HORMONAL CONTROL OF MAMMOGENESIS, LACTOGENESIS, AND GALACTOPOIESIS.
Upload
chastity-daltonCategory
view
237download
7
Dystocia

2
Breastfeeding
3
What is lactogenesis?
Lactogenesis is a series of cellular changes by which mammary epithelial cells differentiate and mature into secretory cells. This process occurs in two stages. Stage 1 : takes place during the second half of pregnancy and marks the development of secretory units in the breast and the production of small amount of milk. After about 15 to 16 weeks of gestation, a minute amount of milk containing lactose and casein is secreted. Further differentiation of mammary epithelial cells is prevented by the high levels of circulating progesterone during pregnancy. This stage also notably coincides with colostrum production.
Lactogenesis is a series of cellular changes by which mammary epithelial cells differentiate and mature into secretory cells. This process occurs in two stages. Stage 1 : takes place during the second half of pregnancy and marks the development of secretory units in the breast and the production of small amount of milk. After about 15 to 16 weeks of gestation, a minute amount of milk containing lactose and casein is secreted. Further differentiation of mammary epithelial cells is prevented by the high levels of circulating progesterone during pregnancy. This stage also notably coincides with colostrum production.
4
Lactogenesis
Following delivery, circulating progesterone levels become markedly decreased with removal of the placenta. This hormonal change, along with the elevation of both prolactin and cortisol, triggers the onset of copious milk production, known as stage 2 of lactogenesis.
Following delivery, circulating progesterone levels become markedly decreased with removal of the placenta. This hormonal change, along with the elevation of both prolactin and cortisol, triggers the onset of copious milk production, known as stage 2 of lactogenesis.

5
Lactogenesis
*Lactation is maintained and regulated throughout the breastfeeding period by multiple hormones. Removal of milk from the breast via nipple stimulation triggers the release of prolactin and oxytocin from the anterior and posterior pituitary gland, respectively.
* *Prolactin is required for milk secretion, whereas oxytocin is responsible for the contraction of myoepithelial cells leading to milk ejection. A breastfeeding occurrence will result in an elevation of blood prolactin for the next breastfeeding.
*Lactation is maintained and regulated throughout the breastfeeding period by multiple hormones. Removal of milk from the breast via nipple stimulation triggers the release of prolactin and oxytocin from the anterior and posterior pituitary gland, respectively.
* *Prolactin is required for milk secretion, whereas oxytocin is responsible for the contraction of myoepithelial cells leading to milk ejection. A breastfeeding occurrence will result in an elevation of blood prolactin for the next breastfeeding.
6
How can I counsel a woman regarding initiation, frequency and duration of breastfeeding?According to the American Academy of Pediatrics, breastfeeding should begin promptly after birth. Although nursing is frequency based on infant demand, it is recommended that it occur approximately 8 to 12 times per day. The duration of feeding varies among individuals. The time spent breastfeeding decreases as the infant matures. Typically, 10 to 15 minutes is spent on each breast immediately after delivery. By one month of age, the infant spends approximately 8 to 10 minutes per breast during feeding.
According to the American Academy of Pediatrics, breastfeeding should begin promptly after birth. Although nursing is frequency based on infant demand, it is recommended that it occur approximately 8 to 12 times per day. The duration of feeding varies among individuals. The time spent breastfeeding decreases as the infant matures. Typically, 10 to 15 minutes is spent on each breast immediately after delivery. By one month of age, the infant spends approximately 8 to 10 minutes per breast during feeding.

7
Is supplementation necessary for infants who
are breastfeeding? Breast milk is often sufficient as the sole source of nutrition during the first six months of life. In the case of prematurity or maternal iron deficiency, it is recommended that iron supplements be added to the infant’s diet. In addition, vitamin D may also be given before six months of age to infants with inadequate exposure to sunlight or whose mothers are deficient. Formula supplementation is recommended if an infant shows failure to thrive while breastfeedig and efforts to improve nursing are unsuccessful.
Breast milk is often sufficient as the sole source of nutrition during the first six months of life. In the case of prematurity or maternal iron deficiency, it is recommended that iron supplements be added to the infant’s diet. In addition, vitamin D may also be given before six months of age to infants with inadequate exposure to sunlight or whose mothers are deficient. Formula supplementation is recommended if an infant shows failure to thrive while breastfeedig and efforts to improve nursing are unsuccessful.
8
What are the benefits of breastfeeding?
Research outlining the significant health advantages of breastfeeding in both infants and mothers is widespread. In addition to providing superior nutrition for the newborn, breast milk contains immunoglobulins (largely secretory IgA) that offer protection against infection. *Colostrom: a thick , yellowish milky fluid sometimes secreted near the end of pregnancy, and particularly the second or third day postpartum.
Research outlining the significant health advantages of breastfeeding in both infants and mothers is widespread. In addition to providing superior nutrition for the newborn, breast milk contains immunoglobulins (largely secretory IgA) that offer protection against infection. *Colostrom: a thick , yellowish milky fluid sometimes secreted near the end of pregnancy, and particularly the second or third day postpartum.
9
What are the benefits of breastfeeding?
Colostrom contains high levels of secretory IgA. Human milk also carries factors that stimulate cellular growth and differentiation in the newborn.Breastfeeding benefits the mother as well. During milk let-down, oxytocin is released, which causes uterine contractions and a decreased risk of both ovarian and breast cancer associated with breastfeeding in women.
Colostrom contains high levels of secretory IgA. Human milk also carries factors that stimulate cellular growth and differentiation in the newborn.Breastfeeding benefits the mother as well. During milk let-down, oxytocin is released, which causes uterine contractions and a decreased risk of both ovarian and breast cancer associated with breastfeeding in women.

10
Definition
**Dystocia literally means difficult labor and it is characterized by abnormally slow progress of labor
It is the consequence of four distinct abnormalities that may exist singly or combination
**Dystocia literally means difficult labor and it is characterized by abnormally slow progress of labor
It is the consequence of four distinct abnormalities that may exist singly or combination

11
**How is labor different for a multiparous woman than a nullip
aroue one?Nulliparous: fetal descent and cervical effacement occur before dilation. The process of descent and effacement can start weeks before active labor begins.Multiparous: effacement and descent often do not begin until well into active labor. Frequently, descent does not occur until the second stage.
Nulliparous: fetal descent and cervical effacement occur before dilation. The process of descent and effacement can start weeks before active labor begins.Multiparous: effacement and descent often do not begin until well into active labor. Frequently, descent does not occur until the second stage.
12
How does one determine if the patient is truly in active
labor? Women presenting with painful contractions who are less than 4 cm dilated should be evaluated for the contraction pattern characteristic of active labor. In the absence of a good contraction pattern, a lack of cervical change after an hour of observation indicates that the women is not in active labor.
Women presenting with painful contractions who are less than 4 cm dilated should be evaluated for the contraction pattern characteristic of active labor. In the absence of a good contraction pattern, a lack of cervical change after an hour of observation indicates that the women is not in active labor.
13
How does one determine if the patient is truly in active
labor? Nulliparous women in latent and early labor frequently experience hypertonic contraction patterns that are painful but do not produce cervical change. In these cases, once fetal well-being has been established therapeutic rest can bring the woman relief and either stop the contractions altogether or allow the woman to wake up in active labor. Medications that can be used for therapeutic rest include sedatives, antihistamines, and narcotics.
Nulliparous women in latent and early labor frequently experience hypertonic contraction patterns that are painful but do not produce cervical change. In these cases, once fetal well-being has been established therapeutic rest can bring the woman relief and either stop the contractions altogether or allow the woman to wake up in active labor. Medications that can be used for therapeutic rest include sedatives, antihistamines, and narcotics.

14
How does one determine if the patient is truly in active
labor?
Artificial rupture of membranes during latent labor is relatively contraindicated during latent labor, as the risk of infection, cord prolapse, and malpresentation are great.
Artificial rupture of membranes during latent labor is relatively contraindicated during latent labor, as the risk of infection, cord prolapse, and malpresentation are great.

15
Abnormal of the powers(uterine contractility and maternal expulsive effort)
Abnormalities of passenger(the fetus)Abnormalities of the passage(the birth canal)Abnormalities of the psychologic factors
Abnormal of the powers(uterine contractility and maternal expulsive effort)
Abnormalities of passenger(the fetus)Abnormalities of the passage(the birth canal)Abnormalities of the psychologic factors
What causes dysfunctional labor (dystocia) **
16
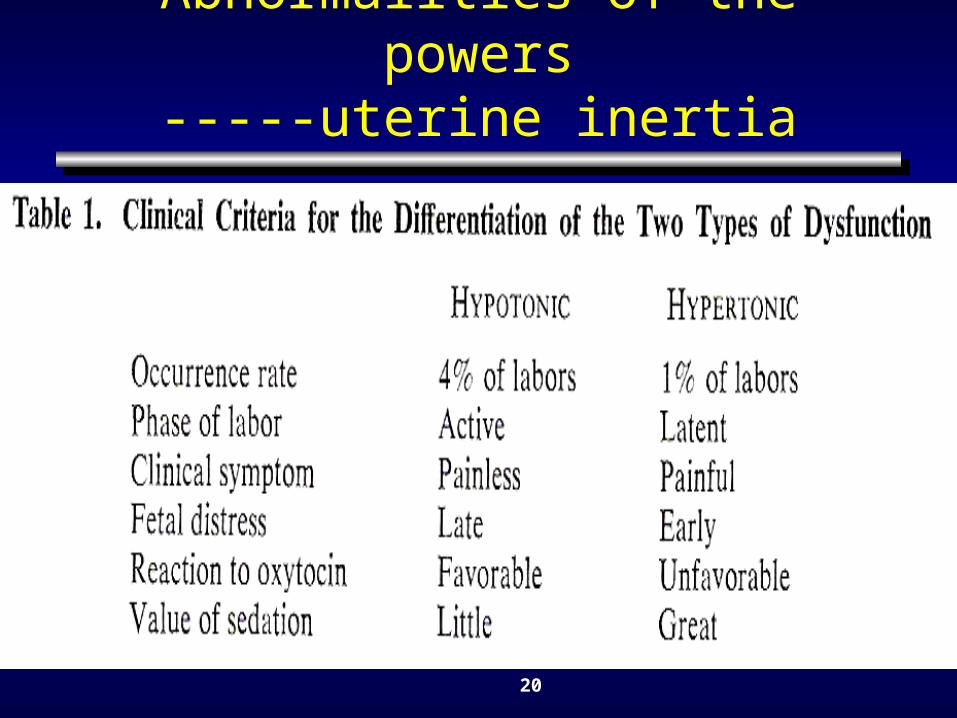
Abnormalities of the powers
Uterine dysfunction hypotonic primary
uterine inertia secondary
Uterine hypertonic
Dysfunction
uterine hypercontractility
Uterine dysfunction hypotonic primary
uterine inertia secondary
Uterine hypertonic
Dysfunction
uterine hypercontractility
17
**What constitutes an abnormal constraction pattern?
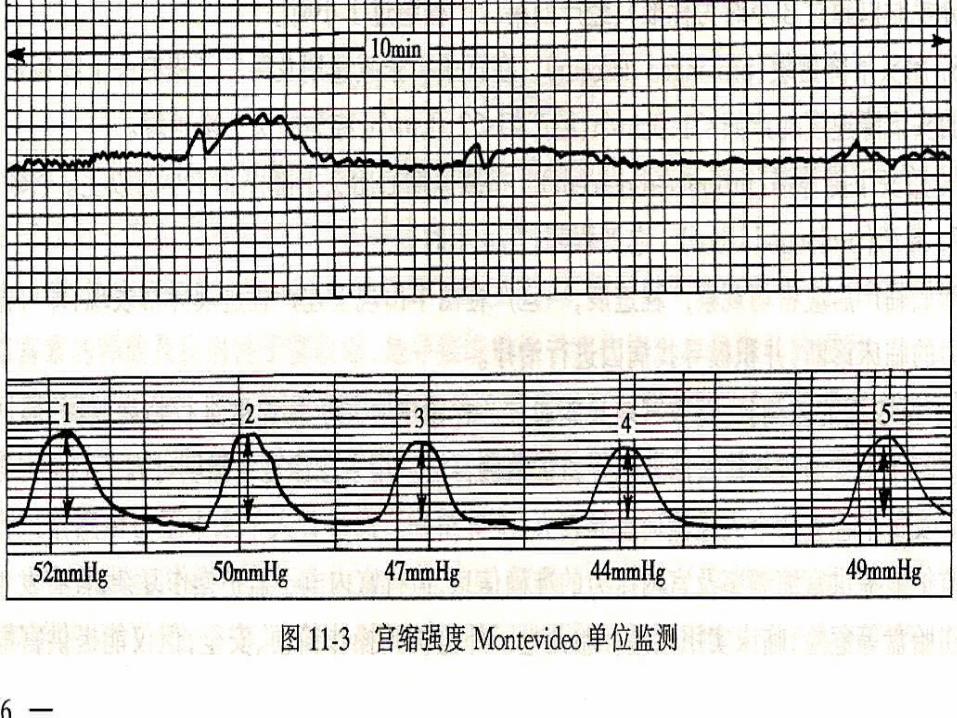
In active labor, an effective labor pattern usually consists of contractions that occur every 2 to 5minutes, last approximately 60 sec , have a resting tone of 10mmHg, and have an apical intrauterine pressure of at least 40mmHg. Both approaching and into the second stage, contractions usually become more frequent and intense (occurring every 2 to 3 minutes).
In active labor, an effective labor pattern usually consists of contractions that occur every 2 to 5minutes, last approximately 60 sec , have a resting tone of 10mmHg, and have an apical intrauterine pressure of at least 40mmHg. Both approaching and into the second stage, contractions usually become more frequent and intense (occurring every 2 to 3 minutes).

18
**What constitutes an abnormal constraction pattern?
An ineffective contraction pattern can be either hypotonic or hypertonic.
* Hypotonic contractions are coordinated but do not create sufficient intrauterine pressure for labor to progress.
* Hypertonic contractions are characterized by strong but disorganized myometrial activity that causes significant intrauterine pressure but fails to effect progress.
An ineffective contraction pattern can be either hypotonic or hypertonic.
* Hypotonic contractions are coordinated but do not create sufficient intrauterine pressure for labor to progress.
* Hypertonic contractions are characterized by strong but disorganized myometrial activity that causes significant intrauterine pressure but fails to effect progress.
19
Abnormalities of the powers-----uterine inertia
Etiology of uterine inertia**Cephalopelvic disproportion or Fetal malpositi
on Abnormal of uterine muscleImbalance of endocrine systemAdministration of analgesiapsychical-factorsOthers : fatigue
Etiology of uterine inertia**Cephalopelvic disproportion or Fetal malpositi
on Abnormal of uterine muscleImbalance of endocrine systemAdministration of analgesiapsychical-factorsOthers : fatigue
20
Abnormalities of the powers-----uterine inertia

21
At what point is labor considered
dysfunctional?
There are several different established time frames used to monitor the progress of active labor. The Friedman Curve is the oldest and probably still the most widely used.
There are several different established time frames used to monitor the progress of active labor. The Friedman Curve is the oldest and probably still the most widely used.

22

23
Abnormalities of the powers-----uterine inertia
Clinical findingsFailure to progress:* Lack of progressive cervical
dilatation*Lack of fetal decent
Clinical findingsFailure to progress:* Lack of progressive cervical
dilatation*Lack of fetal decent
24
**Prolonged latent phase:>20 hours in a primiparous patient, >14 hours in a multparous patient.**Protraction disorders: slower than normal cervical dilation or descent of the fetus. See table below.**Arrest disorders: no cervical dilation in >2 hours in the active phase or an arrest of descent of the fetus ( no movement in >1 hour in the second stage of labor).
**Prolonged latent phase:>20 hours in a primiparous patient, >14 hours in a multparous patient.**Protraction disorders: slower than normal cervical dilation or descent of the fetus. See table below.**Arrest disorders: no cervical dilation in >2 hours in the active phase or an arrest of descent of the fetus ( no movement in >1 hour in the second stage of labor).
25
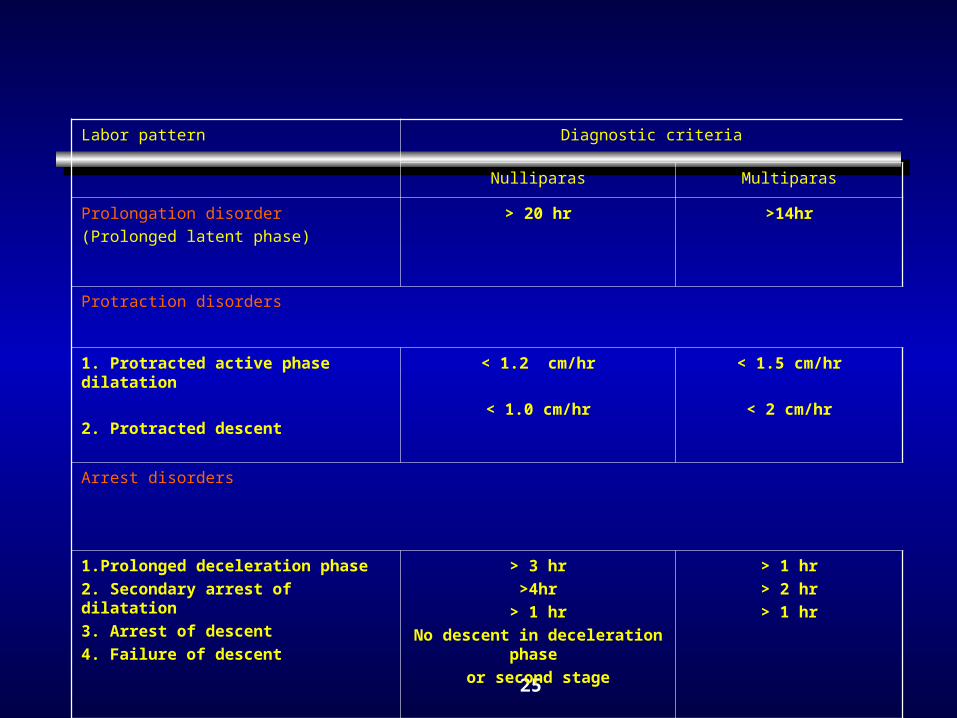
Labor pattern Diagnostic criteria
Nulliparas Multiparas
Prolongation disorder
(Prolonged latent phase)
> 20 hr >14hr
Protraction disorders
1. Protracted active phase dilatation
2. Protracted descent
< 1.2 cm/hr
< 1.0 cm/hr
< 1.5 cm/hr
< 2 cm/hr
Arrest disorders
1.Prolonged deceleration phase
2. Secondary arrest of dilatation
3. Arrest of descent
4. Failure of descent
> 3 hr
>4hr
> 1 hr
No descent in deceleration phase
or second stage
> 1 hr
> 2 hr
> 1 hr

26
Abnormalities of the powers-----uterine inertia
DiagnosisPalpation:
strength
duration
frequency
Tocodynamometer
Vaginal examination
DiagnosisPalpation:
strength
duration
frequency
Tocodynamometer
Vaginal examination
27

28
**What are effects of uterine inertia on mother and fetus
mother fatigue
acidosis infection postpartum hemorrhage cesarean section rate
fetus birth injury , distress
prolapse of umbilical cord stillbirth
mother fatigue
acidosis infection postpartum hemorrhage cesarean section rate
fetus birth injury , distress
prolapse of umbilical cord stillbirth

29
How can I augment hypotonic uterine contractions?
1.general management psychological support nutrition support sedation 2.physical methods urethral catheterization enema (enteroclysis) acupuncture
1.general management psychological support nutrition support sedation 2.physical methods urethral catheterization enema (enteroclysis) acupuncture
30
How can I augment hypotonic uterine contractions?
3. medication: *Pitocin (oxytocin) can correct hypotonic contraction patt
erns associated with causes other than infection: The standard of care is to start intravenous Pitocin at 1 to
2 milliunits per minute via pump and increase by 1 to 2 milliunits every 15 to 20 minutes until contractions are every 2 to 3 minutes, lasting 60 seconds, and without signs of fetal distress. Although protocols vary. Pitocin should be limited to 20 milliunits per minute until further assessment has been made.
oxytocin : 2.5U + 5%GS 500ml 5mU/ml begin from 8drop / min Diazepam 10mg iv
3. medication: *Pitocin (oxytocin) can correct hypotonic contraction patt
erns associated with causes other than infection: The standard of care is to start intravenous Pitocin at 1 to
2 milliunits per minute via pump and increase by 1 to 2 milliunits every 15 to 20 minutes until contractions are every 2 to 3 minutes, lasting 60 seconds, and without signs of fetal distress. Although protocols vary. Pitocin should be limited to 20 milliunits per minute until further assessment has been made.
oxytocin : 2.5U + 5%GS 500ml 5mU/ml begin from 8drop / min Diazepam 10mg iv

31
How can I augment hypotonic uterine contractions?
4. AROM : Slow labor can also be augmented by artif
icial rupture of membranes (AROM). AROM is both safest and most effective when the cervix is at least 4 to 5 cm dilated and the fetal head is engaged.
Performing amniotomy before the head is engaged can allow the cord to prolapse, a life-threatening situation for the fetus that requires an emergency cesarean section.
4. AROM : Slow labor can also be augmented by artif
icial rupture of membranes (AROM). AROM is both safest and most effective when the cervix is at least 4 to 5 cm dilated and the fetal head is engaged.
Performing amniotomy before the head is engaged can allow the cord to prolapse, a life-threatening situation for the fetus that requires an emergency cesarean section.

32
Abnormalities of the powers-----uterine inertia
Hypertonic
Sedative
CS
Hypertonic
Sedative
CS

33
Abnormalities of the powers----- hypercontractility
Clinical findings and diagnosis*Precipitate delivery: <=3h
Constriction ring of uterus
Tetanic contraction of uterus
Clinical findings and diagnosis*Precipitate delivery: <=3h
Constriction ring of uterus
Tetanic contraction of uterus
34
What are the effects of hypercontractility on mother and fetus
Precipitate delivery:<=3h soft birth canal trauma Rupture of uterus Fetal distress Fetal death stillbirth
Precipitate delivery:<=3h soft birth canal trauma Rupture of uterus Fetal distress Fetal death stillbirth
35
Abnormalities of the powers----- hypercontractility
ManagementProphylaxisTocolytic therapiesForcepsOperation
ManagementProphylaxisTocolytic therapiesForcepsOperation