E Gfr 2008
66
eGFR: Implications, Limitations & Clinical applications Malvinder S. Parmar MB, MS, FRCPC, FACP, FASN Associate Professor, Northern Ontario Medical School Assistant Professor, University of Ottawa
Transcript of E Gfr 2008

eGFR: Implications, Limitations & Clinical applications
Malvinder S. ParmarMB, MS, FRCPC, FACP, FASN
Associate Professor,
Northern Ontario Medical School
Assistant Professor,
University of Ottawa
‘EGFR’ vs ‘eGFR’What is the difference?
EGFR
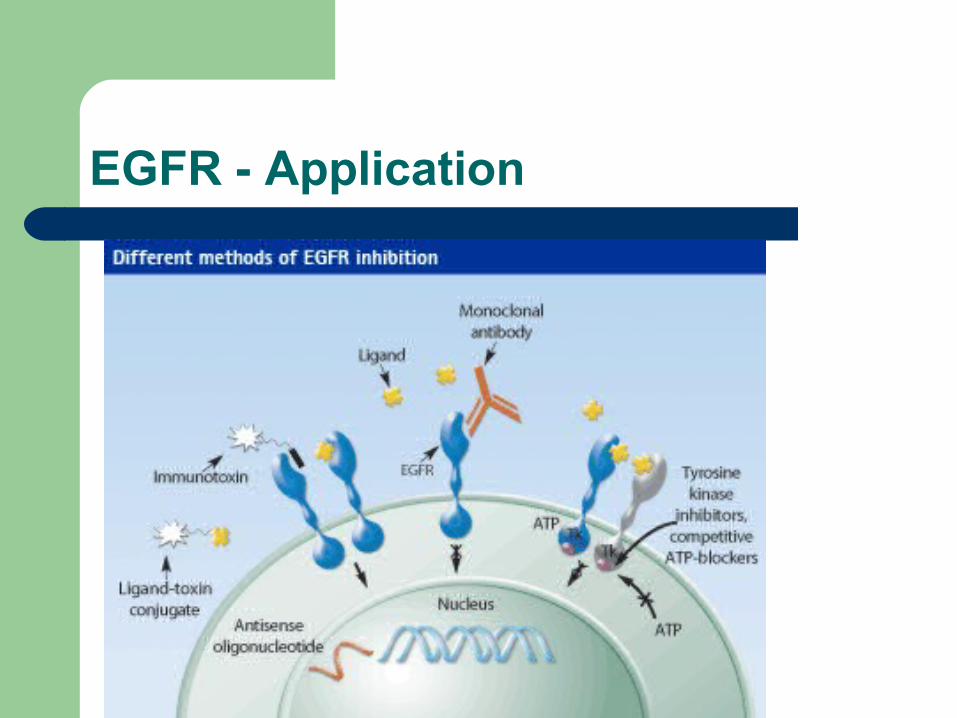
EGFR - Application
‘EGFR’ vs ‘eGFR’
EGFR– Epidermal Growth Factor Receptor
eGFR– Estimated Glomerular Filtration Rate
What is the difference?
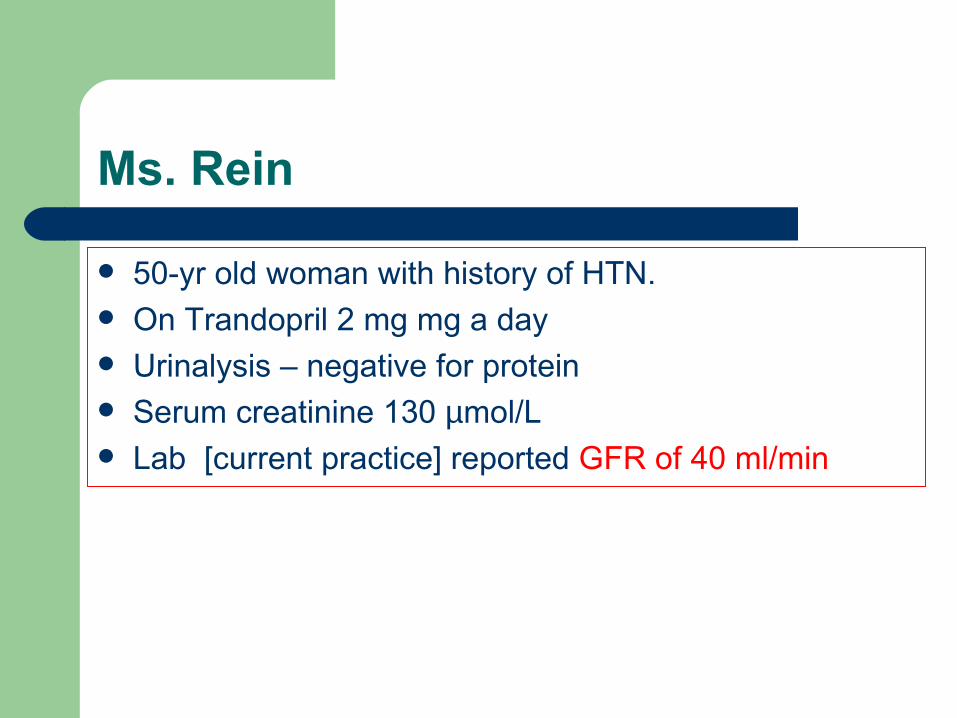
Ms. Rein
50-yr old woman with history of HTN. On Trandopril 2 mg mg a day Urinalysis – negative for protein Serum creatinine 130 µmol/L Lab [current practice] reported GFR of 40 ml/min
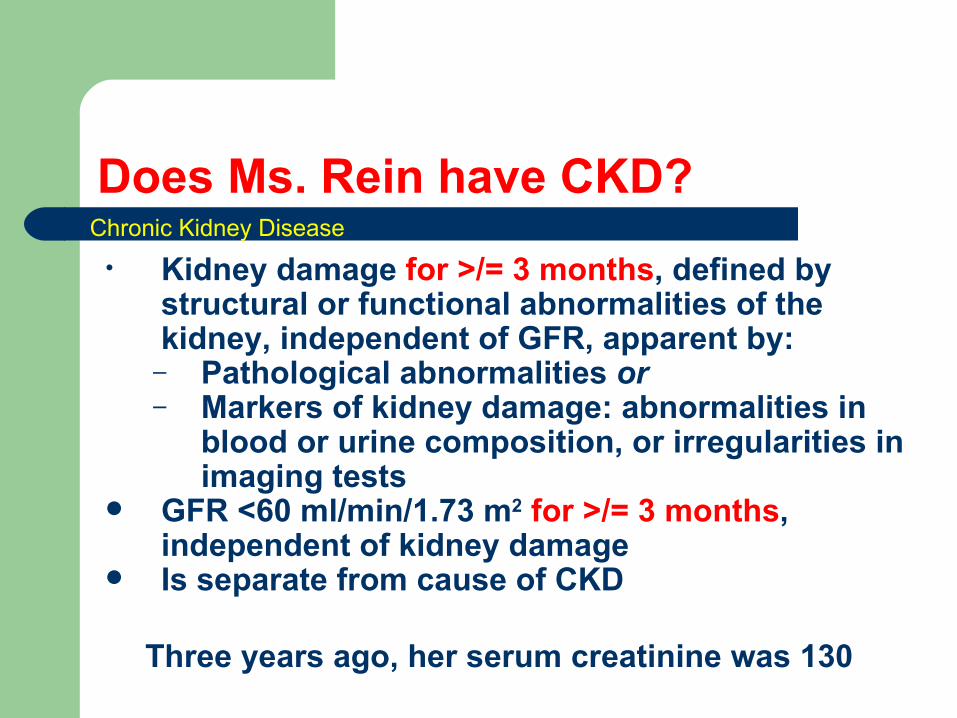
Does Ms. Rein have CKD?
• Kidney damage for >/= 3 months, defined by structural or functional abnormalities of the kidney, independent of GFR, apparent by:
– Pathological abnormalities or– Markers of kidney damage: abnormalities in
blood or urine composition, or irregularities in imaging tests
GFR <60 ml/min/1.73 m2 for >/= 3 months, independent of kidney damage
Is separate from cause of CKD
Chronic Kidney Disease
Three years ago, her serum creatinine was 130
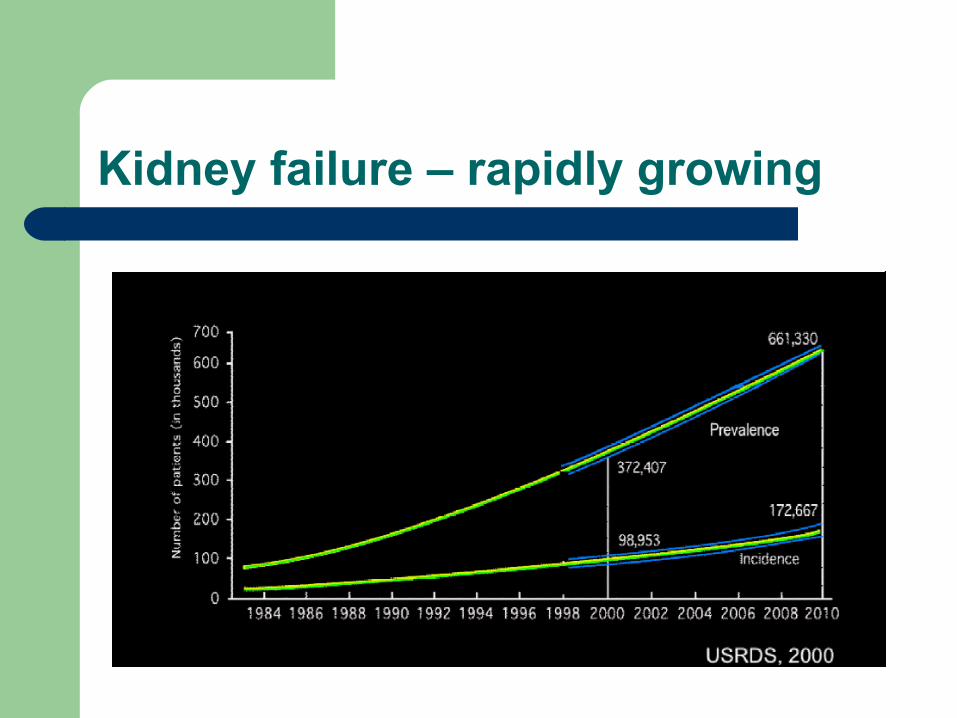
Kidney failure – rapidly growing
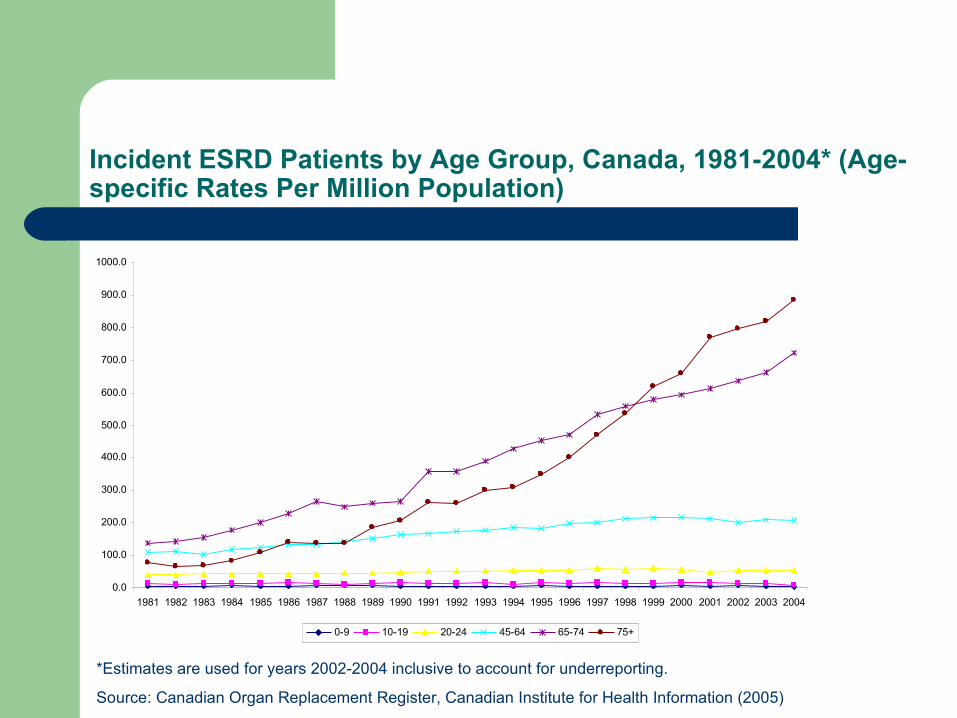
Incident ESRD Patients by Age Group, Canada, 1981-2004* (Age-specific Rates Per Million Population)
*Estimates are used for years 2002-2004 inclusive to account for underreporting.
Source: Canadian Organ Replacement Register, Canadian Institute for Health Information (2005)
0.0
100.0
200.0
300.0
400.0
500.0
600.0
700.0
800.0
900.0
1000.0
1981 1982 1983 1984 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
0-9 10-19 20-24 45-64 65-74 75+
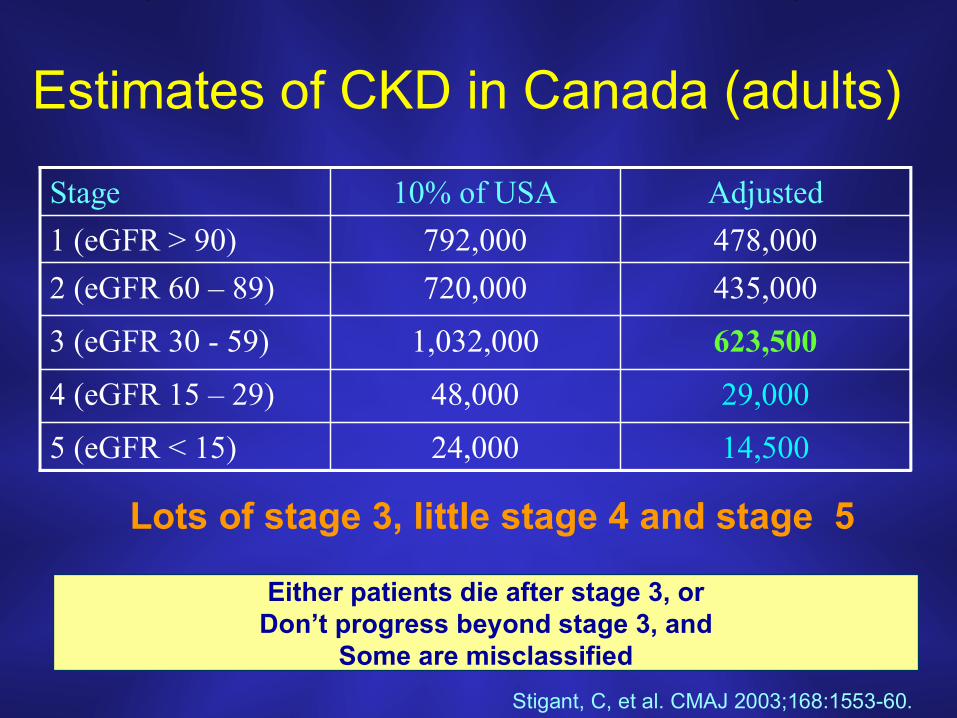
Estimates of CKD in Canada (adults)
14,50024,0005 (eGFR < 15)
29,00048,0004 (eGFR 15 – 29)
623,5001,032,0003 (eGFR 30 - 59)
435,000720,0002 (eGFR 60 – 89)
478,000792,0001 (eGFR > 90)
Adjusted10% of USAStage
Stigant, C, et al. CMAJ 2003;168:1553-60.
Lots of stage 3, little stage 4 and stage 5
Either patients die after stage 3, orDon’t progress beyond stage 3, and
Some are misclassified
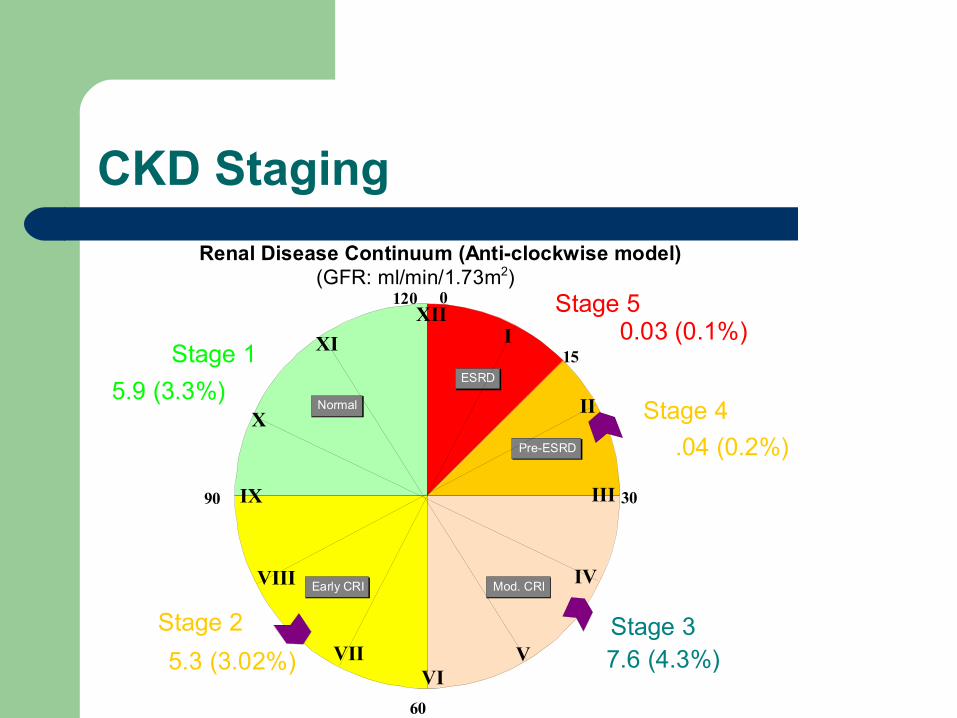
CKD Staging
Pre-ESRD
ESRD
Normal
Early CRI Mod. CRI
120
90
60
30
15
XII0
XI
X
IX
VIII
VIIVI
V
IV
III
II
I
Renal Disease Continuum (Anti-clockwise model)(GFR: ml/min/1.73m2)
Stage 1
Stage 2 Stage 3
Stage 4
Stage 5
5.9 (3.3%)
5.3 (3.02%) 7.6 (4.3%)
.04 (0.2%)
0.03 (0.1%)
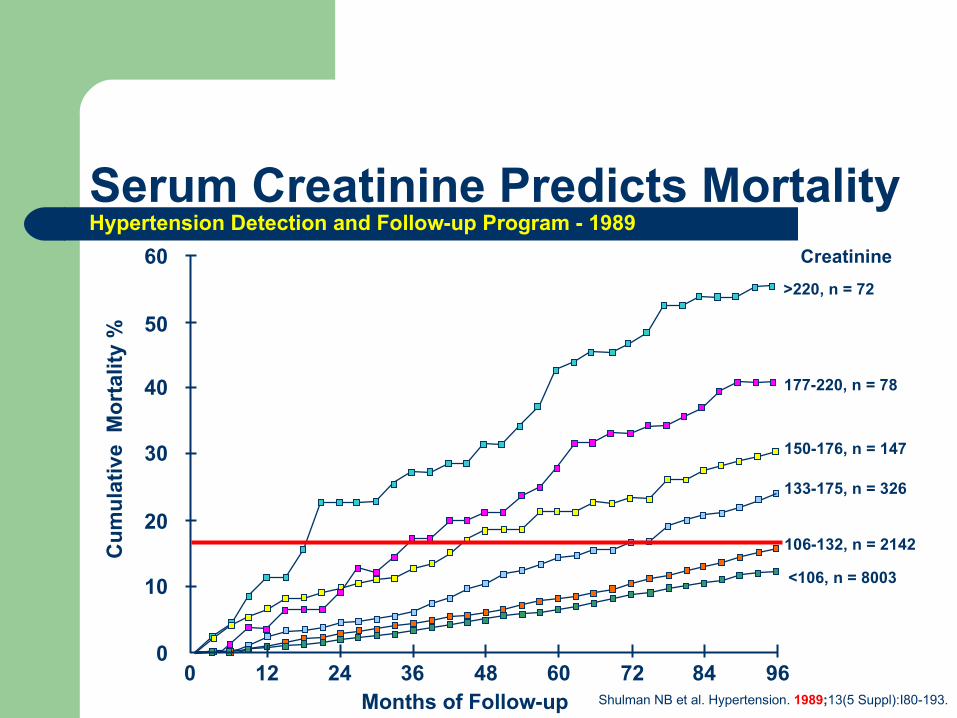
Shulman NB et al. Hypertension. 1989;13(5 Suppl):I80-193.
40
50
60
30
20
10
00 12 24 36 48 60 72 84 96
Months of Follow-up
Cu
mu
lati
ve M
ort
alit
y %
>220, n = 72
177-220, n = 78
150-176, n = 147
133-175, n = 326
106-132, n = 2142
<106, n = 8003
Creatinine
Serum Creatinine Predicts MortalityHypertension Detection and Follow-up Program - 1989
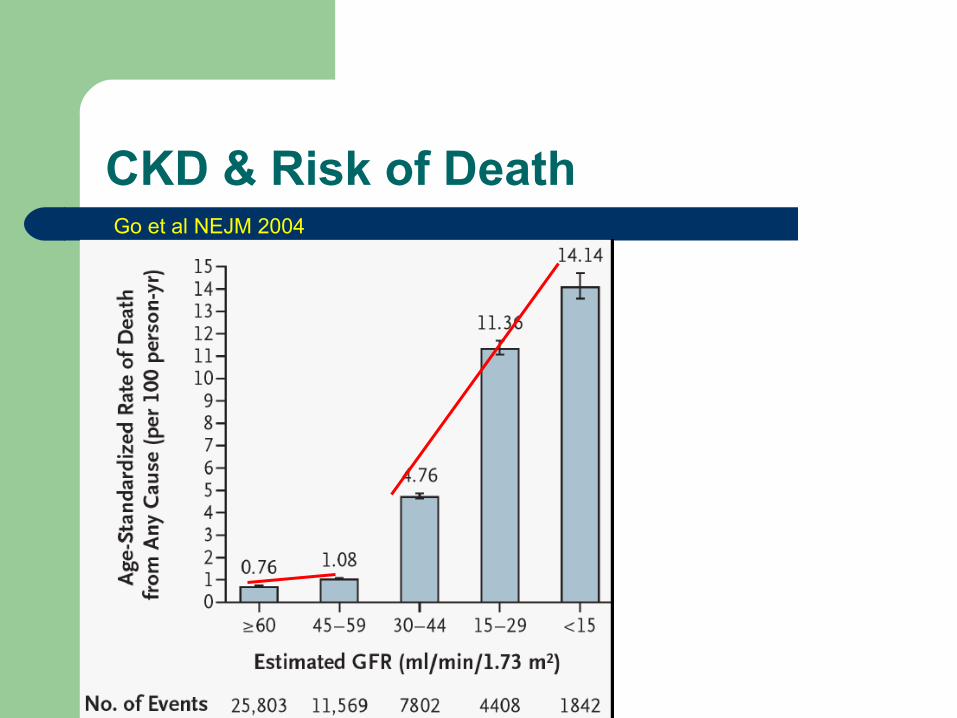
CKD & Risk of DeathGo et al NEJM 2004
Assessing Kidney function
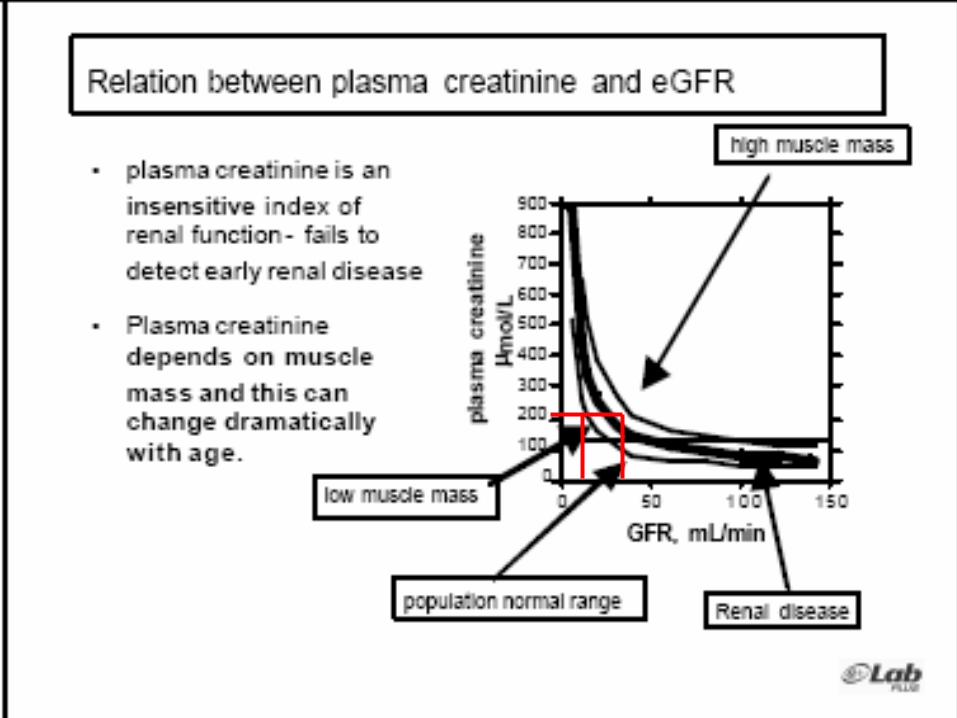
Serum creatinine– Non-linear association with GFR
Clearance/GFR– Inulin clearance
Gold standard, not widely available– Clearance of radio-labeled markers [iothalamate]
Accurate but expensive– 24-hr urine collection - creatinine clearance
Often inaccurate collections– Estimating equations – for GFR
Recommended for most
What are the various methods to assess kidney function?
Serum Creatinine
May not rise until late stages of CKD– >50% loss of kidney function
Creatinine increases through puberty, then declines with age [as GFR]
Serum creatinine - problems
Non-renal influences: gender, ethnicity and age nutrition/diet drugs (e.g. cimetidine) muscle mass
Clinical utility: Poor sensitivity for CKD Not useful in ARF Muscle wasting disorders
Analytical problems: Non-specificity (protein, ketones, ascorbic acid) (pseudo-chromogens) Spectral interferences (icterus/lipemia/hemolysis) No international standardization
Glomerular Filtration Rate [GFR]
Volume of plasma water filtered through glomerular membranes per unit of time– Normalized to 1.73 m2
Measured as clearance from plasma into urine of a substance that is,– Freely filtered– Not protein bound– Neither secreted, nor absorbed by tubules– Not removed from blood by extra-renal process
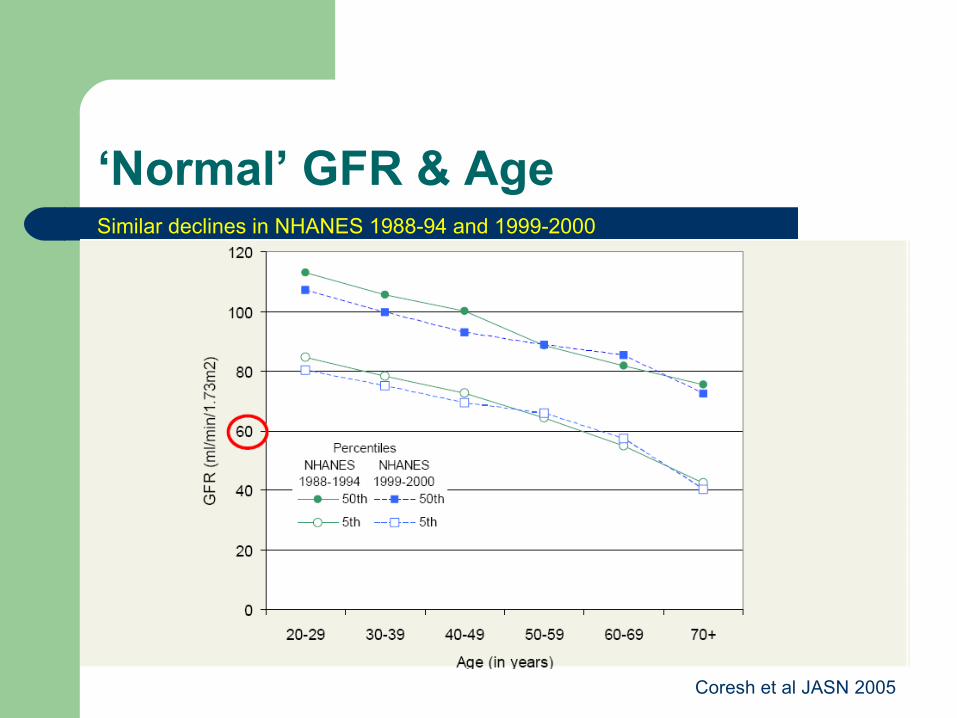
‘Normal’ GFR & AgeSimilar declines in NHANES 1988-94 and 1999-2000
Coresh et al JASN 2005
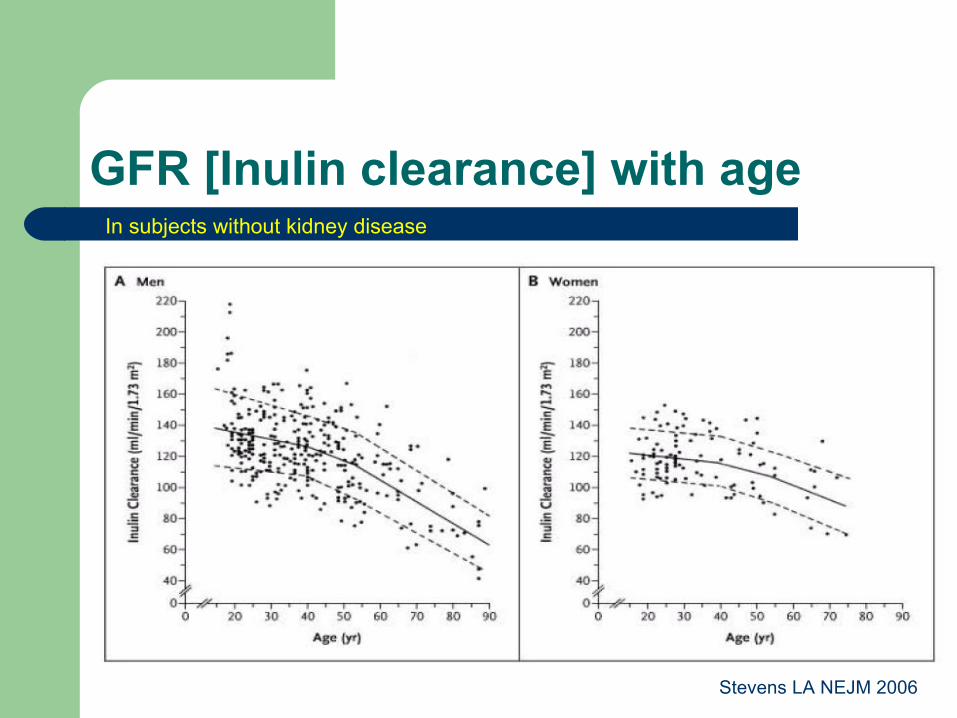
GFR [Inulin clearance] with ageIn subjects without kidney disease
Stevens LA NEJM 2006
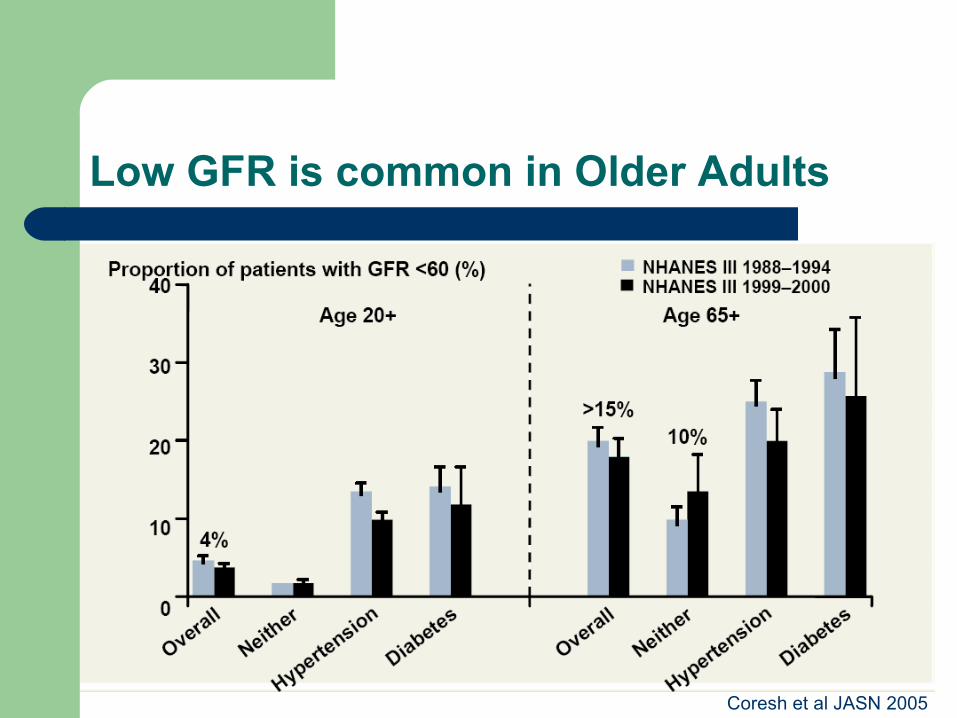
Low GFR is common in Older Adults
Coresh et al JASN 2005
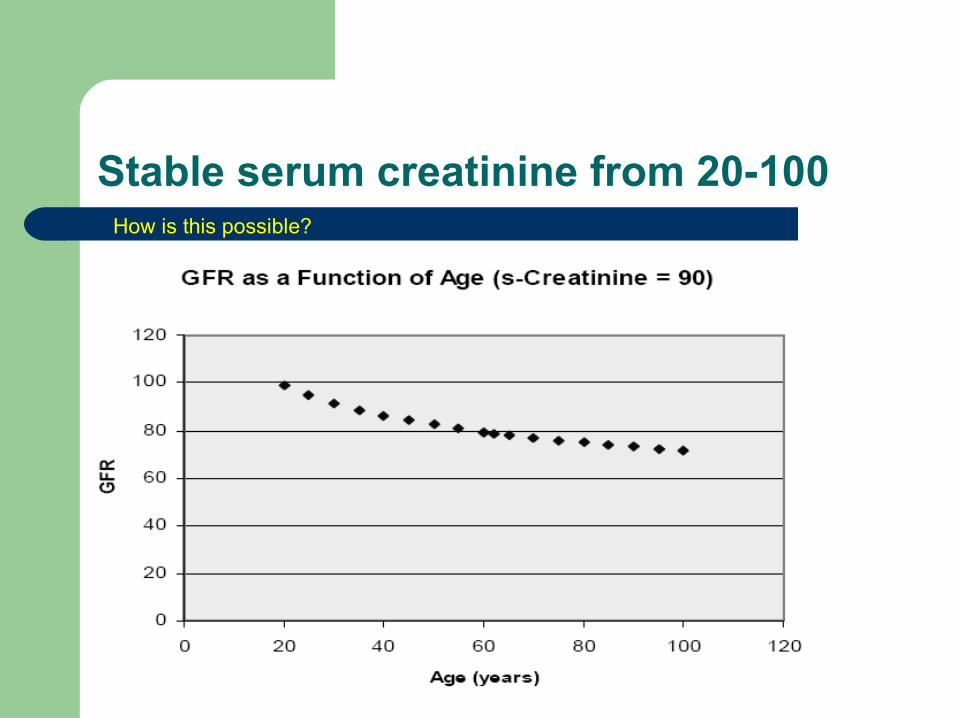
Stable serum creatinine from 20-100How is this possible?

Changes in GFR & Muscle Mass with Age
Serum Creatinine
GFR
Muscle Mass

Serum Creatinine is NOT GFR
GFRml/min
Serum Creatinineumol/L Proportional to:
Muscle Productionml/min
Assessing GFR
Exogenous Markers– Inulin clearance – ‘Gold standard’, expensive, not
widely available– Radio-isotopes [125I-Iothalamate, 51Cr-EDTA] –
accurate but expensive Endogenous Markers
– Creatinine clearance – needs accurate urine collection, time-consuming
Estimating equations [eGFR]
GFR and Clearance
Clearance = UcrV/Pcr
Clearance = GFR, if– Production rate is constant– Substance is freely filtered– Excreted unchanged in urine
Creatinine clearance vs. True GFR
Creatinine clearance, co-incidentally, matches fairly well to GFR down to 60 ml/min
– 10% of urinary creatinine is from tubular secretion– 10% of serum creatinine is from non-creatinine chromogens– These values cancel each other Ucr/Scr
Creatinine clearance becomes progressively higher than true GFR, when GFR falls below 60 ml/min
– Because tubular and extra-renal secretion of creatinine increases as GFR decreases
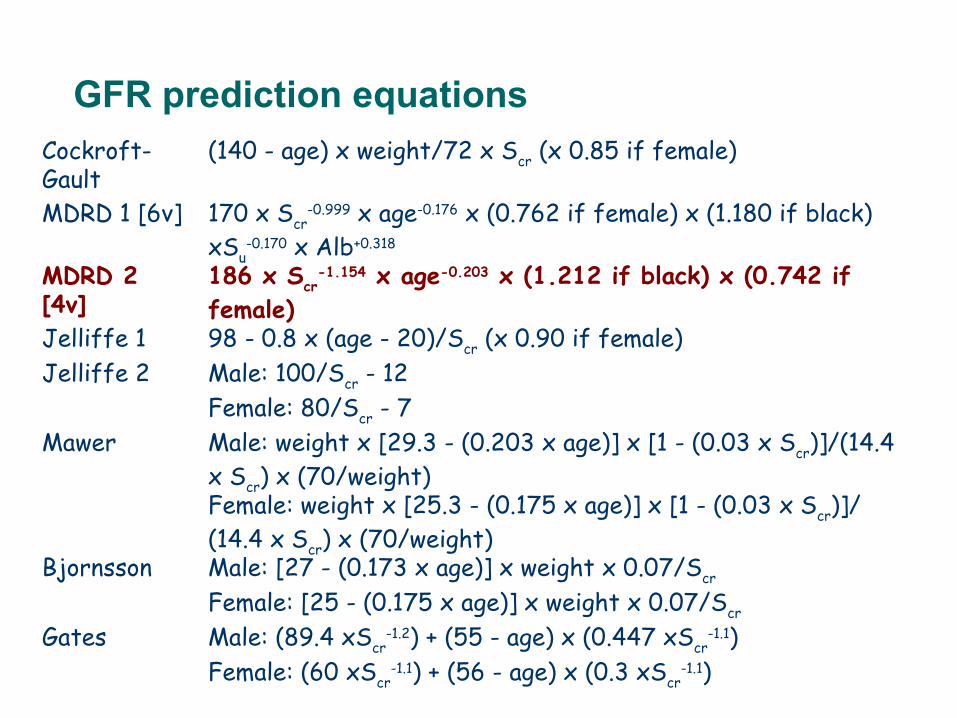
GFR prediction equationsCockroft-Gault
(140 - age) x weight/72 x Scr (x 0.85 if female)
MDRD 1 [6v] 170 x Scr-0.999 x age-0.176 x (0.762 if female) x (1.180 if black)
xSu-0.170 x Alb+0.318
MDRD 2 [4v]
186 x Scr-1.154 x age-0.203 x (1.212 if black) x (0.742 if
female)Jelliffe 1 98 - 0.8 x (age - 20)/Scr (x 0.90 if female)Jelliffe 2 Male: 100/Scr - 12
Female: 80/Scr - 7Mawer Male: weight x [29.3 - (0.203 x age)] x [1 - (0.03 x Scr)]/(14.4
x Scr) x (70/weight)Female: weight x [25.3 - (0.175 x age)] x [1 - (0.03 x Scr)]/(14.4 x Scr) x (70/weight)
Bjornsson Male: [27 - (0.173 x age)] x weight x 0.07/Scr
Female: [25 - (0.175 x age)] x weight x 0.07/Scr
Gates Male: (89.4 xScr-1.2) + (55 - age) x (0.447 xScr
-1.1)Female: (60 xScr
-1.1) + (56 - age) x (0.3 xScr-1.1)
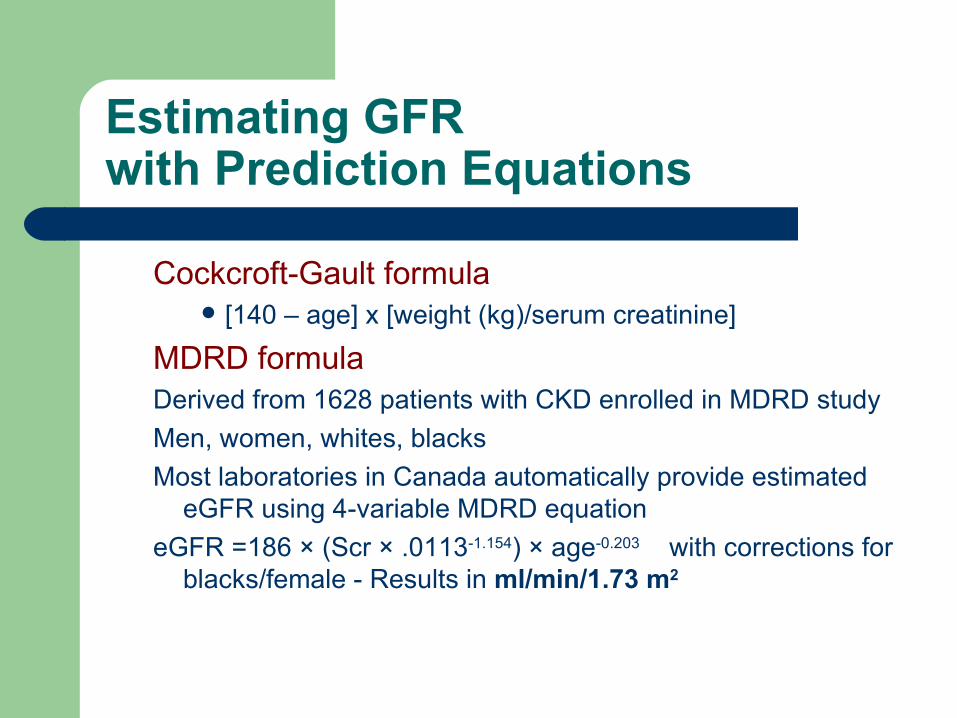
Estimating GFR with Prediction Equations
Cockcroft-Gault formula [140 – age] x [weight (kg)/serum creatinine]
MDRD formula Derived from 1628 patients with CKD enrolled in MDRD study
Men, women, whites, blacks
Most laboratories in Canada automatically provide estimated eGFR using 4-variable MDRD equation
eGFR =186 × (Scr × .0113-1.154) × age-0.203 with corrections for blacks/female - Results in ml/min/1.73 m2
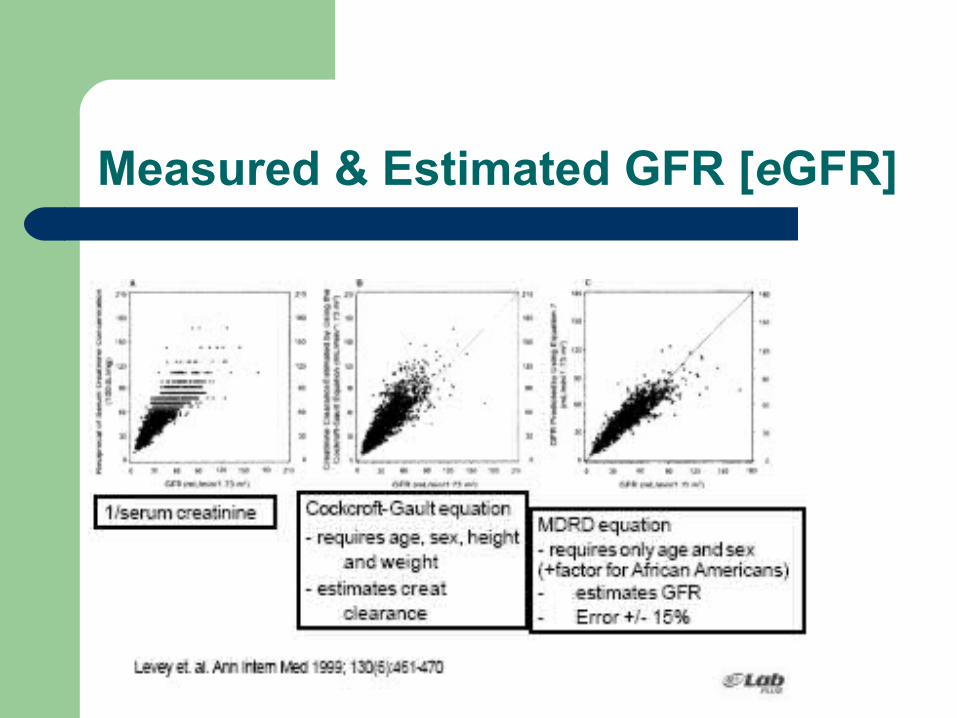
Measured & Estimated GFR [eGFR]
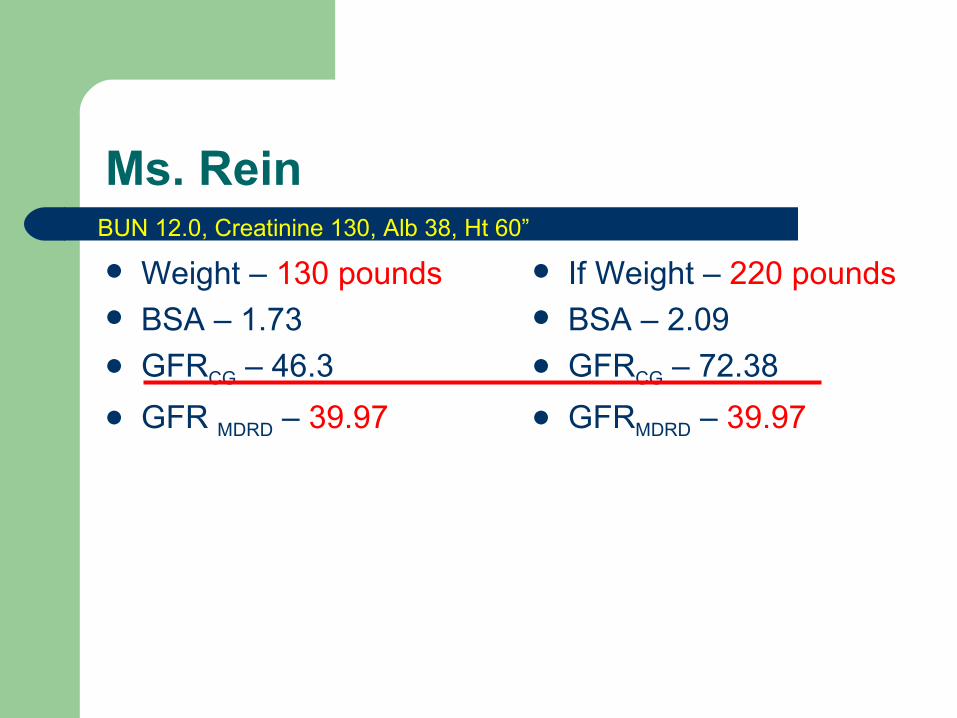
Ms. Rein
Weight – 130 pounds BSA – 1.73 GFRCG – 46.3
GFR MDRD – 39.97
If Weight – 220 pounds BSA – 2.09 GFRCG – 72.38
GFRMDRD – 39.97
BUN 12.0, Creatinine 130, Alb 38, Ht 60”
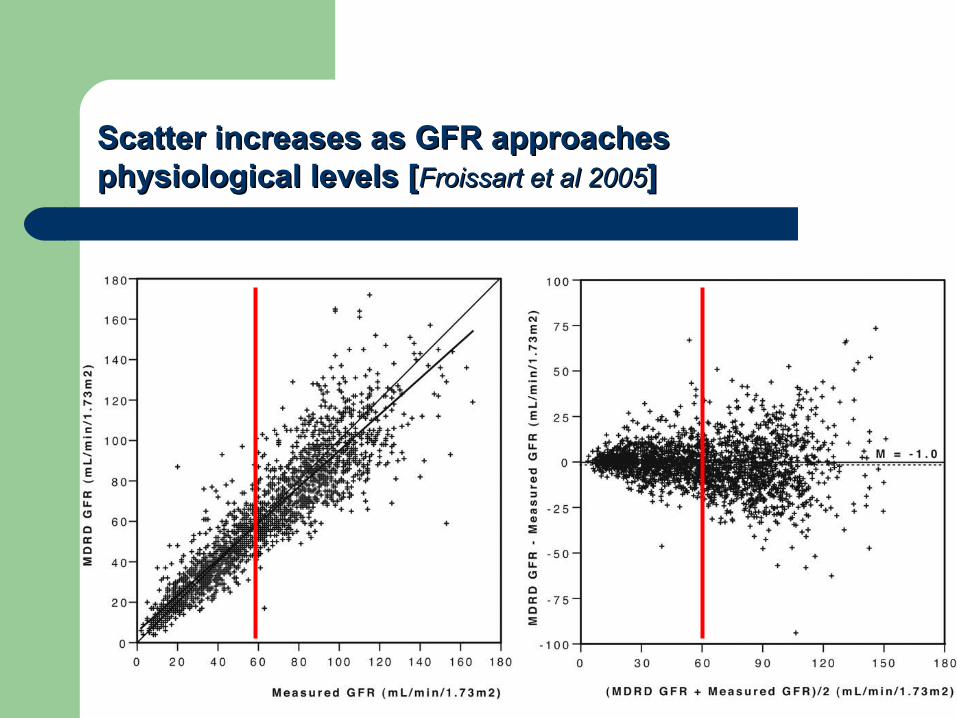
Scatter increases as GFR approaches Scatter increases as GFR approaches physiological levels [physiological levels [Froissart et al 2005Froissart et al 2005] ]
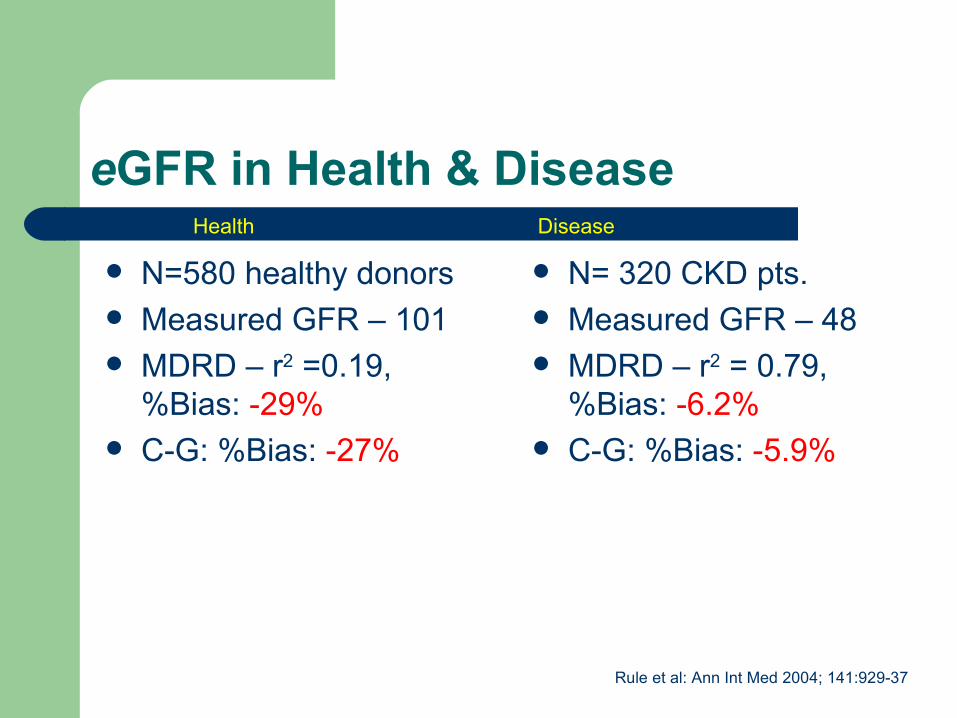
eGFR in Health & Disease
N=580 healthy donors Measured GFR – 101 MDRD – r2 =0.19,
%Bias: -29% C-G: %Bias: -27%
N= 320 CKD pts. Measured GFR – 48 MDRD – r2 = 0.79,
%Bias: -6.2% C-G: %Bias: -5.9%
Health Disease
Rule et al: Ann Int Med 2004; 141:929-37
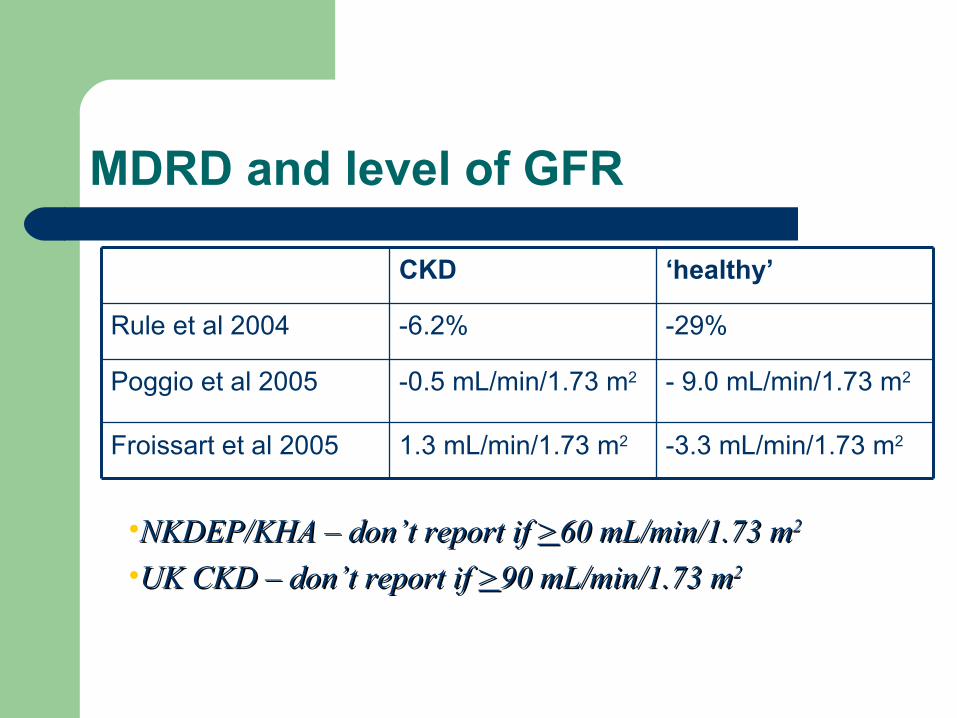
MDRD and level of GFR
-3.3 mL/min/1.73 m21.3 mL/min/1.73 m2Froissart et al 2005
- 9.0 mL/min/1.73 m2-0.5 mL/min/1.73 m2Poggio et al 2005
-29%-6.2%Rule et al 2004
‘healthy’CKD
•NKDEP/KHA – don’t report if NKDEP/KHA – don’t report if >>60 mL/min/1.73 m60 mL/min/1.73 m22
•UK CKD – don’t report if UK CKD – don’t report if >>90 mL/min/1.73 m90 mL/min/1.73 m22
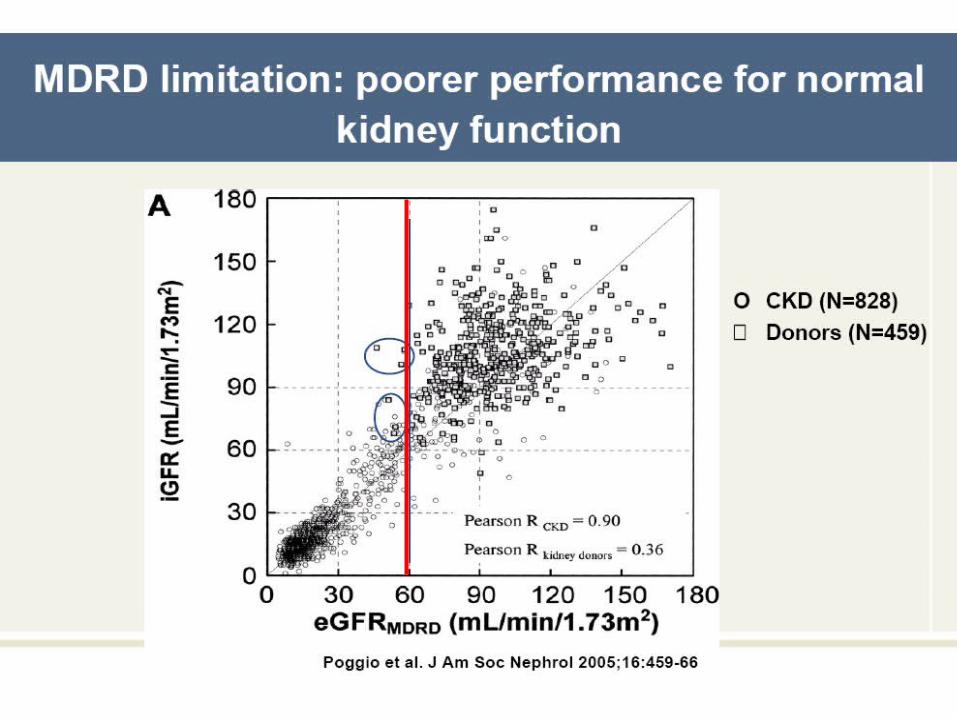
eGFR-MDRD:Limitations
NOT for DRUG DOSING! These recommendations are not to be applied to drug dosing calculations.
ASSUMES “STEADY STATE” . If kidney function is changing rapidly, monitor serum creatinine
eGFR-MDRD:Limitations
Creatinine assay subject to interferences
-acetoacetate, ascorbic acid, fructose, pyruvate, cephaolosporins, creatine, proline (avoid hyperalimentation fluid contamination), chronic lidocaine administration; bilirubin. In vivo inhibition of creatinine secretion occurs with cimetidine or trimethoprim.
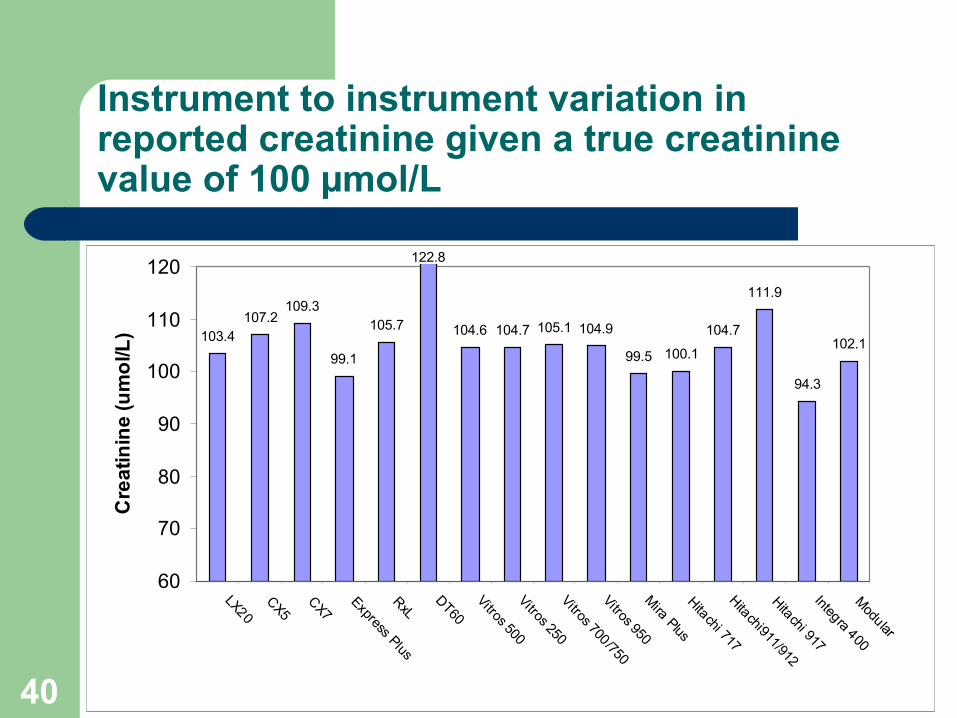
12/02/09Courtesy of David Seccombe, UBC & CEQUAL40
Instrument to instrument variation in reported creatinine given a true creatinine value of 100 µmol/L
103.4107.2
109.3
99.1
105.7
122.8
104.6 104.7 105.1 104.9
99.5 100.1
104.7
111.9
94.3
102.1
60
70
80
90
100
110
120
LX20
CX5
CX7
Express PlusRxL
DT60
Vitros 500Vitros 250Vitros 700/750Vitros 950M
ira PlusHitachi 717Hitachi911/912Hitachi 917Integra 400M
odular
Cre
ati
nin
e (
um
ol/L
)
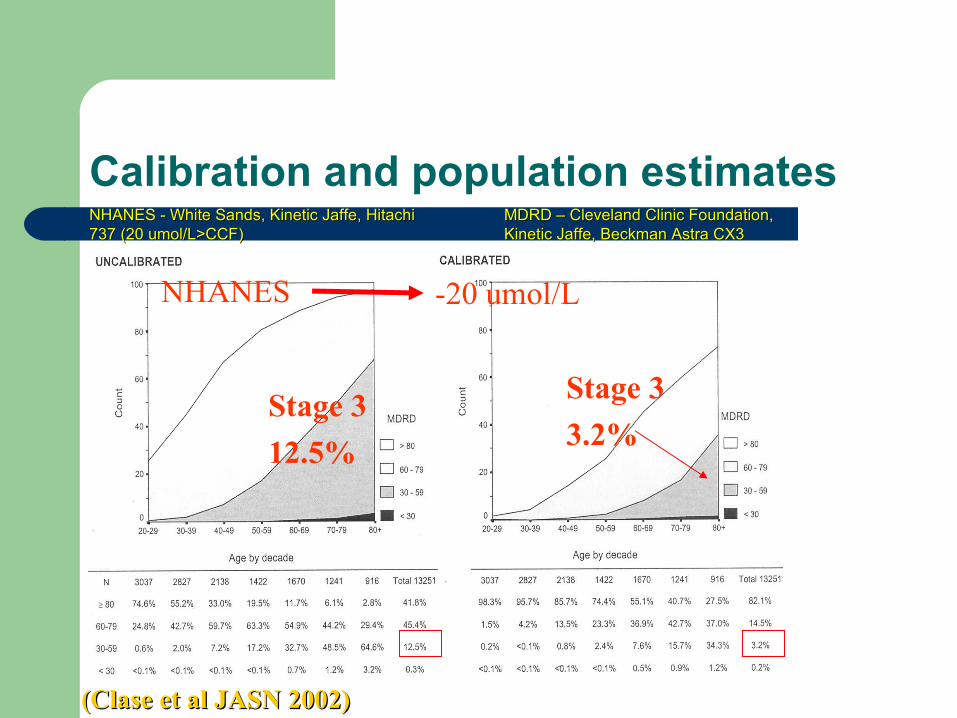
Calibration and population estimates
Stage 3
12.5%
Stage 3
3.2%
-20 umol/LNHANES
(Clase et al JASN 2002)(Clase et al JASN 2002)
MDRD – Cleveland Clinic Foundation, MDRD – Cleveland Clinic Foundation, Kinetic Jaffe, Beckman Astra CX3Kinetic Jaffe, Beckman Astra CX3
NHANES - White Sands, Kinetic Jaffe, Hitachi NHANES - White Sands, Kinetic Jaffe, Hitachi 737 (20 umol/L>CCF)737 (20 umol/L>CCF)
Creatinine StandardizationMatters
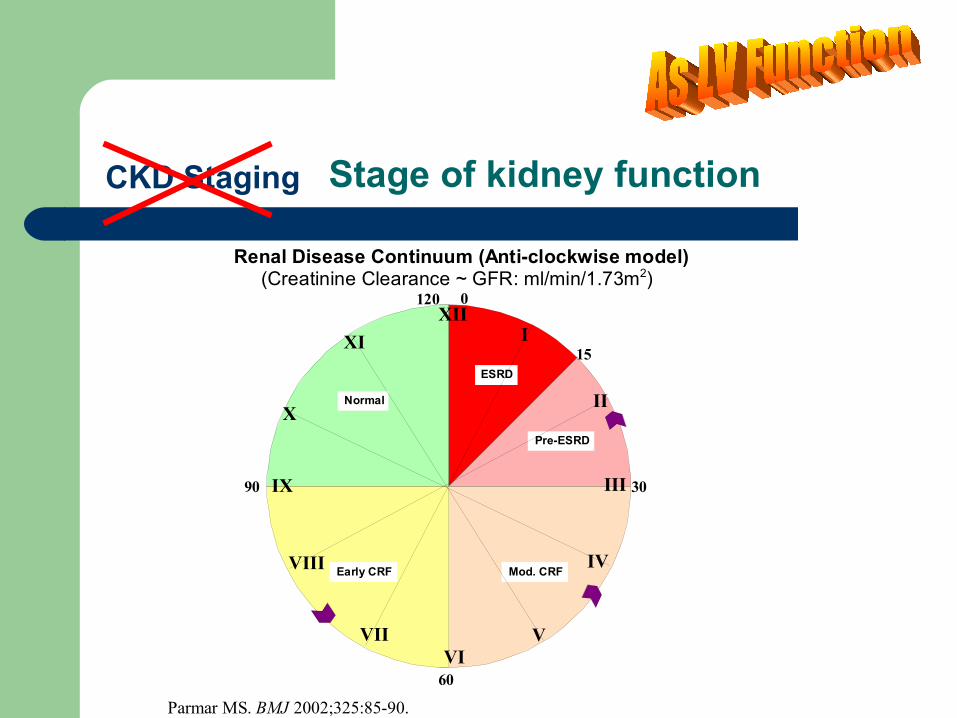
Stage of kidney function
Pre-ESRD
ESRD
Normal
Early CRF Mod. CRF
120
90
60
30
15
XII0
XI
X
IX
VIII
VIIVI
V
IV
III
II
I
Renal Disease Continuum (Anti-clockwise model)(Creatinine Clearance ~ GFR: ml/min/1.73m2)
Parmar MS. BMJ 2002;325:85-90.
CKD Staging
CKD
CKD [DN], stage 4 CKD [senile kidney],
stage 3
Diabetic nephropathy, stage 4 KF
Senile kidney, stage 3 KF
Current classification More accurate classification
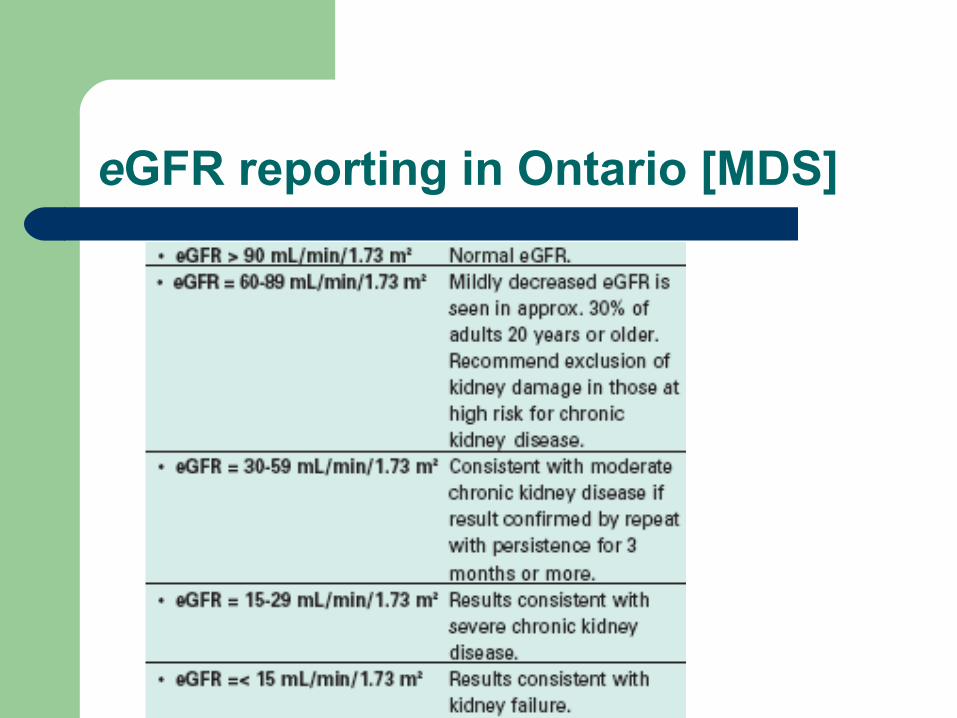
eGFR reporting in Ontario [MDS]
Not reliable – When kidney function is changing rapidly– When there are rapid water shifts– For extremes of age and weight– For amputees or paraplegic patients or diseases of
skeletal muscle– For drug dosing (eGFR is in ml/min/1.73m2)– In Pregnancy
As reliable as serum creatinine measurement
Caution(s) in the Interpretation of eGFR
Limitations
Conclusions - GFR
GFR is the best overall index of kidney function Gold-standard GFR techniques are not
practical for the entire CKD population Estimates of GFR are better/more practical
than creatinine clearance Estimates of GFR are more sensitive for CKD
than serum creatinine alone
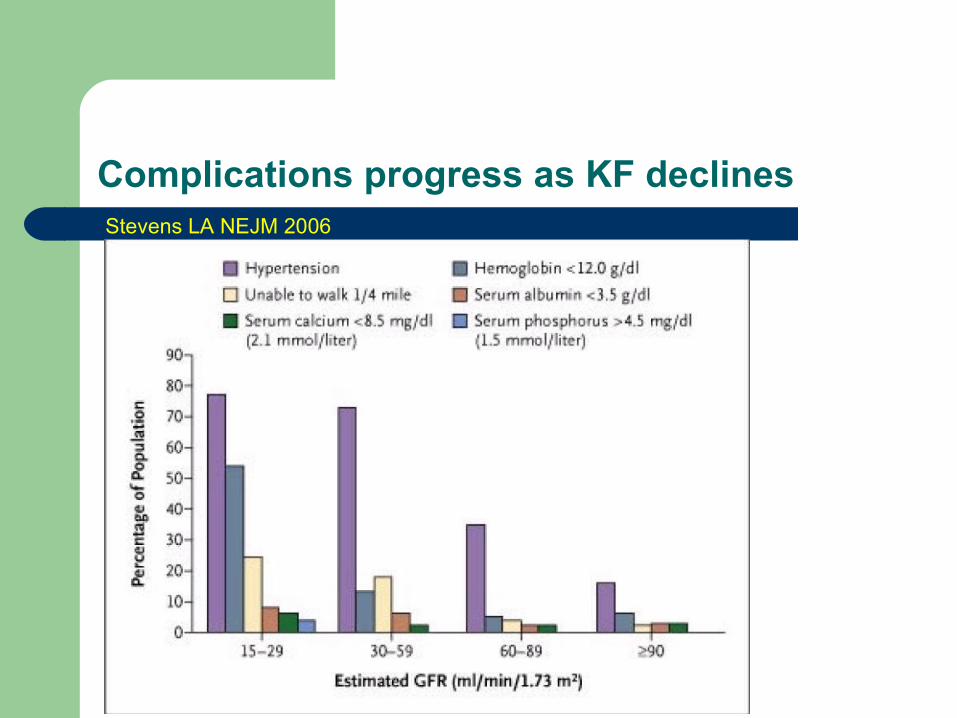
Complications progress as KF declinesStevens LA NEJM 2006
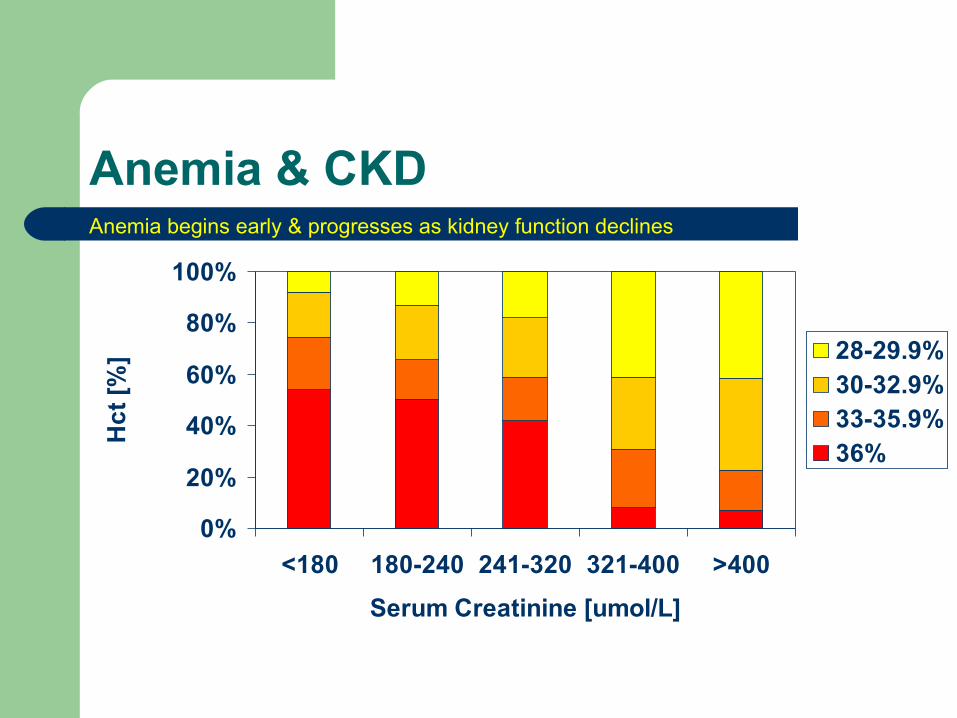
Anemia & CKD
0%
20%
40%
60%
80%
100%
<180 180-240 241-320 321-400 >400
Serum Creatinine [umol/L]
Hc
t [%
] 28-29.9%30-32.9%33-35.9%36%
Anemia begins early & progresses as kidney function declines
When to Refer
• Newly discovered CKD: All patients must undergo investigations re cause, potential reversibility of disease Refer to a specialist if the cause is uncertain
– Established, progressive decline in kidney function– Preparation for dialysis or transplantation (or both):
adequate preparation requires at least 12 months of relatively frequent contact with a renal-care team Referral should occur, at the latest, when CrCl is <30mL/min
– Other potential reasons to refer:– Proteinuria >1 g/day– The presence of complex metabolic abnormalities– Resistant hypertension in the patient with CKD
• Mendelssohn et al. CMAJ. 1999;161(4):413-17.
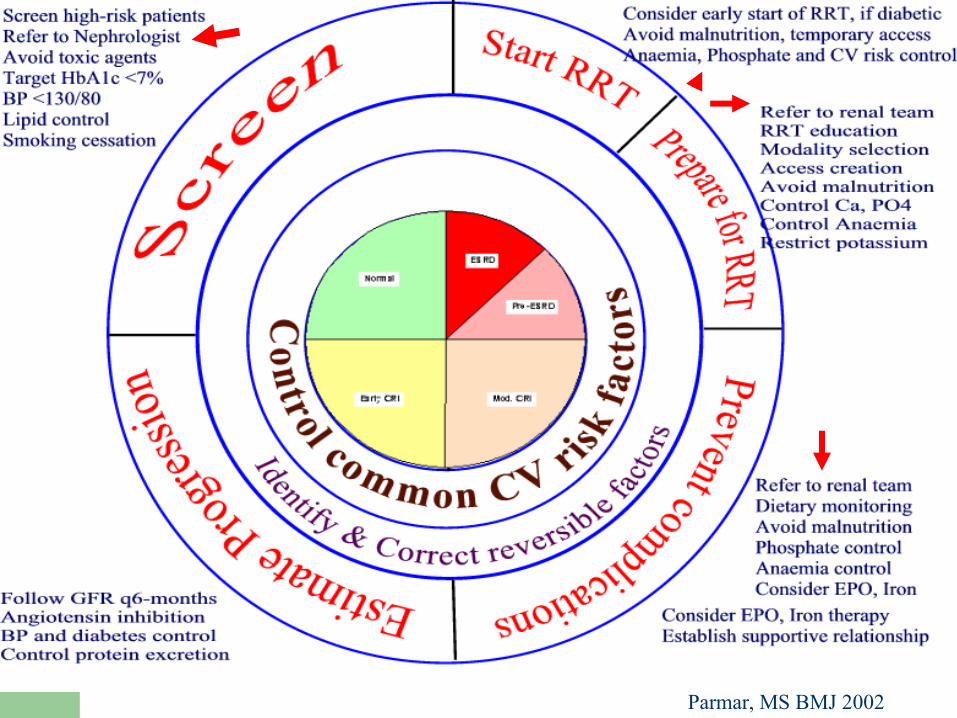
Parmar, MS BMJ 2002
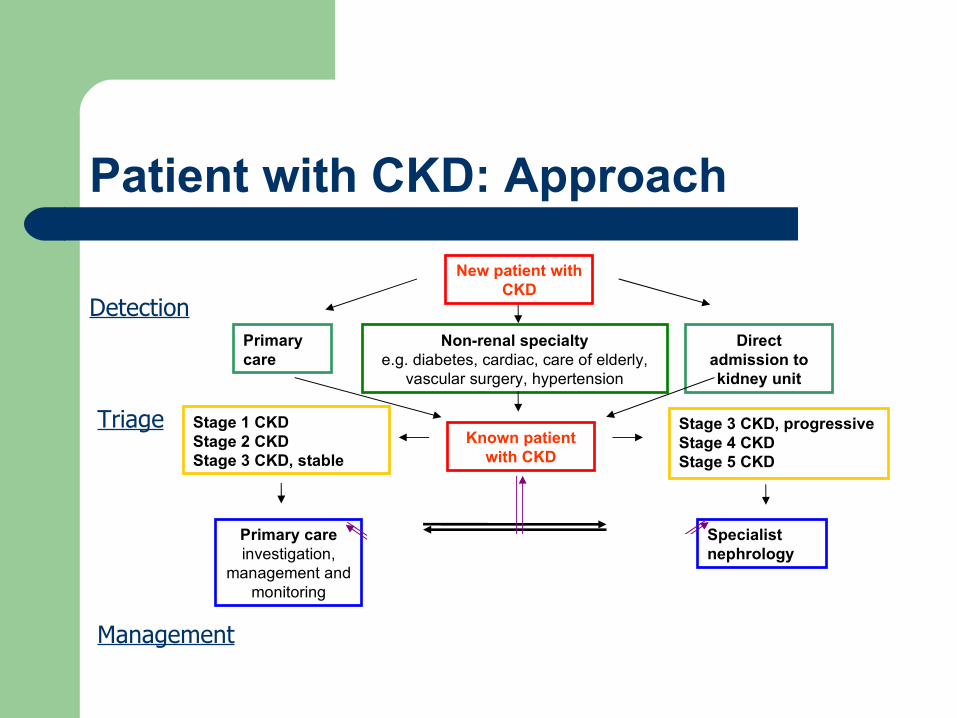
Patient with CKD: Approach
Stage 1 CKDStage 2 CKDStage 3 CKD, stable
New patient with CKD
Primary care
Non-renal specialtye.g. diabetes, cardiac, care of elderly,
vascular surgery, hypertension
Direct admission to kidney unit
Primary careinvestigation,
management and monitoring
Specialist nephrology
Known patient with CKD
Stage 3 CKD, progressive Stage 4 CKDStage 5 CKD
Laboratory results
Detection
Triage
Management
Chronic Kidney Disease
Is prevalent in general population Regardless of the cause, CKD progresses over
time to ESRD or death. Is associated with a host of co-morbidities Many of the co-morbidities develop early in the
course of CKD, and increase the risk of morbidity and mortality over the course of disease progression
Timely intervention can prevent progression and associated co-morbidities
Ms. Rein
Develops upper abdominal pain You requested a contrast CT abdomen She asks 2 questions:
– What is her risk of contrast-induced kidney damage?
– What can be done to prevent contrast-induced kidney damage?
Risk factors for Contrast Nephropathy
Pre-existing kidney disease – single most risk factor– Directly proportional to the degree of CKD– Estimated risk = Serum creatinine [µmol/L]/10
Diabetes mellitus– Likely related to underlying associated CKD– Diabetes with normal KF = Non-diabetic with normal KF– Diabetes with CKD > Non-diabetic with CKD
Volume of contrast agent used– Direct relationship with Volume of agent– Estimated volume = 440 x weight [Kg]/S. creatinine [µmol/L] – with
maximum volume of 300 ml Cardiac function Multiple myeloma
– O.6% to 1.25% [not at increased risk provided volume expansion is achieved at time of study]
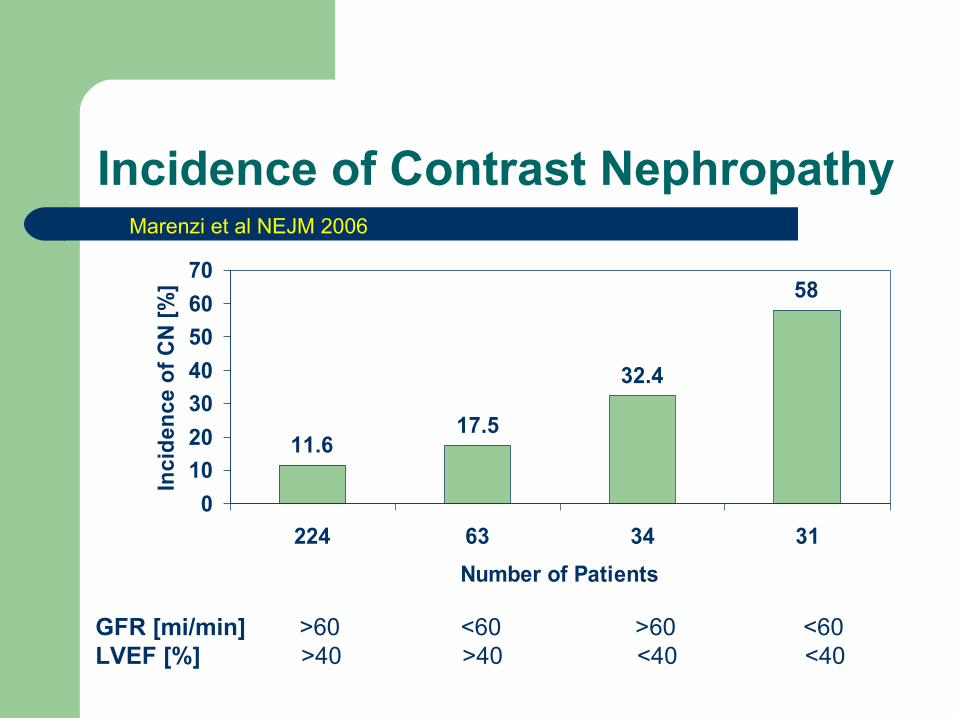
Incidence of Contrast Nephropathy
11.617.5
32.4
58
0
10
20
30
40
50
60
70
224 63 34 31
Number of Patients
Inci
den
ce o
f C
N [
%]
GFR [mi/min] >60 <60 >60 <60LVEF [%] >40 >40 <40 <40
Marenzi et al NEJM 2006
What is Ms. Rein’s risk of contrast nephropathy?
She has CKD – stage 3, eGFR 40ml/min Her serum creatinine is 130 Estimated risk based on serum creatinine is
130/10 = 13%
What can be done to prevent this risk?
Avoid NSAID – before procedure Assure adequate hydration Use of low-osmolar or iso-osmolar contrast agent
[often currently used] Use lower possible volume and not to exceed the
estimated volume Hydration – Oral or Intravenous Saline or sodium bicarbonate N-acetylcysteine – Oral with/without intravenous bolus,
what dose – high-dose or standard dose
N-acetylcysteine – Standard [600 mg BID] vs. High-dose [1200 mg BID]
Randomly assigned 354 patients undergoing primary PCI [1:1:1 ratio] either to control, or standard dose of N-acetylcysteine [600 mg IV bolus before PCI followed by 600 mg orally BID for 48-hours or high-dose of N-acetylcysteine [1200 mg IV bolus before PCI followed by 1200 mg BID for 48-hours]
20 of 354 [5.7%] pts had creatinine above 133 However, GFR <60 was present in 35 [29%] in control
group, 33 [29%] in standard dose and 26 [22%] in high-dose group [p=0.36]
Marenzi et al NEJM 2006
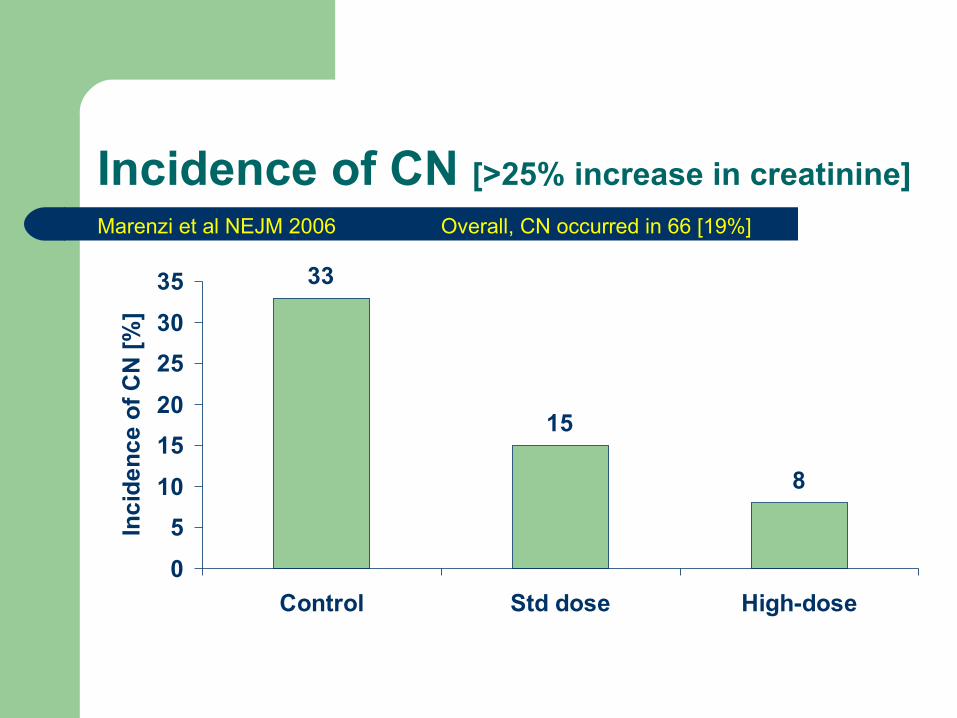
Incidence of CN [>25% increase in creatinine]
33
15
8
0
5
10
15
20
25
30
35
Control Std dose High-dose
Inc
ide
nc
e o
f C
N [
%]
Marenzi et al NEJM 2006 Overall, CN occurred in 66 [19%]
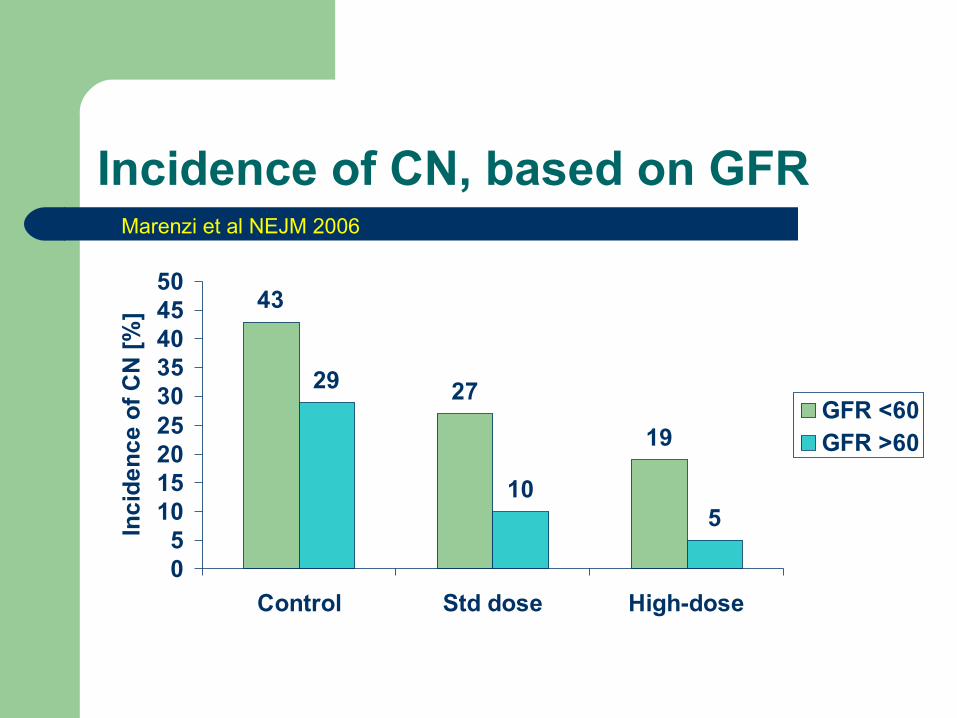
Incidence of CN, based on GFR
43
27
19
29
105
05
101520253035404550
Control Std dose High-dose
Inc
ide
nc
e o
f C
N [
%]
GFR <60GFR >60
Marenzi et al NEJM 2006
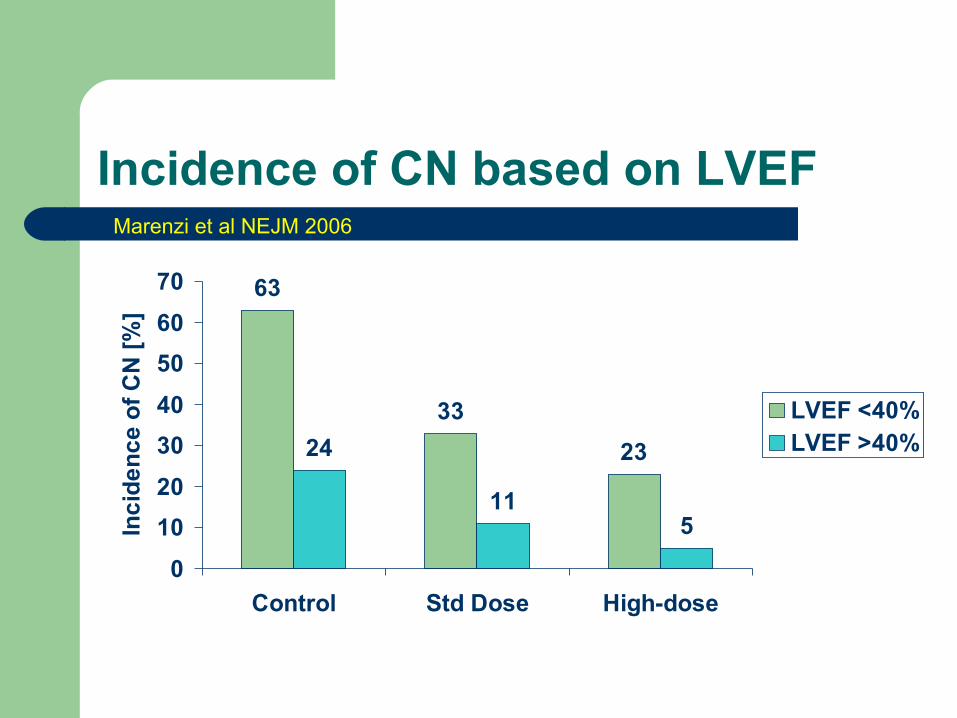
Incidence of CN based on LVEF
63
33
2324
115
0
10
20
30
40
50
60
70
Control Std Dose High-dose
Inc
ide
nc
e o
f C
N [
%]
LVEF <40%LVEF >40%
Marenzi et al NEJM 2006
Thank you“A classic is a book that has never finished saying what it has to say”
Italo Calvino (1923-1985), Italian Writer
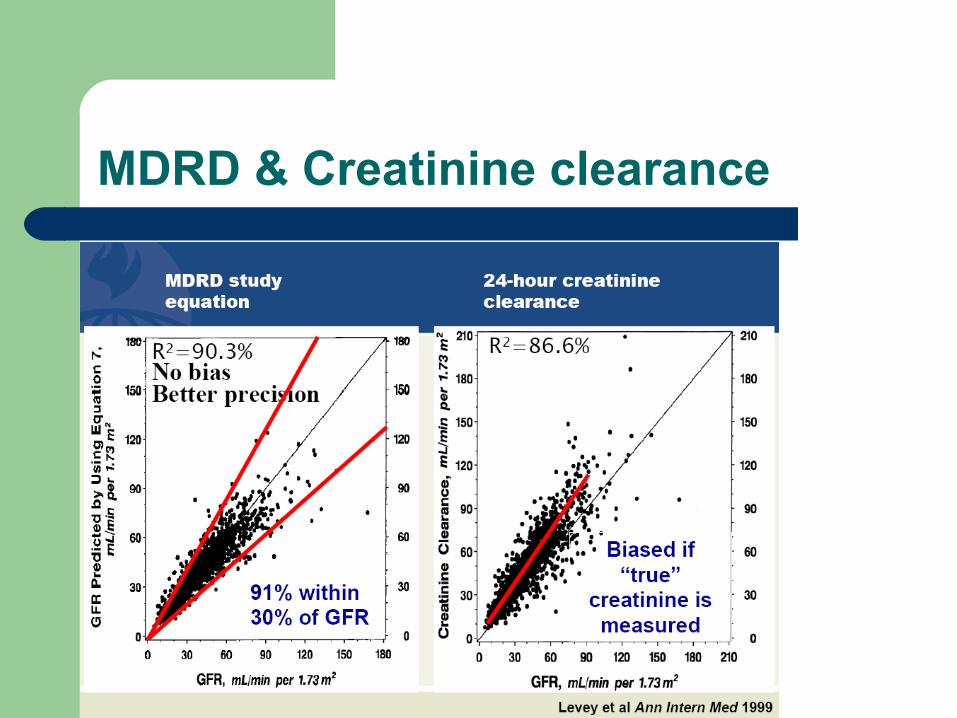
MDRD & Creatinine clearance
eGFR-MDRD:Limitations
In the MDRD study:
91% of eGFR results were within 30% of their true values.
98% were within 50% of their true values