
Douglas, Guy, & Hart, 2009, Psychosis as a Risk Factor for Violence to Others - A Meta-Analysis
Upload
chelsey-onealCategory
view
218download
2
Early Intervention in Psychosis‘At Risk Mental States’
Cognitive Therapy for People at High-Risk of Developing Psychosis
Dr. Aoiffe Kilcommons Clinical PsychologistDr. Sophie Parker Clinical Psychologist

•Cognitive therapy main interventionCognitive therapy main intervention
•However it can be helpful to interweave However it can be helpful to interweave alternative interventionsalternative interventions
•Use of case management skills such as Use of case management skills such as assistance with housing, bills, assistance with housing, bills, negotiations with negotiations with college/employer/neighbours. college/employer/neighbours.
•Crisis intervention skills at times such as Crisis intervention skills at times such as becoming homeless, traumatic events becoming homeless, traumatic events etc. Encourage strategies to manage etc. Encourage strategies to manage these crises. these crises.
Framework of CT for ARMS

•Develop therapeutic relationshipDevelop therapeutic relationship
•AssessmentAssessment
•Establish shared problem listEstablish shared problem list
• Translate into ‘smart’ goalsTranslate into ‘smart’ goals
• FormulationFormulation
• Interventions derived from Interventions derived from formulationformulation
•Relapse preventionRelapse prevention
Intervention Process

Practical• Offer flexible appointments, time and venue Offer flexible appointments, time and venue • Rapid response to referralRapid response to referral• ConsistencyConsistency
Therapy• Socialise to cognitive model, focus on Socialise to cognitive model, focus on
distress distress • Success early in therapySuccess early in therapy• Problem orientatedProblem orientated• Collaborative, shared, prioritised, SMART Collaborative, shared, prioritised, SMART
goalsgoals• LanguageLanguage• Incorporate case management strategiesIncorporate case management strategies
Engagement

Common Themes in EDIE 1 Problem
Lists (French and
Morrison, 2003)•Anxiety - I’m going mad / identity
- Social anxiety- Worry & metacognition- PTSD
•Mood & activity- Boredom / depression / hopelessness / self-esteem- College/job/money
•Social Networks- Relationships – friends, family, partners- Loneliness / lack of confidant

• ““I am unhappy with where I live.”I am unhappy with where I live.”• ““I feel anxious and paranoid when I leave the I feel anxious and paranoid when I leave the
house.”house.”• ““I worry that people know what I’m thinking”.I worry that people know what I’m thinking”.• ““I feel depressed.”I feel depressed.”• ““I worry about people laughing at me when I go I worry about people laughing at me when I go
out.”out.”• ““I need to get a job.”I need to get a job.”• ““I want more money.”I want more money.”• ““I have difficulties expressing myself”. I have difficulties expressing myself”. • ““I want to know what is wrong with me.”I want to know what is wrong with me.”• ““I need a girlfriend.”I need a girlfriend.”
Problems

• When I go out, I would like to be able to distinguish with When I go out, I would like to be able to distinguish with more certainty if people are laughing at me or whether I more certainty if people are laughing at me or whether I just feel this is the case (reduce distress from 60% to just feel this is the case (reduce distress from 60% to 30%).30%).
• To begin to understand if what I am experiencing is the To begin to understand if what I am experiencing is the start of psychosis.start of psychosis.
• To find out what alternative accommodation is available To find out what alternative accommodation is available and contact various housing agencies in order to get on and contact various housing agencies in order to get on their waiting lists. their waiting lists.
• If I felt less anxious I would like to be able to leave the If I felt less anxious I would like to be able to leave the house and go to the local shops when I felt like it (and at house and go to the local shops when I felt like it (and at least 3 x a week).least 3 x a week).
Goals

•Formulation
•Normalisation
•Working with metacognitive beliefs
•Generating possibilities for intrusions
•Safety behaviours
•Selective attention
•Activity scheduling
•Relapse prevention
Intervention Strategies

•The formulation using the intrusions The formulation using the intrusions model (Morrison 2001) is developed model (Morrison 2001) is developed within sessions 1 & 2. within sessions 1 & 2.
•The aim is to help the person make The aim is to help the person make sense of their experiences in more sense of their experiences in more rational and less distressing ways rational and less distressing ways
•One aim of this process is also to One aim of this process is also to highlight occasions when their highlight occasions when their interpretations may not lead to interpretations may not lead to distress. distress.
Formulation

Morrison, A. P. (2001) The interpretation of intrusions in psychosis: An integrative cognitive approach to hallucinations and delusions. Behavioural and Cognitive Psychotherapy, 29, 257-276.
CT for ARMS: Morrison’s cognitive model of psychosis
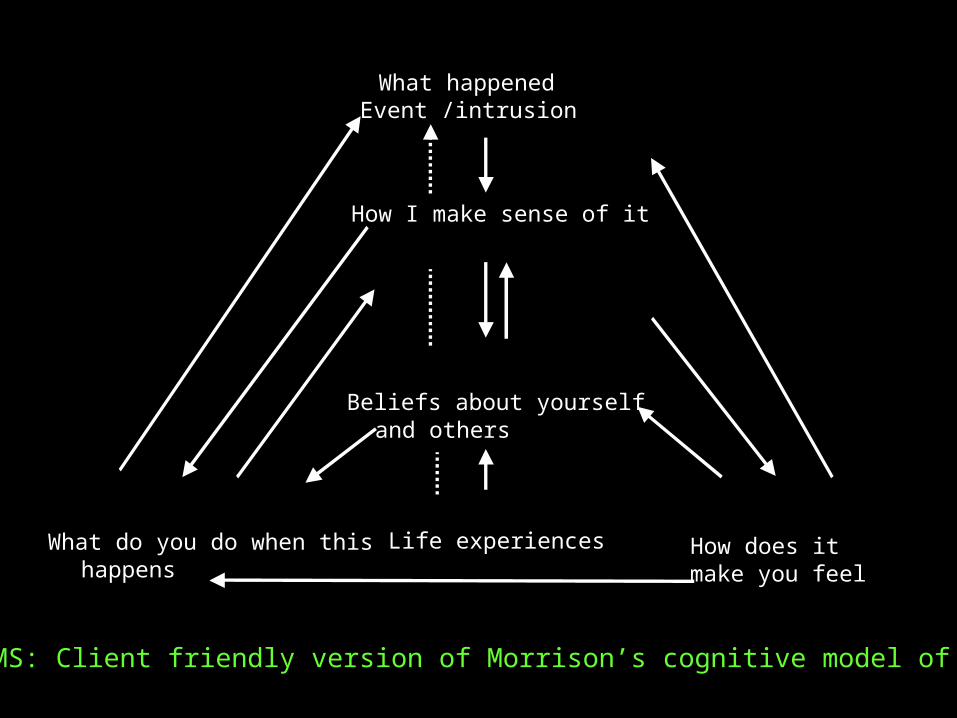
What happenedEvent /intrusion
How I make sense of it
Beliefs about yourselfand others
Life experiencesWhat do you do when thishappens
How does it make you feel
CT for ARMS: Client friendly version of Morrison’s cognitive model of psychosis
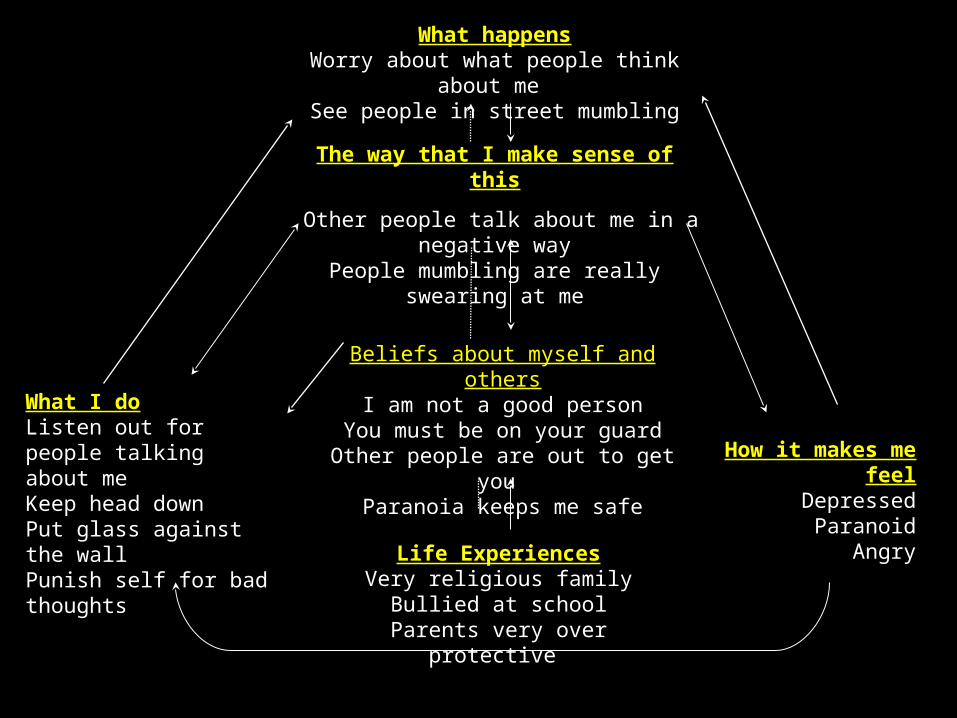
The way that I make sense of this
Other people talk about me in a negative wayPeople mumbling are really swearing at me
What happensWorry about what people think about me
See people in street mumbling
How it makes me feelDepressed
ParanoidAngry
What I doListen out for people talking about meKeep head downPut glass against the wallPunish self for bad thoughts
Beliefs about myself and othersI am not a good person
You must be on your guardOther people are out to get you
Paranoia keeps me safe
Life ExperiencesVery religious family
Bullied at schoolParents very over protective

What I make of itI must be going mad
I must not let other people see I am going madWhen mum is drunk she tells me I am going mad
What happensHear whispering and laughing
See bodiesThink about harming people
How it makes me feelAngry
AgitatedAnxious
DepressedFear
What I doTry to stay in total control of thoughts and behavioursLook out for things happening to me
How do you understand yourself and others?
I should be in total controlI am going mad
The symptoms I am experiencing mean I am going mad
Life ExperiencesHave always been interested I what
happens in a psychiatric ward

What happenedGoing out in public
Day dreaming on the bus
What I make of it
Other people people know what I’m thinking
Beliefs about myself and othersI’m odd, weird
Worrying helps me copeI must be in control of my thoughts at all times People will look down on me for showing anxiety
Experience Lonely childhood.
Bullied. Parents separated age 10 years
What I doWatch out for people looking at me
and giving me strange looksWorry about it
How it makes me feel
uneasyinsecure paranoid

What I make of itThey’re watching me They’re out to get me
What happensI saw someone looking at me
How it makes me feelRacing heart, churning
stomach, sweating,Anxious, upset
What I doKeep my head down and don’t look at anyoneLeave the situation
How do you understand yourself and others?
I’m different from everyone else I’m weird
My father had mental illness so I might too
Life ExperiencesBullied at school
Father had mental illness problems

• This uses the existing body of work from This uses the existing body of work from Kingdon and Turkington (1994). Kingdon and Turkington (1994).
• Their strategy allows distress associated Their strategy allows distress associated with symptoms to be managed by with symptoms to be managed by normalising the experience. normalising the experience.
• In our strategy we use the same In our strategy we use the same approach but more in line with the approach but more in line with the intrusions model we utilise a paper by intrusions model we utilise a paper by Rachman and Silva discussing intrusive Rachman and Silva discussing intrusive thoughts. Thus moving towards a truly thoughts. Thus moving towards a truly normalising approach.normalising approach.
Normalisation

•The model of psychosis described The model of psychosis described directs treatment towards working directs treatment towards working with metacognition. with metacognition.
•Negative beliefs regarding the Negative beliefs regarding the appraisal of the voices as being appraisal of the voices as being dangerous or uncontrollable may dangerous or uncontrollable may give rise to transition to psychosis. give rise to transition to psychosis.
Metacognition

•As with clients who have established As with clients who have established psychotic symptoms generating psychotic symptoms generating possibilities for the psychotic experience possibilities for the psychotic experience can be extremely helpful in terms of can be extremely helpful in terms of assessment and also treatment. assessment and also treatment.
• The development of an exhaustive list is The development of an exhaustive list is essential, with belief ratings, and emotions essential, with belief ratings, and emotions generated associated with this belief. generated associated with this belief.
•Subsequently, work through each Subsequently, work through each possibility generating evidence for and possibility generating evidence for and against each. against each.
Generating Alternative Explanations
GENERATING ALTERNATIVE EXPLANATIONS
•Advantages / disadvantages
•Exhaustive range of possible explanations
Socratic dialogue Being creative
•Belief ratings for each (0-100%) with associated emotions
•Evidence for and against each one

ALTERNATIVE EXPLANATIONS: Case
Example • Situation: I have been seeing things like dead bodies or images of myself hung in my wardrobe
• Current explanation: I am going mad/ have a brain tumour
• Current mood associated with this belief: Frightened
Other explanations Belief rating
Associated Mood
God is punishing me for something I have done in a previous life
40 % Frightened
Ghosts 75 % Scared
Brain tumour 100 % Doesn’t bother me
Going mad 85 % Depends, okay or very frightened
Perhaps stress and Kate’s life
90 % Unsure

EVIDENCE FOR AND AGAINST: Case example
Belief to be examined I have a brain tumour
Associated Mood Doesn’t bother me
Belief rating 100%
Evidence for Evidence Against
• I am having lots of strange experiences.
• People with a brain tumour have strange experiences
• I have bad headaches at times
• People with brain tumours get progressively worse
• I have been getting better
• I have been learning to make sense of these experiences
• When I make sense of them they reduce and go away, this would not be the case if it was a brain tumour
• My headaches usually respond to paracetamol, which would have little effect on a tumour
Belief rating (re-rating)Alternative Thought
70%Maybe things are more related to stress which I suppose would also explain the headaches
Associated Mood More relaxed

Alternative Explanations: Case example
What happenedWalking through the supermarket
One way of Thinking
“Others can read my mind”
Things I do
• Look out for strange looks •Worry
Feelings
Insecure Paranoid
Another way of thinking
“Oh I’m being silly – it’s not happening”
Feelings
Reassured
Things I do
Carry on as normal
OR

•Safety behaviours in the maintenance of Safety behaviours in the maintenance of anxiety disorders have been extensively anxiety disorders have been extensively reviewed. reviewed.
• The model of psychosis presented here The model of psychosis presented here emphasises the idea of self and social emphasises the idea of self and social knowledge. Safety behaviours knowledge. Safety behaviours perpetuate faulty self and social perpetuate faulty self and social knowledge. knowledge.
•A full exploration of safety behaviours A full exploration of safety behaviours should be undertaken and these should should be undertaken and these should be highlighted and experiments be highlighted and experiments undertaken to test their utility for the undertaken to test their utility for the client. client.
Safety Behaviours

Examples of Safety Behaviours
Experience Interpretation
Safety Behaviour
Saw people laughing whilst out walking
People in the street are talking about me
To keep head down, walk fast and purposefully
Visual hallucinatory experience, seeing a man sat on a chair
I am going mad
Not look at the chair and get out of the room as quickly as possible
Shop keeper looking at me
They know I am going mad
Said very little (if I talk it will confirm I am going mad).
Visual hallucination of dead body on wardrobe
I am going mad/ losing control
Hide head under the cover

BEHAVIOURAL EXPERIMENT: Case example
Thought to be tested: When I feel anxious other people will notice my hands shaking and will think I’m weird and laugh at me.
Belief in thought: (0-100%) Before experiment: 100% After experiment: 40%
Experiment to test thought
Likely problems
Strategies to deal with problems
Expected outcome
Actual outcome
Alternative thought
Do usual (5 minutes), exaggerate (5 minutes), drop (5 minutes)
I will feel too scared to do what’s asked of me
Tell my self that this is worth a go, it’s only for 15 minutes
People will think I’m weird
I looked more anxious when I did my usual things
Maybe some things I do don’t help me

•This has been strongly implicated in This has been strongly implicated in our experience of working with this our experience of working with this client group. client group.
•Many clients have discussed this as Many clients have discussed this as a means of confirming their a means of confirming their experiences in conjunction with experiences in conjunction with safety behaviours as indicating they safety behaviours as indicating they are at risk of impending psychosis.are at risk of impending psychosis.
Selective Attention
• Frequently people are beginning to Frequently people are beginning to isolate themselves, reducing the isolate themselves, reducing the frequency and duration of contacts frequency and duration of contacts they have with people and this leads they have with people and this leads into further preoccupation with into further preoccupation with thoughts. thoughts.
•The use of activity scheduling can be The use of activity scheduling can be a valuable means of monitoring and a valuable means of monitoring and impacting upon activity levels. impacting upon activity levels.
Activity Scheduling

•Familiar cognitive interventions developing blueprint of therapy.
•This should be provided in a medium which is amenable to the person eg written or audio tape.
Staying Well

•To increase awareness in primary care To increase awareness in primary care services, secondary care services, services, secondary care services, voluntary sector, further education and voluntary sector, further education and the communitythe community
•To increase referrals through:To increase referrals through:
1. Training for potential referrers1. Training for potential referrers
2. Rapid response2. Rapid response
3. Flexible approach to client3. Flexible approach to client
4. Positive, user friendly service4. Positive, user friendly service
Our Approach


















