system can be restored to its normal
operable state within a given timeframe, using the prescribed practices and procedures. Itstwo main components are serviceability (ease of conducting scheduled inspections and
servicing) and reparability (ease of restoring service after a failure).
Our system maintainability mainly depends on simulation and cost and also on some other
factors like hospital support, traffic, weather. If all works fine then our system can efficiently
determine the routing structure in real time disaster. This can probably reduce number of
deaths in disaster.
3.6. System Availability:This is one of the crucial elements of our system, as our subsystem directly dealswith lives of patients while routing, the routing subsystem should be available at all times
from the instance just after the disaster to the instance treatment starts.The subsystem
makes sure that at any point of time, there shouldnt be a scenario in which patient is left
unattended due to some sort of unavailability of the system.
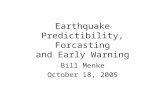
3.7: Use Case
-
8/12/2019 Earthquake forcasting
19/29
-
8/12/2019 Earthquake forcasting
20/29
4. Conclusion:
1] The model gives greater priority to severely injured patients thereby the total patient
waiting time considering the patient survivability times reduced and effective and more
efficient use of hospital resources can be accomplished.
2] The model can predict the patient waiting times for any patient mix, and thereby, therouting of patients can be done effectively in order to receive medical attention as soon as
possible.
Subsystem 4: PreHospital Time
1.Introduction
1.1. Scope
To study the effects of pre-hospital transport time on patient waiting time and mortality. Ifthe transport time is too long, this might change the severity of the patients injuries, thereby
reducing the available survivability time.
1.2. Purpose
Patients during a disaster are classified according to the severity of injuries/illness. High
prehospital transport times can increase the severity level lead to the development of a
more serious severity type.Therefore, prehospital transport time is considered as an
important factor affecting the mortality rate.
1.3 Subsystem Overview
Our subsytem includes a database containing information about patient mixes of various
severities and information about the classification of patients according to severity level of
patients entered by Severity Assessment Subsystem.
-
8/12/2019 Earthquake forcasting
21/29
2. Use Case Diagram
3. Requirements :
3.1 Operational Performance Characteristics :
To analyse the hypothesis that a prehospital time threshold exists that when
exceeded, significantly increases the waiting time and the mortality of patients
transported directly from the scene of injury to the closest hospital.
Coordinating and taking inputs from the Severity Analyst present at the location of
the disaster.
A real time simulation model will take severity level of the injured people as input
-
8/12/2019 Earthquake forcasting
22/29
and will prepare a priority queue in order to make the routing easier .
3.2 System Capabilities:
The system is capable to take sufficiently large number of inputs, so as to be able to
handle disasters of any level.
The system ensures adherence of emergency medical services to the protocol, as
well as subsequent associations with patient treatment times and outcomes by
linking data with the other related parts of the system.
The system is capable of coordinating with the routing system.
3.3 System Feasibility:
The system consists of a good and well experienced severity analyst so that proper
and accurate level of severity can be known in real time.
The priority queue depends on many factors like age, brain damage suffered if any,
burns etc. Thus, a well modelled queue is used.
To ensure feasibility, various details of hospitals is used while making the priority
queue, for eg:- if a person needs surgery and another has suffered bone damage
and needs orthopaedic then they must be placed accordingly in the queue so that
they can be transported to specialised hospitals.
3.4 System Reliability:
As the system takes into consideration a large number of factors to decide the level
of injuries suffered, the priority queue which is returned is very much reliable.
As system uses the organised data collected from the survey team, it is able to
make the queue in a systematic and in real time.
Three levels of severity are implemented, so as to properly organise and simplify
the priority queue formed.
3.5. System Maintainability:
The system needs real time updation of the databases at the time of disasters.
For example,during a disaster the hospitals need to update their status after admittingevery patient. This database needs to be maintained at a common place where all the
hospitals and ambulance can see it and also make changes to it. In this way the ambulance
will be able to check which is the NEAREST HOSPITAL with AVAILABLE
RESOURCES.This will help in reducing the pre-hospital transport time.
-
8/12/2019 Earthquake forcasting
23/29
3.6. System Availability:
This is one of the crucial elements of our system, as our subsystem directly deals with lives
of patients , the system should be available in all kind of scenarios and at all the times . The
two basic structural components needed are : The availability of hospitals that meet the need of patients.
The availability of a Expert Analyst , who can study the effects of prehospital
transport time in real time and can accordingly give input to Routing Team.
3.7. System Development:
The system can be developed as it is being used. It can be developed further by taking into
consideration various case studies like the Bhuj Earthquake , Tsunami , or the recent
Bomb Blasts in Hyderabad.
3.8. Dependency:
Our subsystem depends on other subsystems and vice-versa in the following manner:
The Severity Assessment Subsystem provides us details about the severity of levels
of patients.
Our Subsystem Analyst studies and analyses the input and accordingly gives input
to Routing Subsystem.
4. Conclusion:
The model can study the effects of prehospital transport time and can accordingly predict
the patient waiting times for any patient mix, and thereby, the routing of patients can be
done effectively in order to receive medical attention as soon as possible.
-
8/12/2019 Earthquake forcasting
24/29
Subsystem 5: Post Disaster Relief
1. Introduction1.1. ScopeProvide relief medically,emotionally and financially to the patients once he/she is within the
confines of the hospital and provide proper routing to other speciality wards or other hospitals
depending upon the change in the severity of the patients.
1.2. PurposeTo provide comfort as well as convenience to the patient and others by calming them down
,provide emotional support in case of any panicking ,shifting them to different hospital(oncethe severity level changes), communicating and engaging the relatives of the patient and
evacuating hospitals in case of a threat to the hospital. Thereby, reducing severity and
discomfort caused to victims of disaster.Also equipping hospitals with backup facilities like
communication systems,power,blood and pharmacy in case of a large amount of patients.
1.3. Subsystem OverviewSubSystem includes following components:
1] Database containing the severity of the patients so that we can update them whenever
there is change in severity of the patients.
2] Properly equipped and comfortable facilities for shifting of patients from the wards to the
ambulance.
3] Well equipped Ambulance dedicated just for shifting of patients from one hospital to
others.
4] Back up services such as communication systems for informing patients relatives,
-
8/12/2019 Earthquake forcasting
25/29
increased medication required in case of larger amount of patients arrived,power and
networking backup which might fails as result of the disaster.
5] Economic plans to provide relief to the patients.
6] Counselling and assisting team to provide moral support to patients.
2. Referenced Documents :
http://www.urban.org/UploadedPDF/411348_katrinahospitals.pdf
Bradford H Gray and Katy Hebert.
3. Requirements :
3.1 Operational Performance Characteristics :
3.1.1 System Definition
Analysis of change in the severity of the patients and subsequently providing proper
translocation to other hospitals.This Subsystem takes care of the patients personal needs
as well as makes the whole system efficacious by taking care of the backup services.
3.1.2 System Missions:
1] Estimating the currently available resources within the hospitals and shifting of patients
in case severity of the patients cannot be treated with the available resources of hospital.
2] To provide maximum comfort and convenience to the patients by communicating with
their relatives.
3] Encourage and provide emotional support to patients.
4] Keeping in contact with the backup services and agencies (especially transport and
pharmaceutical ).
5] Continuous assessment of severity of patients and shifting them to other speciality
hospital in case severity level increases or to local hospitals,theatres or school in case
severity level decreases.
6] To provide for a ready-response to all foreseeable problems identified above.
7] To prepare hospital staff and relatives alike for emergency evacuation in case the
hospital itself gets affected adversely
8] To ensure a patients complete recovery post treatment both physically as well as
emotionally
9] To make suggestions to the local government on resource utilization to enable the
community to be better prepared in case disaster strikes again.
http://www.google.com/url?q=http%3A%2F%2Fwww.urban.org%2FUploadedPDF%2F411348_katrinahospitals.pdf&sa=D&sntz=1&usg=AFQjCNGx7JNwWkvUU8caOl2Xgj5Rw_1SxQ -
8/12/2019 Earthquake forcasting
26/29
3.1.3 System Phases of Operation:
1] Once the patient reaches the hospital,he/she is under continuous evaluation regarding
changes in its severity levels.Thus our system will take input from the severity analyst
present inside the hospital.
2] If the severity level of the patient is out of scope of treatment of the hospital immediateactions is taken by our system for translocation of the patients.
3] Relatives of the patients who are operated in a particular hospitals are informed.
4] Even after the patients are operated they are under continuous evaluation regarding the
severity levels by the severity analyst,and thus shifting accordingly to the other speciality
hospitals.
5] If the patient's severity level reduces to level 1 he can be transferred to local hospitals or
theatres or camps.
6] Our system will be ready with the back up plans regarding evacuation of the hospitals if
the hospital is got to be affected by the disaster or power failure or requirement of more
medication.
7] After all this our assisting team will take a survey of patients who are in need of the
economic aids related to their operations and then will talk to the government to provide for
the same.
3.2 System Capabilities:
1] Our system is capable to manage any difficult circumstances like power and
communication failure.
2] Hospital is capable of sustaining itself incase the hospital itself is damaged due to the
disaster.
3] Hospital can cope up with large number of patients by setting up of temporary hospitals
in places like schools,hospitals and hotels.
4] Our system also deals with the sudden shortage of pharmaceuticals and blood in case
of high casualties
3.3 System Feasibility:
1]The medical staff (like nurses) and the patients relatives can be easily instructed to
provide emotional support to the patients.
2]Essential advice and guidance will be provided by other relief teams at establishments.
3]Disaster preparedness and response courses may be conducted in identified prone
areas.
-
8/12/2019 Earthquake forcasting
27/29
3.4 System Reliability:
The system will prove very reliable in case a disaster strikes because :
1] Nearly all possible foreseeable shortcomings in hospital operations like
power,communications etc are covered which ensures a high level of reliability.
2]Taken into consideration the backup plans for damage caused to the hospital itself.3] Special attention is paid to a patients emotional recovery including involving his/her
relatives as part of recovery
4] The local government is also intimated about the latest changes in status quo
post-disaster. Also once post-disaster survey is completed appropriate guidelines can be
suggested to be incorporated as part of law.
5] The patients situation when applying for governmental aid can also be passed on to the
concerned authority.
3.5. System Maintainability:
This involves a large amount of work from the team as :
1] The team has to continuously update the database after conducting surveys in different
hospitals during critical base.
2] The local authorities are also to be kept in constant touch
3] Maintaining back up facilities at hospitals does require a significant amount of capital
investment from the parent organizations of the hospital concerned.4] As patient mix during disaster is dynamic the hospitals are to be intimated with the
lessons learnt from various disasters around the world along with the treatment techniques,
which are constantly updated on a central server.
5] Also the local schools and theatres must be surveyed and emergency aid packets be
warehoused in them so that emergency camps can be easily set up
3.6. System Development:
We can expand our system by including warning indicators:
1] Early warnings: These are the best if we can provide them.They provide valuable time to
other systems which may be helpful in managing the situation at the time of disaster.
2] Management of slow-onset hazards (such as drought) will be easy as the meteorological
services are reliable enough to predict the climatic changes in a region,also they provide a
long warning time.
-
8/12/2019 Earthquake forcasting
28/29
3]We need to have an idea about the risk perception of the local community. The risk
perception may vary from society to society and we need to be able to explain them the
situation.
4]An effective communication system should be established and the readiness of supplies,
equipment, transport, communication and personnel should be confirmed.
4. Use-Case Diagram
-
8/12/2019 Earthquake forcasting
29/29