Early safety assessment of drug candidates: Utility of in ... · Early safety assessment of drug...
29
Early safety assessment of drug candidates: Utility of in vitro pharmacological profiling Laszlo Urban, Steven Whitebread, Jacques Hamon, Gul Erdemli , Eugen Lounkine & Patrick Mueller 1 Preclinical Safety Profiling & PreClinical Safety, NIBR Cambridge F.D.A. Issues Strictest Warning on Diabetes Drugs
Transcript of Early safety assessment of drug candidates: Utility of in ... · Early safety assessment of drug...

Early safety assessment of drug candidates:
Utility of in vitro pharmacological profiling
Laszlo Urban, Steven Whitebread, Jacques Hamon, Gul
Erdemli , Eugen Lounkine & Patrick Mueller1
Preclinical Safety Profiling & PreClinical Safety, NIBR
Cambridge
F.D.A. Issues Strictest Warning on Diabetes Drugs

Safety Risks: Mitigation in support of risk
management
• Moving from idiosyncratic towards target based ADRs:– Links between chemical structure – target – molecular mechanism –disease (human)
– Data analysis and interpretation based on learning processes: modeling & simulation;
SAR, predictive in silico tools to cluster in vitro–in vivo–clinical data with structures
• Introduction of parallel, iterative optimization of potency/
efficacy, drug-like properties, including ADRs
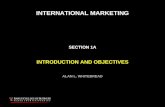
Toxicities leading to drug withdrawal from the US market (1976-2005)
Wilke RA et al. Nature Revs Drug Discovery 6 (2007)
1
2
3
4
5
6
Hepatotoxicity (6)
Nephrotoxicity (2)
Cardiotoxicity (2)
TdP (6)
Rhabdomyolysis (2)
Other (10)

Risk mitigation and risk management
Chemical
series / scaffold
Single
molecule
Risk
management
Risk
mitigation
Efficacy
Safety

EARLY and SHORT iterative cyclesTo maximize safety profile of lead molecules
LEAD STAGE
ACTIVELY optimizing safety
profile is of utmost importance
LATER STAGES
Safety-related activities largely
restricted to recognition,
assessment and management
of adverse effects.
Tailored mitigation strategies:
Off-target safety profiling
EARLY and SHORT
iterative cycles
Test
Evaluate
Design • MinimizedAttrition atlater stages
• MaximizedSafetyprofile

What are the Chances of Success?Pergolide Ropinirole

What are the Chances of Success?Pergolide
Withdrawn:
Valvular heart disease
Ropinirole

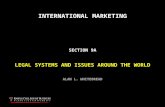
GPCRs 38
Transporters 4
Ion channels 8Enzymes 5
Nuclear receptors 5
Proteases 4
Kinases 8
In vitro Safety Profiling Assay Panels: What & Why to Include?
Primary assay panel (24 targets)
Full assay panel (72 targets)GPCRs 12
Transporters 3
Ion channels 1
Enzymes 4
Nuclear receptors 2
• Targets associated with serious ADRs & high hit rates
• Biochemical & functional cellular assays
• + assays with lower hit rates• + additional functional cellular
assays• + kinases & proteases
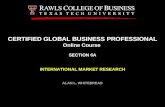
In vitro arsenal for early safety assessment Human target based assays

Clinical
Development
Lead
identification
Lead
Selection
Lead
Optimization
CCPre-clinical
Development
Early identification of
potential liabilities &
promiscuity.
Assessment based
on chemical series
Full characterization
before administration in
humans – Mechanistic
understanding
Design liability out
using SAR on
individual targets
In vitro safety pharmacology panelsWhen and how are they used ?
ManageMitigate
Primary Full Primary Full, Selectivity
Individual assays on request

Determining association with clinical ADRs
9
Selecting drugs,
adverse effects, and
subpopulationsStrong signal
identification
Distribution in
subpopulations
Compound
structure and
names
Selected adverse
reactions
Observed number of reports
Exp
ecte
d n
um
be
r o
f re
po
rts
Adolescents
Females

Determining association with clinical ADRs
10
Selecting drugs,
adverse effects, and
subpopulationsStrong signal
identification
Distribution in
subpopulations
Compound
structure and
names
Selected adverse
reactions
Observed number of reports
Exp
ecte
d n
um
be
r o
f re
po
rts
Adolescents
Females

O O
NHS
O
O
OH
Cardiac ADRs of marketed PPAR agonists
Rosiglitazone Troglitazone Pioglitazone
Common features
Same target and same indication
All drugs are in the same chemical class
All generate cardiovascular ADRs , however to different extent
All are “clean” of off-target cardiovascular effects

Rosiglitazone & Pioglitazone: “Clean” off-target profile....
AERS reports:
Cardiac disorders (leading)Eye disorders
GI disorders
Hepatobiliary disorders
Metabolism and nutrition
Musculoskeletal and connective tissue
Nervous system (cerebrovascular)
Psychiatric
Renal and urinary
Respiratory, thoracic
Social
Vascular
....however, the clinical
picture is different:

ADR profile of competitor: same indication/different target Sitagliptin (Januvia)
Cardiac Renal/urinary (no cancer) Hepatobiliary
No reports No reports No reports
Skin disorders Pancreatitis
Target: DPP4 (inhibitor) Indication: Type II Diabetes

Targets Potential ADRs Clinical evidence
• hERG inhib. Ventricular arrhythmia Terfenadine, astemizole, cisapride
• 5HT2B ag. Cardiac valvulopathy Fenfluramine, Pergolide
• PDE4 inhib. Emesis, vasculitis- PDI 747
• H1 antag Sedation Antihistamines
• M2 antag Bronchoconstriction Rapacuronium
• NMDA Channel inhib. Hallucination PCP (Phencyclidine)
• Dopamine D1 ag. Dyskinesia Levodopa
• EGFR inhib. Acneiform RashGefitinib, Erlotinib, Lapatinib,
Panitumumab (Black box)
Compounds withdrawn from market or failed during clinical development due to safety
Examples of targets associated with clinical ADRs

In vitro profiling is informative but limited.....(The entire relevant target space cannot be profiled in vitro)
....in silico approaches can predict potential off-targets based on chemical similarity to known ligands
Profiling panels Potential (off)-targets
Hopkins & Groom, Nature Rev. Drug
Disc. 1, 727
in vitro in silico
15

Compound sets
Drugs with adverse effect
Compounds binding
target XY
Linking targets and ADRs using chemical featuresStatistical models as a “common language”
Structural
features
Score
Score
Score
SScore
Scheiber et al. 2009, J Med Chem 52, p. 3103
Shared chemical features

How to interpret off-target data?Introduction of Off-target coverage
IC50 = 1µM Cmax = 1µM
Cmax = 10µM
Cmax = 0.1µM
10x coverage(ie. exposure 10x above IC50
= 0.1x MARGIN)
1x coverage(ie. exposure just at IC50
= 1x margin)
0.1x coverage(ie. exposure 10x below IC50
= 10x MARGIN)
10x
10x

Case study: Balanced early assessment of cardiosafety
From hERG inhibition to cardiac off-target panel
!

PDE3 is expressed in cardiomyocytes & platelets
Increases inotropy in the heart
Indication: Cardiotonic in heart failure (Milrinone) - Thrombocytopenia (Anagrelide)
ADR: PDE3 inhibitors increase mortality in ~10% of chronic heart failure patients
PDE3: An off-target associated with serious ADR in CHF
FPC
[nM]
hPDE3 IC50
[nM]
Fractional Coverage
(Cther, free / IC50)
Milrinone (Primacor® – discontinued) 284 290 0.98
Enoximone (Perfan® - ↑ mortality) 846 1300 0.65
Inamrinone (Inocor® – discontinued) 8974 15900 0.56
» Conclusion: For clinically significant PDE3 inhibition free therapeutic plasma
concentrations at or even below the hPDE3 IC50 are sufficient.
» Fractional target coverage of marketed drugs can determine likelihood of off-
target specific effects of drug candidates at TFPC (AUC or Cmax, free)

c-Met inhibitors show strong PDE3 inhibition – myocyte necrosis
PF-04254644
PDE3: 0.2µM°
°AGUIRRE, SA. Et al, Toxicologic Pathology, 2010
N
N NN
N
N
N Chiral
*Fibrosis of the myocardial interventricular
septum
Control rat myocardium
7 day treatment with PF
10

(Off-)target coverageExample using marketed PDE3 inhibitors
Human PDE3 IC50
[µM]
Total drug:
Cth
[µM]
PPB
[%]
Free drug:
Cth
[µM]
Total drug:
Coverage
(Cmax ÷ IC50)
Free drug:
Coverage
(Cmax ÷ IC50)
Inamrinone(US: Inocor® – discontinued)
15.9 12.8 30 8.97 0.81 0.56
Milrinone(US: Primacor® – discontinued)
0.29 0.95 70 0.28 3.3 0.98
Enoximone(EU: Perfan® - increased mortality)
1.88.9
(Cmax)85
1.3
(Cmax)4.9 0.72
CPD X(terminated)
0.280.722
(Cmax)94
0.043
(Cmax)2.6 0.15
» Conclusion: For clinically significant PDE3 inhibition plasma concentrations just at the hPDE3 IC50 are sufficient.
» Target coverage of marketed drugs can be used to interpret PK/PD of off-target-specific effects
• Consider (pharmacological) plasma concentrations (Cmax) of drug candidates showing SPECIFIC off-target activity at 1° target of marketed drugs.
Indicated for the short-term
intravenous treatment of patients
with acute decompensated heart
failure (inotropic vasodilator).

(Off-)target coverageExample using marketed PDE3 inhibitors
CPD X dog
Dog, upon single dose:
• Inotropic effect (LVEF ↑)
• Chronotropic effect (HR ↑)
• Endocardial hemorrhage

Recommended activity flowchart for off-target
mitigation and management
THR < 30%
Metabolites > 10%
abundance of parent
Cold Met-ID (MAP) Plasma protein binding
(rodent, NON-RODENT, human)
kinase panel
(for kinase inhibitors
only)Full panel & hERG
FOR METABOLITES
hERG RLB
Primary panel
CANDIDATE DeclarationPrimary panel
ADME assays
Select panel
Lead Nomination
SELECTIVITY determination
Series-specific risk assessmt.
(refer to decision strat. flow chart
& Profiling Wiki)COVERAGE determination
(refer to decision strat. flow chart)
SAFETY INDEX
assessment
(based on in vivo tox / safety
pharmacology studies)
Green lines depict "yes", red lines depict "no"; Diamonds: decisions; Boxes: activities
#1: special request for assay in case off-target only in Full panel
Chemical series
(Risk mitigation)Single molecule
(Risk management)
SAR-based off-target
mitigation
"Candidate Selection"
Full panel
ADME assays

Example of early assessment and mitigation: The chemistry viewCorrelation of target LipE with major off-target activities
High LipE predicts for favorable hERG, solubility and DDI profile
Bottom 8 (LipE <5)
100% hERG active
75% insoluble
50% CYP3A4 active
Top 8 (LipE >8)
38% hERG active
0% insoluble
0% CYP3A4 active
Middle 13 (LipE 5-8)
77% hERG active
15% insoluble
23% CYP3A4 active
Target LipE

Chemistry considerations for successful mitigation
To improve chances of success and speed of lead optimization, focus on PROPERTIES of leads and add potency EFFICIENTLY
Be proactive in selecting quality – potency is the easiest thing to improve!
Hypothesis driven reduction of liabilities must include increased emphasis on physicochemical relationships
Potency, permeability and metabolic stability all correlated to physicochemical properties
Don’t improve solubility by adding a basic amine that has hERGaffinity - which has to be made less basic and then
increases metabolism,
reduces permeability,
decreases oral exposure,
increases molecular weight
results in metabolite issues that
requires EXHAUSTIVE preclinical profiling resource

Critical evaluation of early ADR
mitigation
• Technical considerations– Poorly optimized physicochemical properties, HT automation
might compromise data quality
– Exposure is not adequate
• Tactical considerations– Single target vs. pathway considerations
– Preference of management vs. mitigation
– Ignorance of integrative assessment
• Strategic considerations– Drug repositioning requires safety assessment adjusted to the
new indication
– Interpretation of complex data could lead to wrong conclusions
– Overestimation of predictive value – importance of follow-ups

Conclusions
• Early integrated risk assessment supports mitigation of
predicted clinical toxicities, ADRs
• Correct prediction depends on the knowledge of the
target associated with an ADR and the calculated TI
• Knowledge of the chemical structural and biological
target environment enables the development of in silico
technologies to support safety assessment
• Risk/Benefit evaluation is essential for clinical candidate
selection when off-target liabilities persist
• Medicinal chemistry can drive off-target mitigation by
linking physicochemical features or off-target SAR with
biological performance

Literature and links
Whitebread S, Hamon J, Bojanic D, Urban L (2005) In vitro Safety Pharmacology profiling: An
essential Tool for Drug Development. Drug Discovery Today; 10(21):1421-1433.
http://dx.doi.org/10.1016/S1359-6446(05)03632-9
Hamon J, Whitebread S (2009) In vitro safety pharmacology profiling: An important Tool to Decrease
Attrition. In: Faller B, Urban L (eds). Hit and Lead Profiling. Weinheim: Wiley VCH, p. 273-295.
http://share.nibr.novartis.intra/cpc/psp/Shared%20Documents/Literature/Hamon%20and%20Whitebre
ad%202009%20book%20chapter%20in%20Hit%20and%20Lead%20Profiling.PDF
Hamon J, Whitebread S, Techer-Etienne V, Le Coq H, Azzaoui K, Urban L (2009) In vitro safety
pharmacology profiling: What else beyond hERG? Future Med Chem; 1(4):645-665.
http://www.future-science.com/doi/full/10.4155/fmc.09.51. Erratum in: http://www.future-
science.com/doi/full/10.4155/fmc.09.128
Scheiber J, Jenkins JL, Sukuru SC, Bender A, Mikhailov D, Milik M, Azzaoui K, Whitebread S,
Hamon J, Urban L, Glick M, Davies JW (2009) Mapping Adverse Drug Reactions in Chemical
Space. J Med Chem; 52(9):3103-3107. http://dx.doi.org/10.1021/jm801546k
Azzaoui K, Hamon J, Faller B, Whitebread S, Jacoby E, Bender A, Jenkins J, Urban L (2007)
Modeling Promiscuity Based on in vitro Safety Pharmacology Profiling Data. ChemMedChem; 2(6):
874-880. http://dx.doi.org/10.1002/cmdc.200700036
Bender A, Jenkins J, Glick M, Davies J, Azzaoui K, Hamon J, Urban L, Whitebread S (2007)
Analysis of Pharmacology Data and the Prediction of Adverse Drug Reactions and Off-Target Effect
From Chemical Structure. ChemMedChem; 2(6): 861-873. http://dx.doi.org/10.1002/cmdc.200700026
28 | Off-Target Workshop | 2011 | Business Use Only

Steven Whitebread Dejan Bojanic
Jacques Hamon Michael Shultz
Dmitri Mikhailov Bob Pearlstein
Gul Erdemli Clayton Springer
Dejan Bojanic Bill Kluwe
Patrick Mueller PeterK Hoffmann
Doriano Fabbro
Kamal Azzaoui
Sepp Scheiber
Jeremy Jenkins
Acknowledgement