
eader in digital CPD healthcare professionals COVID-19 ...
8
SEPTEMBER 2021 I 1 Leader in digital CPD for Southern African healthcare professionals COVID-19 Earn 3 free CEUs © 2021 deNovo Medica Professor Wolfgang Preiser Professor and Head: Division of Medical Virology Department of Pathology, Faculty of Medicine and Health Sciences Stellenbosch University and NHLS Tygerberg COVID-19 vaccines: facts, myths and advances Learning objectives You will learn: • Factors that have enabled the rapid development of SARS-CoV-2 vaccines • The immune response to vaccination • The different types of SARS-CoV-2 vaccines and their constituent ingredients • Adverse events associated with commonly available SARS-CoV-2 vaccines. Introduction In primary care, clinicians and frontline healthcare professionals have to cope with a wide spectrum of views and concerns about COVID-19 vaccination. These concerns are often expressed as: ’The vaccine was developed too quickly to be safe’; ‘It’s all a plot by others to control us ordinary working folk’; ‘What about mercury, microchips and other toxic chemicals – we don’t know what’s in it!’ This review of COVID-19 vaccine-related facts has been prepared to help clinicians answer questions from their patients and reassure themselves of the latest facts, the situation in South Africa and clinical issues such as: what about vaccinating my HIV patients, newer trivalent vaccines (active against the original, beta and delta variants), and whether COVID-19 will become a seasonal disease or ‘a disease of the unvaccinated’, as suggested by Professor Anthony Fauci, well-known to South African clinicians for his work in HIV/AIDS and other immunodeficiency diseases. This report was made possible by an unrestricted educational grant from Cipla. The content of the report is independent of the sponsor. © iStock/1297769933 Reviewed by:
Transcript of eader in digital CPD healthcare professionals COVID-19 ...
SEPTEMBER 2021 I 1
Leader in digital CPD for Southern African healthcare professionals
COVID-19Earn 3 free CEUs
© 2021 deNovo Medica
Professor Wolfgang PreiserProfessor and Head: Division of Medical VirologyDepartment of Pathology, Faculty of Medicine and Health SciencesStellenbosch University and NHLS Tygerberg
COVID-19 vaccines: facts, myths and advances
Learning objectivesYou will learn:
• Factors that have enabled the rapid development of SARS-CoV-2 vaccines
• The immune response to vaccination
• The different types of SARS-CoV-2 vaccines and their constituent ingredients
• Adverse events associated with commonly available SARS-CoV-2 vaccines.
IntroductionIn primary care, clinicians and frontline healthcare professionals have to cope with a wide spectrum of views and concerns about COVID-19 vaccination. These concerns are often expressed as: ’The vaccine was developed too quickly to be safe’; ‘It’s all a plot by others to control us ordinary working folk’; ‘What about mercury, microchips and other toxic chemicals – we don’t know what’s in it!’
This review of COVID-19 vaccine-related facts has been prepared to help clinicians answer questions from their patients and reassure themselves of the latest facts, the situation in South Africa and clinical issues such as: what about vaccinating my HIV patients, newer trivalent vaccines (active against the original, beta and delta variants), and whether COVID-19 will become a seasonal disease or ‘a disease of the unvaccinated’, as suggested by Professor Anthony Fauci, well-known to South African clinicians for his work in HIV/AIDS and other immunodeficiency diseases.
This report was made possible by an unrestricted educational grant from Cipla. The content of the report is independent of the sponsor.
© iS
tock
/129
7769
933
Reviewed by:
2 I SEPTEMBER 2021
COVID-19 vaccines: facts, myths and advances
ISSUE: The vaccines were developed too fast, so they are not safe
The vaccines were developed quickly because vaccine platforms had been developed for a so-called ‘Disease X’, particularly in the United States, Oxford and Germany, initi-ated in 2017 by the Norway-based Coalition for Epidemic Preparedness and Innovation (CEPI) and the WHO.
Disease X was the name for an anticipated, future hypothetical viral disease. So there were experts, including John Nkengasong, from the Africa Centres for Disease Control and Prevention, grouped in an expert board, raising funds and calling for research propos-als to develop these vaccine platforms (www.cepi.net), particularly targeting Middle East Respiratory Syndrome (MERS), also a coro-navirus, and Lassa fever.
While SARS-CoV-2 was not specifically anticipated, the possibility of a dangerous emergent pathogen challenging our health
was. Researchers were therefore not taken entirely by surprise and already had an arma-mentarium, including vaccine-producing plat-forms, that could be tailored to the individual genetic components of the new SARS-CoV-2 virus. A lot of research on HIV and other vaccines also benefited SARS-CoV-2 vaccine development.
Generous funding by several governments allowed the testing and clinical trial phases to be expedited, sometimes overlapping (i.e. the next phase started before the previous one was completed). The extra funds avoided the stop-start, phase-by-phase approach typical of drug (and vaccine) development. Reassuringly, a number of SARS-CoV-2 vac-cines faltered and failed, as expected (https://www.nytimes.com/interactive/2020/science/coronavirus-vaccine-tracker.html). Candidate vaccines that made it proved to be efficacious and safe.
ISSUE: Which vaccine, which platform, which technology is best and safest?
All vaccines aim to safely elicit immunity against one or more specific viral antigens so that the immune system will recognise and render harmless the virus if a person becomes infected. Most currently approved SARS-CoV-2 vaccines are based on the virus’s spike protein, which is an important target of the immune response. The spike protein on its own does not cause COVID-19. The vacci-nated person’s immune system recognises the spike protein as foreign and produces anti-bodies and immune cells against it. Figure 1
depicts how immunity develops.1
There are three main types of COVID-19 vac-cine currently available:• Nucleic acid vaccines such as BioNTech/
Pfizer and Moderna (Figure 2)• Viral vector vaccines such as Johnson &
Johnson/Janssen and AstraZeneca (Figure 3)
• Inactivated whole-virus vaccines such as CoronaVac (Sinovac COVID-19 vaccine).
Nucleic acid vaccinesThese vaccines use genetic instructions, in the form of messenger RNA (mRNA) that encodes for a selected coronavirus protein. This prompts the temporary production of the protein by the vaccine recipient, which elicits an immune response. The mRNA is broken down shortly after vaccination.
The nucleic acid is taken up by the recipient’s cells, which then churn out copies of the virus protein; most available vaccines are based on the virus’s spike protein, which is an impor-tant target of the immune response. The spike protein does not cause COVID-19. The Pfizer/BioNTech and Moderna vaccines are based on mRNA technology.
There are currently no DNA vaccines widely available, but India has just recognised the first DNA vaccine, known as the three-dose ZyCoV-D vaccine (Zydus Cadila). This vac-cine works by injecting genetically engineered plasmids that prompt the body to produce the spike protein of COVID-19, eliciting the production of protective antibodies.
A useful and continuously updated resource on these vaccines as authorised in the EU is available at https://www.ema.europa.eu/en/medicines/human/EPAR/comirnaty. These vaccines are safe and relatively easy to develop, making use of the virus’s genetic material only, not the virus itself (Figure 2).
Useful resources• Vaccine knowledge
project: https://vk.ovg.ox.ac.uk/vk/
SEPTEMBER 2021 I 3
COVID-19 vaccines: facts, myths and advances
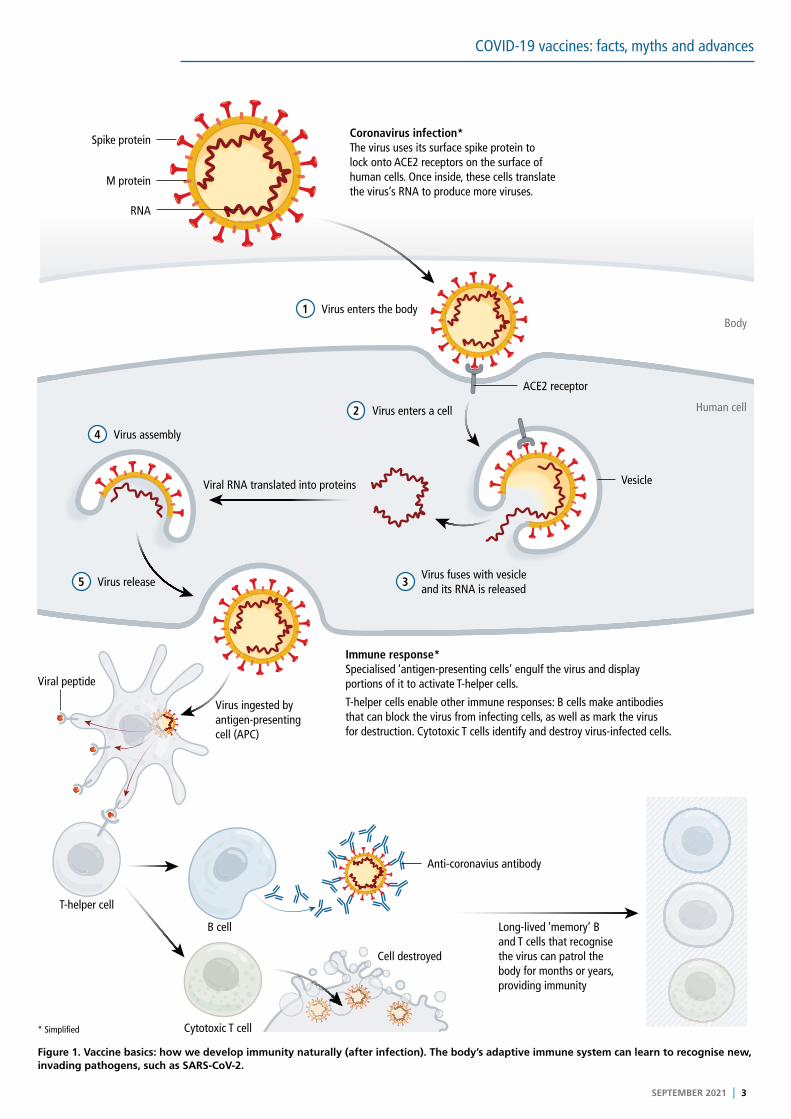
Figure 1. Vaccine basics: how we develop immunity naturally (after infection). The body’s adaptive immune system can learn to recognise new, invading pathogens, such as SARS-CoV-2.
Coronavirus infection*The virus uses its surface spike protein to lock onto ACE2 receptors on the surface of human cells. Once inside, these cells translate the virus’s RNA to produce more viruses.
Virus enters the body
Spike protein
M protein
RNA
Immune response*Specialised ‘antigen-presenting cells’ engulf the virus and display portions of it to activate T-helper cells.
T-helper cells enable other immune responses: B cells make antibodies that can block the virus from infecting cells, as well as mark the virus for destruction. Cytotoxic T cells identify and destroy virus-infected cells.
Long-lived ‘memory’ B and T cells that recognise the virus can patrol the body for months or years, providing immunity
Virus ingested by antigen-presenting cell (APC)
Viral RNA translated into proteins
Viral peptide
Anti-coronavius antibody
Cell destroyed
Cytotoxic T cell* Simplified
T-helper cell
B cell
1
Virus enters a cell
Virus fuses with vesicle and its RNA is released
Virus assembly
Virus release
ACE2 receptor
Vesicle
Human cell
Body
2
3
4
5
4 I SEPTEMBER 2021
COVID-19 vaccines: facts, myths and advances
Viral vector vaccines The AstraZeneca/Oxford and Johnson & Johnson/Janssen vaccines are based on this technology.
These vaccines use another virus, in this case an adenovirus, that has been modified so it cannot reproduce and does not cause dis-ease. The viral vector has been engineered
to contain the gene for making the SARS-CoV-2 spike protein. The adenovirus vector introduces the SARS-CoV-2 gene into the vaccinated person’s cells, which then produce the viral spike protein. The immune system recognises this as foreign and mounts an immune response (Figure 3).
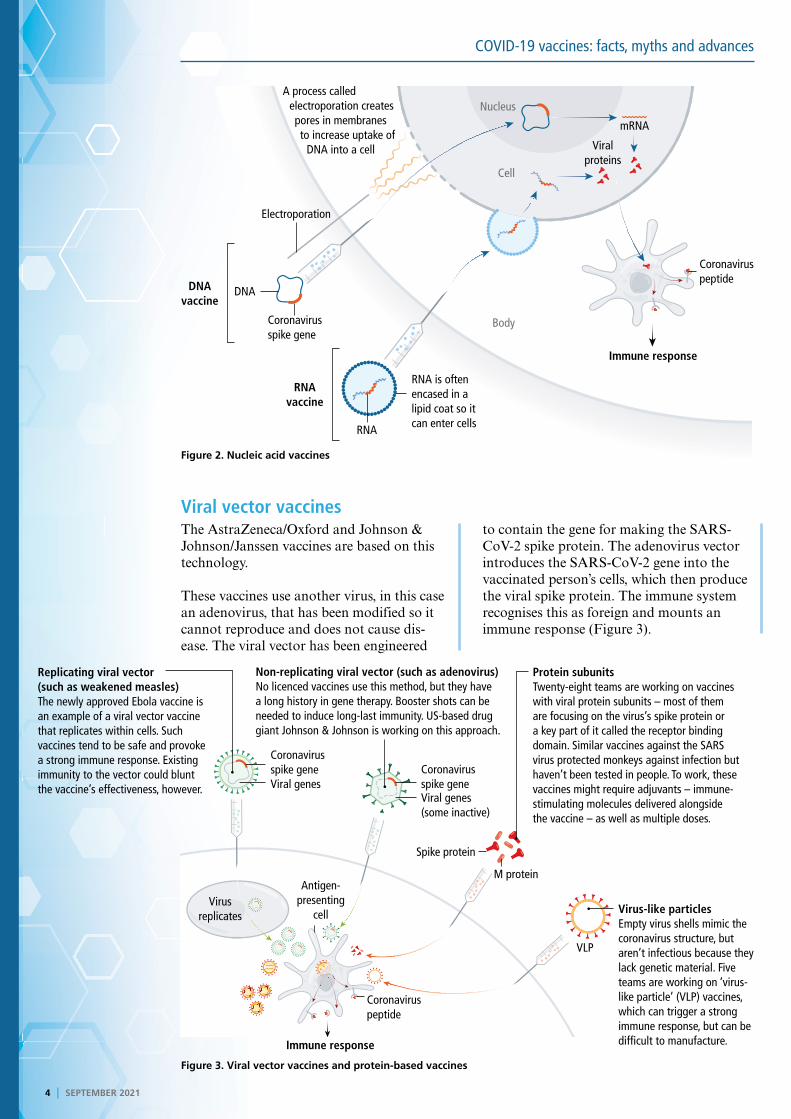
Figure 2. Nucleic acid vaccines
Figure 3. Viral vector vaccines and protein-based vaccines
Replicating viral vector (such as weakened measles)The newly approved Ebola vaccine is an example of a viral vector vaccine that replicates within cells. Such vaccines tend to be safe and provoke a strong immune response. Existing immunity to the vector could blunt the vaccine’s effectiveness, however.
Non-replicating viral vector (such as adenovirus)No licenced vaccines use this method, but they have a long history in gene therapy. Booster shots can be needed to induce long-last immunity. US-based drug giant Johnson & Johnson is working on this approach.
Protein subunitsTwenty-eight teams are working on vaccines with viral protein subunits – most of them are focusing on the virus’s spike protein or a key part of it called the receptor binding domain. Similar vaccines against the SARS virus protected monkeys against infection but haven’t been tested in people. To work, these vaccines might require adjuvants – immune-stimulating molecules delivered alongside the vaccine – as well as multiple doses.
Virus-like particlesEmpty virus shells mimic the coronavirus structure, but aren’t infectious because they lack genetic material. Five teams are working on ‘virus-like particle’ (VLP) vaccines, which can trigger a strong immune response, but can be difficult to manufacture.
VLP
M protein
Spike protein
Virus replicates
Antigen-presenting
cell
Coronavirus peptide
Immune response
Coronavirus spike gene Coronavirus
spike geneViral genesViral genes (some inactive)
A process called electroporation creates pores in membranes to increase uptake of
DNA into a cell
Electroporation
Coronavirus spike gene
DNA vaccine
RNA vaccine
Immune response
RNA is often encased in a lipid coat so it can enter cells
Coronavirus peptide
mRNA
Viral proteins
Nucleus
Body
Cell
RNA
DNA
SEPTEMBER 2021 I 5
COVID-19 vaccines: facts, myths and advances
EARN FREECPD POINTS
Join our CPD community at
and start to earn today!
www.denovomedica.com
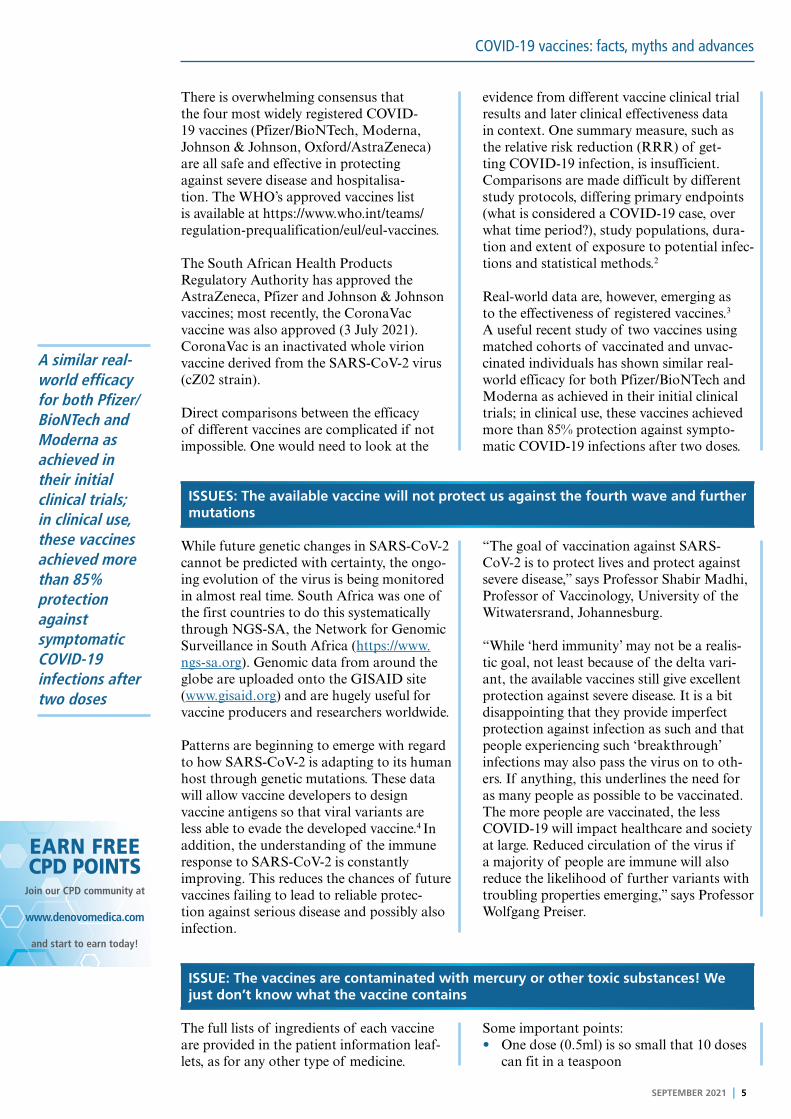
A similar real-world efficacy for both Pfizer/BioNTech and Moderna as achieved in their initial clinical trials; in clinical use, these vaccines achieved more than 85% protection against symptomatic COVID-19 infections after two doses
There is overwhelming consensus that the four most widely registered COVID-19 vaccines (Pfizer/BioNTech, Moderna, Johnson & Johnson, Oxford/AstraZeneca) are all safe and effective in protecting against severe disease and hospitalisa-tion. The WHO’s approved vaccines list is available at https://www.who.int/teams/regulation-prequalification/eul/eul-vaccines.
The South African Health Products Regulatory Authority has approved the AstraZeneca, Pfizer and Johnson & Johnson vaccines; most recently, the CoronaVac vaccine was also approved (3 July 2021). CoronaVac is an inactivated whole virion vaccine derived from the SARS-CoV-2 virus (cZ02 strain).
Direct comparisons between the efficacy of different vaccines are complicated if not impossible. One would need to look at the
evidence from different vaccine clinical trial results and later clinical effectiveness data in context. One summary measure, such as the relative risk reduction (RRR) of get-ting COVID-19 infection, is insufficient. Comparisons are made difficult by different study protocols, differing primary endpoints (what is considered a COVID-19 case, over what time period?), study populations, dura-tion and extent of exposure to potential infec-tions and statistical methods.2
Real-world data are, however, emerging as to the effectiveness of registered vaccines.3 A useful recent study of two vaccines using matched cohorts of vaccinated and unvac-cinated individuals has shown similar real-world efficacy for both Pfizer/BioNTech and Moderna as achieved in their initial clinical trials; in clinical use, these vaccines achieved more than 85% protection against sympto-matic COVID-19 infections after two doses.
ISSUES: The available vaccine will not protect us against the fourth wave and further mutations
While future genetic changes in SARS-CoV-2 cannot be predicted with certainty, the ongo-ing evolution of the virus is being monitored in almost real time. South Africa was one of the first countries to do this systematically through NGS-SA, the Network for Genomic Surveillance in South Africa (https://www.ngs-sa.org). Genomic data from around the globe are uploaded onto the GISAID site (www.gisaid.org) and are hugely useful for vaccine producers and researchers worldwide.
Patterns are beginning to emerge with regard to how SARS-CoV-2 is adapting to its human host through genetic mutations. These data will allow vaccine developers to design vaccine antigens so that viral variants are less able to evade the developed vaccine.4 In addition, the understanding of the immune response to SARS-CoV-2 is constantly improving. This reduces the chances of future vaccines failing to lead to reliable protec-tion against serious disease and possibly also infection.
“The goal of vaccination against SARS-CoV-2 is to protect lives and protect against severe disease,” says Professor Shabir Madhi, Professor of Vaccinology, University of the Witwatersrand, Johannesburg.
“While ‘herd immunity’ may not be a realis-tic goal, not least because of the delta vari-ant, the available vaccines still give excellent protection against severe disease. It is a bit disappointing that they provide imperfect protection against infection as such and that people experiencing such ‘breakthrough’ infections may also pass the virus on to oth-ers. If anything, this underlines the need for as many people as possible to be vaccinated. The more people are vaccinated, the less COVID-19 will impact healthcare and society at large. Reduced circulation of the virus if a majority of people are immune will also reduce the likelihood of further variants with troubling properties emerging,” says Professor Wolfgang Preiser.
ISSUE: The vaccines are contaminated with mercury or other toxic substances! We just don’t know what the vaccine contains
The full lists of ingredients of each vaccine are provided in the patient information leaf-lets, as for any other type of medicine.
Some important points:• One dose (0.5ml) is so small that 10 doses
can fit in a teaspoon

6 I SEPTEMBER 2021
COVID-19 vaccines: facts, myths and advances
• The constituent list allows the clinician to determine whether patients with known allergies should avoid a certain vaccine product and rather receive an alternative one
• The content of the vaccine is explained in terms of how it is produced: e.g. for the Oxford/AstraZeneca vaccine, the patient leaflet explains that the vaccine contains replication-deficient (unable to multiply) chimpanzee adenovirus which codes for the SARS-CoV-2 spike glycoprotein.
Other non-active ingredients are listed, such as L-histidine (an amino acid component of almost all human proteins), magnesium chlo-ride (salt and stabiliser), ethanol (0.002mg/dose, less than the amount found in natural foods such as bread, for example), sucrose (sugar, as stabiliser), sodium chloride (salt, as stabiliser), disodium edetate dihydrate (pre-servative, used also in some foods), water for injection.
ISSUE: The vaccines can cause serious side effects, especially the Oxford/AstraZeneca one, which has caused blood clots that lead to cerebral and venous thrombosis
The potential side effects of the SARS-CoV-2 vaccines have been much publicised in South Africa and beyond. The harmful effects and consequences of infection with SARS-CoV-2 have received much less public attention, leading to a highly distorted risk perception.
It is absolutely normal and expected that very rare side effects do not become apparent dur-ing clinical trials of vaccines. The reason is that with perhaps 10 000 or 20 000 trial par-ticipants, a side effect affecting one in 100 000 people is unlikely to be observed. That certain side effects were uncovered during the vac-cine roll-out is a tribute to the surveillance systems working well. Vaccine safety moni-toring efforts are designed to monitor vaccine recipients for ill health and death following vaccination and then determine a possible causality. Unfortunately, these basic princi-ples are often not generally understood, lead-ing to claims like: ‘Hundreds are dying after receiving the vaccine’ – something perhaps not unexpected when large numbers of old
or very frail people are vaccinated, as even when they are not vaccinated, their risk of death is substantial because of their age and frailty. The important question is whether these deaths are related to the vaccine. This is determined by thorough investigations conducted by independent bodies of all noti-fied cases for which sufficient information is provided.
The very rare development of a vaccine-induced immune thrombotic thrombocyto-penia (VITT) following the administration of adenoviral vector vaccines (AstraZeneca and Johnson & Johnson) is now better understood. It occurs as a moderate to severe thrombocytopenia with thrombotic com-plications, particularly cerebral sinus vein thrombosis. The Southern African Society of Thrombosis and Haemostasis recently pro-duced expert guidance for the clinical man-agement of VITT.5 Its key recommendations are summarised in Table 1.
Table 1. Key recommendations for managing VITT
• VITT is an extremely rare but potentially fatal complication of vaccination with adenoviral vector vaccines
• It is important to consider this complication, because management differs from other thrombotic events and standard treatment may worsen outcomes
• Thrombosis with thrombocytopenia 4 -16 days post vaccination should prompt clinicians to consider the entity
• Thrombocytopenia post vaccination may be due to many other reasons in the absence of thrombosis, such as malaria, HIV or immune thrombocytopenia
• Patients with VITT should not be given heparin, platelet transfusions or warfarin (acutely).
That certain side effects were uncovered during the vaccine roll-out is a tribute to the surveillance systems working well
SEPTEMBER 2021 I 7
COVID-19 vaccines: facts, myths and advances
EARN FREECPD POINTS
Join our CPD community at
and start to earn today!
www.denovomedica.com
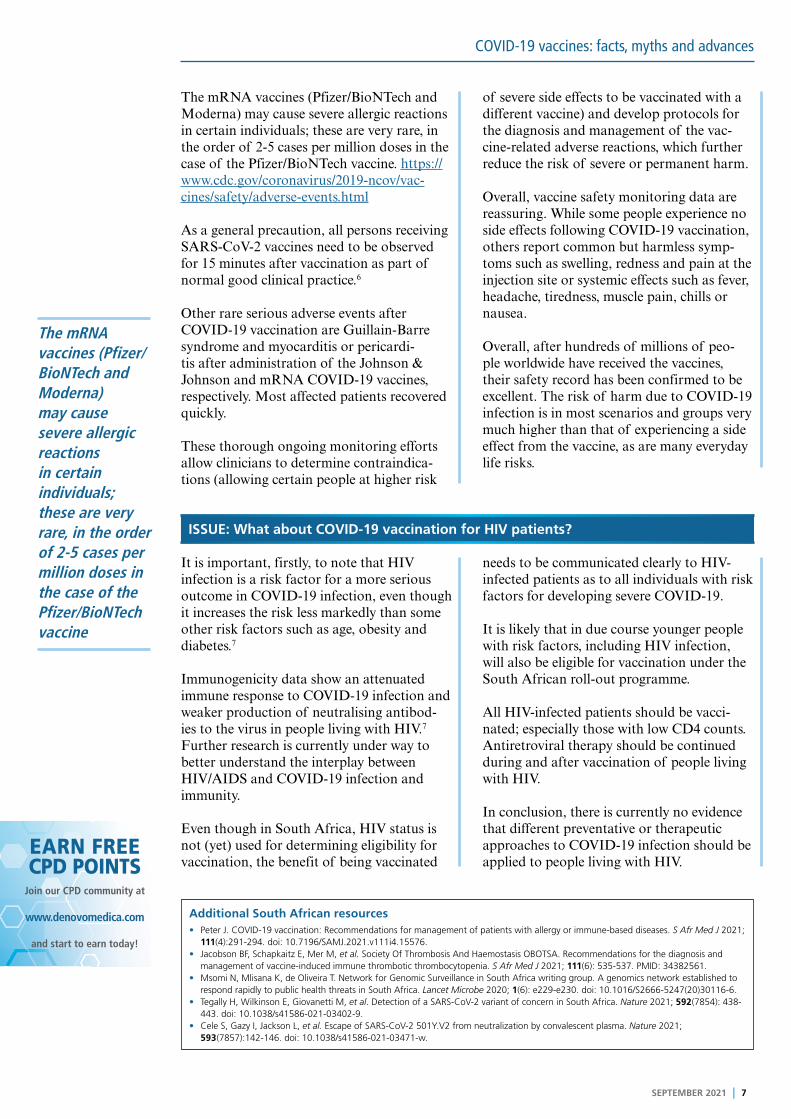
The mRNA vaccines (Pfizer/BioNTech and Moderna) may cause severe allergic reactions in certain individuals; these are very rare, in the order of 2-5 cases per million doses in the case of the Pfizer/BioNTech vaccine. https://www.cdc.gov/coronavirus/2019-ncov/vac-cines/safety/adverse-events.html
As a general precaution, all persons receiving SARS-CoV-2 vaccines need to be observed for 15 minutes after vaccination as part of normal good clinical practice.6
Other rare serious adverse events after COVID-19 vaccination are Guillain-Barre syndrome and myocarditis or pericardi-tis after administration of the Johnson & Johnson and mRNA COVID-19 vaccines, respectively. Most affected patients recovered quickly.
These thorough ongoing monitoring efforts allow clinicians to determine contraindica-tions (allowing certain people at higher risk
of severe side effects to be vaccinated with a different vaccine) and develop protocols for the diagnosis and management of the vac-cine-related adverse reactions, which further reduce the risk of severe or permanent harm.
Overall, vaccine safety monitoring data are reassuring. While some people experience no side effects following COVID-19 vaccination, others report common but harmless symp-toms such as swelling, redness and pain at the injection site or systemic effects such as fever, headache, tiredness, muscle pain, chills or nausea.
Overall, after hundreds of millions of peo-ple worldwide have received the vaccines, their safety record has been confirmed to be excellent. The risk of harm due to COVID-19 infection is in most scenarios and groups very much higher than that of experiencing a side effect from the vaccine, as are many everyday life risks.
ISSUE: What about COVID-19 vaccination for HIV patients?
It is important, firstly, to note that HIV infection is a risk factor for a more serious outcome in COVID-19 infection, even though it increases the risk less markedly than some other risk factors such as age, obesity and diabetes.7
Immunogenicity data show an attenuated immune response to COVID-19 infection and weaker production of neutralising antibod-ies to the virus in people living with HIV.7 Further research is currently under way to better understand the interplay between HIV/AIDS and COVID-19 infection and immunity.
Even though in South Africa, HIV status is not (yet) used for determining eligibility for vaccination, the benefit of being vaccinated
needs to be communicated clearly to HIV-infected patients as to all individuals with risk factors for developing severe COVID-19.
It is likely that in due course younger people with risk factors, including HIV infection, will also be eligible for vaccination under the South African roll-out programme.
All HIV-infected patients should be vacci-nated; especially those with low CD4 counts. Antiretroviral therapy should be continued during and after vaccination of people living with HIV.
In conclusion, there is currently no evidence that different preventative or therapeutic approaches to COVID-19 infection should be applied to people living with HIV.
The mRNA vaccines (Pfizer/BioNTech and Moderna) may cause severe allergic reactions in certain individuals; these are very rare, in the order of 2-5 cases per million doses in the case of the Pfizer/BioNTech vaccine
Additional South African resources• Peter J. COVID-19 vaccination: Recommendations for management of patients with allergy or immune-based diseases. S Afr Med J 2021;
111(4):291-294. doi: 10.7196/SAMJ.2021.v111i4.15576.• Jacobson BF, Schapkaitz E, Mer M, et al. Society Of Thrombosis And Haemostasis OBOTSA. Recommendations for the diagnosis and
management of vaccine-induced immune thrombotic thrombocytopenia. S Afr Med J 2021; 111(6): 535-537. PMID: 34382561. • Msomi N, Mlisana K, de Oliveira T. Network for Genomic Surveillance in South Africa writing group. A genomics network established to
respond rapidly to public health threats in South Africa. Lancet Microbe 2020; 1(6): e229-e230. doi: 10.1016/S2666-5247(20)30116-6.• Tegally H, Wilkinson E, Giovanetti M, et al. Detection of a SARS-CoV-2 variant of concern in South Africa. Nature 2021; 592(7854): 438-
443. doi: 10.1038/s41586-021-03402-9.• Cele S, Gazy I, Jackson L, et al. Escape of SARS-CoV-2 501Y.V2 from neutralization by convalescent plasma. Nature 2021;
593(7857):142-146. doi: 10.1038/s41586-021-03471-w.

DisclaimerThe views and opinions expressed in the article are those of the presenters and do not necessarily reflect those of the publisher or its sponsor. In all clinical instances, medical practitioners are referred to the product insert documentation as approved by relevant control authorities.
8 I SEPTEMBER 2021
COVID-19 vaccines: facts, myths and advances
EARN FREECPD POINTS
Are you a member of Southern Africa’s leading
digital Continuing Professional Development
website earning FREE CPD points with access to
best practice content?
Only a few clicks and you can register to start
earning today
Visit
For all Southern African healthcare professionals
www.denovomedica.com
DeNovo Medica
@deNovoMedica
deNovo Medica
Find us at
Published by
70 Arlington Street, Everglen, Cape Town, 7550Tel: (021) 976 0485 I [email protected]
© 2021 deNovo MedicaReg: 2012/216456/07
This summary report was compiled for deNovo Medica byJulia AalbersBSc Hons
Key learnings
• The SARS-CoV-2 genome was made available globally early during the initial COVID-19 outbreak in Wuhan
• The rapid development of COVID-19 vaccines has benefited from earlier research on vaccines for MERS, Ebola and Lassa fever
• The vaccine hesitancy of your patient can be reduced by the clinician’s confidence and by providing supportive information.
NOW EARN FREE CPD POINTS
Click here to access and submit deNovo Medica’s CPD modules
ReferencesClick on reference to access the scientific article1. Callaway E. The race for coronavirus vaccines: a graphical
guide. Nature 2020; 580(7805): 576-577.
2. Olliaro P, Torreele E, Vaillant M. COVID-19 vaccine efficacy and
effectiveness – the elephant (not) in the room. Lancet Microbe
2021; Published April 20, 2021.
3. Pawlowski C, Lenehan P, Puranik A, et al. FDA-authorized
mRNA COVID-19 vaccines are effective per real-world evidence
synthesized across a multi-state health system. Med 2021; 2:
979-992.
4. Van Dorp L, Acman M, Richard D, et al. Emergence of genomic
diversity and recurrent mutations in SARS-CoV-2. Infect Genet
Evol 2020; 83: 104351.
5. Jacobson BF, Schapkaitz E, Mer M, et al. Society of Thrombosis
and Haemostasis OBOTSA. Recommendations for the diagnosis
and management of vaccine-induced immune thrombotic
thrombocytopenia. S Afr Med J 2021; 111(6): 535-537. PMID:
34382561.
6. Banerji A, Wickner PG, Saff R, et al. mRNA vaccines to prevent
COVID-19 disease and reported allergic reactions: Current
evidence and suggested approach. J Allergy Clin Immunol Pract
2021; 9(4): 1423-1437.
7. Boulle A, Davies MA, Hussey H, et al. Risk factors for COVID-19
death in a population cohort study from the Western Cape
Province, South Africa. Clin Infect Dis 2020; ciaa1198. doi:
10.1093/cid/ciaa1198. [Epub ahead of print]. PMID: 32860699;
PMCID: PMC7499501.
8. Spinelli M, Lynch KA, Yun CA, et al. SARS-CoV-2
seroprevalence and IgG levels are lower among people living
with HIV. Virtual conference on retroviruses and opportunistic
infections, San Francisco, CA. March 6-10, 2021. Abstract 627.


















