
E-Bulletin - UniKL...RCMP Bulletin page: 4 Salam and dear all, We are now ready to serve the country...
35
E-Bulletin RCMP Vol 4, 2009 June 15 EXERCISE TIPS FOR DIABETES ASTHMA Differences Between Asthma And Copd The weather in this second quarter of the year has been very warm or to some extent hot , Whatever the weather is, businesses at the college must go as usual for the better, or much better EDITORIAL Chemistr y And Pharmacy DR. MOHD AZHAR MOHD NOOR - KIDNEY TRANSPLANT OPERATION
Transcript of E-Bulletin - UniKL...RCMP Bulletin page: 4 Salam and dear all, We are now ready to serve the country...
RCMP Bulletin page 1
E-BulletinR
CM
P
Vol 4, 2009 June 15
EXERCISETIPS FOR
DIABETESASTHMADifferences Between Asthma And Copd
The weather in this second quarter of the year has been very warm or to some extent hot , Whatever the weather is, businesses at the college must go as usual for the better, or much better
EDITORIAL
Chemistry And P h a r m a c y
DR. MOHD AZHAR MOHD NOOR - KIDNEY TRANSPLANT OPERATION

RCMP Bulletin page: 2
EDITORIAL BOARD ADVISOR Professor Dr. Hashami Bohari
HEAD OF EDITORIAL BOARDDr. Mohammad Abdul Rahman
EDITOR Professor Dr. Awang IPR Dr. V. GopalakrishnanEn. Nordin Abdul RasidPn. Siti Noraihan Sheikh Ahmad
SECRETARYPn. Julilah Adri
DESIGN Mohd RizalMohd Iskandar
EDITORIALThe weather in this second quarter of the year has been very
warm or to some extent hot. Weather forecast predicts that hot days are likely to extend till September, possibly as an el nino.
How we wish that the weather remains cool and cozy at all times. That is a man’s wish. When a day is hot, we wish it to be
cool and vice versa. Anyway, whatever the weather change is, it is beyond our control, although at times we are successful in
seeding rains. Accept as the changes are and do whatever we can at our best to benefit from the changes, for each change has
its own merit – dry hot bright days are good for rubber tapers; moderately wet rainy days are good for plants, especially after a
long dry spell.
Whatever the weather is, businesses at the college must go as usual for the better, or much better, for excellence which the
Dean has spelt out clearly in the acronym ‘CITIE’ which stands for commitment, integrity, teamwork, innovation and excellence.
CITIE are our core values and standards for our behaviour towards excellence. They can be memorized, internalized and translated into the desired behaviour of excellence – possibly
as a UniKL RCMP branding endeavour. CITIE is innovatively printed on a business-card size paper, can be inserted snuggly
in our wallets, and appears to remind us of our core values and standards for excellence, every time we open our wallets.
Simply, just do that.
Since its birth, this bulletin is a way forward towards achieving that excellence. It is a forum for us to share ideas
and disseminate information that can be useful for planning, implementing and evaluating programmes, projects, activities and efforts towards achieving excellence, in line with CITIE.
The Editorials thanks all contributors who have made this issue of our bulletin possible. We look forwards for everybody’s
contributions for success of the up-coming issues.
Yours sincerely,
Professor Dr Awang IPREditorial

RCMP Bulletin page 3
Deputy Dean (Academic) Corner
Few Lines From Prof Hashami
Thank you very much for giving me the opportunity to drop few lines for the 4th issue of our e-bulletin. Basically I’m proud with the think tanks and the team work that have put their strength together in managing the e-bulletin. I believe if more heads should we put together the quality can be sustained.
Time flies swiftly without realizing we are already in the midst of year 2009. RCMP calendars are already occupied with various events and activities. For the past quarter year RCMP has done numerous activities for staffs and students. Our Open Day at RCMP premise, Open Ceremony for the 40 Youths from Southern Thailand by Tun Jeanne Abdullah followed by Closing and Certificate Giving Ceremony also for the 40 Youths from Southern Thailand done by Deputy Defence Minister, Datuk Dr. Abdul Latiff bin Ahmad at Nikko Hotel, Ampang, Kuala Lumpur and Sports Day at MSI, Kulim.
On the 11th and 12th July 2009, RCMP will be expecting at least 180 students from various parts of Malaysia. Since the number of students is growing tremendously each year, therefore we are coming up with a 10 storey building. This new building will accommodate more than 800 students, nursing hostel for males and females’ students, academic and non academic offices, laboratory and many more. We expected it to be completed by year 2012.
Later by end of June, all RCMP staffs will gather at Marina Cove for Family Day. The days are just around the corner. This is the first time after 8 years RCMP is organizing such an activity to show the appreciation to our committed staffs. I believed most of us are very excited and eagerly waiting for the big day. Actually more activities will be arranged to suit all levels.
Finally, I would like to wish all fathers in RCMP a Happy Father’s Day. May all of us proud to be family members of RCMP.
Warmest RegardsProf Dr. Hashami bin Bohari

RCMP Bulletin page: 4
Salam and dear all,
We are now ready to serve the country but we want to
come back here again to pursue our Diplomas. Thank
you, Thank you, Thank you to UniKL- RCMP that
change our life and please pray for us -The 40 youths
Thursday, 11 June 2009 was a memorable day to cherish for the 40 young girls from Southern
Thailand who received their Nursing Aide Certificate from Deputy Defence Minister, Datuk Dr. Abdul Latiff bin Ahmad at Nikko Hotel, Ampang, Kuala Lumpur. The 40 girls completed their one year training programme from 16 June 2008 till 16 June 2009 at UniKL-RCMP. They were accompanied by their beloved parents who came all the way from various parts of Southern Thailand invited and initiated by Malaysian TASK FORCE 2010 to share the prestigious moment. Among other honourable guests were Mr. Kamthorn Sithtichoti, representing the Thailand Ambassador to Malaysia, UniKL-RCMP Chairman Datuk Zamani bin Md Noor and Director General of Malaysia and Thailand TASK FORCE.
When they came here a year ago, they encounter many difficulties adjusting themselves in a foreign country especially culture and language barrier but they determined to go
extra mile to excel in their study because they believed good luck does not strike twice at their door. Coming from a religious background, with limited knowledge about Malaysia, having low self confidence ultimately they managed to pull through and address all these problems. RCMP turned them by leaps and bounds. Today they make their parents and communities feel proud of them. Upon reaching home jobs are already waiting for these girls to serve the Narathiwat Hospitals. According to UniKL-RCMP Chairman Datuk Zamani bin Md Noor, this pilot project will continue with bigger dimension and most likely in future RCMP will train orderly (male nurses). Last but not least he thanked UniKL-RCMP academic and non-academic staffs for their unlimited support that helps to materialize this programme. More stories about these young girls in Utusan Malaysia and Berita Harian on Friday 12 June 2009.

RCMP Bulletin page 5

RCMP Bulletin page: 6
EXERCISETIPS FOR
DIABETESDiabetes is a syndrome of disordered metabolism, usually due to a combination of hereditary and environmental causes, resulting in abnormally high blood sugar level. Diabetes develops due to a diminished production of insulin in type 1 or resistance to its effects in type 2 and gestational. Both types lead to hyperglycemia, which largely causes the acute signs of diabetes: excessive urine production, resulting compensatory thirst & increased fluid intake, blurred vision, unexplained weight loss, lethargy and changes in energy metabolism.In the diabetic management along with medications the roll of diet plan & exercise plays the key roll to control your diabetes & limit the complications.Here some exercise tips to your diabetic control.
Before You Start:
Exercise Tips:
Before start the exercise consult your doctor/physiotherapist/diabetic nurse. Because the diabetic people are at higher risk of heart and circulation problems, so your health advisor may want to check your heart, eyes, and feet.
Go for Low-Impact Exercise. Knowing you’re doing something safe -- especially if you have painful neuropathy or loss of sensation removes one barrier to exercise: fear. Change to something that would be low-impact or even non-weight-bearing, says Trence, such as aerobic classes where you’re sitting in a chair or using an exercise ball. Other options:
Swimming. Water supports your muscles, bones, and joints as you swim, especially helpful if you’re overweight or have diabetic nerve pain in your feet. A longtime favorite of exercise experts over the years, swimming avoids the pounding on your feet, knees, and hips from a high-impact sport like jogging.
Cycling. Biking is safely low-impact - as long as you stay safely aboard - and you can ride outside for a change of scenery, or ride with a friend on stationary bikes in a health club.
Yoga. “I think yoga is underutilized in people with diabetes,” says Trence. “It’s a wonderful exercise, particularly for people who need to be more controlled in their movements and not
be pounding the pavement.”
RCMP Bulletin page 7
Shoot for 30 Minutes, 5 Days a Week.
Do the exercise for 30 minutes a day, five days a week. - Start with a short warm up period to help prepare your muscles, heart and lungs. Gentle stretches for five to 20 minutes help reduce injury. - Build slowly over time, so you keep feeling successful and having fun. - Don’t worry if, some days, you can’t do a full 30 minutes all at once. You can meet your daily goal of 30 minutes with 10 minutes of yard work in the morning, 10 minutes of vacuuming after lunch, and a brisk 10-minute walk after dinner. - Start with simple things, says Trence, like parking farther from the door or using the stairs when you can.
Make It Social.
Behavioral medicine experts all agree: social support helps keep you going when the going gets tough. And what’s tougher than trying to make lifestyle changes?- Make regular weekly dates with a friend, neighbor, or family member to walk or exercise with you. You may be more likely to stay committed since you won’t want to let the other person down. - Consider joining a local walking or hiking club, so you get outside, get some fresh air, and meet new people. You may find it’s easier to exercise when you let others do the planning. - Check out groups like a softball team, volleyball team, or cycling club. Your local Y might have a swim team for adults. Or a local school may need a volunteer coach
Make It Fun.
Choose activities you enjoy - or at least enjoy some aspects of. Otherwise, it’s a cinch you’ll back out when your commitment flags. So don’t join the dance workout at the Y just because your wife loves it - though if you’re a music lover, a dance class could be just your style. Bowling might be right up your alley. But if you’ve never had any hand-eye coordination or “ball sense,” then taking up tennis or volleyball may not be your thing.- Think back to high school or college: what did you love to do back then? Were you a great softball player, golfer - or love to shoot hoops? Look for a club, gym, or community center where you can join a pick-up league. - Find people at your fitness level, so you won’t feel overly frustrated. - Fun is unique to each person. For you, something may be fun because it’s new. For others, pleasure is something familiar and comfortable. Know thyself, and trust thyself.
You Don’t Have to Sweat. All exercise isn’t alike. Aerobic exercise raises your heart rate, helps you lose weight, and does make you sweat. But all your exercise doesn’t have to be so hard that you need to sweat to reap the benefits. Try strength training, like lifting weights, and working on your flexibility by stretching or taking a yoga class.- Mix it up. Try a combo of activities that build your aerobic fitness, strength, and flexibility. You’ll get more benefits - and be less prone to injury and boredom. - Modification is the key. If you can’t do a regular push-up, for instance, you can do a few push-ups against a wall, so it’s a lot less work for your arms and shoulders. Go for a sense of success: if you feel successful, you’re more likely to stay with it. - You don’t have to spend money for club dues. With so many exercise videos and DVDs out now, says Trence, people can exercise at home and try new things.

RCMP Bulletin page: 8
Try Something New.
In the wake of the fitness boom, you have more choices than ever for new forms of exercise. Avoid boredom or feeling like exercise is a chore by trying something new.- Try a water aerobics class or other swim class at your local pool. - Take a class in a new sport or activity, like golf, badminton, kayaking, or ballroom dancing. - Try yoga, tai chi, and other exercise that enhances your mind/body connection, encourages relaxation, and brings on a sense of well-being. The more fun you have with it, the more likely you’ll create a healthy, active lifestyle that invigorates you and helps you manage diabetes for a lifetime.
EXERCISETIPS FOR
DIABETES

RCMP Bulletin page 9
ASTHMADifferences Between Asthma And Copd
Asthma
Asthma is a chronic inflammatory disorder of the airways in which many cells and cellular elements play a role. The chronic inflammation is associated with airway hyperresponsiveness that leads to recurrent episodes of wheezing, breathlessness, chest tightness, and coughing, particularly at night or in the early morning. These episodes are usually associated with widespread, but variable, airflow obstruction within the lung that is often reversible either spontaneously or with treatment. ORAsthma is a chronic inflammatory disorder of the airways associated with hyperresponsiveness, reversible airflow limitation, and respiratory symptoms.
AETIOLOGY
Asthma is a heterogeneous disease with interplay between genetic and environmental factors.
Factors Influencing the Development and Expression of Asthma
1. Host Factors
Genetic (e.g., genes pre-disposing to atopy and genes pre-disposing to airway hyperresponsiveness), obesity (certain mediators such as leptins) and sex
RISK FACTORS
1. Cigarette Smoking
However, only 15% of the variability in FEV1 is noted in chronic smokers (pack-years). This finding suggests that additional environmental and/or genetic factors contribute to the impact of smoking on the development of airflow obstruction.2. Airway Responsiveness and COPD
It has demonstrated that there is increased airway responsiveness to a variety of exogenous stimuli in patients with COPD
3. Respiratory Infections
Although respiratory infections are important causes of exacerbations of COPD, the association of both adult and childhood respiratory infections to the development and progression of COPD remains to be proven.
COPD
Chronic Obstructive Pulmonary Disease (COPD) is a disease state characterized by airflow limitation that is not fully reversible.COPD includes emphysema, an anatomically defined condition characterized by destruction and enlargement of the lung alveoli; chronic bronchitis, a clinically defined condition with chronic cough and phlegm; and small airways disease, a condition in which small bronchioles are narrowed.

RCMP Bulletin page: 10
AETIOLOGY
2. Environmental Factors Allergens• Indoor: Domestic mites, furred animals (dogs, cats,mice), cockroach allergen, fungi, molds, yeasts• Outdoor: Pollens, fungi, molds, yeastsInfections (predominantly viral)Occupational sensitizersTobacco smoke (Passive or active smoking)Outdoor/Indoor Air PollutionDiet (infants fed formulas of intact cow’s milk or soy protein)
Intrinsic Asthma (Non-atopic) • Approximately 10% • Negative skin test to common inhalant allergens • Normal serum concentrations of IgE• Later onset of disease (adult-onset asthma)• Commonly have concomitant nasal polyps, and may be aspirin-sensitive• Little is understood about mechanism.• The immunopathology in bronchial biopsies and sputum appears to be identical to that found in atopic asthma. • There is recent evidence for increased local production of IgE in the airways, suggesting that there may be common IgE mediated mechanisms.
PATHOGENESIS
Asthma is associated with a specific chronic inflammation of the mucosa of the lower airways.The inflammation affects all airways including the upper respiratory tract and nose but its physiological effects are most pronounced in medium-sized bronchi but small airway inflammation is found particularly in patients with severe asthma.The pattern of inflammation in the airways appears to be similar in all clinical forms of asthma, whether allergic, non-allergic, or aspirin induced, and at all ages.Inflammatory cells: Mast cells, eosinophils,CD4+ T lymphocytes, macrophages, neutrophils and epithelial cells Histopathology of a small airway in fatal asthma. The lumen is occluded with a mucous plug, there is goblet cell metaplasia, and the airway wall is thickened, with an increase in basement membrane thickness and airway smooth muscle. (Harrison)Characteristic finding: thickening of the basement membrane due to subepithelial collagen deposition. A marker of eosinophilic inflammation in the airway, as eosinophils release fibrogenic factors.
Risk Factors
3. Occupational ExposuresAlthough several specific occupational dusts and fumes are likely risk factors for COPD, the magnitude of these effects appears to be substantially less important than the effect of cigarette smoking.
4. Ambient Air PollutionIn most populations, ambient air pollution is a much less important risk factor for COPD than cigarette smoking.
5. Passive, or Second-Hand, Smoking ExposureAlthough passive smoke exposure including exposure of children to maternal smoking has been associated with reductions in pulmonary function, the importance of this risk factor in the development of the severe pulmonary function reductions in COPD remains uncertain.
6. Genetic ConsiderationsSevere 1 antitrypsin ( 1AT) deficiency is a proven genetic risk factor for COPD (1–2%). There is also increasing evidence that other genetic determinants also exist
PATHOPHYSIOLOGY
Increases in the residual volume (RV) and the residual volume/total lung capacity ratio (RV/TLC), nonuniform distribution of ventilation, and ventilation-perfusion mismatching (V/P)
PATHOLOGY
Pathological changes characteristic of COPD are found in the proximal airways, peripheral airways, lung parenchyma, and pulmonary vasculature.Changes in large airways cause cough and sputum, while changes in small airways and alveoli are responsible for physiologic alterations.
Inflammatory cellsNeutrophils, macrophages, CD8+ T lymphocytes and eosinophils
RCMP Bulletin page 11
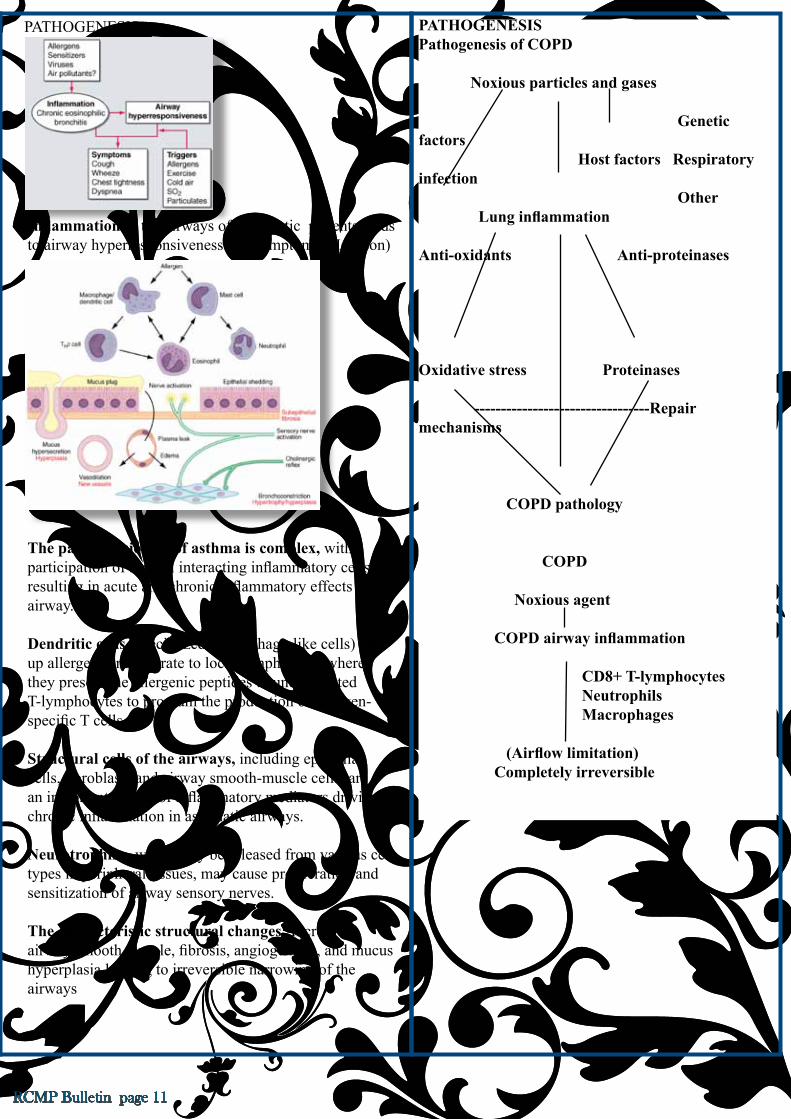
Inflammation in the airways of asthmatic patients leads to airway hyperresponsiveness and symptoms (Harrison)
The pathophysiology of asthma is complex, with participation of several interacting inflammatory cells, resulting in acute and chronic inflammatory effects on the airway.
Dendritic cells (specialized macrophage-like cells) take up allergens and migrate to local lymph nodes where they present the allergenic peptides to uncommitted T-lymphocytes to program the production of allergen-specific T cells.
Structural cells of the airways, including epithelial cells, fibroblasts and airway smooth-muscle cells, are an important source of inflammatory mediators driving chronic inflammation in asthmatic airways.
Neurotrophins, which may be released from various cell types in peripheral tissues, may cause proliferation and sensitization of airway sensory nerves.
The characteristic structural changes: Increased airway smooth muscle, fibrosis, angiogenesis, and mucus hyperplasia leading to irreversible narrowing of the airways
PATHOGENESISPathogenesis of COPD
Noxious particles and gases
Genetic factors Host factors Respiratory infection Other Lung inflammation
Anti-oxidants Anti-proteinases
Oxidative stress Proteinases
---------------------------------Repair mechanisms
COPD pathology
COPD Noxious agent
COPD airway inflammation
CD8+ T-lymphocytes Neutrophils Macrophages
(Airflow limitation) Completely irreversible
PATHOGENESIS

RCMP Bulletin page: 12
Although there is a proportion of patients even with mild or moderate asthma that have a predominance of neutrophils.
PREVALENCE
The prevalence of asthma is ~10–12% of adults and 15% of children in developing countries. A rising incidence appears to be associated with increased urbanization. Asthma can present at any age with a peak age of 3 years. In childhood, twice as many males as females are asthmatic, but by adulthood the sex ratio has equalized.
PREVALENCE
Data from prevalence surveys carried out in a number of countries, using standardized methods and including spirometry, estimate that up to about one-quarter of adults aged 40 years and older may have airflow limitation classified as Stage I: Mild COPD or higher.
CLINICAL FEATURES AND DIAGNOSIS
A clinical diagnosis of asthma is often prompted by symptoms such as episodic breathlessness, wheezing, cough, and chest tightness. (Night/early morning)Episodic symptoms after an incidental allergen exposure, seasonal variability of symptoms and a positive family history of asthma and atopic disease are also helpful diagnostic guides.
CLINICAL FEATURES AND DIAGNOSIS
There may be no abnormal physical findings between each attack or when asthma is under control.Typical physical signs during attack are inspiratory, and to a great extent expiratory, wheezes throughout the chest, and there may be hyperinflation.
CLINICAL PRESENTATION
Consider COPD, and perform spirometry, if any of these indicators are present in an individual over age 40. These indicators are not diagnostic themselves, but the presence of multiple key indicators increases the probability of a diagnosis of COPD.• Dyspnea: Progressive (worsens over time)Usually worse with exercisePersistent (present every day)Described by the patient as an “increased effort to breathe,” “heaviness,” “air hunger,” or “gasping.”• Chronic cough: May be intermittent and may be unproductive.• Chronic sputum production:Any pattern of chronic sputum production may indicate COPD.• History of exposure to risk factors:Tobacco smoke (including popular local preparations).Occupational dusts and chemicals.Smoke from home cooking and heating fuel.EXAMINATIONIn the early stages: entirely normal physical examination Current smokers: signs of active smoking, including an odor of smoke or nicotine staining of fingernailsMore severe disease: Prolonged expiratory phase and expiratory wheezing/signs of hyperinflation (barrel chest)/sitting in the characteristic “tripod” position/cyanosis
CLINICAL FEATURES AND DIAGNOSIS
The three most common symptoms in COPD are cough, sputum production, and exertional dyspnea.A diagnosis of COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and/or a history of exposure to risk factors for the disease. The diagnosis should be confirmed by spirometry

RCMP Bulletin page 13
To confirm the diagnosis of asthma
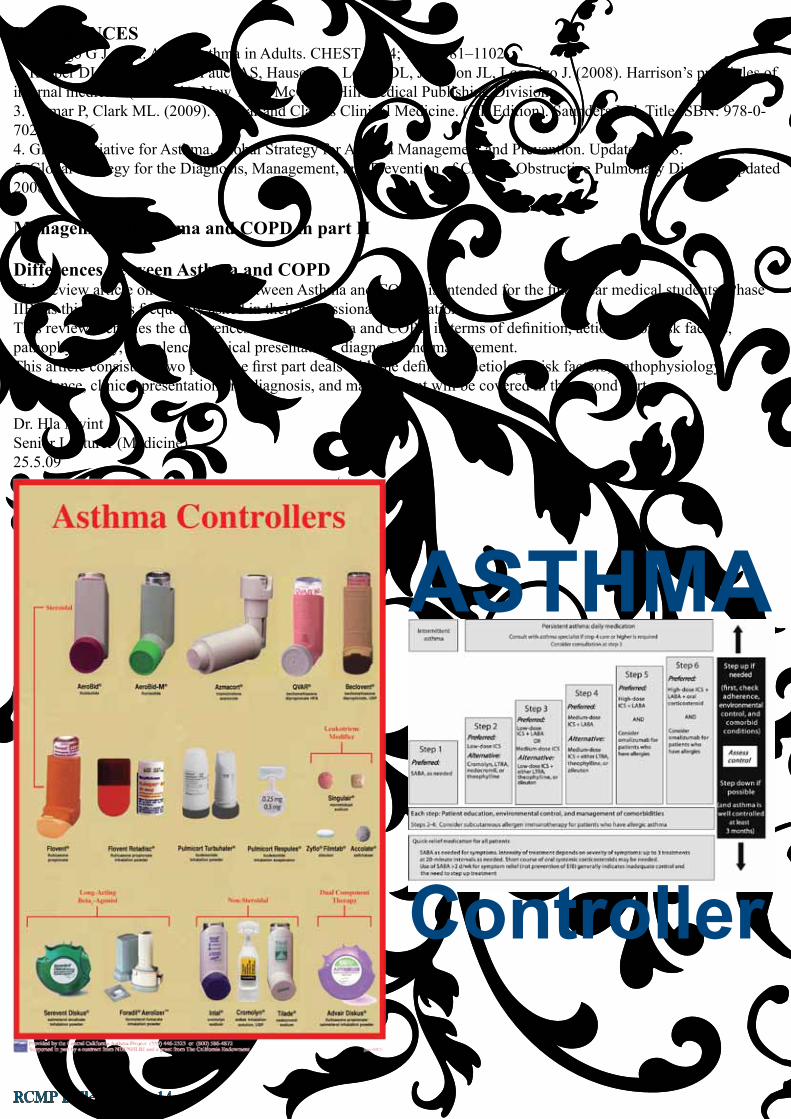
The degree of reversibility in FEV1 which indicates a diagnosis of asthma is generally accepted as ≥ 12% and ≥ 200 ml from the pre-bronchodilator value.Although spirometry is the preferred method of documenting airflow limitation, a 60 L/min (or 20% or more of prebronchodilator PEF) improvement after inhalation of a bronchodilator, or diurnal variation in PEF of more than 20% suggests a diagnosis of asthma.
Classification of Asthma Severity by Clinical
Features Before Treatment*IntermittentSymptoms less than once a weekBrief exacerbationsNocturnal symptoms not more than twice a month• FEV1 or PEF a 80% predicted• PEF or FEV1 variability < 20%Mild PersistentSymptoms more than once a week but less than once a dayExacerbations may affect activity and sleepNocturnal symptoms more than twice a month• FEV1 or PEF a 80% predicted• PEF or FEV1 variability < 20 – 30%Moderate PersistentSymptoms dailyExacerbations may affect activity and sleepNocturnal symptoms more than once a weekDaily use of inhaled short-acting _2-agonist• FEV1 or PEF 60-80% predicted• PEF or FEV1 variability > 30%Severe PersistentSymptoms dailyFrequent exacerbationsFrequent nocturnal asthma symptomsLimitation of physical activities• FEV1 or PEF ` 60% predicted• PEF or FEV1 variability > 30%*The worst feature determines the severityClassification.Its main limitation is its poor value in predicting what treatment will be required and what a patient’s response to that treatment might be. (GINA)For this purpose, a periodic assessment of asthma control (refers to control of the manifestations of disease) is more relevant and useful. (GINA)
DIAGNOSIS
Spirometric Classification of SeverityStage I: Mild FEV1/FVC < 0.70 FEV1 ≥ 80% predictedSymptoms of chronic cough and sputum production may be present, but not always.Stage II: Moderate FEV1/FVC < 0.70 50% ≤ FEV1 < 80% predictedStage III: Severe FEV1/FVC < 0.70 30% ≤ FEV1 < 50% predictedStage IV: Very Severe FEV1/FVC < 0.70 FEV1 < 30% predicted or FEV1 < 50% predicted plus chronic respiratory failure
FEV1: forced expiratory volume in one second; FVC: forced vital capacity; respiratory failure: arterial partial pressure of oxygen (PaO2) less than 8.0 kPa (60 mm Hg) with or without arterial partial pressure of CO2 (PaCO2) greater than 6.7 kPa (50 mm Hg) while breathing air at sea level.Additional investigations1. Bronchodilator reversibility testing. Despite earlier hopes, neither bronchodilator nor oral glucocorticosteroid reversibility testing predicts disease progression, whether judged by decline in FEV1, deterioration of health status, or frequency of exacerbations in patients with a clinical diagnosis of COPD and abnormal spirometry.2. Arterial blood gas measurementThis test should be performed in stable patients with FEV1 < 50% predicted or with clinical signs suggestive of respiratory failure or right heart failure.3. Alpha-1 antitrypsin deficiency screening- COPD at a young age (< 45 years) - A strong family history of the diseaseA serum concentration of 1 antitrypsin < 15-20% of the normal value is highly suggestive of homozygous 1 antitrypsin deficiency.
DIAGNOSIS
When performing spirometry, measure:• Forced Vital Capacity (FVC) and• Forced Expiratory Volume in one second (FEV1).Calculate the FEV1/FVC ratio. Spirometric results are expressed as % predicted using appropriate normal values for the person’s sex, age, and height.Airflow limitation (FEV1/FVC < 70%;FEV1 ≥ 80% predicted) and sometimes, but not always, chronic cough and sputum production.
RCMP Bulletin page: 14
REFERENCES1. Rodrigo G J. et al. Acute Asthma in Adults. CHEST 2004; 125:1081–11022. Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. (2008). Harrison’s principles of internal medicine (17th Ed.). New York: McGraw-Hill Medical Publishing Division.3. Kumar P, Clark ML. (2009). Kumar and Clark’s Clinical Medicine. (7th Edition). Saunders Ltd. Title ISBN: 978-0-7020-2993-64. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. Updated 2008.5. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Updated 2008.
Management of asthma and COPD in part II
Differences between Asthma and COPDThis review article on ‘Differences between Asthma and COPD’ is intended for the final year medical students (Phase IIB) as this topic is frequently asked in their professional examination.This review identifies the differences between asthma and COPD in terms of definition, aetiology or risk factors, pathophysiology, prevalence, clinical presentation, diagnosis and management. This article consists of two parts: the first part deals with the definition, aetiology/risk factors, pathophysiology, prevalence, clinical presentation and diagnosis, and management will be covered in the second part.
Dr. Hla MyintSenior Lecturer (Medicine)25.5.09
ASTHMA
Controller

RCMP Bulletin page 15
Chemistry And P h a r m a c y
CHEMISTRY AND LIVE
S u b m i t t e d b y : M a y w a n H a r i o n o , D e p a r t m e n t o f P h a r m a c y , U n i K L - R C M P
Have you ever wondered why ice melts and water evaporates? Why leaves turn colors in the fall and how a battery generates electricity? Why keeping food cold slows their spoilage and how our bodies use food to maintain life? Chemistry supplies answers to these questions and countless others like them.
Chemistry is the study of the properties of materials and the changes that materials undergo. One of the joys of learning chemistry is seeing how chemical principles operate in all aspects of our lives, from everyday activities like lighting a match to more far-reaching matter like the development of drugs to cure cancer.Chemistry provides important understanding of our world and how it works. It is an extremely practical science that greatly impacts our daily living. Indeed, chemistry lies near the heart of many matters of public concern: improvement of health care, conservation of natural resources, protection of the environment, and provision of our everyday needs for food, clothing, and shelter. Using chemistry, we have discovered pharmaceutical chemicals that enhance our health and prolong our lives. We have increased food production through the development of fertilizers and pesticides. We have developed plastic and other materials that are used in almost every facet of our lives. Unfortunately, some chemicals also have the potential to harm our health or the environment. It is in our best interests as educated citizens and consumers to understand the profound effects, both positive and negative, that chemicals have on our lives and to strike an informed balance about their usage.
Talking about pharmacy, the first thing that we remember about this term is a drug. Pharmacy is the study of compounds that are used in the health improvement and to prolong our lives. In fact, whether organic or inorganic, the drug is a chemical compound. Pharmacy studies about a chemical compound that starts from the chemical isolation from natural products or synthetic, evaluation of pharmacological activity, drug design, formulation in the pharmaceutical dosage forms, and its clinical application.
Figure 1. Some of the chemistry phenomenon such as melting ice, water evaporation, and battery generation
RCMP Bulletin page: 16
Why chemistry is very important in pharmacy studies? Using chemistry, we can isolate the chemical compound from natural product. The first thing we should consider when we want to isolate chemical from natural product is the solvent choice. How can we decide which solvent is suitable to extract and to isolate the chemical compound? The answer is the suitable polarity between chemical and solvent. How can we know that? Of course, the molecule structure will show how polar it is. Almost drug is presented as organic compound. Physical-organic chemistry explains how molecule structure influences their polarity. Therefore, flavonoide glycoside, i.e. epigallo catechine from green tea, is a polar substance that is preferred to be extracted by water which is also a polar solvent. In contrast, terpenoide such us taxol (anticancer) from paclitaxel, which has length hydrocarbon chain tend to be extracted by chloroform, a non polar solvent, because of its non polar properties.
Figure 3. The molecule structure of epigallo catechine from green tea (left side) and taxol from paclitaxel (right side)

RCMP Bulletin page 17
Drug isolation from natural products yields only in a very little quantity. Production of synthetic compound solves that problem in purpose of the scaling up development. How can we make a synthetic compound? Of course, using organic chemistry we can design what reagent should be used in reaction and what catalyst should be added to make its reaction faster. Curcumin, the yellow pigment from turmeric (Curcuma sp L.) that has been found having antioxidant, anticancer, anti-inflammatory and antibacterial effect which can be synthesized by reacting vanillin and 2, 4-pentanedione.
Pharmacology is the study about how drug can influence the anatomy-physiological function disorder in the body. Specifically, it talks about pharmacokinetic and pharmacodynamic of the drug. Pharmacokinetic explains about the drug absorption, its distribution, metabolism, and excretion. Chemistry will explain why Phenobarbital, a hypnotic drug, has the absorption better than its salt, sodium phenobarbital. Because when phenobarbital has been presented in gastro-intestinal area, it will be kept in a molecule form that will be absorbed faster than its salt which is easier to be an ionized form. Acid-base properties of the drug will influence which organ can absorb it better. Aspirin, a pain killer, has acid property, therefore it will be absorbed in a gastric better than in an intestine. In contrast, quinine, antimalaria, has a base character so it will be absorbed in an intestine better than in a gastric.
Distribution of the drug into site of action will be influenced by their drug-plasma protein binding site. Once the drug has bound strongly to the protein in a large quantity, it will be distributed poorly. Why are the drug highly bound to protein? Biochemistry will answer that the drug which can form hydrogen bond, disulfide bond or coordinative bond that will be highly bound to the protein site. The dose should be adjusted to reach the same drug plasma concentration in the different volume of distribution. A drug which has been strongly bound to albumin is diazepam, one of tranquilizers.
H3CO
HO
O O
OCH3
OH
H3CO
HO
H
O
+
O
H3C
O
CH3
vanillin
2,4-pentanedione
curcumin
Figure 4. The reaction of curcumin synthesis (left side) and turmeric rhizome (right side)
H3CO
HO
O O
OCH3
OH
H3CO
HO
H
O
+
O
H3C
O
CH3
vanillin
2,4-pentanedione
curcumin
H3CO
HO
O O
OCH3
OH
H3CO
HO
H
O
+
O
H3C
O
CH3
vanillin
2,4-pentanedione
curcuminH3CO
HO
O O
OCH3
OH
H3CO
HO
H
O
+
O
H3C
O
CH3
vanillin
2,4-pentanedione
curcumin
Figure 5. The molecule structure of Phenobarbital, sodium Phenobarbital, aspirin and quinine
RCMP Bulletin page: 18
H3CO
HO
O O
OCH3
OH
H3CO
HO
H
O
+
O
H3C
O
CH3
vanillin
2,4-pentanedione
curcumin
Figure 6. The molecule model of albumin and the molecul structure of diazepam
Metabolism is talking about a biotransformation of a drug from the non polar molecule structure to be the polar itself that is catalyzed by a liver enzyme, cytochrome (CYP) P450. What reaction will be carried out during this transformation? Oxidation, reduction, hydrolysis, glucuronidation, and sulfation will polarize the drug and cause it to be excreted from the body. Usually, the drug is active when they were in the non polar form. How can metabolism influence the drug effect? The drug which has first pass effect will be metabolized faster than the normal itself. Therefore, it will reduce the active form of drug in giving the maximum therapeutic effect. The dose adjustment should be administered during this phenomenon. How can we recognize which drug will be oxidize or hydrolyze by cytochrome P450. Of course, the molecule structure will show their reactivity toward a certain reaction. Paracetamol, a fever reducer, tend to be metabolized whereby glucuronidation after oxidation during the first phase metabolism. Because the oxidation of paracetamol become p-N-acetylaminobenzoquinon (NAPQ) is not polar enough to be eliminated from the body, glucuronidation is highly required to avoid this drug accumulation in the body.
Figure 7. The metabolism pathway of paracetamol
Excretion is the end of the long trip of the drug through the body. The drug excretion depends on the polarity of drug that has been talked above, its molecule size and a renal pathophisiology. The glomerulus of the kidneys will allowed the drug in the certain molecule size that is permeable toward glomerulus membrane. How can we know the molecule size of drug? Of course, from the molecule structure we will be able to calculate molecule weight itself. How can we recognize the normal function of the renal? One of the ways to identify that condition is by using clearance creatinin calculation. Creatinin is the kind of external protein. More over, it’s about biochemistry of protein. While pharmacokinetic is talking about the destiny of the drug through the body, pharmacodynamic is talking about the response of organ toward the drug. Its response will depend on the drug-receptor interaction. Receptor is kinds of protein that will specifically bind the drug depend on their specific part of structure and thermodynamic energy binding suitability. In recent development, the thermodynamic energy binding can be calculated computationally via receptor docking. This is very helpful in drug design

RCMP Bulletin page 19
and discovery. Therefore, we will not waste our time to examine the unknown compound one by one without any reasonable consideration to ensure that one can be prospected to be the new drug or not. Computational method on medicinal chemistry that has been familiar in quantitative structure-activity relationship (QSAR) studies will predict the probability of unknown compound to be developed as a new drug.
Formulation is the activity that the drug will be prepared in a pharmaceutical dosage form. It will deliver the drug to be taken effectively, efficiently, safety and acceptably by patient. Formulation will talk about the dose calculation, what preparation will be formulate, incompatibility of the drug both in physically or chemically. Chloramphenicol palmitate is less bitter than its base, an anti typhoid antibiotic, therefore, chloramphenicol palmitate is more suitable than chloramphenicol itself when it is administered to the pediatric patients. But chloramphenicol palmitate is less soluble in water than chloramphenicol base. How can we recognize their own drugs? Of course, it depends on its molecule structure. Chloramphenicol palmitate is an ester that is less polar than the base form itself. Therefore, the dosage form that is suitable for chloramphenicol palmitate is a suspension. A suspension is a solid drug dispersion in water that is stabilized by a suspending agent. The suspending agent is a chemical compound that has both polar and non polar properties in its molecule. Once more, it’s about the chemical structure.
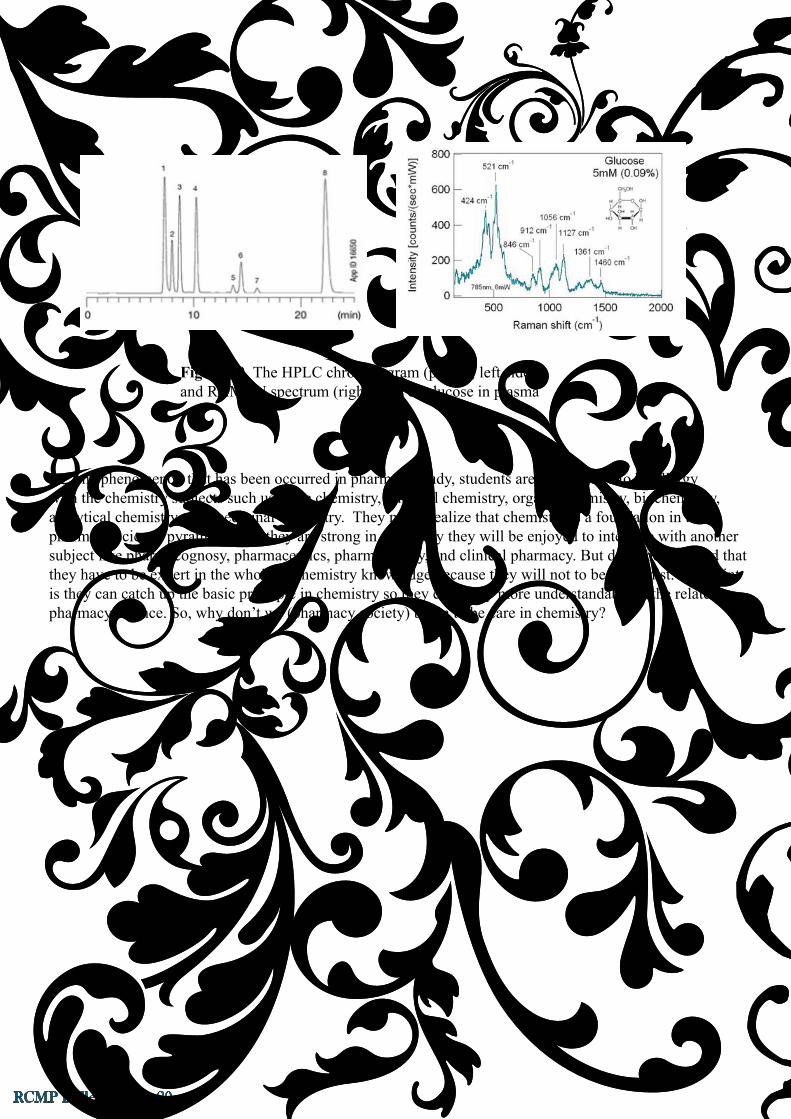
Has it been much enough? Not yet. Clinical pharmacy is the top of applied pharmacy sciences. One part of clinical practices is a clinical data interpretation. The question is how can we obtain the clinical data such us blood sugar concentration, blood cholesterol level, SGPT-SGOT etc.? Of course, the answer is the application of instrumental analytical chemistry. We can detect and calculate the presence of chemical compound in biological sample such us urine, plasma, saliva, tears, feces and sweat by HPLC and spectroscopy instrument. The principle of analytical chemistry will be applied during operation this instrument.
Figure 8. The histaminic receptor docking to the agonist
H3CO
HO
O O
OCH3
OH
H3CO
HO
H
O
+
O
H3C
O
CH3
vanillin
2,4-pentanedione
curcumin
Figure 9. The molecule structure of chloramphenicol and chloramphenicol palmitate and its suspension
RCMP Bulletin page: 20
Figure 10. The HPLC chromatogram (peak 4; left side) and RAMAN spectrum (right side) of glucose in plasma
One phenomenon that has been occurred in pharmacy study, students are seemed like to be allergy with the chemistry subjects such us basic chemistry, physical chemistry, organic chemistry, biochemistry, analytical chemistry, and medicinal chemistry. They never realize that chemistry is a foundation in the pharmacy science pyramid. Once they are strong in chemistry they will be enjoyed to integrate with another subject like pharmacognosy, pharmaceutics, pharmacology, and clinical pharmacy. But don’t be assumed that they have to be expert in the whole of chemistry knowledge because they will not to be a chemist. The point is they can catch up the basic principle in chemistry so they can study more understandable in the related pharmacy science. So, why don’t we (pharmacy society) begin to be care in chemistry?
RCMP Bulletin page 21
Medical Education Experience in Singapore
Five gruelling days. Getting up at the crack of dawn, rushing to catch the train and bus, following a non-stop 9 to 5 schedule of lectures, discussions and brainstorming sessions, all with barely enough time to catch a breath. It was a far cry from home, where I had the car even for short trips; not getting my daily exercise from rushing to catch the bus. The fast-paced, physically taxing week in Singapore showed me just how pampered we are here. This trip, however, has proven to be a really worthwhile and gainful experience, and I thank Dr Cheong for encouraging me to go.
This outing actually involved 2 workshops: Best Practices in Assessment, and Evaluation and Curriculum Design, organized and held at the National University of Sinagapore School of Medicine. The workshops were very well organized and were participated by representatives from numerous institutions in Malaysia as well as other regions e.g. Thailand, the Phillipines and the Middle East. In some activites, we were divided into small groups and given tasks to carry out, present and discuss. This opened my eyes to how different our opinions can be, despite being in the same field. I also got to know a good number of doctors from different parts and universities on a more personal level, thereby affording me a larger pool of talent to network and share ideas.
One thing I noticed though was that there were many Singaporean consultants interested in teaching who actively participated. This goes to show that academics from this part of the world are now taking serious interest in medical education. While several Malaysian universites still do not have a medical education unit, I believe that it is now time for us at UniKL/RCMP to start one of our own.
Currently, there is a very passionate debate on seemingly two contradictory positions on medical education establishments. One group believes the success achieved in recent years by medical schools in transforming students into good physicians the traditional way; the other poses a less congratulatory view. The latter argues that medical schools are remarkably resistant to adopting the science of medical education. They think medical schools are lagging behind in the advancement in the science of education management, and becoming more and more redundant. Most of us, who are teachers now, have likely been brought up by the teacher-centric trditional method of medical education whereby we’re fed lots and lots of facts to remember. The paradigm has now shifted in the reverse, more student-centred direction. Now, we need to determine what sort of doctors we want to produce, and then put in the process accordingly to produce that end.
I have no intention to go into the details of what I have learned at this point, perhaps if there is interest, I will share some thoughts and readings in future ebulletin postings.
Posted by Dr C.T. Chua

RCMP Bulletin page: 22
N E W S&UPDATES
Recruitment Trip To London
Change managementThe true change manager starts with redefining the purposes of the organisation in the light of fully analysed external change. Next come the internal changes required if those purposes are to be met. Then you tackle the people, starting at the top. Will they or won’t they whole-heartedly accept the new purposes and internal reforms? If they won’t or can’t, they can’t stay - especially if their job is chief executive.
Solutions like these may be tough to implement ? and we are the first to admit it. But unless you are aware of what needs doing, it’s unlikely you’ll ever become a top manager
“Look, we can’t fall into old patterns.We have to think of a plan!”- Lisa Simpson

RCMP Bulletin page 23
Announcement Of Deputy Dean
Practikal StudentUNIKL RCMP OPEN DAY
16 MAY
2009
Staff on duty: 70
Visitors:
50 public and 440 students from 11 schools:-
SMK Raja Permaisuri Bainun, Ipoh
SMK Agama Raja Perempuan Ta’ayah, Ipoh
SMK Sultan Yussuf, Batu Gajah, Perak
Sekolah Berasrama Penuh Integrasi
Gopeng,Perak
SMK Agama Kerian, Simpang Empat,
Semanggol, Perak
SM Sains Raja Tun Azlan Shah, Taiping
SMK King Edward VII, Taiping
MRSM Lenggong, Perak
MRSM Pengkalan Hulu, Perak
MRSM Taiping, Perak.
Kolej Mara Kuala Nerang, Kedah

RCMP Bulletin page: 24
MEMOTo : All Staff and Students From :RoseSuzilaYahaya,OfficerHumanCapitalDepartment c.c :ProfessorDr.HashamibinBohari,HeadofCampus/Dean
Date :25thMay2009
Ref.No. :PCMSB/UNIKLRCMP/HR/MEMO/9007/091/05/09
Subject :AdjournmentofUniKLRCMPThirdAssembly
Last Saturday night, Prof. Dato’ Dr. Abdul Hakim bin Juri, President of UniKL has announced that all sport contingents members have been given leave on Monday (25th May 2009).
As such, our third assembly is now being adjourned to Wednesday, 27th May 2009. Venue, time and itinerary remain unchanged. Please be informed accordingly.
All inconvenience is highly regretted.
Thank you.
Best regards,
Rose Suzila YahayaHuman Capital Department
/rsy
UNIVERSITIKUALALUMPURROYALCOLLEGEOFMEDICINEPERAK(HUMANCAPITALDEPARTMENT)MEMO

RCMP Bulletin page 25
KINDLY BE INFORMED THAT DR. MOHD AZHAR BIN MOHD NOOR, HEAD OF OBSTETRIC & GYNECOLOGY TOGETHER WITH HIS SON, MOHAMED AFZANIZAL HAD UNDERGO A KIDNEY TRANSPLANT OPERATION ON FRIDAY 15TH MAY 2009. DR. MOHD AZHAR DONATED ONE OF HIS KIDNEYS TO HIS ELDEST SON MOHAMED AFZANIZAL.
DR. MOHD AZHAR WAS DISCHARGED ON TUESDAY, 19 MAY 2009 AND IN THE PROCESS OF RECOVERY AT HIS RESIDENT IN KUALA LUMPUR BUT HIS SON IS STILL IN ICU FOR FUTHER OBSERVATION. IMMEDIATELY AFTER THE OPERATION MOHAMED AFZANIZAL WAS PUT UNDER SUPERVISION BY FOUR GROUPS OF CONSULTANTS FROM NEFROLOGY AND UROLOGY IN GENERAL HOSPITAL KUALA LUMPUR. HIS IS NOW IN STABLE CONDITION.
TO ALL UNIKL RCMP CITIZEN LET US ALL PRAY FOR HIS SPEEDY RECOVERY AND FINALLY BE ABLE TO RESUME WORK AS USUAL AS SOON AS POSSIBLE.
THANK YOU.
EXECUTIVE
CORPORATE COMMUNICATION
DR. MOHD AZHAR MOHD NOOR - KIDNEY TRANSPLANT OPERATION

RCMP Bulletin page: 26
HAPPY MULTIPLEXINGDr.V. GopalakrishnanSenior Lecturer in Microbiology University Kuala Lumpur-Royal College of Medicine Perak
Introduction
Before the introduction of molecular techniques, laboratory diagnosis of infections, especially viral infection, relied on isolation, detection of antigen or antibodies of specific agents from the various fluids of the human system, which usually provide only retrospective evidence of infection. Impact of laboratory diagnosis of viruses on acute patient management was relatively small because of the time taken for the virus to replicate and produce a characteristic cytopathic effect in cell culture or for development of a specific antibody response.
Polymerase chain reaction (PCR)
Advent of molecular diagnostic methods in diagnosis, especially for viral diseases, has drastically reduced the time for detection of the etiological agent. During the recent past polymerase chain reaction and other DNA signal and target amplification techniques have resulted in these molecular diagnostics becoming key procedures in detection and identification of a pathogen. Standard PCR usually uses one pair of primers to amplify a specific sequence. Routine use of PCR is increasing in diagnostic laboratory settings and in research laboratories.
Multiplex PCR (MPCR)
Recent developments in PCR technology facilitate the development of multiplex PCR, one variant that overcomes the previous shortcomings and also increases the diagnostic capability of PCR. MPCR uses multiple pairs of primers to amplify many sequences simultaneously. The presence of many PCR primers in a single tube could cause many problems, among these, the increased formation of mis-primed PCR products and “primer dimérs”, and the enhanced amplification of shorter DNA fragments. The technique using more than one pair of primers helps in detection of more than one target sequence in a reaction. It has rapidity, saving considerable time and effort without compromising on quality and utility.
The utility of multiplex PCR has been successfully applied in many areas of nucleic acid diagnostics, which include gene deletion analysis, mutation and polymorphism analysis, quantitative analysis, and RNA detection. The use of MPCR in infectious diseases has received high acclaim and is widely used as a valuable method for identification and detection etiologies including typing and analysis of transgenic organisms, amplification of multiple DNA regions for SNP analysis, amplification and analysis of micro satellites, and typing of and detection of bacteria and viruses fungi and/or parasites.
Studies have been conducted to improve the utility of the PCR technique for routine use in a diagnostic laboratory, by designing a single multiplex PCR assay and also to increase the molecular sensitivities of the assays used to raise confidence in a negative result. Combinations of such multiplex PCR have been standardized to detect the pathogens. Based on improvisations on this technique, systems are in place to detect pathogens on organ system based infections. For example multiplex PCR have been developed to detect etiological agent of keratoconjuntivitis, by using primer pairs to detect HSV, adenovirus and Chlamydia trachomatis (the common etiologies of keratoconjuntivits). Similarly,

RCMP Bulletin page 27
combination PCR has been developed to detect agents in genital ulcer disease, acute respiratory infections and so on.
Development of multiplex PCR should follow a rational approach by way of including or excluding the detection of specific pathogens by the assay. Selection of these pathogens can be organ specific or symptom specific or be based on the epidemiology of the pathogens. Few straightforward solutions like hot start PCR or use of Amplitaq in the PCR assay greatly improve the sensitivity and specificity of the assay, by way of eliminating non specific reactions.
Application
PCR has greatly improved the sensitivity of detecting mutations in genomic DNA. e.g.: 12 mutations have been detected in gastric carcinomas; multiple mutations in the cystic fibrosis gene as well as ‘ras’ oncogenes in gastrointestinal cancers. In addition, primer-mediated restriction polymorphism has enhanced by 20%, the sensitivity of detection of codon 12 k-ras mutations in colorectal cancers. Another application of multiplex PCR is microdeletion screening. This can be applied to the ‘X’ and ‘Y’ chromosomes (male genomic DNA) or to hybrid cell lines (rodent-human) containing only one copy of a human chromosome of interest. To detect the etiologic agent of acute conditions such as meningitis and encephalitis a technique rapid enough should be employed. Multiplex PCR has proved to be one such powerful tool. Added to this, the feasibility of simultaneous screening for viruses, bacteria and parasites in CSF specimens has increased the utility of the multiplex PCR in meningitis and encephalitis.
Conclusion
Thorough evaluation and validation of new PCR and multiplex PCR procedures is essential by means of checking the sensitivity and specificity of the assay using purified nucleic acids. Through its speed, reliability and sensitivity, PCR assay has met the specific criteria of the diagnostic laboratory. In years to come, PCR will become the “gold standard” test for microbial infections, mainly viral infections.
RCMP Bulletin page: 28
On Monday 18 May 2009, a meeting was held in Putrajaya between UniKL, MARA and MoHE chaired by the Sec Gen of MoHE. The meeting was also attended by representatives from EPU, MoF, and KKLW (Kem Kemajuan Luar Bandar & Wilayah).
At the meeting, the Sec Gen of MOHE confirmed that the YAB Prime Minister in a discussion with the Chief Secretary to Government (KSN) has agreed and decided that UniKL shall remain under MARA and not transferred to MoHE.
Please be informed that the latest decision will not be made known through the media. As such, all matters concerning UniKL and its relationship to MARA (i.e. study loan, etc) remains and continue as usual. Staff involved in handling enquiries from students and parents may say that a decision has been made that UniKL stays with MARA. Thank you. Sincerely, Prof Dato’ Dr Abdul Hakim Juri, DSAP, BSc, PhD, FMSET, Federal Cross of Merit GermanyPresident / Chief Executive OfficerUniversiti Kuala Lumpur1016 Jalan Sultan Ismail50250 Kuala LumpurTel : +603 21754007 Fax : +603 21754567URL : www.unikl.edu.my
UniKL to Remain Under MARA
RCMP Bulletin page 29
MEMO
RCMP Bulletin page: 30
Penang Tuan Haji Md. Tamin bin Haji Ali
Ipoh Encik R. EllagupillaiThe late Encik N. Nadarajah (later to serve Kuala Lumpur).
Kuala Lumpur The late Encik N. Ponnampalam (brother of Encik N. Nadarajah)
Seremban The late Encik Wong Chan Leng
Malacca Tuan Haji Ismail
byHj. Silahudin Jarjis Mat Jiri
This paper is being written with the intention of exposing the younger generation of radiographers to the history of the radiological services and training of radiographers in Malaysia.
Chronology of Significant Related Events
SUMMARY OF THE RADIOLOGICAL SERVICES AND TRAINING OF RADIOGRAPHERS IN MALAYSIA
Pioneers In The Field Of Diagnostic Radiography
X-ray Departments were normally operated by a few selected Dressers, later renamed as Hospital Assistants. Retrospectively, the few Dressers that that could be identified as pioneers in the field of Radiology were listed as follows:-
Radiologists of The Same Era
Colonial Radiologists that contributed immensely and also paved the way towards the expansion of the radiological services in Malaysia up to the moment of Merdeka were:
• Dr. J.S Webster• Dr. J.S. Winchester• Dr. G.B. Garlick• Dr. D.R. McPherson• Dr. C.T. MacArthy• Dr. W.B. Young
A Dr. P.T.K. Nayer was also identified, and later served in Alor Setar until his retirement.
The Japanese Occupation (1941 – 1945)
The Japanese Imperial Army completely took over the x-ray services in the country. An x-ray worker was paid $3.00 a day (banana currency) and 90 cents a day to a darkroom worker plus free ration of rice, sugar and Japanese cigarettes.
The Return of the British Administration (1946 – 1957)
September 1945 •The British Military Administration took over the Radiological Services in the country.
•The X-ray Department of General Hospital Kuala Lumpur was under the charge of a military radiologist assisted by army radiographers.•The first civilian radiologist to assume office in Kuala Lumpur was Dr. C.T. MacArthy (also the Medical Officer in-charge of the General Hospital).•Manual processing was the order in fashion of the day.•Radiographs were hung up to dry on clothes line.
The First Organised Training Programme For X-ray Staff 1947
• The first organized training programme for x-ray personnel was established through the initiative and indefatigable effort by Dr. C.T. MacArthy.• Six Hopital Assistants were selected from all the states to undergo training in the X-ray Department of the General Hospital, Kuala Lumpur.• The training duration was increased from 1 year to 18 months.• Training was divided into 2 parts – theory and practical.
3rd February 1896 The first x-ray set was installed in Taiping, Perak just a few months following the discovery of x-ray by Prof. W.C. Roentgen.The first so-called patient was an ikan bawal putih (pomfret)
October 1897 20 months following the Taiping installation, Ipoh received its first x-ray set donated by Messrs Yeow Tet Sin and Li Thung, in commemoration of Queen Victoria’s Diamond Jubilee.
15 February 1910 General Hospital Kuala Lumpur acquired its first x-ray set.21 Septemebr 1910 Penang General Hospital received its first x-ray set from Messrs Siemens Brothers.15 February 1934 Mr. Chee Swee Seng donated an x-ray set to the General Hospital, Malacca.

RCMP Bulletin page 31
• Lectures at the Technical College (now Universiti Teknologi Malaysia) of Jalan Semarak, Kuala Lumpur.• Practical – in the X-ray Department of the General Hospital Kuala Lumpur by an expatriate radiographer – a Mrs. Mann.• Upon graduation, the successful candidates were designated as X-ray Assistants.
1949
•Dr. D.R. McPherson succeeded Dr. MacArthy and Mrs. Mann was replaced by Miss Meeke (Mrs. Simon).•Dr. D.R.McPherson was instrumental in bringing about further changes to the radiological services throughout the country.•Old equipment were condemned and new equipment, mainly Philips were installed.
The First Overseas Training for X-ray Assistants
•Three X-ray Assistants were awarded Federal Government Scholarships to pursue a 2-year course in Radiography leading to the Diploma of the Society of Radiographers, United Kingdom, (now known as the College of Radiographers).•In view of their previous training and experience, the training programme was shortened to 18 months.•Subsequently, many other x-ray assistants were given the same opportunities to complete their training in Radiography, in Glasgow, London, Melbourne and Auckland.•Dr. McPherson eventually retired and was succeeded by Dr. W.B. Young.•Miss Meeke was succeeded by Miss Yeast, who was later replaced by Miss Pope (the last of the colonial Radiographers).
The First Malaysian Radiologist 1951
•Penang acquired its first full-time radiologist, Dr. Richard Paul.•Dr. Richard Paul introduced the first light beam diaphragm centring device.•Dr. T.D. Brick subsequently succeeded Dr. Richard Paul.•Eventually, Dr. Omar bin Din, the first Malaysian Radiologist took over from Dr. Richard Paul.•Dr. Omar bin Din played a very significant role in the development of radiological services in Malaysia in the post Merdeka era.
The Inaugration of the Federation of X-ray Staff Union
1st April 1956 - September 1969
•The inaugural meeting of the Federation of X-ray Staff Union was held in Ipoh.•The Union was to play a very important role in bringing about all improvements pertaining to salary structure, terms and conditions of service.•The Union was admitted as an affiliate of the International Society of Radiographers and Radiological Technicians (ISRRT) in Tokyo.
The Merdeka Years (1958 – 1969)
1957 •Dr. Omar bin Din succeeded Dr. W.B. Young as the new local Consultant Radiologist.•Dr. Omar bin Din brought about tremendous progress and
development to x-ray departments throughout the country both in terms of personnel and equipment.
February 1972
•General Hospital Kuala Lumpur moved into its new 13 rooms X-ray Department, with its modern and sophisticated medical imaging equipment.•Dr. Omar bin Din received his Datukship (J.M.N.) for his outstanding services.•Y.B. Dato’ Dr. Haji Omar bin Din left the service to go into private practice.•The late Y.B. Dato’ Dr. Hussein bin Abdul Ghani took over the onerous duties of Consultant Radiologist, States of Malaysia.
The School of Radiography, General Hospital Kuala Lumpur
1960•Mr. K.C. Denley and Mr. W.J. Ashworth, two high ranking officials of the Society of Radiographers, United Kingdom were invited by the Malaysian Health Ministry to inspect the local School of X-ray Assistants, with a mission to elevate its training programme and status to that of a School of Radiography, which would be recognized as one of its external training centres in Asia.
8th March 1963
•Mr. E.J.W. Quick, a Council Member of the Society of Radiographers, United Kingdom, arrived in Kuala Lumpur to discharge his duties as a Colombo Plan Adviser to the local School of Radiography.•The fist intake of students for diagnostic radiography training was from the rank of and file of hospital assistants and a staff nurse.
1964
The second and subsequent intakes were made from school certificate secondary school leavers, with five credits.•The first intake of four radiotherapy students joined the first year training only. They completed their final training in Hong Kong.•Mr. E.J.W. Quick acquired concessions from the Society of Radiographers, United Kingdom to enable all Malaysian X-ray Assistants who could not be admitted into the local School of Radiography, to qualify as Radiographers by sitting a section, a part or parts, as the case may be, of the Society of Radiographers, U.K. examinations as external students.•The Society of Radiographers, U.K. was generous enough to flex the ruling by granting the following concessions:
X-Ray Assistant Examinationsi) Less than 5 years’ service Part 1 & 2ii) More than 5 years’ but less than 10 years’ service Part 2iii) More than 10 years’ service Special Viva
• Eventually, most of the X-ray Assistants, qualified as Radiographers in this manner.
26 December 1963

RCMP Bulletin page: 32
•Mr. E.J.W. Quick completed his tour of duty.•His place was taken over by Tuan Hj. Ahmed Meah bin Baba Ahmed.
1964 •Tuan Hj. Ahmed Meah bin Baba Ahmed was appointed as the first Principal.
The Australian Correspondence Course
The course was spread over a period of 3 years. The successful candidates were awarded a Certificate of Competency by the Conjoint Board which is equivalent to the Diploma of Radiography of the College of Radiographers, U.K.
The National Tuberculosis Centre (Pusat TIBI Negara, now known as the Institut Perubatan Respiratori, Hospital Kuala Lumpur)
•In the early sixties, the National Tuberculosis Centre was established with Dr. Sodhy as the Head of the Centre. •Mr. D. Lack from Australia was appointed as the Colombo Plan Adviser to organize and implement the Mass Miniature Radiography (M.M.R.) campaign to eradicate tuberculosis.•Several mobile and static X-ray units toured the whole country on a survey mission.•Mobile x-ray operators were recruited by the Malaysian Ministry of Health.
Institute of Neurology, General Hospital Kuala Lumpur
•Cerebral angiography was started in Kuala Lumpur in 1965•Two diagnostic radiographers were later sent to Chicago and Montreal to undergo post-graduate training in cerebral angiography.
Institute of Radiotherapy, Oncology & Nuclear Medicine
•In 1965, Dato’ Dr. S.K. Dharmalingam was appointed as the first Malaysian Consultant Radiotherapist.•Its modern and sophisticated apparatus was regarded among the best part in South East Asia.•The modernized department enabled the establishment of a practical training placement of therapeutic student radiographers, in full compliance of the requirement of the College of Radiographers, U.K.
The University Hospital
•The University Hospital was established in 1966.•It was equipped with a modern X-ray Department, comprising of the most modern and sophisticated apparatus, donated by the Australian Government.•The department’s first Radiologist was Dr. H. Luke and subsequently succeeded by Prof. Dr. Joginder Singh.•The first Senior Radiographer was Mr. Lord and the first Malaysian Senior Radiographer was Mr. Alwin Kan.
The Malaysian Society of Radiographers
•The Malaysian Society of Radiographers was officially registered with the Registrar of Societies in February 1968.•Became the official Malaysian affiliate to the International
Society of Radiographers and Radiological Technicians (I.S.R.R.T.)•In April 1975, The Malaysian Society of Radiographers hosted the Fourth Teachers’ Seminar in Kuala Lumpur, whereby 34 countries from all over the world, congregated in Kuala Lumpur.
The Therapeutic Arm of The School of Radiography, General Hospital Kuala Lumpur.
1st May 1969, Mr. E.R. Hutchinson assumed office as the Colombo Plan Adviser, and helped to pave the way to establish a therapeutic training programme for radiographers at General Hospital Kuala Lumpur.
The National University of Malaysia (U.K.M.)
•The first two–room Radiology Department was inaugurated in April 1978.•The department was headed by Prof. Dr. Ismail Saad.
Current Training Centres For Medical Imaging (Radiography)
A. Government Sector
Diploma Level : College of Allied Health Science, Sg. Buloh. College of Radiography & Medical Imaging, HSA Johor Bahru. College of Medical Imaging, PPUM. Fakulti Sains Kesihatan Bersekutu, UiTM Jalan Othman.
Degree Level : Fakulti Sains Kesihatan Bersekutu, UKM. Fakulti Sains Kesihatan Bersekutu, UiTM Jalan Othman. Jabatan Pengimejan Bioperubatan, Fakulti Perubatan, Universiti Malaya, Lembah Pantai, Kuala Lumpur.
B. Private Sector Diploma Level : UniKL RCMP, Ipoh Perak. MAHSA, Kuala Lumpur. MASTERSKILL, Cheras. KIST, Bachok, Kelantan.
Degree Level : Fakulti Sains Kesihatan Bersekutu, UIA, Kuantan.
References:
DR. F.Y. KHOO, 1981, “X-Rays in Singapore” 1st Edition, Pages 6, 13, 43, 56. Singapore University Press for the Radiological Society of Singapore.
HAJI AHMED MEAH & ENCIK KWOK KOON KOW, “Brief History of The Radiological Services in Malaysia”, Pages 10 – 17, Majuray December 1983, Journal of The Malaysian Society of Radiographers.

RCMP Bulletin page 33
To all members of the Academic Staff and Student of UniKL RCMP are cordially invited for the UniKL RCMP‐Nestle Nutrition CME programme. Topic: Establishment Of Microbiota and Influencing Factors Including C section ‐ Concept Of Probiotics Speaker: Assoc. Prof. Dr Patricia , Conway Centre of Marine Biofueling and BioInnovation, School of Biotechnology and Biomolecular Sciences, University of New South Wales, Australia. Chairman: Assoc. Prof. Dr Abdul Karim Russ Hassan, Microbiology Unit , Universiti Kuala Lumpur Royal College of Medicine Perak. Date & Time: Friday, 12th June 2009 @ 11.30 AM ‐12.30 PM Followed by refreshment/lunch Place: Blue Lecture Theatre, UniKL RCMP The CME Programme is sponsored by Nestle Nutrition. For further inquiry please contact Assoc Prof. Dr Karim [email protected] or ext: 152
CME Programme

RCMP Bulletin page: 34
NETBALL-4 APRIL - HBUK
No. Nama Jawatan Bola Sepak
BolaTampar
SepakTakraw
BolaJaring
Badminton
Bowling
PingPong
1 Nur Azlina Bt Mohd Said Pegawai x x
3 Azrul Nizuan Pembantu Tadbir x4 Shahrul Ramadhan Bin Khalili Pegawai x x5 Abdol Roes B. Md Som Pembantu Tadbir x x6 Khairol Anuar Sharif Pembantu Am x7 Azlan Abdul Hamid Juruteknik ( Bangunan) x x8 Hasni Bin Hassan Juruteknik ( Bangunan) x x9 Normarziah bt. Mohd Noor Pembantu Tadbir x
10 Kapten (B) Zabani Bin Hj. Abdul Pengurus Jabatan Modal Insan x x11 Zulhelmi Bin Yahya Arif Pembantu Tadbir x12 Marina Binti Abdul Kadir Eksekutif x13 Nor Azrin Bt. Abdul Samad Pembantu Tadbir x14 Nor Fairuz Liyana Bt. Ahmad Pembantu Tadbir x
15 Nor Azhar Bin Abdullah Penolong Pengurus x16 Noorhayati Binti Hawari Eksekutif x x17 Tun Hazman Bin Abd Latif Pegawai x x18 Abd. Hadi Faruq Bin Ab Wahab Juruteknik IT x x19 Ahmadil Ekhwan Bin Ali Juruteknik IT x x
Mr. Thian Yee Wei2
Senarai staf UniKL RCMP yang terlibat dengan SSUK 2009 di UniKL MSI, Kulim
Pejabat Dekan
Jabatan Pentadbiran & Kewangan
Jabatan Modal Insan
Penolong Pengurus Besar Kewangan & Pentadbiran x
Jabatan Teknologi Maklumat
Perkhidmatan Akademik

RCMP Bulletin page 35
Recreation Exco, Sports & Recreation Club UniKL RCMP will organising aerobic class for staff fitness. Below are the details. Those who interested to participate, just come at our first session (2nd June 2009, Tuesday) to register.
AEROBIC EXERCISE CLASS
· Day : Tuesday
· Time : 5.30 pm to 6.30 pm
· Starting date : 2nd June 2009
· Venue : Uni KL RCMP (foyer level 3)
· Fees : Members - free
Non-members - RM 10 per month
For more info, please contact :
i) Cik Nurfizah (ext : 206)
ii) Cik Hikmah (ext : 219)
A e r o b i c E x e r c i s e C l a s s i s B a c k ! ! ! !


















