E-prescribing in community-based practices: successes and barriers
25
E-prescribing in community-based practices: successes and barriers Michael A Fischer, M.D., M.S. Division of Pharmacoepidemiology and Pharmacoeconomics Department of Medicine Brigham and Women’s Hospital Harvard Medical School
description
E-prescribing in community-based practices: successes and barriers. Michael A Fischer, M.D., M.S. Division of Pharmacoepidemiology and Pharmacoeconomics Department of Medicine Brigham and Women’s Hospital Harvard Medical School. Research team. BCBSMA Megan Bell Adrienne Cyrulik, MPH - PowerPoint PPT Presentation
Transcript of E-prescribing in community-based practices: successes and barriers

E-prescribing in community-based practices: successes and
barriers
Michael A Fischer, M.D., M.S.Division of Pharmacoepidemiology and
Pharmacoeconomics
Department of Medicine
Brigham and Women’s Hospital
Harvard Medical School

Research team• Co-authorsRitu Agarwal, PhD
U Maryland
Corey Angst, PhD
Notre Dame
Cate Desroches, PhD
MGH
• BCBSMA– Megan Bell– Adrienne Cyrulik, MPH
• Tufts Health Plan– Julie Newton
• Zix Corporation– Angus MacDonald– Scott Plunkett

Background
• Promise of e-prescribing– Improved safety– Value– Efficiency
• Slow spread to community-based practices– Uncertain what drives successful e-prescribing
uptake in community setting

Study setting
• Initiated by BCBSMA and Tufts Health Plan
• Partnered with ZixCorp, providing physicians with PocketScript system
• Program began in early 2004

Prior studies – erx adoption
Fischer et al, JGIM, 2008

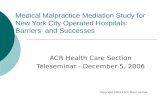
Prior studies – e-rx and costs
50%
52%
54%
56%
58%
60%
62%
64%
-6 -5 -4 -3 -2 -1 1 2 3 4 5 6 7 8 9 10 11
Month relative to 1st e-prescription
Per
cen
t T
ier
1
Control prescribers
Intervention prescribers, e-prescriptionsIntervention prescribers, non-e-prescriptions
Start of e-prescribing
Fischer et al, Arch Int Med, 2008, in press

Prior studies – e-rx and safety
• Most alerts over-ridden by prescribers– Weingart et al. Arch Int Med, 2003
• Reviews suggest reduced ADEs, but inadequate studies in outpatient setting– Ammenwerth et al. JAMIA, 2008

Study questions
• What is the experience of community-based practices that adopt electronic prescribing systems?
• What barriers remain to successful adoption and use of e-prescribing?
• Where has e-prescribing succeeded; has it created new problems?

Study design
• Focus groups– Conducted spring 2008– Prescribers and office staff
• Internal medicine, pediatrics, FP, cardiology, nephrology
– Both current and former users• High/low volume, abandoned, transitioned to EMR
• Interviews– Detailed discussions with prescribers

Findings
• E-prescribing positives
• Ongoing challenges/barriers

E-prescribing positives
• Prescription security
• Financial gain
• Office efficiency
• Medication safety
• Insurance issues
• Communication with pharmacy

E-prescribing positives
• Prescription security– Less people touch the actual prescription– Patients cannot lose the prescription– Patients cannot tamper with prescription

E-prescribing positives
• Financial gain– Direct incentives a major factor
• Initial adoption subsidized• Later incentives for ongoing use
– Potential gains in patient satisfaction• “if we can reduce wait times, we’ve succeeded”• Unclear of RoI in terms of practice billing

E-prescribing positives
• Office efficiency– Major changes in practice workflow
• Less calls for front-end staff• Refills and other non-critical medication issues
can be batched for MD review
– Frees staff time and attention• Less interruption of work• Pharmacy information is updated and accurate• Perceived ROI, but hard to quantify

E-prescribing positives
• Medication safety– Quick review of patient medication history
• Available round the clock, out of office
– Alerts about drug-drug interactions• Office staff appreciated reminders• Physicians less certain, many alerts dismissed
– Ability to identify patients on a specific drug• Especially useful for recalls
– “I can identify all the patients on..”

E-prescribing positives
• Insurance issues– Can see if a drug is not covered
• Avoids callbacks, increased patient satisfaction
– Ability to identify patients on a specific drug• Also useful for prescribing incentive programs

E-prescribing positives
• Communication with pharmacy– Timely flow of information
– Ability to send specific messages• e.g.: “no more refills until patient sees doctor”

Ongoing challenges/barriers
• Learning curve
• Usability
• Reliability
• Safety concerns
• Patient resistance
• Data security

Ongoing challenges/barriers
• Learning curve– New skill: “not covered in medical school”– Difficult for older prescribers– High burden on champions/superusers– New tasks for some personnel – source of
resistance– Lack of support– “Locked in” with initial vendor choice

Ongoing challenges/barriers
• Usability– Types of devices/interfaces– Problems with some pharmacies– Inability to transmit to PBMs
• Reliability– Connectivity/network problems, loss of
productivity– Resistance for sick patients or weekends

Ongoing challenges/barriers
• Safety concerns– Selecting wrong patient– Selecting wrong drug (Cipro/Cialis)– Some doses/formulations not in system– Drug alerts not perceived as helpful:
“ignore almost all”– Some alerts may be handled by non-
prescribers in the process of queuing

Ongoing challenges/barriers• Patient resistance
– Wanting something in hand (older pts)– Bad experiences with failed transmissions– Inability to transmit to PBMs
• Data security– Concern about whether transmitting patient
data creates liability exposure– Concern about prescribing data and
tracking/profiling– Who owns the data: cost of changing

Summary observations
• Overall positive experience – almost none would “turn back the clock”
• Successes: office efficiency, pharmacy communication, formulary information, prescription security
• Barriers/challenges: Learning curve, reliability, questionable safety impact

Summary observations
• Benefits more apparent in larger practices with high volume of chronic mediations– More opportunities to streamline workflow– Prescription volume/management is seen
as a major issue at baseline– Possible financial gains easier to perceive

Next steps
• On-site visits to observe system use, validate focus group observations
• Large-sample survey to test generalizability of initial findings
• Quantitative studies of e-rx impact on cost, safety, adherence, clinical outcomes