Early intrauterine development of mixed giant … · Early intrauterine development of mixed giant...
6
Rom J Morphol Embryol 2015, 56(2 Suppl):851–856 ISSN (print) 1220–0522 ISSN (on-line) 2066–8279 CASE REPORT Early intrauterine development of mixed giant intracranial teratoma in newborn: a case report LUMINIŢA PĂDURARU 1,2) , DANIELA CLAUDIA SCRIPCARU 3) , GABRIELA-ILDIKO ZONDA 1,2) , ANDREEA-LUCIANA AVASILOAIEI 1,2) , MARIA STAMATIN 1,2) 1) Department of Mother and Child Medicine, Division of Neonatology, “Grigore T. Popa” University of Medicine and Pharmacy, Iassy, Romania 2) Regional Center of Neonatal Intensive Care Level III, “Cuza Vodă” Clinical Hospital of Obstetrics and Gynecology, Iassy, Romania 3) Department of Pathology, “Cuza Vodă” Clinical Hospital of Obstetrics and Gynecology, Iassy, Romania Abstract Teratoma is one of the most frequent fetal intracranial tumors, but it usually grows very quickly and the fetus is generally a stillborn. Rare cases have slow development or are located in areas that afford immediate surgery after birth with variable chances of survival. Even more rare cases survive days or weeks, but with no chance of surgical treatment and with prolonged palliative care. We present a 34 weeks premature infant, born by C-section with a giant intracranial tumor, whose origin could not be ascertained, occupied almost all-intracranial space and survived 25 days with supportive care. The histological examination established a G3 mixed teratoma, predominantly with immature cells from all three embryonic layers. The cerebellum was normal and infra-mesencephalic structures were present. The infant presented with severe anemia and mild respiratory distress, and was out of neurosurgical therapeutic resources. Antenatal examination was normal until 30 weeks, when fetal ultrasound described a degree of hydrocephalus, but no tumor was individualized. Conclusions: G3 type complex teratoma, even rare, can be localized at cerebral level and get giant development and growth only in the third trimester of pregnancy, ending with a neonate that has no chance of survival. Such cases cannot benefit of therapeutic interruption of pregnancy and generate serious difficulties for parents and clinicians. Keywords: teratoma, newborn, giant cranial tumor. Introduction As germ cell tumors, teratomas are comprised of cells originating from at least two and usually all three embryonic layers: ectoderm, mesoderm and endoderm. Intracranial localization is rare and unusual. However, they represent the majority of fetal intracranial tumors (26–50%). They may be divided in two main categories: intra and extra-axial, which differ in epidemiology and clinical presentation. Intra-axial tumors, located within the cerebral hemispheres, appear either during pregnancy or in the neonatal period. They present as large tumors that increase head circumference and more commonly occur in the supratentorial area. Extra-axial teratomas usually appear during childhood or early adulthood and are typically smaller. They usually arise in the pineal or suprasellar regions, and may generate obstructive hydrocephalus due to impingement on the mid brain. From the histological point of view, according to the WHO (World Health Organization) classification of intra- cranial tumors, germ cell tumors (GCTs) are categorized into germinomas and non-germinomatous germ cell tumors (NGGCTs). The latter include teratoma (classified into mature, immature and teratoma with malignant trans- formation), embryonal carcinoma, yolk sac tumor, chorio- carcinoma and mixed germ cell tumors [1]. Immature teratomas in children are rare (16%) and they are mostly grade 3 (G3), mainly with ovarian localization [2]. From primary pediatric central nervous system tumors statistic done on 763 cases in China, studies concluded a predo- minance for male gender (male/female ratio 4.67:1) [3]. We report a rare case of giant intracranial tumor developed in mid intrauterine life, with rapid development and cerebral atrophy, in a case of 34 weeks gestational age (GA) premature infant that survived 25 days and was associated with severe anemia at birth. Case report The infant was born by C-section at 34 weeks GA, after 11 hours of ruptured membranes, in our Level III Clinical Hospital of Obstetrics and Gynecology, with an Apgar score of 6-6-6-6 at 1-5-10-20 minutes. Pre-ductal SpO 2 (saturation of peripheral oxygen) was in normal ranges after birth and in the next hours and days, with oxygen supplementation in hood. Weight was 3500 g, length of 46 cm, thoracic perimeter 26 cm, cranial peri- meter (CP) 50 cm (with giant CP for his length and GA, far higher than 97 percentile). Blood type and Rh were AII positive. Mother, 23-year-old, homemaker, is married to a 24- year-old husband. No pathological medical conditions were declared or identified for the parents. Mother was II gesta, I para, AII positive and the gestation was uneventful until 30 weeks, when at an ultrasound examination for bio- physical profile, the obstetrician described an intracranial tumoral structure and hydrocephalus. Previous ultrasounds performed at 19 and 24 weeks gestation were normal. A R J M E Romanian Journal of Morphology & Embryology http://www.rjme.ro/
-
Upload
hoangkhuong -
Category
Documents
-
view
219 -
download
0
Transcript of Early intrauterine development of mixed giant … · Early intrauterine development of mixed giant...
![Page 1: Early intrauterine development of mixed giant … · Early intrauterine development of mixed giant ... but with intrauterine death at 29 weeks [5]. Fetal . Early intrauterine development](https://reader040.fdocuments.in/reader040/viewer/2022021900/5b63022f7f8b9ade588b8aac/html5/page/1.jpg)
Rom J Morphol Embryol 2015, 56(2 Suppl):851–856
ISSN (print) 1220–0522 ISSN (on-line) 2066–8279
CCAASSEE RREEPPOORRTT
Early intrauterine development of mixed giant intracranial teratoma in newborn: a case report
LUMINIŢA PĂDURARU1,2), DANIELA CLAUDIA SCRIPCARU3), GABRIELA-ILDIKO ZONDA1,2), ANDREEA-LUCIANA AVASILOAIEI1,2), MARIA STAMATIN1,2)
1)Department of Mother and Child Medicine, Division of Neonatology, “Grigore T. Popa” University of Medicine and Pharmacy, Iassy, Romania
2)Regional Center of Neonatal Intensive Care Level III, “Cuza Vodă” Clinical Hospital of Obstetrics and Gynecology, Iassy, Romania
3)Department of Pathology, “Cuza Vodă” Clinical Hospital of Obstetrics and Gynecology, Iassy, Romania
Abstract Teratoma is one of the most frequent fetal intracranial tumors, but it usually grows very quickly and the fetus is generally a stillborn. Rare cases have slow development or are located in areas that afford immediate surgery after birth with variable chances of survival. Even more rare cases survive days or weeks, but with no chance of surgical treatment and with prolonged palliative care. We present a 34 weeks premature infant, born by C-section with a giant intracranial tumor, whose origin could not be ascertained, occupied almost all-intracranial space and survived 25 days with supportive care. The histological examination established a G3 mixed teratoma, predominantly with immature cells from all three embryonic layers. The cerebellum was normal and infra-mesencephalic structures were present. The infant presented with severe anemia and mild respiratory distress, and was out of neurosurgical therapeutic resources. Antenatal examination was normal until 30 weeks, when fetal ultrasound described a degree of hydrocephalus, but no tumor was individualized. Conclusions: G3 type complex teratoma, even rare, can be localized at cerebral level and get giant development and growth only in the third trimester of pregnancy, ending with a neonate that has no chance of survival. Such cases cannot benefit of therapeutic interruption of pregnancy and generate serious difficulties for parents and clinicians.
Keywords: teratoma, newborn, giant cranial tumor.
Introduction
As germ cell tumors, teratomas are comprised of cells originating from at least two and usually all three embryonic layers: ectoderm, mesoderm and endoderm. Intracranial localization is rare and unusual. However, they represent the majority of fetal intracranial tumors (26–50%). They may be divided in two main categories: intra and extra-axial, which differ in epidemiology and clinical presentation. Intra-axial tumors, located within the cerebral hemispheres, appear either during pregnancy or in the neonatal period. They present as large tumors that increase head circumference and more commonly occur in the supratentorial area. Extra-axial teratomas usually appear during childhood or early adulthood and are typically smaller. They usually arise in the pineal or suprasellar regions, and may generate obstructive hydrocephalus due to impingement on the mid brain.
From the histological point of view, according to the WHO (World Health Organization) classification of intra-cranial tumors, germ cell tumors (GCTs) are categorized into germinomas and non-germinomatous germ cell tumors (NGGCTs). The latter include teratoma (classified into mature, immature and teratoma with malignant trans-formation), embryonal carcinoma, yolk sac tumor, chorio-carcinoma and mixed germ cell tumors [1]. Immature teratomas in children are rare (16%) and they are mostly grade 3 (G3), mainly with ovarian localization [2]. From primary pediatric central nervous system tumors statistic
done on 763 cases in China, studies concluded a predo-minance for male gender (male/female ratio 4.67:1) [3].
We report a rare case of giant intracranial tumor developed in mid intrauterine life, with rapid development and cerebral atrophy, in a case of 34 weeks gestational age (GA) premature infant that survived 25 days and was associated with severe anemia at birth.
Case report
The infant was born by C-section at 34 weeks GA, after 11 hours of ruptured membranes, in our Level III Clinical Hospital of Obstetrics and Gynecology, with an Apgar score of 6-6-6-6 at 1-5-10-20 minutes. Pre-ductal SpO2 (saturation of peripheral oxygen) was in normal ranges after birth and in the next hours and days, with oxygen supplementation in hood. Weight was 3500 g, length of 46 cm, thoracic perimeter 26 cm, cranial peri-meter (CP) 50 cm (with giant CP for his length and GA, far higher than 97 percentile). Blood type and Rh were AII positive.
Mother, 23-year-old, homemaker, is married to a 24-year-old husband. No pathological medical conditions were declared or identified for the parents. Mother was II gesta, I para, AII positive and the gestation was uneventful until 30 weeks, when at an ultrasound examination for bio-physical profile, the obstetrician described an intracranial tumoral structure and hydrocephalus. Previous ultrasounds performed at 19 and 24 weeks gestation were normal. A
R J M ERomanian Journal of
Morphology & Embryologyhttp://www.rjme.ro/
![Page 2: Early intrauterine development of mixed giant … · Early intrauterine development of mixed giant ... but with intrauterine death at 29 weeks [5]. Fetal . Early intrauterine development](https://reader040.fdocuments.in/reader040/viewer/2022021900/5b63022f7f8b9ade588b8aac/html5/page/2.jpg)
Luminiţa Păduraru et al.
852
previous pregnancy was finalized with elective abortion at 21 years. No history of teratogenic agents during pregnancy, or family history of congenital malformations was identified.
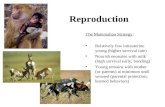
Clinical examination described a giant head with a small viscerocranium and enlarged neurocranium (Figures 1 and 2), fragile, incompletely developed head bones and enlarged sutures and fontanelles, moldering parietal-occipital area. The skin was pale and fragile; the abdomen was enlarged, with hepatomegaly. The infant presented with mild tachypnea at 55 breaths/min., hypotonia and moderate reactivity.
Figure 1 – 34 weeks GA newborn with
macrocrania; CP=50 cm.
Figure 2 – 34 weeks GA newborn with huge head,
small viscerocranium and large neurocranium,
enlarged sutures and fontanelles, moldering parietal-occipital area.
Immediately after the transfer to the neonatal intensive care unit (NICU), the infant received three cell pack transfusions for anemia (pale skin and a Hb of 5.6 g/dL with a Ht of 17.4%), that raised the Hb at 11.8 g/dL and the Ht at 36% in 16 hours. Parenteral nutrition and oxygen supplementation in hood with 5 L/min. were given.
In the meanwhile, several imagistic and functional investigations were performed:
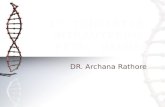
Transfontanellar ultrasound described giant atypical non-cerebral structures, with mixed areas of hyperlucency and cystic appearance hypoechogenic structures that inva-ded all intracranial space, and slight narrow area of cerebral structure compressed in the basal area, but with rudimental structure (Figures 3 and 4). Doppler signal was present, proving vascularization. Median line structures and ventri-cular system were absent (Figure 5). Cerebellar structures were present (Figure 6).
Computer cranial tomography ascertained the total absence of normal cerebral structures, displaced by an amorphous tumoral tissue mass, totally non-homogenous, with areas of smooth tissue, small areas of cerebrospinal fluid cysts, round and linear areas of calcifications (Figure 7), alternating with imprecisely delimitated hyper-dense areas that herniate outside the cranial space with approximately 4.2 cm in the posterior-occipital left side (Figure 8). Very hypoplastic, undifferentiated cerebellar structures were described (Figure 9).
Figure 3 – Transfontanellar ultrasound: mixed areas of transonic cystic appearance and hypoechogenic struc-tures invading all intracranial space.
Figure 4 – Transfontanellar ultrasound: giant tumor structure with slight narrow area of cerebral tissue compressed in the basal area.
Figure 5 – Transfontanellar ultrasound: median line structures and ventricular system could not be identified.
Figure 6 – Transfontanellar ultrasound: cerebellum present with normal diameter for gestational age.
![Page 3: Early intrauterine development of mixed giant … · Early intrauterine development of mixed giant ... but with intrauterine death at 29 weeks [5]. Fetal . Early intrauterine development](https://reader040.fdocuments.in/reader040/viewer/2022021900/5b63022f7f8b9ade588b8aac/html5/page/3.jpg)
Early intrauterine development of mixed giant intracranial teratoma in newborn: a case report
853
Figure 7 – CT scan: total absence of normal cerebral structures and amorphous tumoral tissue mass; small areas of cephalorachidian liquid cysts and calcifications.
Figure 8 – CT scan: same huge tumor in sagittal section with areas of smooth tissue in a tumoral mass imprecisely delimitated and partial herniation.
Figure 9 – CT scan: hypoplastic cerebellar structure with undiffer-entiated pattern.
Neurosurgical examination concluded that the case is outside the therapeutic possibilities, with no chances of survival.
At that moment, the decision of discontinuing intensive care was taken, after informing the parents about the infant’s severe outcome.
Clinical and paraclinical data revealed severe jaundice from day 4, initially with indirect bilirubin (152 mg/L from a total of 160 mg/L), and progressively, until day 24 with elevated direct bilirubin (192 mg/L from a total of 218 mg/L). Constantly, the infant presented with hypo-proteinemia and elevated liver enzymes. TORCH (toxo-plasmosis, other agents, rubella, cytomegalovirus, herpes simplex) investigation was negative.
No infection was detected by biochemical and bacterio-logical routine tests. Progressive intracranial hypertension developed, with an increase of the cranial circumference of 4 cm.
After 25 days of thermal comfort, oxygen supplemen-tation in hood and lately free flow, antibiotic prophylaxis with Ampicillin for seven days, intravenous Fentanyl in continuous perfusion for pain relief, parenteral nutrition for eight days and progressive initiation of enteral feedings by gavage, a fatal severe episode of apnea occurred.
Macroscopic examination described a giant tumor (approximately diameter 15 cm and 1.45 kg) with semi-solid consistency, areas of necrosis and hemorrhage,
areas of microcystic pattern (Figure 10). A small island of rudimental cerebral tissue was observed in left parietal margin. No supratentorial middle structures were identified (Figure 11). The tumor was partially herniated between the parietal and occipital rudimental head bones, in the area of an enlarged posterior fontanelle (Figure 12). The cerebellum was present, with normal appearance and size according with gestational age (Figure 13).
The histological examination detected a giant teratoma with very small islands of rudimental cerebral tissue, with mature and immature structures, suggestive for G3 type. For histological study, classical stains of Hematoxylin–Eosin (HE) were used. There were predominant immature embryonal tissues (neuroectodermal annulus and tubes included in glial tissue) (Figure 14), immature mesen-chymal tissue with mixoid patency, and immature carti-laginous focal differentiation, osteoid, immature endo-dermal structures, such as intestinal epithelium (Figure 15), hepatic (Figure 16) striated muscle and nerve (Figure 17) and renal tissue. The mature types structures identified were: squamous epithelium, retinal epithelium, hyaline cartilage (Figure 18), muscular tissue and multiple small plexus choroid cysts. There were also large and extended areas of hemorrhage and tumor necrosis. Liver structures presented with biliary thrombi, brown, granular intra-cellular pigment in Kupffer cells, focal erythropoiesis areas.
Figure 10 – Giant tumor with semi-solid consistency, areas of micro-cystic pattern, hemorrhage and necrosis.
Figure 11 – Island of rudimental cerebral tissue, but no supraten-torial middle structures; amorphous tumoral mass.
Figure 12 – Tumor herniation through the posterior fontanelle.
![Page 4: Early intrauterine development of mixed giant … · Early intrauterine development of mixed giant ... but with intrauterine death at 29 weeks [5]. Fetal . Early intrauterine development](https://reader040.fdocuments.in/reader040/viewer/2022021900/5b63022f7f8b9ade588b8aac/html5/page/4.jpg)
Luminiţa Păduraru et al.
854
Figure 13 – Cerebellum with normal appearance and size.
Figure 14 – Immature and mature cartilage, choroid plexus cysts, squamous epithelium with an immature glial tissue background (HE staining, ×40).
Figure 15 – Immature intestinal epithelium (HE staining, ×200).
Figure 16 – Immature hepatic tissue (HE staining, ×200).
Figure 17 – Striated muscle and nerve (HE staining, ×100).
Figure 18 – Mature and immature hyaline cartilage (HE staining, ×200).
Discussion
According to Cassart et al. [4] congenital intracranial teratomas represent around 0.5% to 1.9% of all pediatric tumors. The mean gestational age at intrauterine diag-
nostic, if done, is 27 weeks gestation. Standard views of the fetal head at the time of an anatomy scan do not rule out this aggressive tumor, as presented in recent case presentation with a very similar teratoma to the one we present, but with intrauterine death at 29 weeks [5]. Fetal
![Page 5: Early intrauterine development of mixed giant … · Early intrauterine development of mixed giant ... but with intrauterine death at 29 weeks [5]. Fetal . Early intrauterine development](https://reader040.fdocuments.in/reader040/viewer/2022021900/5b63022f7f8b9ade588b8aac/html5/page/5.jpg)
Early intrauterine development of mixed giant intracranial teratoma in newborn: a case report
855
ultrasound examination may detect the majority of tumors, but later in intrauterine life, and even so, the rapid growth of such teratomas does not allow for the indication of deliberated interruption of pregnancy. Magnetic resonance imaging (MRI) is very accurate in illustrating the mor-phologic features of this tumor, and may be more helpful in early stages for better decision-making [6]. As expected, fetuses with intracranial teratomas have the worst prog-nosis, and no child with such a lesion has survived [7–9], despite postnatal tempted neurosurgical intervention for ablation and ventriculoperitoneal shunt [10, 11]. Our case survival for 25 days could be explained by the presence of respiratory and cardiovascular centers from rudimental central nervous structures. As in many cases published in the literature [12–15], we could not identify the origin of this tumor, although it would be for scientific benefit. They typically arise in the midline, predominantly from the pineal gland, but not always, and involve the third ventricle [16]. Comparing with intracranial teratomas that develop later in childhood, fetal intracranial teratomas associate polyhydramnios, are the most common fetal brain tumor and have a worse outcome [17].
In an extensive review on 45 cases of brain neonatal tumors, Buetow et al. showed that in teratomas coarse calcification was a constant feature [18]. Our case pre-sented also with some calcifications.
Perinatal intracranial teratomas contain mature and immature tissues but lack malignant germ cell tumor components [19]. Cytogenetically, the karyotype of tera-tomas is identical to the host [20]. Alpha-fetoprotein dosing was proved to have significant correlation with detection and development of intracranial teratoma [6, 7, 10, 21]. Most intracranial teratomas are isolated diseases [22, 23], like our case, lacking associated anomalies, although some intracranial teratomas are associated with pulmonary hypoplasia [24] or high output cardiac failure [25].
A giant teratoma with poor vital prognosis and fatal outcome represents a high challenge for clinicians, as prolonged sufferance is frustrating for both parents and professionals. Ethical aspects are to be considered, similar to the situation of anencephalic cases that survives several days, even weeks, despite providing only basic care.
More research would be useful to identify immuno-histochemical, serological or genetic markers for early development or predisposition of rapid growth complex teratoma, to allow development of a clinical protocol for detecting this in the first trimester and to proceed to a therapeutic interruption of pregnancy. The recurrence risk is not yet well established, as genetic predisposition was not demonstrated. Thus, genetic advice is not available, although it would be useful.
Conclusions
G3 type complex teratoma, even if rare, can be localized at the cerebral level and get huge development and growth only in the third trimester of pregnancy, ending with a neonate that has no chance of survival. Such cases cannot benefit of therapeutic interruption of pregnancy and generates serious difficulties for parents and clinicians. Early intrauterine detection by ultrasound and, if necessary, even MRI, could prevent the birth of such newborns and
their survival with no quality of temporary life. More research to identify a significant marker to detect the development of such tumor is necessary.
Conflict of interests The authors declare that they have no conflict of
interests.
References [1] Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC,
Jouvet A, Scheithauer BW, Kleihues P. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol, 2007, 114(2):97–109.
[2] Heifetz SA, Cushing B, Giller R, Shuster JJ, Stolar CJ, Vinocur CD, Hawkins EP. Immature teratomas in children: pathologic considerations: a report from the combined Pediatric Oncology Group/Children’s Cancer Group. Am J Surg Pathol, 1998, 22(9):1115–1124.
[3] Zhang R, Shen WQ, Zhou LF. Primary pediatric central nervous system tumors statistic: study of 763 cases in a single institution. Zhonghua Yi Xue Za Zhi, 2007, 87(7):442–447.
[4] Cassart M, Bosson N, Garel C, Eurin D, Avni F. Fetal intra-cranial tumors: a review of 27 cases. Eur Radiol, 2008, 18(10):2060–2066.
[5] Khan Z, Watson WJ. Congenital intracranial teratoma. J Ultra-sound Med, 2010, 29(7):1147–1149.
[6] Mazouni C, Porcu-Buisson G, Girard N, Sakr R, Figarella-Ballanger D, Guidicelli B, Bonnier P, Gamerre M. Intrauterine brain teratoma: a case report of imaging (US, MRI) with neuro-pathologic correlations. Prenat Diagn, 2003, 23(2):104–107.
[7] Kamil D, Tepelmann J, Berg C, Heep A, Axt-Fliedner R, Gembruch U, Geipel A. Spectrum and outcome of prenatally diagnosed fetal tumors. Ultrasound Obstet Gynecol, 2008, 31(3):296–302.
[8] Isaacs H Jr. I. Perinatal brain tumors: a review of 250 cases. Pediatr Neurol, 2002, 27(4):249–261.
[9] Thakran A, Rao S, Sreenivas M, Khurana N. Massive con-genital intracranial immature teratoma: an autopsy report. Indian J Pathol Microbiol, 2012, 55(2):272–274.
[10] Sandow BA, Dory CE, Aguiar MA, Abuhamad AZ. Best cases from the AFIP: congenital intracranial teratoma. Radiogra-phics, 2004, 24(4):1165–1170.
[11] Thust SC, Nandi D, Hann G. Acting on macrocephaly in the neonatal period: an illustrative case of congenital teratoma. BMJ Case Rep, 2014, Jan 16.
[12] Canan A, Gülsevin T, Nejat A, Tezer K, Sule Y, Meryem T, Gülşen E. Neonatal intracranial teratoma. Brain Dev, 2000, 22(5):340–342.
[13] Schlembach D, Bornemann A, Rupprecht T, Beinder E. Fetal intracranial tumors detected by ultrasound: a report of two cases and review of the literature. Ultrasound Obstet Gynecol, 1999, 14(6):407–418.
[14] Yilmaz E, Zümrütbaş N, Korucuoğlu Ü, Bozkurt N, Efetürk T, Biri A. Fetal intracranial tumor with antenatal diagnosis. Peri-natal Journal, 2008, 16(1):36–39.
[15] Atalar M, Güner A, Çetin A. Prenatal and postmortem imaging findings of fetal intracranial teratoma. Cumhuriyet Med J, 2009, 31(1):66–70.
[16] Rickert CH. Neuropathology and prognosis of foetal brain tumours. Acta Neuropathol, 1999, 98(6):567–576.
[17] Woodward PJ, Sohaey R, Kennedy A, Koeller KK. From the archives of the AFIP: a comprehensive review of fetal tumors with pathologic correlation. Radiographics, 2005, 25(1):215–242.
[18] Buetow PC, Smirniotopoulos JG, Done S. Congenital brain tumors: a review of 45 cases. AJR Am J Roentgenol, 1990, 155(3):587–593.
[19] Işik N, Sìlav G, Güçlüer B, Elmaci I. Diagnosis and mana-gement of the congenital cranial teratomas: report of four cases and review. J Neurol Sci (Turk), 2012, 29(4):877–890.
[20] Bhattacharya B, Cochran E, Loew J. Pathologic quiz case: a 27-week female fetus with massive macrocephaly and generalized anasarca. Congenital immature intracranial tera-toma with skull rupture and high output cardiac failure. Arch Pathol Lab Med, 2004, 128(1):102–104.
![Page 6: Early intrauterine development of mixed giant … · Early intrauterine development of mixed giant ... but with intrauterine death at 29 weeks [5]. Fetal . Early intrauterine development](https://reader040.fdocuments.in/reader040/viewer/2022021900/5b63022f7f8b9ade588b8aac/html5/page/6.jpg)
Luminiţa Păduraru et al.
856
[21] Tsutsumi S, Kondo A, Yasumoto Y, Ito M. Rapid growth of congenital diffuse brain tumor considered to be teratoma: case report. Neurol Med Chir (Tokyo), 2008, 48(7):322–325.
[22] Chien YH, Tsao PN, Lee WT, Peng SF, Yau KI. Congenital intracranial teratoma. Pediatr Neurol, 2000, 22(1):72–74.
[23] Pinto V, Meo F, Loiudice L, D’Addario V. Prenatal sono-graphic imaging of an immature intracranial teratoma. Fetal Diagn Ther, 1999, 14(4):220–222.
[24] Sherer DM, Abramowicz JS, Eggers PC, Metlay LA, Sinkin RA, Woods JR Jr. Prenatal ultrasonographic diagnosis of intra-cranial teratoma and massive craniomegaly with associated high-output cardiac failure. Am J Obstet Gynecol, 1993, 168(1 Pt 1):97–99.
[25] Weyerts LK, Catanzarite V, Jones MC, Mendoza A. Prenatal diagnosis of a giant intracranial teratoma associated with pulmonary hypoplasia. J Med Genet, 1993, 30(10):880–882.
Corresponding author Luminiţa Păduraru, Lecturer, MD, PhD, Department of Mother and Child Medicine, Division of Neonatology, “Grigore T. Popa” University of Medicine and Pharmacy, 16 Universităţii Street, 700115 Iassy, “Cuza Vodă” Clinical Hospital of Obstetrics and Gynecology, 34 Cuza Vodă Street, 700038 Iassy, Romania; Phones +40232–213 000, +40232–237 008, +40745–631 053, e-mail: [email protected] Received: January 30, 2015
Accepted: August 10, 2015