
E course functional masticatory system in virtualclassroom
40
Page 1 of 40 Functional Masticatory System (FMS) In Virtual Classroom. Olufemi Jeremiah Olubodun (CDT, Pg. Dip. Education; Pg. Dip ICTs (Ed), Pg. E-Teaching, M.Ed) Faculty of Dental Sciences, Department of Restorative Dentistry, University of Lagos, Lagos Nigeria. [email protected] , [email protected]
-
Upload
olufemi-jeremiah-olubodun -
Category
Health & Medicine
-
view
72 -
download
0
Transcript of E course functional masticatory system in virtualclassroom

Page 1 of 40
Functional Masticatory System (FMS) In Virtual Classroom.
Olufemi Jeremiah Olubodun (CDT, Pg. Dip. Education; Pg. Dip ICTs (Ed), Pg. E-Teaching, M.Ed)
Faculty of Dental Sciences, Department of Restorative Dentistry, University of Lagos, Lagos Nigeria.

Page 2 of 40
ABSTRACT This paper delineated a short course named Functional Masticatory System into modules for delivery through a learning technology (Fonter) as against the original format (Standalone) in order for the course to be taken interactively by undergraduate dental students and hopes to proof to its readers the possibilities of delivering a life science course fully online. There shall be a teacher whose role will change from imparting knowledge to a moderator of learning activities. I therefore attempted to structure a study guide as a working tool for the learner to go through the course materials derived from the original work of a team of dental educators at the World Health Collaboration centre for Oral Health Care Planning and Future Scenarios, College of Dental Science University of Nijmegen, The Netherlands. (WHOCC). I introduced the course in the background section of this paper in order to open-up readers to some details about the course by explaining some important concepts and practices behind the making of the study guide and with some other details on making the guide workable. This e-course was divided into four modules and each module is divided into tasks, activities, and resources sections in the overview table below. The simplification of the course materials provides the student the opportunities of learning the course in modules and therefore space their participation in a flexible way. The students are expected to look up resources in the Internet for journals and scholarly articles to complement minilectures given for each module.
INTRODUCTION This paper examines the course materials which were originally prepared by WHOCC team under the headship of Professor Nico Creugers. It was prepared by adapting course materials for a self-learning methodology where a learner interacts with an already made course materials namely: video, audio, text, and illustrations etc in order to understand the course contents all in a CD. The course was a product of well-researched study on the masticatory functions of the human oral system. One major objective of the self-study course is to reach as many dental professionals as possible around the globe on the concept of how the oral system could function efficiently with a view to addressing arising changes, and mal-functionality due to ageing, and pathology etc. Like any self-study courses the learner is alienated- it is him and the computer. It is however well-represented in the literatures that collaboration among teams resolves the feeling of alienation of the student unlike in self-study approaches (Jaques, D & Salmon, G. 2003). The study guide which was derived from the courses contents in the CD below is the new format in which the course materials were presented so that it will be possible to have a class cohort work on the course activities in a learning management system (LMS) that is meet in a virtual classroom in order to carryout the outlined activities. The study guide is a self-driven outline of tasks and activities derived from the original course materials. The modules are interdependent and in coordinated arrangement in the present outline. The difference between the original materials and the present one is that the study guide is a delineation of the original materials into learnable units for ease of learning for virtual learning environment. It is the responsibility of the e-tutor to adapt course materials for virtual learning environment for learners to take the course by interacting with course materials and one another using the tools available within the LMS for discussion and undertaking outlined tasks and activities without the e-tutor imparting knowledge. It is therefore a strategic tool for the tutor to guide learners in what to do without restriction on scope and contents. The e-tutor in his new roles moderates online activities including assessment of students’ performance as well as stands by as a guide for occasional intervention if need be. The basis of this approach is named socio-constructivist pedagogy where it is the responsibility of the learner to construct knowledge as a result of social interactivity amongst learner and with learning objects. He is a knowledge ‘constructor’, taking charge of his learning, while the tutor in this situation supports the learner which is why it is called study guide not a syllabus with its characteristic restriction as we have in traditional learning. Although the learner is presented with a study guide but he is not restricted on what and what he should do with the course materials. Socio-constructivism is therefore a concept that explains knowledge construction by the learner among group of learners (Wikipedia, 2008).

Page 3 of 40
According to Olubodun, O.J. (2008) ‘A study guide in this context is an online tool that the tutor prepares by delineating the contents of the curriculum in simple, interpretable and learnable units which may be reviewed by the institution, or the students in the course of running the course. It is a document for the learner in which all tasks, activities etc are suggested but not restricted within a flexible time frame for the course contents to be undertaken in order to reach the course objectives and the award of credits. It is a self-driven document that works on the principles of socio-constructivist pedagogy which places the learner in the centre of learning process with the teacher only playing the roles of a moderator of learning events. It is a suitable tool for collaborative activities where contents are delivered 100% via a Learning Management System (LMS).’
What makes the study guide work as a strategic tool?
1. It encourages collaborative activities 2. It promotes individual abilities to grow self-managing competences and confidence. 3. It works on flexible schedules that allow learners to take possession of their learning. 4. Study units are presented in short, precise, workable and hence easily understandable
style. 5. Study units are prepared to be interdependent, cohesive and correlated. 6. Each module and subunits have allocated credit units for learner to measure progress,
plan activities of learning and self-assess own work. 7. It is an assessment tool just as well as a study tool etc.
BACKGROUND The subject of occlusion continues to be of interest from the early days in the dental school both for undergraduate dental surgery or dental technology students and in our daily professional practices as dental operators and educators. To new dental students occlusion may just mean closing of the patient’s upper and lower jaws when the teeth are in close contact, and in interdigitated position. This write-up will endeavour to discuss occlusion from functional characteristics and in relation to the possibilities of impairment. Why study occlusion? The relationship of the upper and lower jaws sometime fails due to loss of teeth, dislocation due to accident resulting in the fracture of the bone of the jaw or the temporo-mandibular joint (TMJ). In any of these cases functional occlusion may be impaired. Where tooth loss is recorded the procedures for restoration are various and the options and practices in the type of material and appliance depend on the choice the patient makes and the experienced decision of the dental operator. However, the overall objective in the treatment plan will among other things be to decide on the best option on appliances and method that will restore the patient back to normal life with minimal alteration to his mastication and oral functions. The dental profession however relies on the adaptive capacity of the oral cavity and hence need only to ensure decisions are made on the best material, appliances and method for maximizing its gains. Needless to say that the occlusion concept is relevant to the dental clinic and the laboratory as concerted efforts are always required to produce the best result. A malfunctional occlusion commences from dysfunction of the stomatognatic system, but this dissertation will concern itself with the impact of tooth loss on impaired dentition rather than overall consequences of dysfunction of the stomatognatic system. Dysfunction of occlusion An abnormal function of the masticatory system poses lots of challenges. It is often a subject of concern especially when complex cases ensues that requires fabrication of a dental restoration. A functional occlusion is a multi-contact function of the occlusal surfaces of the teeth in the oral cavity when the upper and lower jaws are in dynamic relationship. This therefore does not suggest that when some teeth are missing in the mouth we could not describe functional

Page 4 of 40
occlusion. It is true that missing teeth do not suggest unhealthy occlusion so also functional occlusion is not a description for a situation when all the teeth in the mouth are present (Creugers, Net al 2003). Functional occlusion is therefore when the upper and lower jaws are in dynamic relationship regardless of the number of teeth in the mouth while the teeth maintain multi-contact functionality. Occlusion however could be centric, lateral, protrusive, and retrusive when respectively the occluding surfaces maintain maximum contact; the mandible maintain left and right positions to the centric occlusion; the mandiblular teeth maintain anterior position to the centric occlusion; and the mandibular teeth maintain posterior position to the centric occlusion. In any of the above descriptions of occlusion it could be traumatic when for instance there is a loss of some number of teeth especially posterior teeth and they are not replaced within a short time which may alter the patient’s masticatory pattern or when teeth in a denture are badly arranged resulting in stress due to uneven distribution of masticatory load during mandibular movement. A dental appliance should therefore be able to resolve difficulties arising from malfunction of the mandible due to tooth loss which also may affect the TMJ. The number and type of teeth that may be missing before the said malfunction could occur could begin with one tooth except the wisdom teeth. The resultant effect of drifting or supra eruption of teeth alters their angulations which could alter patient’s original mastication and hence occlusion which could give rise to dysfunction of the stomatognatic system. Functional disturbances can be present in both impaired and complete dentitions. ‘An impaired dentition is a dentition of which one or several teeth are missing’ (Cruegers, N. et al 2003). Stomatognatic system and occlusion
The failure of the stomatognatic system to meet the functional demands of an individual is a description of dysfunction of occlusion. A dentition is therefore functionally disturbed ‘when the adaptive capacity of the individual is exceeded. When an occlusion is functioning well, there is equilibrium between occlusal stability and applied forces. This equilibrium is a dynamic balance and tooth loss might disturb this balance. The disturbance can be temporary: teeth will migrate; the patient will adapt his functional level (chewing etc) until a new equilibrium is attained. But in some cases the adaptive capacity of patient is too low and the occlusion becomes functionally disturbed’ (Creugers, N et al, 2003).
Consequences of tooth loss. The early stages of human growth give rise to probable causes of disturbances in the development of the dentition which may affect the growth of the dentition e.g. hypopasie, amelogenesis imperfacta or in cases of complete dentition; agenetic. Poor oral hygiene may lead to periodontal diseases arising from the growth of plague and eventual loss of teeth. The roles of excessive bruxism, trauma, smoking etc are other causes of tooth loss. Tooth loss may lead to imbalances in occlusion with arising restorative demands. Other considerations Ideally natural teeth and the entire oral cavity are due to serve for a life time but failure arises due to natural and un-natural causes and it is the responsibility of an individual to submit himself to routine oral hygiene habit and checks to forestall failure. Inability to comply with the necessary healthy habit may give rise to deficiencies and eventual failure of the oral system. Practices like eating healthy foods will be advisable but when processed foods like biscuit are consumed without commensurate cleanliness of the teeth and observance of routine checks the oral cavity’s stability is jeopadised causing failure. Other oral health maintenance practices e.g. fluoridation as a preventive measure against tooth decay may be helpful in a redeemable situation but where bacterial activities are initiated and concentrated the affected site of the tooth may damage resulting in caries, tooth decay , periodontal diseases and eventual loss. METHODS AND MATERIALS The study guide was drawn based on the course material for Pedagogy for online learning short

Page 5 of 40
course of Global Virtual University Japan. Course materials were delineated into modules while each module into ‘task, activities, resources, and minilectures. The modules are derived from the course materials from the CD and are crafted into subtopics with clearly defined objectives. The roles of the tutor among other things are to study the topics from the original materials and re-adapt it for online learning. In other to ensure the success of the study guide additional tools are added to support the learner both in undertaking the course and in the assessment of the activities on the course. These tools are:
Study calendar
Rubrics
Course description. The minilectures are introductory notes for each module. The purpose is to give short but precise details on the module so that the course registrants will be guided and directed on the extent of coverage of contents etc. The study calendar (Appendix I) further stretches what the learners are expected to do on the activities and the time schedules within which the course is expected to come to completion. The Rubrics (Appendix II) is an information gathering tool on student participation and performance on the course. The course description (Appendix III) is a document that spells out short details for each module, credit worth, offering institution, and mode of course delivery etc. The learner uses the guide as a work plan from module to module by undertaking the contents according to the time schedules in order to earn the stated credits.

Page 6 of 40
Module 1
HEALTHY OCCLUSION (Minilecture)
Healthy occlusion when compared with normal occlusion redefines what is preferably
referred to as ideal occlusion, which Ash and Ramfjord (1995) described as rare. A
healthy occlusion possesses some identifiable characteristics, which are considered along
functional and biological criteria.
What can be defined as healthy occlusion fall within a range of consideration, which
makes a dentition with ‘for example inter dental spaces a large horizontal overlap or
missing molar still (can be) healthy’. So variations in anatomy of the stomatognatic
system or an ‘incomplete dentition is not a direct indication for treatment’. However
because of the variability of the stomatognatic system and individual demands on his
dentition there are standard considerations for the treatment of prosthodontics patient.
The criteria as listed below by Creugers, N et al. 2003:
“A complete dentition contains 28 teeth, the third molars not included.
Influence of muscles (lips, tongue, cheeks) on the arch form, tooth position and
stability.
Horizontal and vertical overlap.
The standard is that anterior teeth of the lower and upper jaw have an overlap of
1-3 mm for both the vertical and horizontal overlap.
Apparent teeth at rest and when smiling.
The average maxillary display with the lips at rest is 1.9 mm in men and 3.4 mm
in women. Younger people display more maxillary tooth structure than middle-
aged and older patients. Also important in prosthodontic treatment is the vertical
and horizontal smile line; does a patient display much gingival tissue and what
teeth are displayed when smiling?
Symmetry of the upper front teeth.
In the ideal situation the dental midline coincide with the median line of the face.
The upper front teeth should be symmetrical in shape and alignment. However,
the goal is to achieve a balance between idealism and diversity because in a subtle
way natural dentitions are always asymmetrical.
Sagital and transverse relations
An Angle Class I relationship can be seen as the standard.
Changes with aging
Wear of teeth is one of the processes that can be seen in a dentition of an older
person. It is difficult, however, to define clearly the fine dividing line between
what can be seen as caused by age or pathology (Crothers, 1992).

Page 7 of 40
Static and dynamic occlusal relations.
A dentist should be aware of the morphological characteristics of the different
tooth types and the force distribution in different occlusions”.
For prosthodontics patient, two important objectives are likely in focus depending on the
problem diagnosed. If anterior teeth are missing then esthetic and speech remain the
focus of treatment decision. On the other hand if it is chewing difficulties arising from
loss of some posterior teeth the restoration of occlusion and chewing functions will
dictate the treatment options. The above categorization can be summed up into what can
be referred to as functional characteristics of the teeth as component of the stomatognatic
system.
Functional units have two parts namely: Occlusal and aesthetic units. All aesthetic
considerations involve the anterior teeth (esthetic units) while occlusion issue involves
the premolars and molars in posterior teeth (occlusal units).
According to Creugers, N et al. 2003 “The teeth never function separately but always in
pairs”. Therefore “the antagonistic unit is called the functional unit”. In the table below,
which shows the various functional units and their relationship, “one antagonistic molar
pair is considered equivalent to two antagonistic premolar pairs. If not specified from
now on occlusal units are counted in premolar equivalents”.
Location Name Number
Anterior area Esthetic units 6
Premolar area Occlusal units 4
Molar area Occlusal units 4 (8*)
Total Functional units 14 (18*)
* in premolar equivalents (Creugers, N et al. 2003).
Table 1.1 Functional Units
A look at the posterior (occlusal units) and anterior (esthetic units) teeth shows as
depicted in table below the varying functional roles different tooth types play in the
mouth.

Page 8 of 40
Anterior teeth Premolars Molars
Biting + - -
Chewing - + +
Speech + - -
Esthetics ++ + +/-
Stability/support
TMJ + + +
Dental arch + + +
+ = primary involvement
- = no or secondary involvement (Creugers, N et al. 2003)
Table 1.2 Functional assessments of the different tooth types.
It is important therefore to state that ‘the more occlusal units are absent the more difficult
it is to define the lines between a healthy occlusion and an unhealthy occlusion’. A
healthy occlusion should therefore perform the chewing, esthetic and parafunction roles.
The study of occlusion is made clearer with the clarification of some terms within all
considerations that relate with the movement of the mandible. These movements are
determined by the ‘anatomic structures like teeth ligaments, TMJ and muscles’, which
are explained in Posselt diagram below:
Mandibular border movements
in the saggital plane.
R = rest position
RCP-T = rotational hinge movement
opening
CR = centric relation
IP = intercuspal position
RCP = retruded contact position
RCP-IP = slide in centric Posselt diagram
P = maximal protrusive movement
O = maximal opening
T-O = translation phase of opening

Page 9 of 40
R-IP = habitual closure
(Creugers, N. et al. 2003)
The above analysis and discussion emphasise contemporary approaches on the concept of
occlusion but there existed past concepts which still guide today understanding of the
concept of occlusion.
Monson’s sphere and Bonwill’s triangle are among the earliest concepts which guide
dentist on the guidelines for balanced occlusion.
“Balanced occlusion is the occlusion in which simultaneously equal contacts are
maintained among opposing tooth surfaces throughout the entire excursion” Other
concepts include the concepts formed by a group of dentists in 1926 and they called their
society Gnathological Society of California. They rely on the study of the reproduction of
the Temporomandibular joint (TMJ) movements as guide in achieving balanced
occlusion. This society later reconsidered a modification of gnathological concept which
metamorphosised to mutually protected occlusion and the concept that follows namely
group function occlusion.
Another concept is named functionalism: “In this concept maximal inter-cuspation takes
place in the retruded contact position and intercupal position and in the distance between
these two positions (free centric)”. In anticipation on this free centric, one favoured
point-contact opposite flat planes during maximum inter-cuspation”
In attaining healthy occlusion Creugers, N et al. (2003) suggested the following important
considerations:
“Absence of pathological manifestations in all parts of the stomatognatic
system (teeth, periodontium, muscles and Temporo Mandibular Joint (TMJ)).
Satisfactory function/oral comfort, a healthy occlusion meets a person’s
individual demands in a satisfying way on for example chewing and esthetics.
Variability in form and function; a healthy occlusion can present itself in
many different ways.
Adaptive capacity; the stomatognatic system has the ability to adapt to
changing circumstances.
The ability of a biological system to re-adjust to its surrounding keep it in continuous
function and survival. The ability to readjust counts on age, psychological attitude, state
of the tissues and it differs from the various adaptive mechanisms of the stomatognatic
system which are hereby considered and related.

Page 10 of 40
Location Adaptation mechanism
Teeth Attrition
Periodontium Increase in mobility
Migration
TMJ Remodeling
Muscles (CNS) Changes in contraction pattern
Tongue Interposition in diastema
Table 1.3 Adaptation mechanisms of the stomatognatic system (Creugers, N et al.
2003).
Adaptive capacity could be represented in the listed situations
1. Adjustment of the morphological and/or function, muscles contraction pattern, the
alveolar bone and the TMJ. The young people mostly responded faster.
2. Attrition of teeth: Teeth migration, wear and muscles contraction pattern common
among adult.
3. Eating slower.

Page 11 of 40
Module 2
THE IMPAIRED DENTITION(Minilecture)
An impaired dentition is a case posing challenges in oral function arising from loss of
‘one or several teeth’ in an arch or aches distorting the combined functions of the
components of the stomatognatic system. The chewing mechanism is impaired with loss
of a molar or more while “missing anterior teeth will occasional lead to esthetic and
phonetic problems” but because of the eating of refined food missing molars may not
have to lead to chewing problems.
Impaired dentition therefore could mean any of the following:
1. Shortened dental arch (SDA)
2. Tooth loss (bound or free-end space)
3. Combination of 1 & 2 above.
An individual whose demands are not met in terms of coping with distortion in the
adaptive capacity arising from manifested problems in the stomatognatic system (teeth,
periodontium, muscles and TMJ) is said to have a ‘functionally disturbed occlusion
which can lead to cracked tooth syndrome, tooth-wear, tooth mobility, muscle ache, joint
arch and joint wear’.
Causes of impaired dentition:
1. Disturbances during development stages of dentition (hypoplasie, amelogenesis
imperfecta, agnetic)
2. Poor oral hygiene resulting in caries and periodontal diseases leading to tooth
loss.
3. ‘Failing dental care has negative influence on the dentition’.
4. Trauma, excessive bruxism, smoking causing periodontal problem without regard
to adaptive capacity of the stomatognatic system and due to lack of full
understanding of this situation
The loss of a tooth was thought to “ultimately lead to the degradation of the entire
occlusion”. Today “the loss of one or more teeth leads to a disturbance of the functional
balance of the remaining teeth (Kayser, 1996) and the structural and functional changes
that follow… may be considered an adaptation on one hand and on the other pathological
condition. It is difficult to define the line between pathology and adaptation”.
See the table below and discuss the various functions of their absence in different regions
of the mouth.

Page 12 of 40
Function
Tooth loss
Anterior Premolar Molar
1. Beginning of digestion
Biting Yes No No
Chewing No Yes Yes
Taste No No No
Swallow No No No
2. Communication
Speech Yes No No
Mimics Yes No No
Esthetics Yes Yes Yes (?)
3. Stability
Dentition Yes Yes Yes
TMJ No No Yes
4. Parafunction
Clenching and grinding ? ? No
Table 2.1 Will tooth loss in a specific region have consequences for oral function?
(Creugers, N et al. 2003)
The changes as shown in the table above are influenced by a number of factors, which
could be broadly placed in two headings thus:
I. Local factors e.g. number of missing teeth, location etc.
II. Systemic factors e.g. age, general health etc.
Often it is believe that loss of a tooth can lead to mandibular overclosure, increased
pressure on the joint, alteration of the condyles and consequent Temporomandibular
Disorder (TMD) but “studies failed to demonstrate any relationship between missing of
molar support and signs and symptoms of TMD except for osteo-arthrosis in the TMJ
(Pullinger et al, 1993). Except in cases of extreme SDA (only anterior support) TMD
were reported” (De Kanter, 1990). The capacity of the stomatognatic system to adapt to
loss of molar seems to be great (Kayser, 1996).
Bilateral premolar supports and provides sufficient mandibular stability and prevents
TMD.
In addressing impaired dentition it is important to understand its patterns namely partially
dentate situation with tooth-bound spaces and shortened dental arch. This situation gives
rise to a number of problems, which can be complicated or non-complicated.

Page 13 of 40
Module 3
SHORTENED DENTAL ARCH (Minilecture)
In the past it was believe that every lost tooth must be replaced but current studies as
supported by the works of Elderton (1993) and Kayser (1987) concluded that replacement
of every single tooth lost could lead to overtreatment and hence have iaotrogenic side
effects. Loss of teeth in the mouth as a result of physiological and pathological
consequences could lead to SDA as defined thus:
“A Shortened Dental Arch (SDA) is a dentition with reduction of teeth starting
posteriorly. An SDA-dentition with all anterior and premolars present is called a
premolar dentition. This dentition consists of four (4) occlusal units”. (Creugers, N et al.
2003).
The number of posterior teeth missing in an arch determines the length of SDA, which
does not necessarily make the dentition unhealthy.
How many teeth are at least needed to come up to the criteria of a healthy occlusion?”
Find below a table that gives varied details as consequent of work of some notable
researchers on functional assessment of different tooth types answering the question on
what a healthy occlusion is.
Study Number of teeth
Haraldson & Carlsson, 1979 ‘median of 9 pairs of occluding teeth’
Agerberg & Carlsson, 1981 ‘20 well-distributed teeth’
Käyser, 1981 ‘discomfort begins with < 10 pairs’
Cushing & Sheiham, 1986 ‘no problems with ≥ 20 teeth’
Leake et al., 1994 ‘no need to replace if 3 or more posterior
functional teeth are present’
Rosenoer & Sheiham, 1995 ‘people were satisfied even with all molars
missing’
Table 3.1 Functional assessments of the different tooth types. (Creugers, N et al.
2003)
On examination of SDA can still be healthy and that “missing posterior teeth are not very
important from a subjective aspect” and that premolars can still render similar functions
as molars so they do not have exclusive function (Kayser, 1981). Although SDA case
could still be healthy but the following changes among others may still take place:
Increased vertical overlap (overbite)
Decrease in mastication

Page 14 of 40
Increase occlusal wear etc.
Further studies pointed at different conclusions which among other things states that SDA
could provide satisfactory oral functions and comfort. SDA could provide enough
mandibular support to prevent TMD symptoms etc (Witter, 1994 Par I & II).
The WHO (1992) oral health strategy states. “The retention throughout life of a
functional esthetic, natural dentition of not less that twenty (20) teeth and not requiring
prosthesis” remains her definition of primary aim of dental care.
The molars present highest risk of plaque deposits, and hence are “The most frequently
extracted teeth” (Eckerbom et al. 1992, Sheiman, 1997& Brown et al, 1989).

Page 15 of 40
Module 4
TREATMENT PLANNING (Minilecture)
There are quite challenging facts presented by researches on the need to have dental
treatment but it is important to note that these needs are various and can be guided along
the following considerations:
1. The satisfaction of people with depleted dentition
2. Satisfaction with as low as four (4) occlusal units in the mouth
3. Satisfaction of ‘people even with all teeth missing’ (Rosenoer & Sheiham, 1999)
4. Satisfaction when ‘three (3) or more posterior functional teeth are present’
(Leake, et al, 1994).
These are challenges, which provide bases for treatment variability in addition to the facts
that several subjective and objective factors play significant roles which could be linked
to the following:
_ the Patient (“…his physic, physical and financial possibilities embodying his personal
gains and desires-age, health’)
_ the dentist (“…his knowledge and practical possibilities…Moreover, the availability
and capacities of a dental laboratory will influence treatment planning”). A dentist “was
educated with a ‘philosophy of treatment’ within his dental school and so has certain
convictions”
_ the health care system (Health care differs in every country e.g. insurance coverage
can be persuasive… for a certain treatment option).
_ oral health (‘Oral hygiene and motivation to change habits; caries activity; periodontal
problems; occlusal problems; bruxism; degree of impaired ness and Angle class are the
basic dental problems’).
_ scientific knowledge etc. (‘Provided evidence concerning restorations and
prosthodontics appliances influences the different views of treatment’).
(Creugers, N. et all 2003).
If there is no problem in oral function then why start treatment? Teeth should only be
replaced if a problem can be solved. This approach is called problem-oriented treatment
planning. “Problem solving treatment is a way to organize a patient’s treatment in a
predictive and systemic order” (WHO Collaborative Centre for oral Health care planning
and future Scenarios, 2006).
However the treatment option that adopts problem-solving approach will require a step-
by-step strategy that may involve first of all an information gathering technique and other
steps as listed in the table below:

Page 16 of 40
Phase Problem solving approach
1 Gathering information
2 Recognition
3 Problem listing
4 Treatment strategy
5 Preliminary treatment planning
6 Therapy
- preparatory phase
- evaluation and final treatment planning
- specific restorative phase (corrective)
- maintenance and supportive phase
7 Evaluation and prognosis
Table 4.1 Treatment planning structure according to problem solving method
(Creugers, N et al. 2003).
As important as the above strategy the need to source information on the media and
patient history, extra oral examination, intra oral examination among others contribute to
treatment option and hence treatment variability.
Gathering of information in order to diagnose the patient oral health status could be
divided into:
1. Medical and Patient’s history
2. Extra oral examinations
3. Intral oral examination
4. Radiography examination
5. Diagnostic casts
As mentioned earlier the above list may not be exhaustive and not necessarily in the
manner above but the information obtained is useful in taking decisions on the treatment
option required but it is necessary to consider here the traditional treatment approach and
problem solving option as they relate in this decision making process as the dentist’s
stand as well as the differing goals of any of these options could make or mar the entire
process.
The table below clearly shows this comparison:

Page 17 of 40
Traditional approach Problem solving approach
Diagnosis Impaired dentition Problem listing
Indication Complete morphological
recovery
Always replace
absent teeth
Rigid
Uniform
Problem solving
Selective replacement
of absent teeth
Dynamic
Individual variation
Treatment
characteristic Quantitive overtreatment Quantitive reduction
Table 4.2 Differences between traditional and problem solving treatment approach
(Creugers, N et al. 2003)
The problem-oriented approach allows flexibility and initiative as well as ingenuity of the
dentist in that if a tooth or more is lost it does not present a case for treatment. So if
function is not compromised and a problem will not be solved there is no need to treat
(over treatment). This approach therefore suggests to the dentist the need to divide teeth
‘according to their function and importance into; strategic teeth, non-strategic and
undesirable teeth’.
“Strategic teeth are always to be preserved unless prognosis is bad)
Non- strategic teeth are preserved conditionally
Undesirable teeth are eliminated in time”
Is it possible to have teeth that are undesirable, strategic in a mouth etc as listed above?
Does this categorisation count in the treatment of an oral malady? What kinds of teeth are
so categorised?
Treatment strategy is a set of plan to initiate intervention in order to arrest a declining
oral situation. In this case a number of treatment possibilities is considered against
observable declining oral conditions. The table below depicts probable strategies:

Page 18 of 40
Observation Treatment possibilities
Insufficient oral hygiene Oral hygiene instruction
Sugar intake frequency Instruction about consequences
Cavities, fractured and mobile
teeth Extraction, restoration, decapitation
Endodontic/peri-apical problems Extraction, endodontic treatment
Tooth bound spaces Complete denture, partial denture,
frame denture, no intervention
Finances To take into account when
choosing treatment options
(Creugers, N et al. 2003)
You will be presented with some details about some patients’ and it will be required of
you to present a treatment plan of a critique of your colleagues work in the same way.
Find below a sample patient record for consideration. However there are more in the
resources section.
The sample patient data below from the works of Creugers, N et al. 2003.
Patient: Love
Age 30, male.
Medical and patients history: - has an esthetic problem
- has not visited a dentist for 4 years
- is in good health
- drinks 20 cups of coffee with sugar per day
- can spend about €1000 per year.
Clinical examination:
Extra oral: - no particularities
Intra oral and x-rays:
- gingivitis/plaque
- pockets of >5 mm: 16, 15, 13, 12, 11, 22, 23, 26, 27, 34, 36, 46.
- missing 24, 14, 17, 37, 47, 31
- caries: 16, 15, 13,12,11,21,22,23, 25, 26, 27, 36, 35, 34, 33, 41, 42, 43, and 45.
- several teeth have been treated endodontically (12, 11, 21, 32, 41, 42).
- peri-apical problems: 21, 26, 27, 32, 35, 41, and 42.
Recognition
The combination of very poor oral hygiene, very high sugar frequency and no regular
dental visits has led to much plaque and extended caries. This has led furthermore to
gingivitis and pockets (bone loss) and several peri-apical problems. And all though the
patient is instructed several times already his oral hygiene level stays very poor.

Page 19 of 40
Problem list
1. Motivation/oral hygiene level.
2. Sugar frequency.
3. Gingivitis.
4. Pockets.
5. Caries 25, 33, 34, 35, 45 and extended 15, 16, 26, 27, 36, 41, 42, 43, 46
6. Peri-apical problems: 21, 26, 27, 32, 35, 41, and 42.
7. Financial possibilities.
Strategy
To anticipate on the patient’s wishes and to motivate the patient for oral hygiene, the
anterior upper teeth were treated first (caries was eliminated, and composite laminates
were made). Unfortunately this has not led to better oral hygiene, so the patient can be
assessed as very unmotivated. Treatment is thus oriented on monitored degradation of
the dentition.
Possible treatment options
Motivation/oral hygiene level: instruction
Sugar frequency: instruction
Gingivitis: instruction, professional
cleaning.
Pockets: extraction, professional
cleaning.
Caries: extraction, restoration.
Peri-apical problems: extraction, endodontic
treatment.
Financial possibilities: phased treatment, less
expensive treatment options.
* Missing teeth (after therapy eliminating other problems): removable partial acrylic
denture, frame denture,
complete (over)denture,
Preferable treatment options
It is essential to preserve alveolar bone as long as reasonably possible. Treatment should
be directed towards these strategic teeth important for bone height (think of canines).
For the present teeth this means, that those teeth which can be kept by relatively simple
means, are kept for now. Teeth in need for elaborate treatment (think of endodontic
treatment/crowns) and have a doubtful prognosis (deep pockets/peri-apical lesions) are
extracted.
Instruction for oral hygiene and concerning sugar frequency is given in order to preserve
the remaining teeth, thus alveolar bone.

Page 20 of 40
Teeth 15, 25, 26, 32, 34, 35 and 45 cannot be preserved by simple means (have either
deep pockets, caries or endodontic problems). Teeth 16 and 27 will be restored.
Tooth 33 has extended caries, but is essential for bone preservation.
Also tooth 43 is essential, but has less caries.
Now it is possible to make a removable partial denture in the lower jaw. But this would
complicate even more the oral hygiene for the patient (the 36 and 46 would be even
harder to clean). Also they show pockets already. So it is decided to make an overdenture
in the lower jaw (phase 2). The 33 and 43 are to be treated endodontically.
To spread treatments over time (financially as well), these molars will not be extracted at
once, some molar support is kept for the moment. After recovering from the initial
extractions the immediate dentures can be made (if all are extracted in one time, the fit of
the denture will be less accurate).
After extraction in the upper jaw a removable partial denture will be made to replace the
missing teeth (phase 2).
Acknowledgement
I hereby acknowledge the works of: (Ask, B., Bjørke, S.A., Haugen, H.: Pedagogy for
online learning E-teaching 1; 2006. ) where I derived the guidelines to make this study
guide and from where all Reflection items were drawn.
The course description was also adopted from Global Virtual University course
description template
The said course was undertaken by UNU/GVU; and Agder University College Norway.
My gratitude goes to Prof. Nico Creugers and his team for permission to use the FMS CD
that contained all the resources used in preparing the study guide.
Page 21 of 40
Course Titles: Functional Masticatory System (FMS)
Credit worth: 10 ECTS.
Delivery Type: 100% online with e-tutor moderating.
LMS: Fronter (www.fronter.com, www.moodle.com)
Course Term: Part time.
Duration: 5-10 weeks
Target group: Dental Professionals and students interested in online learning of FMS for
continuous professional development (CPD).
Aim: The course will impact the needs of dental professionals and students in accessing
latest development in FMS regardless of their location on the globe. It will afford them
the opportunity of improving on their skills at conveniences and in combination with
their daily routines while earning credit for continuous professional development (CPD).
Course structure: This course will run on a Learning Management System (LMS) which
means learner will meet in a virtual classroom to carry out course works and exchange
information as well as perform tasks and other roles together. The emphasis here is on
learning not on teaching as learners interact with peers and all other available resources in
a leaning community. There shall be four (4) modules with suggested ECTS time frame
for learner to perform ‘specified’ tasks and activities. The learner shall however have the
freedom to work within cut-off dates as stated within the study calendar. The learner will
earn a certificate of ten (10) credits on (ECTS) scale in Functional Masticatory System
(FMS).
Learning is enhanced under this pedagogical approach when learners participate actively
in class discussions and carry out course assignment in collaboration with co-learners
according to schedule. The minilectures are designed to open-up discussions but not to be
regarded as the main or only resource for this course. Consequently, course participants
are expected to explore the Internet for necessary materials to enrich their experiences
and discussions within the classroom.
Course overall objectives
You will learn to make choices in a so-called problem-oriented treatment
planning
You will be able to discuss factors that affect the patient, dentist, health care
system and art and science of dentistry.
You will pay special attention to new insights about cases of tooth loss causing
tempromandibular joint disorder (TMD) and answer question on the relationship
between the lack of molar support and TMD.
You will learn about the shortened dental arch (SDA) and the preservation of
strategic teeth, a concept that can be of great help to simplify a treatment plan.
Construction of knowledge base in understanding treatment options in oral care.

Page 22 of 40
Designing problem-oriented treatment plans
You will be able to use virtual classroom and tools to learn in an online learning
environment.
Learn the use of computer support and CD-ROM in dental education.
(Creugers, N. et al, 2003).

Page 23 of 40
HEALTHY OCCLUSION
Objective: Learner will understand what normal and non-normal occlusions are.
Learner will be able to understand the stomatognatic system and the
characteristics.
Content: Stomatognatic system, occlusion, pathology.
Overview
Task Activities Resources Estimated
‘ECTS
Hours’
Task 1: Learn
about healthy
occlusion and the
characteristics.
Activity 1- Synchronous: Read
minilecture 1 and discuss.
Suggest module moderator
among course participants.
Activity 2-Synchronous: Find
the probable definitions of
healthy occlusion. Make a list
of such definitions
Activity 3-Synchronous:
Discuss the characteristics of
healthy occlusion and
summarise discussion.
Activity 4-Asynchronous:
Group work: Discuss
morphological characteristics in
relation to the stomatognatic
system and in recognizing
pathological cases. Use real-
time tool within LMS
Activity 5- Synchronous:
Discuss steps in prosthodontic
treatment.
Minilecture 1,
course CD, www
Use web resources
as well
”
”
”
”
(5)
(3)
(6)
(6)
(6)
Task 2: Learn
about functional
characteristics.
Activity 1- Synchronous:
Discuss functional units and
their characteristics. Summarise
discussion.
Activity 2- Synchronous:
Discuss clinical implication for
tooth replacement.
”
”
(3)
(6)

Page 24 of 40
Task 3:
Terminology and
concepts in
occlusion
Activity 1-Asynchronous:
Group discussion on Posselt
diagram.
Activity 2-Synchronous: Find
and discuss other concepts in
attaining healthy occlusion and
place in group folder
summaries of discussion.
”
”
(8)
(5)
Task 4: Adaptation
Mechanisms
Activity 1-Asynchronous:
Group discussion on adaptation
mechanisms.
”
(6)
Reflection-Synchronous (Place
in folder)
(1)
55 Note: The notional student work hours (ECTS hours) in parenthesis are estimates.
Table 5: Module 1 Study Guide
Further Detailed description of tasks and activities
Task 1: Learn about characteristics of healthy occlusion. Activity 1: Each one in the cohort gives one page summary of the minilecture and they
have to agree on who the module moderator has to be.
Activity 2: Group discusses the topic, healthy occlusion and the find distinction between
it and normal and non-normal occlusion. The tutor forms a dyad and each group presents
a summary of their definition of healthy occlusion.
Activity 3: Individual work: Find the characteristics of healthy occlusion and present
your ‘ideal’ characteristics.
Activity 4: Group work: One group finds the morphological characteristics of
stomatognatic system while the other finds the guidelines for recognising right diagnosis
for associated pathological cases.
Activity 5: Consider standard guidelines in treating prosthodontics patient.
Individual work: Prepare a document of what you consider a standard treatment.
Task 2: Learn about functional characteristics
Activity 1: List the functional units and discuss their characteristics. Make distinction
between the functional units.
Activity 2: Consider clinical implication for tooth replacement, healthy and unhealthy
occlusion. Put summary in group folder.
Task 3: Terminology and concepts in occlusion
Activity 1: Consider different terminologies in healthy occlusion. Discuss Posselt
diagram and the import on the understanding of healthy occlusion. Place individual
summary in personal folder.

Page 25 of 40
Activity 2: Find and discuss other concepts in attaining healthy occlusion and place in
group folder summaries of discussion.
Task 4: Adaptation Mechanisms
Activity 1: Discuss adaptation mechanisms of the stomatognatic system and the impact
on achieving occlusion. Group places summary in group folder.
Reflection
Have a look at the objectives for this module. Did you learn what you were supposed to
learn?
Was it easier or more difficult than you thought?
What was easy, what was difficult?
Was the time estimate correct?
What did you find the most useful/enjoy the most, if any, in the module? Why?
What did you find the least useful/least enjoyable, if any, in the module? Why?
Do you have any proposals for improvements of the module?
Can you think of any way you can improve your own ways of learning?

Page 26 of 40
IMPAIRED DENTITION
Objective: Learner will understand what is impaired dentition and its implications on
oral functions, occlusion and stomatognatic system.
Content: Shortened Dental Arch (SDA), impaired dentition, stomatognatic system.
Overview
Task Activities Resources Estimated
‘ECTS
Hours’
Task 1: Learn about
functionally disturbed
occlusion
Activity 1-Synchronous: Read
minilecture 2, discuss and
suggest module moderator.
Activity 2-Synchronous:
Discuss functionally disturbed
occlusion.
Activity 3-Synchronous:
Individual work: Produce a
document on factors leading to
functionally disturbed
occlusion.
Minilecture 2,
www, course
CD.
”
”
(5)
(8)
(6)
Task 2: Learn about
the consequences of
tooth loss.
Activity 1-Synchronous:
Discuss the impact of tooth loss
to the stomatognatic system.
Activity 2-Synchronous:
Discuss natural compensation
and adaptation principles.
Activity 3-Asynchronous:
Group work on discussion.
Summary of discussions
”
”
”
(5)
(6)
(3)
Task 3: Learn about
TMJ disorder.
Activity 1-Synchronous:
Discuss findings on TMD
disorder.
Activity 3-Synchronous:
Summarise discussion and
place summary in group folder.
”
”
(6)
(3)
Task 4: Learn about
classification and
Patterns of impaired
dentition
Activity 1-Synchronous:
Discuss impaired dentition.
Activity 2-Synchronous:
Discuss patterns in impaired
(4)
(4)

Page 27 of 40
human dentition.
Activity 3-Asynchronous:
Discuss implication of TMD on
FMS.
Reflection-Synchronous
(8)
(1)
61 Note: The notional student work hours (ECTS hours) in parenthesis are estimates.
Table 6: Module 2 Study Guide
Further detailed description of tasks and activities
Task 1: Learn about functionally disturbed occlusion
Activity 1: Discuss minilecture 2 and produce a critique of it. Place individual critique document
in personal folder. Agree who should be the module moderator.
Activity 2: Discuss functionally disturbed occlusion and causes. Summarise discussion
Activity 3: Discuss factors responsible for functionally disturbed occlusion. Individual
work: Produce a document on factors responsible for functionally disturbed occlusion.
Task 2: Learn about the consequences of tooth loss.
Activity 1: Discuss the findings on the consequences of tooth loss to the stomatognatic
system. Produce a summary of discussion.
Activity 2: Discuss the natural compensation and adaptation phenomena on tooth loss.
Individual work: Make one page summary on discussion and place document in personal
folder.
Activity 3: Produce group summary on discussion (One group summarises activity 1
while the other activity 2).
Task 3: Learn about TMD
Activity 1: Group work: One group discusses earlier findings on temporal mandibular
disorder and other discusses current findings.
Activity 2: Summarise discussion and place summary in group folder.
Task 4: Learn about classification and Patterns of impaired dentition
Activity 1: Discuss the classification of impaired human dentition and place summary in
group folder
Activity 2: Discuss patterns in impaired human dentition. Individual work: Produce a
document on impaired dentition.
Activity 3: Group work: Group discusses TMD and the implication on functional
masticatory system (FMS). Summarise discussion.
Reflection

Page 28 of 40
1. Repeat the objectives of the module. Did you learn what you were supposed to learn in
this module?
2. Was it easier or more difficult than you thought?
3. What was easy, what was difficult? Why?
4. What did you find the most useful/enjoy the most, if any, in the module? Why?
5. What did you find the least useful/least enjoyable, if any, in the module? Why?
6. Would you say that your own confidence in subject understanding has grown?
7. Would you say that you have developed your study skills? If so, in what way?
8. Can you think of any way you can improve your own ways of learning?
Page 29 of 40
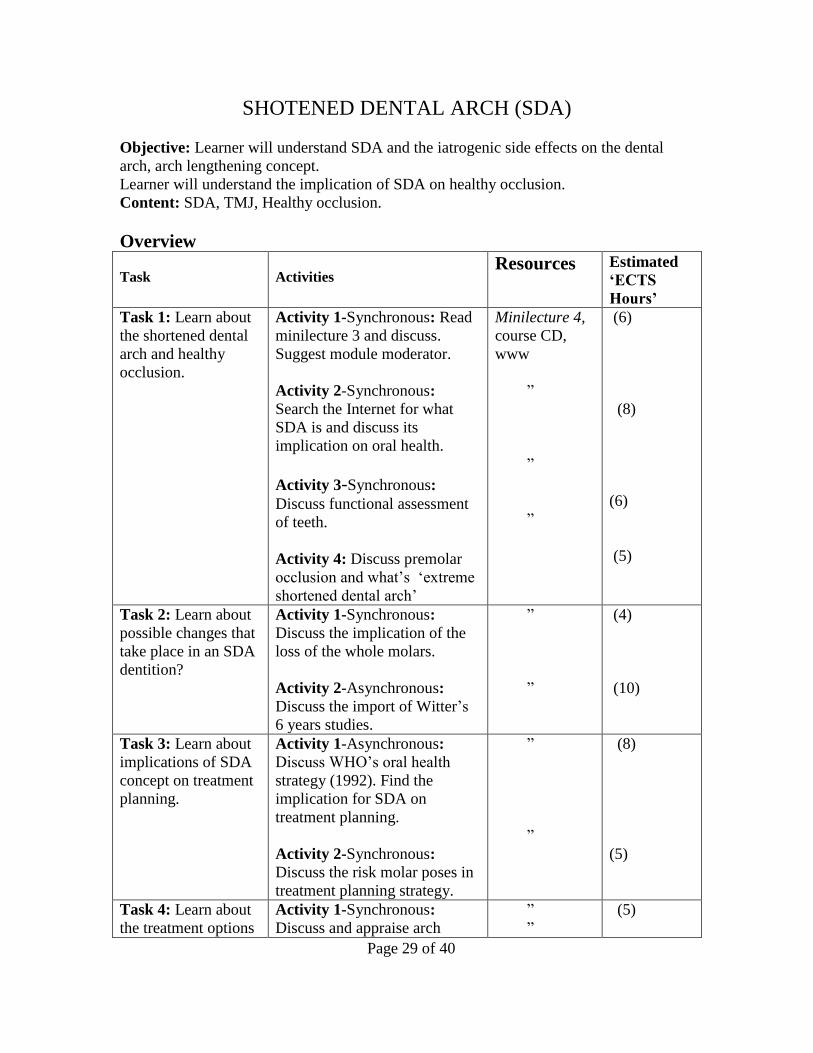
SHOTENED DENTAL ARCH (SDA)
Objective: Learner will understand SDA and the iatrogenic side effects on the dental
arch, arch lengthening concept.
Learner will understand the implication of SDA on healthy occlusion.
Content: SDA, TMJ, Healthy occlusion.
Overview
Task Activities Resources Estimated
‘ECTS
Hours’
Task 1: Learn about
the shortened dental
arch and healthy
occlusion.
Activity 1-Synchronous: Read
minilecture 3 and discuss.
Suggest module moderator.
Activity 2-Synchronous:
Search the Internet for what
SDA is and discuss its
implication on oral health.
Activity 3-Synchronous:
Discuss functional assessment
of teeth.
Activity 4: Discuss premolar
occlusion and what’s ‘extreme
shortened dental arch’
Minilecture 4,
course CD,
www
”
”
”
(6)
(8)
(6)
(5)
Task 2: Learn about
possible changes that
take place in an SDA
dentition?
Activity 1-Synchronous:
Discuss the implication of the
loss of the whole molars.
Activity 2-Asynchronous:
Discuss the import of Witter’s
6 years studies.
”
”
(4)
(10)
Task 3: Learn about
implications of SDA
concept on treatment
planning.
Activity 1-Asynchronous:
Discuss WHO’s oral health
strategy (1992). Find the
implication for SDA on
treatment planning.
Activity 2-Synchronous:
Discuss the risk molar poses in
treatment planning strategy.
”
”
(8)
(5)
Task 4: Learn about
the treatment options
Activity 1-Synchronous:
Discuss and appraise arch
”
”
(5)

Page 30 of 40
for arch lengthening. lengthening treatment options.
Activity 2-Asynchronous:
Discuss arch lengthening
treatment option and relate to
SDA alternative.
Activity 3-Asynchronous:
Discuss contra-indication for
RPD treatment options on the
patient’s oral environment.
”
”
(5)
(4)
Task 5: Learn about
oral health care and
implications on SDA.
Activity 1-Synchronous:
Discuss conventional treatment
option and problem-oriented
approach for SDA.
Activity 2-Synchronous: Group
produces summary document
on discussion
Reflection -Synchronous
”
”
(7)
(3)
(1)
77
Note: The notional student work hours (ECTS hours) in parenthesis are estimates.
Table 7: Module 3 Study Guide
Further detailed description of tasks and activities
Task 1: Learn about the shortened dental arch and healthy occlusion.
Activity 1: Discuss minilecture 3 and produce a summary of it. Agree on should be
module moderator.
Activity 2: Discuss SDA factors responsible for it and the implication on healthy
occlusion. Group summary on discussion.
Activity 3: Discuss functional assessment of different types of teeth and produce a
summary of discussion.
Activity 4: Discuss premolar occlusion and what ‘extreme shortened dental
arch’ is. Summarise your discussion.
Task 2: Learn about possible changes that take place in an SDA dentition?
Activity 1: Discuss the implication of the loss of the whole molars. Summarise
discussion.
Activity 2: Discuss the import of Witter’s 6 years studies in the longitudinal study of
SDA with the anterior teeth present and three to five (5) occlusal units. Tutor will divide
you into group for this discussion. Summarise Discussion and place in group folder.
Task 3: Learn about implications of SDA concept on treatment planning.

Page 31 of 40
Activity 1: Group discussion on WHO’S oral health strategy (1992) and health
implication of SDA on treatment planning. Activity 2: Discussion of the molar, the roles it poses in treatment planning strategy.
Organise yourselves into group for this discussion and produce a summary of your
discussion.
Task 4: Learn about the treatment options for arch lengthening.
Activity 1: Discuss and appraise arch lengthening treatment options and relate to SDA
alternative. The cohort summarises discussion and place summary in group folder.
Activity 2: Group work: One group discusses fixed prosthesis while another discusses
removable prosthodontics as arch lengthening treatment option.
Activity 3: Individual work: Find the contra-indication for RPD treatment options on the
patient’s oral environment. Place summary in group folder.
Task 5: Learn about oral health care and implications on SDA.
Activity 1: Discuss conventional treatment option and problem-oriented approach for
SDA.
Activity 2: Group produces summary document on discussion
Reflection
1. Repeat the objectives of the module. Did you learn what you were supposed to learn in
this module?
2. Was it easier or more difficult than you thought?
3. What was easy, what was difficult? Why?
4. What did you find the most useful/enjoy the most, if any, in the module? Why?
5. What did you find the least useful/least enjoyable, if any, in the module? Why?
6. Would you say that your own confidence in subject understanding has grown?
7. Would you say that you have developed your study skills? If so, in what way?
8. Can you think of any way you can improve your own ways of learning?
9. Was the time estimate for each activity roughly correct?
10. Do you think that the interaction and discussions with your fellow students and tutor
during this module could improve in any way?
11. Do you think that the tutor should have been more or less active, or has s/he found the
right balance?
12. Have the tutor's comments been well-chosen, encouraging and in sufficient quantity?

Page 32 of 40
TREATMENT PLANNING
Objective: Learner will understand different treatment plan/options and their appraisals.
Learner will be able to reflect of treatment planning alternatives.
Content: Treatment planning, problem solving, traditional treatment options.
Overview
Task Activities Resources Estimated
‘ECTS
Hours’
Task 1: Learn about
the variability of
treatment planning.
Activity 1-Synchronous: Read
minilecture 4, discuss and suggest
module moderator.
Activity 2-Synchronous: Discuss
factors responsible for variability in
treatment planning.
Activity 3-Synchronous: Produce a
group hand-in
(5)
(3)
(2)
Task 2: Learn about
traditional and
problem –solving
treatment options.
Activity 1-Asynchronous: Discuss
traditional and problem-solving
treatment approaches.
(6)
Task 3: Learn about
sample patient case
studies.
Activity 1-Synchronous: Produce and
discuss a critique of the patients
whose details are provided and proffer
your choice alternative treatment
options.
Activity 2-Synchronous: Individual
work: Produce a treatment plan for a
fictitious case and defend your
treatment option.
Reflection-Synchronous
(6)
(4)
(1)
31 Note: The notional student work hours (ECTS hours) in parenthesis are estimates.
Table 8: Module 4 Study Guide
Further detailed description of tasks and activities
Task 1: Learn about the variability of treatment planning. Activity 1: Read minilecture 4, discuss and suggest module moderator.

Page 33 of 40
Activity 2: Discuss factors responsible for variability in treatment planning.
Activity 3: Produce a group hand-in
Task 2: Learn about traditional and problem –solving treatment options.
Activity 1: Learn about traditional and problem –solving treatment options
Activity 2: Discuss traditional and problem-solving treatment approaches.
Summarise discussion and place summary document in group folder.
Task 3: Learn about sample patient case studies.
Activity 1: Produce and discuss a critique of the patients whose details are provided and
proffer your choice alternative treatment options.
Activity 2: Individual work: Produce a treatment plan for a fictitious case and defend
your treatment option.

Page 34 of 40
References Ash & Ramfjord (1995) in Creugers, N et al. (2003) Functional Masticatory System,
WHOCC: The Netherlands.
Blakeslee, R.W; Renner, R.P& Shiu, A. (1980) Dental Technology Theory and
Practice. United States, C.V., Mosby Company.
Boucher, C.O. (1947) Dental Prosthetics Manual, United States C.V. Mosby Company
Conrad, R. and Donaldson, J.A. (2004) Engaging the online learner. Activities and
resources for creative instruction, Jossey-Bass guides to online teaching and learning,
volume 1, Wiley, San Francisco.
Creugers, N et al. (2003) Functional Masticatory System, WHOCC: The Netherlands.
De. Kanter (1990) in Creugers, N et al. (2003) Functional Masticatory System,
WHOCC: The Netherlands.
Eckerbom, et al (1992); Sheiman, (1997) & Brown, et al (1989) in Creugers, N et al.
(2003) Functional Masticatory System, WHOCC: The Netherlands.
Jaques, D & Salmon, G. (2007) Learning in Groups: A Handbook for face-to-face and
online Environments, Routledge/Taylors & Francis Group: London and New York.
Kayser, (1996) in Creugers, N et al. (2003) Functional Masticatory System, WHOCC:
The Netherlands.
Witter, 1994 Part I & II) In Creugers, N et al. (2003) Functional Masticatory System,
WHOCC: The Netherlands.
Leake, et al (1994) in Creugers, N et al. (2003) Functional Masticatory System,
WHOCC: The Netherlands.
Morrow, R.M; Rudd, K.D; Eissmann, H.F ed (1981): Dental Laboratory Procedures
Vol. 1-3. United States, C.V., Mosby Company.
Olubodun, O.J. (2008) A study guide based on socio-constructivist pedagogy.
Rosenoer, & Sheiham, (1999) in Creugers, N et al. (2003) Functional Masticatory System
Wikipedia.org (2008) Social Constructivism (Learning theory[online]
http://en.wikipedia.org/wiki/Social_Constructivism_%28Learning_Theory%29

Page 35 of 40
APPENDIX I
RUBRIC
General Appraisal on Participation (Self assessment)
Criteria 0 2 3 4
Cooperation Did not pay
attention to
others did not
value the
opinion of
others
Paid attention
to, but did not
value the
opinion of
others.
Actively paid
attention to,
but it was not
evident that
opinion of
others was
valued
Actively paid
attention to and
valued the
opinions of
others
Contribution Did not
contribute to
the completion
of the tasks
Contributed,
but the work
was inferior or
inadequate
Contributed to
the completion
of the tasks
with adequate
work
Contributed to
the completion
of the tasks and
submitted high-
quality work
Participation Did not
participate in
the group
Occasionally
participated in
the group
Often
participated in
the group
Consistently
participated in
the group
(Conrad&Donaldson, 2004, p.30: Quoted by Ask, B., Bjørke, S.A., Haugen, H.:
Pedagogy for online learning 1 E-teaching 1; 2006.)

Page 36 of 40
APPENDIX II
STUDY CALENDAR
Date Activity Jan 2008.
04 Start up Module 0
09 Post task 2 Activity 1
10 Post reflection
11 Start up Module 1
16 Post Task 1 Activity 1
21 Post Task 1 Activity 2
23 Post Task 1 Activity 3
25 Post Task 1 Activity 4
28 Post Task 1 Activity 5
30 Post Task 2 Activity 1
February
01 Post Task 2 Activity 2
06 Post Task 3 Activity 1
08 Post Task 3 Activity 2
11 Post Task 4 Activity 1
12 Post reflection
13 Start Up Module 2
18 Post Task 1 Activity 1
20 Post Task 1 Activity 2
22 Post Task 1 Activity 3
25 Post Task 2 Activity 1
27 Post Task 2 Activity 2
March
03 Post Task 2 Activity 3
05 Post Task 3 Activity 1
10 Post Task 3 Activity 2
12 Post Task 4 Activity 1

Page 37 of 40
14 Post Task 4 Activity 2
17 Post Task 4 Activity 3
17 Post reflection
18 Start up Module 3
19 Post Task 1 Activity 1
21 Post Task 1 Activity 2
24 Post Task 1 Activity 3
26 Post Task 1 Activity 4
28 Post Task 2 Activity 1
31 Post Task 2 Activity 2
April
02 Post Task 3 Activity 1
07 Post Task 3 Activity 2
09 Post Task 4 Activity 1
11 Post Task 4 Activity 2
14 Post Task 4 Activity 3
15 Post Task 5 Activity 1
16 Post Task 5 Activity 2
17 Post Reflection
21 Post TMA
21 Start Up Module 4
23 Post Task 1 Activity 1
25 Post Task 1 Activity 2
28 Post Task 1 Activity 3
30 Post Task 2 Activity 1
May
02 Post Task 2 Activity 2
03 Post Task 3 Activity 1
Post Task 3 Activity 2
05 Online Exam
08 End of course.
Page 38 of 40
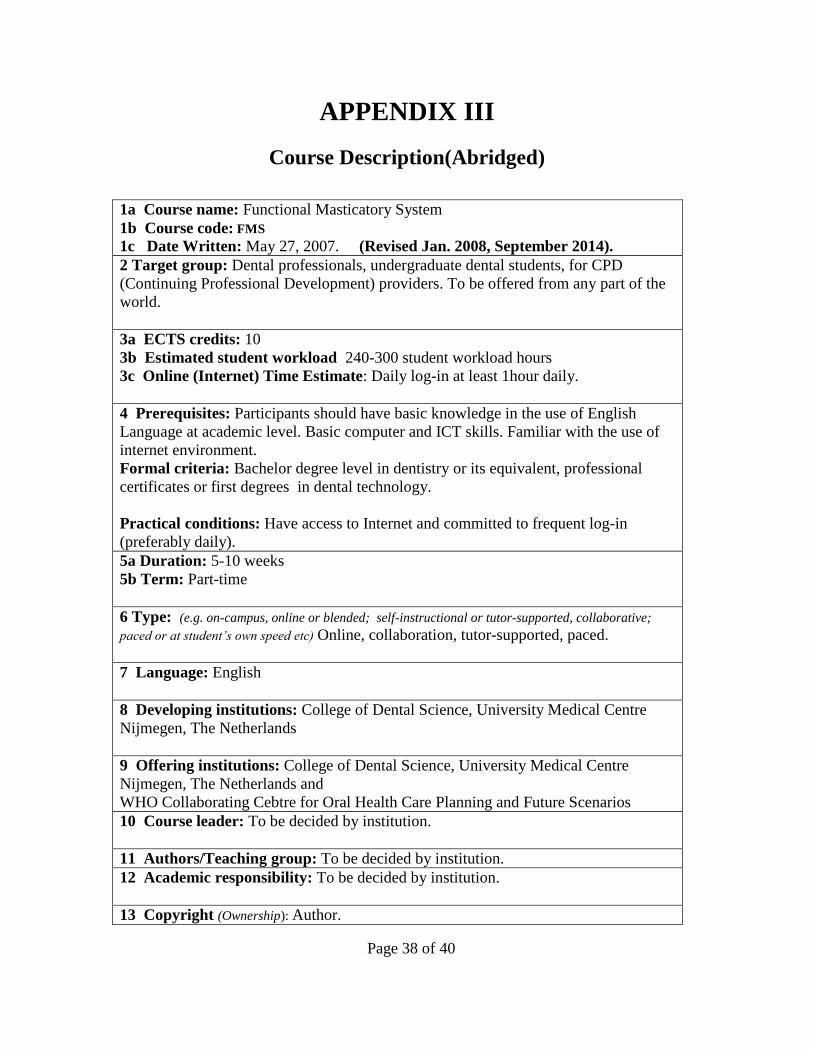
APPENDIX III
Course Description(Abridged)
1a Course name: Functional Masticatory System
1b Course code: FMS
1c Date Written: May 27, 2007. (Revised Jan. 2008, September 2014).
2 Target group: Dental professionals, undergraduate dental students, for CPD
(Continuing Professional Development) providers. To be offered from any part of the
world.
3a ECTS credits: 10
3b Estimated student workload 240-300 student workload hours
3c Online (Internet) Time Estimate: Daily log-in at least 1hour daily.
4 Prerequisites: Participants should have basic knowledge in the use of English
Language at academic level. Basic computer and ICT skills. Familiar with the use of
internet environment.
Formal criteria: Bachelor degree level in dentistry or its equivalent, professional
certificates or first degrees in dental technology.
Practical conditions: Have access to Internet and committed to frequent log-in
(preferably daily).
5a Duration: 5-10 weeks
5b Term: Part-time
6 Type: (e.g. on-campus, online or blended; self-instructional or tutor-supported, collaborative;
paced or at student’s own speed etc) Online, collaboration, tutor-supported, paced.
7 Language: English
8 Developing institutions: College of Dental Science, University Medical Centre
Nijmegen, The Netherlands
9 Offering institutions: College of Dental Science, University Medical Centre
Nijmegen, The Netherlands and
WHO Collaborating Cebtre for Oral Health Care Planning and Future Scenarios
10 Course leader: To be decided by institution.
11 Authors/Teaching group: To be decided by institution.
12 Academic responsibility: To be decided by institution.
13 Copyright (Ownership): Author.

Page 39 of 40
14 Aims (What shall the course achieve in general terms / what the university wants to
achieve with the course):
You will learn to make choices in a so-called problem-oriented treatment
planning
You will discuss factors such as the patient, dentist, health care system and art
and science in dentistry.
You will pay special attention to new insights on cases of tooth loss causing
tempromandibular joint disorder (TMD) and question the relationship between
the lack of molar support and TMD.
You will learn about the shortened dental arch (SDA) and the preservation of
strategic teeth, a concept that can be of great help to simplify a treatment plan.
Construction of knowledge base in understanding treatment options in oral
care.
Designing problem-oriented treatment plans
You will be able to use virtual classroom and tools to learn in group.
Learn the use of computer support and CD-ROM in dental education.
15 Learning resources (Learning material, learning support) LMS, articles, short
minilectures, suggested books and www.
16 Objectives and Learning outcomes of the course (Sets of competences, expressing
what the student will know, understand or be able to do after completion of a process of learning, and
products of this process.)
Students will gain knowledge on completion of the course to:
1. Designing problem-oriented treatment plans
2. You will pay special attention to new insights about cases of tooth loss causing
tempromandibular joint disorder (TMD) and question the relationship between the
lack of molar support and TMD.
3. You will learn about the shortened dental arch (SDA) and the preservation of
strategic teeth, a concept that can be of great help to simplify a treatment plan.
4. Construction of knowledge base in understanding treatment options in oral care.
Students will gain skills in:
1. You will be able to use virtual classroom and tools to learn in a learning
community.
2.Learn the use of computer support and CD-ROM in dental education
17. Content description (Content in each learning unit)
Module 1: Healthy Occlusion.
Learner will understand and be able to differentiate between normal and non-normal
occlusion. They will be able to reflect on functional characteristic of the esthetic and
occlusal units that constituted the functional unit of the oral cavity and the clinical
implications of tooth replacement as it affects the adaptation mechanism of the
stomatognatic system.
Module 2: Impaired dentition.
Learner will be able to reflect on the implication of tooth loss on TMD, functionally
disturbed occlusion and the patterns of impaired dentition. They will gain clearer

Page 40 of 40
understanding on the consequences of this on healthy occlusion.
Module 3: Shortened dental arch
Learner will gain understanding on SDA, changes associated with SDA dentition and
consequences on oral healthcare. The concept of arch lengthening will be understood
in the light of treatment planning.
Module 4: Treatment Planning.
Learner will be able to make quality clinical decisions on treatment options and a
distinction between traditional and problem-solving treatment approaches.
Learner will be able to reflect on sample of patient treatment criteria and hence gain
understanding on how to make a treatment plan.
18. Mode of delivery (LMS, TV, WWW, radio, F2F lectures etc)
Course description, study guide, calendar and 'url' links and suggested books for
reading. Classfronter is the Learning Management System (LMS). Main
communication tools: asynchronous threaded online discussion. Group and individual
assignments and hand-ins and cut-off dates. 19. Infrastructure needed Course participants will be allowed to access the LMS and within which a virtual
office will be available to each participant. Work will take place in virtual classroom,
group room. Internet connectivity is preferably broadband.
20. Teaching methods (Instructional, constructivist, socio-cultural, blended, etc)
Learner-centered with tutor support. 100% online activities, minilecture to set pace for
discussion by the tutor, peer tutoring, group work and individual work. Socio-
Constructivist pedagogical approach with many-to-many communication. 21. Assessment of participants (Portfolio, home exam, participation, on-campus exam etc)
Portfolio, hand-ins, online examination arranged by home office (50%) as end of
course assessment, activities during discussion and materials submitted during course.
22. Bibliography:
Study guide and minilectures, CD-rom, Internet resources etc.
23. LMS administration (Responsible for the online Learning Management System):
Not decided but fronter proposed
24. Course evaluations (Student feedback evaluation form, tutors’ evaluation): There will be reflection on the course after each module as formative evaluation, and
summative evaluation will be conducted on course completion.
25. Other remarks. Nil
26. Fees: $750 USD. (Suggested)


















