Dysphagia in Duchenne Muscular Dystrophy Assessed Objectively by Surface Electromyography
11
ORIGINAL ARTICLE Dysphagia in Duchenne Muscular Dystrophy Assessed Objectively by Surface Electromyography Sally K. Archer • Rachel Garrod • Nicholas Hart • Simon Miller Received: 21 September 2011 / Accepted: 5 October 2012 / Published online: 21 November 2012 Ó Springer Science+Business Media New York 2012 Abstract Objective swallowing assessment is indicated in the management of patients with Duchenne muscular dys- trophy (DMD). Surface electromyography (sEMG) provides a non-invasive, objective method of quantifying muscle activity. It was hypothesised that the measurement of sEMG activity during swallowing would distinguish between pre- served and disordered swallow function in DMD. This comparative study investigated the peak, duration, and rel- ative timing of muscle activity during swallowing of four muscle groups: orbicularis oris, masseter, submental, and infrahyoid. The study included three groups of participants: Nine DMD patients with dysphagia (mean age = 21.7 ± 4.2 years), six DMD patients with preserved swallow func- tion (21.0 ± 3.0 years), and 12 healthy controls (24.8 ± 3.1 years). Dysphagic DMD participants produced signifi- cantly higher normalised peak amplitude measurements than the healthy control group for masseter (61.77 vs. 5.07; p B 0.01) and orbicularis oris muscles (71.87 vs. 26.22; p B 0.05). Intrasubject variability for masseter peak amplitude was significantly greater for dysphagic DMD participants than the other groups (16.01 vs. 5.86 vs. 2.18; p B 0.05). There were no differences in timing measure- ments between groups. Different characteristic sEMG waveforms were observed for the three groups. sEMG pro- vides useful physiological information for the evaluation of swallowing in DMD patients, justifying further study. Keywords Deglutition Á Deglutition disorders Á Dysphagia Á Duchenne muscular dystrophy Á Surface electromyography (sEMG) Á Assessment Á Neuromuscular disease Duchenne muscular dystrophy (DMD) is the most common childhood onset neuromuscular disorder and leads to degeneration of muscle fibres and progressive muscle weakness and death, usually when the patient is in his 20s [1]. Dysphagia is common in DMD, contributing to both mor- bidity and mortality and accelerating respiratory decline [2]. Following a Cochrane review in 2004, which recommended the establishment of appropriate swallowing assessments for patients with chronic muscle disease [2], a series of studies have used videofluoroscopy and questionnaires to investi- gate dysphagia in DMD [3–6]. All studies have shown that dysphagia worsens with age, with increasingly effortful mastication, reduced hyolaryngeal movement, and poor pharyngeal clearance, all attributed to progressive oropha- ryngeal weakness. A discrepancy between findings on vid- eofluoroscopy and subjective accounts has been reported, with patients often underreporting the difficulties observed on assessment [3–5]. These findings all suggest the need for detailed, reproducible, objective swallowing assessments that can quantify and regularly monitor the patients, who may themselves be unaware of their own difficulties. S. K. Archer (&) Centre for Human and Aerospace Physiological Sciences, School of Biomedical Sciences, King’s College London, Guy’s Campus, London SE1 1UL, UK e-mail: [email protected] S. K. Archer Á N. Hart National Institute for Health Research (NIHR) Biomedical Research Centre, Guy’s and St Thomas’ NHS Foundation Trust and King’s College London, London, UK R. Garrod Physiotherapy Department, King’s College Hospital NHS Foundation Trust, Denmark Hill, London, UK S. Miller 62 Southfield Road, Nailsea BS48 1JD, UK 123 Dysphagia (2013) 28:188–198 DOI 10.1007/s00455-012-9429-6
-
Upload
simon-miller -
Category
Documents
-
view
212 -
download
0
Transcript of Dysphagia in Duchenne Muscular Dystrophy Assessed Objectively by Surface Electromyography

ORIGINAL ARTICLE
Dysphagia in Duchenne Muscular Dystrophy Assessed Objectivelyby Surface Electromyography
Sally K. Archer • Rachel Garrod •
Nicholas Hart • Simon Miller
Received: 21 September 2011 / Accepted: 5 October 2012 / Published online: 21 November 2012
� Springer Science+Business Media New York 2012
Abstract Objective swallowing assessment is indicated in
the management of patients with Duchenne muscular dys-
trophy (DMD). Surface electromyography (sEMG) provides
a non-invasive, objective method of quantifying muscle
activity. It was hypothesised that the measurement of sEMG
activity during swallowing would distinguish between pre-
served and disordered swallow function in DMD. This
comparative study investigated the peak, duration, and rel-
ative timing of muscle activity during swallowing of four
muscle groups: orbicularis oris, masseter, submental, and
infrahyoid. The study included three groups of participants:
Nine DMD patients with dysphagia (mean age = 21.7 ±
4.2 years), six DMD patients with preserved swallow func-
tion (21.0 ± 3.0 years), and 12 healthy controls (24.8 ±
3.1 years). Dysphagic DMD participants produced signifi-
cantly higher normalised peak amplitude measurements than
the healthy control group for masseter (61.77 vs. 5.07;
p B 0.01) and orbicularis oris muscles (71.87 vs. 26.22;
p B 0.05). Intrasubject variability for masseter peak
amplitude was significantly greater for dysphagic DMD
participants than the other groups (16.01 vs. 5.86 vs. 2.18;
p B 0.05). There were no differences in timing measure-
ments between groups. Different characteristic sEMG
waveforms were observed for the three groups. sEMG pro-
vides useful physiological information for the evaluation of
swallowing in DMD patients, justifying further study.
Keywords Deglutition � Deglutition disorders �Dysphagia � Duchenne muscular dystrophy �Surface electromyography (sEMG) � Assessment �Neuromuscular disease
Duchenne muscular dystrophy (DMD) is the most common
childhood onset neuromuscular disorder and leads to
degeneration of muscle fibres and progressive muscle
weakness and death, usually when the patient is in his 20s [1].
Dysphagia is common in DMD, contributing to both mor-
bidity and mortality and accelerating respiratory decline [2].
Following a Cochrane review in 2004, which recommended
the establishment of appropriate swallowing assessments for
patients with chronic muscle disease [2], a series of studies
have used videofluoroscopy and questionnaires to investi-
gate dysphagia in DMD [3–6]. All studies have shown that
dysphagia worsens with age, with increasingly effortful
mastication, reduced hyolaryngeal movement, and poor
pharyngeal clearance, all attributed to progressive oropha-
ryngeal weakness. A discrepancy between findings on vid-
eofluoroscopy and subjective accounts has been reported,
with patients often underreporting the difficulties observed
on assessment [3–5]. These findings all suggest the need for
detailed, reproducible, objective swallowing assessments
that can quantify and regularly monitor the patients, who
may themselves be unaware of their own difficulties.
S. K. Archer (&)
Centre for Human and Aerospace Physiological Sciences,
School of Biomedical Sciences, King’s College London,
Guy’s Campus, London SE1 1UL, UK
e-mail: [email protected]
S. K. Archer � N. Hart
National Institute for Health Research (NIHR) Biomedical
Research Centre, Guy’s and St Thomas’ NHS Foundation Trust
and King’s College London, London, UK
R. Garrod
Physiotherapy Department, King’s College Hospital NHS
Foundation Trust, Denmark Hill, London, UK
S. Miller
62 Southfield Road, Nailsea BS48 1JD, UK
123
Dysphagia (2013) 28:188–198
DOI 10.1007/s00455-012-9429-6

Proactive management is recommended for DMD
patients [1] and requires appropriate and timely assessment.
The commonly applied swallowing assessments, e.g., the
bedside swallow assessment, videofluoroscopy and
fibreoptic endoscopic evaluation of swallowing (FEES), are
clinically valuable; however, none provides an easily
accessible, consistently reliable, and objective measure of a
patient’s swallow function. Surface electromyography
(sEMG) is a noninvasive technique that enables measure-
ment of muscle activity [7]. Previous data have shown that it
provides consistent results during swallowing [8], and peaks
in sEMG activity correlate with key swallowing events [9].
The method is easy to administer, can be used while patients
swallow normal food and fluids, and is well tolerated [10]. It
is therefore potentially useful for both single and serial
assessments, enabling the clinician to track change in a
patient’s muscle function over time. Thus, it could be ideally
suited to monitoring swallowing in progressive neuromus-
cular disease, enabling proactive management.
Despite this, there are limited data on the clinical appli-
cation of sEMG in swallowing assessment and, in particular,
on reporting its ability to distinguish between patients with
and without oropharyngeal dysphagia. Although a few
studies have attempted to produce normal ranges for sEMG
during swallowing, [11, 12], their data were not normalised,
which is a major limitation for clinical comparison. As with
other physiological measurements, sEMG activity must be
normalised or scaled against a reference measurement to
provide a meaningful comparison between subjects. This is
to counterbalance the changes in the signal amplitude which
are dependent on the anatomical recording site, extent of skin
preparation, the depth of subcutaneous tissue between the
skin and the muscles, and any variations in the geometry of
action potentials in the muscle with respect to the recording
electrodes [13].
No previous study has investigated the clinical useful-
ness of sEMG in the assessment of swallowing in DMD.
With multichannel sEMG, it is possible to assess several
groups of muscles simultaneously and, therefore, examine
both oral and pharyngeal muscle groups for signs of
myopathy. Previous electromyographic studies of limb
muscles in patients with myopathy reported a reduction in
electromechanical efficiency due to atrophy of muscle
fibres, with patients needing to activate more motor units
with a resultant increase in amplitude of activity to produce
a given force [14]. Furthermore, a decrease in the mean
duration of motor unit action potentials has been found,
reflecting the diffusely distributed loss of muscle fibres
within the motor unit [14–16]. It was therefore hypothe-
sised that sEMG assessment of dysphagic DMD patients
would demonstrate signs of myopathy in the muscles that
are active during swallowing. Specifically, dysphagic
DMD patients would produce increased muscle activity for
swallowing (relative to their maximum activity) compared
to healthy controls, and the activity would be shorter in
duration. It was anticipated that patients with DMD and
preserved swallow function are yet to develop these myo-
pathic changes to their swallowing muscles and therefore
their sEMG data would be comparable with that of healthy
controls. As such, it was hypothesised that non-invasive
measurement and quantification of swallow function by
sEMG would be able to distinguish between DMD patients
with preserved and disordered swallow function.
Methods
Study Design
A prospective, controlled, cross-sectional study was con-
ducted. Ethical approval was obtained from the Royal
Marsden Research Ethics Committee, and Research and
Development (R&D) approval was obtained from the
Guy’s and St Thomas’ R&D department. All participants
gave written informed consent.
Participants
Healthy Volunteers
Male students attending St George’s, University of Lon-
don, were recruited by advertisement. Inclusion criteria
were males aged 16–30 years. Exclusion criteria included
a history of neurological or neuromuscular disease and
dysphagia.
Patient Volunteers
Participants with DMD were recruited from the Lane Fox
Respiratory Unit Outpatient Clinic at St Thomas’ Hospital,
London. Inclusion criteria were a diagnosis of DMD and
age over 16 years. Exclusion criteria included a diagnosis
of any other neurological or neuromuscular disease and
cognitive impairment preventing informed consent. DMD
participants with a clinical history of dysphagia, as deter-
mined from the medical notes and speech and language
therapy database and a Functional Oral Intake Score
(FOIS) [17] of B6, were assigned to Group 1 and those
with no history of dysphagia, who had preserved swallow
function and FOIS of 7, were assigned to Group 2.
Study Protocol
Each participant’s data were collected in a single session of
less than 20 min. During the session, the DMD participants
remained in their usual seated position in their wheelchairs
S. K. Archer et al.: Dysphagia in Duchenne Muscular Dystrophy Assessed Objectively 189
123

and the control group participants were comfortably seated
upright on a plinth with a supporting back rest. Four
miniature preamplifiers [18] were used to record the sur-
face electromyogram of orbicularis oris muscle, masseter
muscle, infrahyoid muscles, and the submental muscle
group. The characteristics of the preamplifiers [18] were
gain of 91,000, common mode rejection ratio of
80–100 dB in the range 50–500 Hz, and frequency
response of 10–1,000 Hz. Prior to electrode placement, the
skin surface was prepared by shaving and then light abra-
sion with NuPrep skin preparative gel (Pulse Medical,
Surrey, UK). The preamplifiers were attached to the skin
with double-sided adhesive foam tape (3M Ltd, Bracknell,
UK). The recording electrodes were 5-mm-diameter Ag/
AgCl discs set in the plastic preamplifier housing, with
centres separated by 20 mm. A third electrode in the
housing acted as a virtual earth. Holes were punctured in
the foam tape, with the holes corresponding with the
electrodes, and were filled with Ten20 conductive paste
(Pulse Medical) to ensure skin contact. The preamplifiers
were then further secured in place on the skin with
Micropore surgical tape (MidMeds, Waltham Abbey, UK).
The placement of the electrodes had the same anatomical
coordinates as described in previous studies [10, 19], which
was confirmed by palpation of each muscle group while the
participant performed the different maximum voluntary
contractions (see below). Electrode placement was always
on the left side and in the vertical plane, as follows:
1. Orbicularis oris: One recording electrode placed
above the upper lip and one below the lower lip, with
the virtual ground lateral to the vermillion border at the
corner of the mouth.
2. Masseter: Electrodes placed vertically along the
masseter muscle.
3. Submental muscles: Electrodes placed midway
between the mandible and the hyoid bone, 1 cm from
midline.
4. Infrahyoid muscles: Electrodes placed lateral to the
thyroid cartilage.
The analogue signals were digitized at 1 kHz and cap-
tured by a data acquisition device [model 1401, Cambridge
Electronic Design (CED), UK] and recorded for sub-
sequent analysis with Spike 2 software ver. 5.20 (CED).
Sampling rate for all four channels was 1,000 Hz. The
signals were rectified and low-pass digitally filtered at
5 Hz, with a 2.5-Hz transition gap, giving filtering com-
parable to previous data [8]. Swallowing data were nor-
malised to the activity recorded during a maximum
voluntary contraction (MVC) of the same muscle group
[13]. After a short practice period to reduce the risk of
fatigue, the participants were instructed to perform three
MVC manoeuvres [20]:
1. Orbicularis oris: Maximal compression of the upper
and lower lips together
2. Masseter: Maximal teeth clenching
3. Submental and infrahyoid muscle groups: The partic-
ipant’s jaw was held closed firmly by the researcher
and the participant was asked to attempt to open their
jaw against this resistance.
Participants were then asked to complete six swallow
trials, each consisting of 5 ml of water administered via a
teaspoon, with a rest of approximately 10 s between
boluses. To reduce the risk of participants altering their
behaviour because of an awareness of being assessed (i.e.,
increasing volitional effort to swallow ‘‘better’’), the pur-
pose of the study was reinforced to the participants before
the swallow trials, i.e., examination of the assessment
capabilities of the equipment, not the individual’s swal-
lowing ability. For each trial, the participant was instructed
to ‘‘Swallow this in your usual way’’ in order to encourage
the participant to swallow normally.
Measurements
For each bolus, the sEMG graphic trace from the first
swallow elicited was examined for patterns, and measure-
ments were made of peak sEMG amplitude, duration of
sEMG activity, and relative onset of the sEMG activity
among the four muscle groups. Offline analysis of sEMG
data was done to avoid observer bias using Spike 2, with a
specific, dedicated software programme ‘‘Swallow EMG,’’
written by CED. To measure resting baseline activity,
vertical cursors were placed 1 s apart prior to the onset of
an MVC manoeuvre or swallow attempt. The software
calculated the mean ± 2 SD. ‘‘Onset’’ of the swallow was
defined as the point where baseline activity increased into a
swallow pattern, which was defined as the point at which
the EMG trace exceeded 2 SD above baseline for that
channel [19, 21]. If multiple peaks occurred above base-
line, measurements were made of the largest peak that
corresponded temporally with those in the other muscle
groups. The end of swallow activity was determined as the
point when the EMG trace returned to within 2 SD of
baseline levels. Mean durations were taken for each muscle
in each participant. To establish the pattern of muscle
activation, the mean onset of the muscle groups was
measured relative to the onset of the submental group,
which was designated as time 0. The submental muscle
group was chosen as it had been shown to produce reliable
sEMG activity during swallowing, which is associated with
hyoid elevation [7, 8]. Peak amplitudes for each muscle
group for each swallow and MVC were recorded and the
mean baseline was subtracted to control for differing levels
of noise and background electromyographic activity.
190 S. K. Archer et al.: Dysphagia in Duchenne Muscular Dystrophy Assessed Objectively
123

Data Analysis
Means and standard deviations (SD) were calculated across
each participant’s six swallows, and amplitude data were
normalised by conversion into a percentage of the mean
peak MVC for that muscle group. Intrasubject variation for
each measure was examined by comparing the SDs across
each individual’s six swallows. Medians and interquartile
ranges (IQR) of duration and normalised amplitude data
were compared between groups and analysed with the
Kruskal-Wallis test. The Mann-Whitney test was con-
ducted post hoc, adjusting for multiple testing by using the
Bonferroni Correction [22]. Means and SDs of the relative
timing of onset of activity were compared between groups
and analysed with the analysis of variance. Both Excel for
Windows Vista (Microsoft Corp., Redmond, WA, USA)
and the Statistical Package for the Social Sciences (SPSS
v16; SPSS, Inc., Chicago, IL, USA)) were used to perform
the statistical analysis of the data.
Reliability
Three healthy control participants were randomly selected,
using the Research Randomizer programme (http://www.resea
rchrandomizer.org), to repeat the sEMG procedure in order to
examine the reproducibility of the results. Due to the small
sample size, differences between the raw data were examined
descriptively, examining mean differences and SD between
the first and second tests. The results for the different muscle
groups were combined for each measure of reliability.
Results
Thirty-two patients met the inclusion criteria: 15 with
dysphagia, of whom nine were recruited to Group 1 (five
declined to take part and one died before his scheduled
appointment); 17 had intact swallow function, of whom six
were recruited to Group 2, and 11 declined to take part.
Twelve healthy participants formed the control group
(Group 3). Group 3 was significantly older than Group 2
(p = 0.03, Table 1). All DMD participants were wheel-
chair users and dependent for all activities of daily living,
including feeding. One participant in Group 2 had a tra-
cheostomy in situ. Group 1 had a significantly lower FOIS
score than both Group 2 and Group 3 participants
(p B 0.001) (Table 1). Two participants in Group 1 had a
percutaneous endoscopic gastrostomy (PEG) tube in situ to
meet their nutrition and hydration needs. Eight participants
in Group 1 were receiving a modified diet (pureed food)
due to dysphagia. The remaining participant in Group 1
was receiving only teaspoons of fluid by mouth and
otherwise was PEG fed. No participants in Group 2 had any
modifications to their diet. No participants in Group 3 had
any history of dysphagia or neurological or gastrointestinal
disease as determined by face-to-face interview.
The sEMG procedure was well tolerated by all partici-
pants and simple to administer, taking less than 10 min to
complete. The technique consistently produced electro-
myographic signals from which objective measurements of
swallowing activity were made. It was not possible to place
a preamplifier in the infrahyoid muscle position in one
participant in Group 1 due to flexed neck posture, and in
the orbicularis oris muscle site on another participant in
Group 1 due to reported skin sensitivity. Therefore, the
results for these muscle groups in Group 1 are based on
eight participants. It was not possible to measure an
infrahyoid muscle MVC in two of the healthy control
participants as activity was not elicited in this muscle group
during the MVC manoeuvre; therefore, the infrahyoid
amplitude measurements for Group 3 are based on ten
participants.
Examination of the sEMG Trace
Representative sEMG swallow waveforms from individu-
als in each group are shown in Fig. 1. All healthy controls
(Group 3) demonstrated clear, easily identifiable, and
measurable peaks of activity during swallowing in each
muscle group, and then activity returned to baseline levels
(Fig. 1a). In contrast, swallow waveforms from participants
in Groups 1 and 2 showed multiple peaks of activity per
swallow (Fig. 1b, c). In addition, activity was prolonged,
and there was evidence of continued activity after the
swallow, without a return to baseline.
Peak Amplitude
Figure 2 and Table 1 show peak-normalised sEMG ampli-
tude during swallowing for each muscle group. Normalised
peak amplitude was significantly higher in Group 1 than in
Group 3 for orbicularis oris and masseter muscles (p = 0.03
and p \ 0.01, respectively, Table 1). Normalised peak
amplitude was also higher for Group 2 than for Group 3 in
these muscle groups, but this did not reach significance. A
similar nonsignificant trend was observed in the infrahyoid
muscle group (p = 0.15). Peak sEMG activity was signifi-
cantly higher in Group 3 than in Group 2 for the submental
muscle group (p = 0.03, Table 1). There were no other
significant between-group differences.
Duration of Activity
There were no differences between the participant groups
with respect to duration of activity and no clear pattern was
observed (Table 1).
S. K. Archer et al.: Dysphagia in Duchenne Muscular Dystrophy Assessed Objectively 191
123

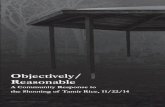
Relative Timing of Activity
The mean order of onset of activity was statistically similar
for all groups: orbicularis oris first, then submental, mas-
seter, and finally infrahyoid (Fig. 3).
Intrasubject Variation
There was significantly higher intrasubject variability in
peak masseter activity in Group 1 than in Group 2
(16.01 % MVC [IQR = 12.82–38.85] vs. 5.86 % MVC
[IQR = 3.58–6.83]; p = 0.02) and in Group 1 than in
Group 3 (16.01 % MVC [IQR = 12.82–38.85] vs. 2.18 %
MVC [IQR = 0.77–6.06]; p =0.02). The difference between
Groups 2 and 3 was not significant. The same trend was
seen for peak amplitude of orbicularis oris and infrahyoid
muscles, with increased variability in the DMD groups and
Group 1 having the most variability, although this did not
reach significance. There were no significant differences
and no trends seen in relative intrasubject variability for
any of the other sEMG measures.
Reliability
The mean differences between the repeated sEMG
assessments were amplitude: 29.12 ± 21.69 % MVC,
duration: 0.69 ± 0.62 s, and relative timing: 0.40 ±
0.24 s.
Discussion
The present study is the first to investigate the clinical
application of sEMG for the assessment of swallowing in
patients with DMD. The technique was well tolerated and
easy to administer, confirming its potential for repeated
objective physiological assessment in patients with pro-
gressive neuromuscular diseases. Of the four muscle
groups tested, there were distinct differences in normalised
peak activity during swallowing between the DMD par-
ticipants with dysphagia, those with preserved muscle
function, and healthy controls. Although there were no
differences in the timing or duration of muscle activity
between the groups, these comparative data provide insight
into the relative activity of orbicularis oris, masseter,
infrahyoid, and submental muscles during swallowing.
Muscle Activation During Swallowing
Dysphagic DMD participants produced greater normalised
peak orbicularis oris and masseter muscle activity during
swallowing, which supports the original study hypothesis.
In healthy subjects, the force produced during swallowing
is only a small percentage of that which can be generated
voluntarily [23]. The dysphagic DMD participants exerted
a relatively higher proportion of maximal activity, i.e., they
were working harder to swallow than the other participant
groups, indicating that they have weaker muscles with less
Table 1 Demographics and
sEMG measurements during
swallowing in the three
participant groups
Data are presented as mean and
[SD] for age and relative timing
of sEMG activity, and as
median and [IQR] for FOIS and
peak and duration of sEMG
activity
* p B 0.05; ** p B 0.01;
*** p B 0.001a Significant difference
between Groups 1 and 2b Significant difference
between Groups 2 and 3c Significant difference
between Groups 1 and 3
Group 1 Group 2 Group 3
(dysphagic DMD
participants)
(nondysphagic
DMD participants)
(healthy controls)
n 9 6 12
Age (years) 21.7 [4.2] 21.0 [3.0]b* 24.8 [3.1]
FOIS 5 [5–5]a*** 7 [7–7] 7 [7–7]c***
Peak sEMG activity (%MVC)
Orbicularis oris 71.87 [49.89–109.82] 58.79 [47.39–66.86] 26.22c* [14.22–52.33]
Masseter 61.77 [25.95–103.50] 19.34 [11.06–36.86] 5.07c** [4.28–13.03]
Submental 25.14 [17.74–86.71] 20.21 [16.09–21.22] 73.46c* [32.68–94.12]
Infrahyoid 80.08 [31.08–91.19] 43.54 [32.94–90.07] 17.71 [9.95–38.22]
Duration of sEMG activity (s)
Orbicularis oris 2.62 [0.55–3.87] 1.89 [1.49–2.25] 1.89 [0.98–2.40]
Masseter 0.29 [0.18–0.54] 0.78 [0.58–1.15] 0.78 [0.55–0.99]
Submental 0.52 [0.36–1.06] 0.95 [0.66–2.31] 1.29 [1.13–1.52]
Infrahyoid 0.45 [0.24–0.76] 0.31 [0.12–0.62] 0.79 [0.70–0.92]
Timing of activity onset relative to submental activity (s)
Orbicularis oris –0.74 [0.85] –0.52 [0.44] –0.71 [0.55]
Masseter 0.09 [0.23] 0.36 [0.53] 0.24 [0.28]
Submental 0 [0] 0 [0] 0 [0]
Infrahyoid 0.16 [0.55] 0.38 [0.47] 0.35 [0.26]
192 S. K. Archer et al.: Dysphagia in Duchenne Muscular Dystrophy Assessed Objectively
123

Fig. 1 Rectified and smoothed sEMG swallow trace by a participant
from each group, with all muscle groups represented. a Healthy
control participant (Group 3). b Dysphagic DMD participant (Group
1). c Nondysphagic DMD participant (Group 2). Dashed line, peak
swallow activity; dotted line, baseline activity ?2 standard deviations
(2 SD). A, onset of swallow activity; B, offset of swallow activity
S. K. Archer et al.: Dysphagia in Duchenne Muscular Dystrophy Assessed Objectively 193
123

functional reserve [23]. This finding is consistent with
previous electromyographic studies of myopathic limb
muscles and is indicative of reduced electromechanical
efficiency, with more motor units activated to give the
same force due to loss of muscle fibres [14]. In contrast, the
submental muscle group followed a different activity pat-
tern, with healthy controls producing a significantly greater
percentage of their MVC during swallowing than nondys-
phagic DMD patients. This could be explained by the
difficulty in performing a MVC of these muscles. By using
a nonswallow task for the MVC (resisted jaw opening),
activation of muscles not normally involved in swallowing
was likely (e.g., platysma) and would have been recorded.
Instructing participants to produce a forceful swallow with
maximum effort may have been a more appropriate tech-
nique to produce the maximum activity of the target
muscles.
Dysphagic DMD participants generally had more vari-
ability in activity between swallows than the other groups
and this was significant in the masseter muscles. It is
suggested that this provides further evidence of muscle
weakness and recruitment of multiple motor units during
swallowing in dysphagic DMD patients. The present study
required participants to swallow six successive teaspoons
of water, which arguably is not a demanding task;
therefore, a further study should be conducted in which
participants swallow larger amounts and/or different tex-
tured boluses which might put greater demands on the
swallowing system, potentially leading to increased dif-
ferences between these groups.
Timing of Activation
The results of the present study indicate that DMD does not
consistently affect timing of muscle activation during
swallowing, which is contrary to the results of Crary et al.
[19] who found significantly shorter activity duration in
sEMG assessments of dysphagic stroke patients, and which
suggests that different disease processes exert different
effects on swallowing, as might be expected. A reduction
in duration of activity was predicted a priori in the dys-
phagic patients as a sign of myopathic changes, reflecting a
shortening in motor unit action potentials from a loss of
fibres [16]. However, this was not found, which may reflect
the recorded sEMG signal being a superimposition of all
active motor units during muscle contraction and therefore
not being sensitive to changes in individual motor units.
There was a consistent pattern of onset of muscle group
activity during swallowing in the present study, which was
preserved in DMD participants with dysphagia. The same
Fig. 1 continued
194 S. K. Archer et al.: Dysphagia in Duchenne Muscular Dystrophy Assessed Objectively
123

sequence of activity in swallowing has been reported pre-
viously [24] and can be related to the order of biomechanical
events in the swallow. The orbicularis oris muscles are
activated first, corresponding to the oral phase of the swal-
low, where the lips are closed to contain the bolus in the oral
cavity [25]. The submental group then elevates the larynx
and may have a role in propulsion of the bolus into the
pharynx [9]. The masseter muscle then activates and stabi-
lises the jaw in the intercuspal position for the onset of
swallowing [26], assisting in the development and mainte-
nance of intraoral pressure to facilitate bolus propulsion.
Finally, the infrahyoid muscles pull the hyoid and attached
larynx downward [27]. The return of the hyoid to the resting
position is a marker of the end of the oropharyngeal swallow
[28]. For all patients and healthy participants, there was an
overlap in the activity for all muscle groups, consistent with
the dynamic nature and overlap of the oral and pharyngeal
components of swallowing.
Examination of the sEMG Trace
All DMD participants, regardless of swallowing status,
produced different patterns on the sEMG trace during
swallowing compared to healthy participants, who pro-
duced clear, easily identifiable single peaks in all muscle
groups as previously reported for healthy subjects [8].
DMD participants had more variable patterns with
numerous and less distinct sEMG peaks, which has also
previously been reported in dysphagic stroke patients [19].
Polyphasic waves on EMG have been reported as a feature
of myopathy, related to loss of muscle fibres within the
motor unit, with recruitment of a greater number of motor
units to compensate for weakness [15]. The baseline sEMG
activity was greater in the DMD participants as also
reported in stroke patients [19]. In DMD, spontaneous
activity, with multiple peaks, complex repetitive dis-
charges, and fibrillation potentials, is well reported in EMG
studies of limb muscles [29] but has not been previously
described in the swallowing muscles.
Despite the marked differences between patients and
healthy controls, there were no consistent pattern differ-
ences in the sEMG trace between the DMD participants
with dysphagia and those with preserved swallow function.
While the nondysphagic patients were not showing clinical
signs of swallowing impairment, the sEMG findings indi-
cate that there were physiological changes to their swal-
lowing muscles. This is consistent with previous data from
oligosymptomatic patients with DMD who showed myo-
pathic changes on needle EMG studies of limb muscles
[15]. This finding may be indicative of the continuum of
disease, which is a particular consideration with recruit-
ment of participants at the more severe end of the disease
spectrum in the present study (from an adult respiratory
clinic). Crary et al. [8] found that observers could reliably
and accurately identify normal swallows from nonswallow
activity in sEMG traces. However, it remains to be deter-
mined whether it is possible to discriminate between nor-
mal and abnormal swallows from their sEMG trace with a
similar level of accuracy.
Reliability
The descriptive test–retest assessment in the present study
was based on a very small sample of healthy partici-
pants and the reproducibility in the patient population
remains unknown. Nonetheless, the mean differences in
Fig. 2 Peak sEMG amplitude
during swallowing for each
muscle group across participant
groups. Group 1, dysphagic
DMD participants; Group 2,
nondysphagic DMD
participants; Group 3, healthy
controls. Medians and
interquartile ranges are
presented, compared with the
Mann-Whitney U test and
corrected for multiple testing
with the Bonferroni Correction.
*p \ 0.05; **p \ 0.01
S. K. Archer et al.: Dysphagia in Duchenne Muscular Dystrophy Assessed Objectively 195
123
measurements across the repeated sEMG assessments in
the present study highlight the need to examine further the
reliability of sEMG before it is used in clinical assessment.
The sEMG signal can be influenced by many factors, which
may be physiological, experimental, or technical and are
likely to affect reproducibility [30]. These influences may
be particularly difficult to control for when using sEMG to
assess muscle activity in swallowing, which is a highly
complex, adaptive motor activity [21]. However, some
authors are already using sEMG to assess swallow function
[10, 31] before arguably necessary research has been
completed.
Critique of the Method
A limitation of this study was the small sample size and the
considerable refusal rate, although no differences were
noted from the medical notes between those who declined
to take part and those who participated, and the patients
were recruited from a tertiary referral centre, enabling
relatively good access to a rare patient population. This
study was necessarily exploratory as no similar work has
been conducted previously, and we believe that this
detailed physiological pilot study has provided the data and
justification to power a larger clinical study to determine
the role of sEMG as a simple, objective, physiological
biomarker for dysphagia. In addition, we appreciate that
the method of classification of DMD participants into
dysphagic and nondysphagic groups could be questioned as
it was based on a diagnosis of dysphagia made by a speech
and language therapist or on a statement of normal swal-
lowing made by a physician, rather than on an instrumental
swallowing assessment. However, all of the patients were
recruited from a specialist centre, with one Specialist SLT
and two experienced consultants in the established team,
all of whom were experienced in assessing swallow func-
tion, and a validated scale (the FOIS) was used to classify
impairment. The healthy control group was older than the
nondysphagic DMD participants, but the difference was
small and there is no reported change in swallowing
function in the healthy population until advanced age [20].
Differences in muscle activity during swallowing
between the groups could be influenced by differences in
intentional effort, i.e., dysphagic patients may have been
actively trying to swallow ‘‘better.’’ However, to control
for this, all participants were given the same instructions
which were aimed to encourage their normal swallowing
behaviour. It is therefore felt that the increase in activity in
the dysphagic patient group is more likely to reflect muscle
weakness. A limitation of sEMG is that all muscles
involved in swallowing cannot be examined, and sEMG
cannot be used to specifically measure lingual strength,
which is important in bolus propulsion [32]. However,
activity of the lingual muscle has been shown to contribute
significantly to the collective signal measured from the
submental region, which was recorded [33], and a strength
of this study was the examination of four different oral and
pharyngeal muscle groups that all contribute to swallow-
ing. Furthermore, the ability of sEMG to detect a repre-
sentative, composite signal of the activity of the underlying
muscle group [30] means it arguably lends itself to the
assessment of swallowing, which incorporates activation of
many muscles.
An accepted method was used for determining onset and
offset of activity, in which baseline ? 2 standard devia-
tions was considered the threshold [19, 21]. However, with
the multiple peaks and activity after the swallow observed
in the patient groups, this method became less reliable.
Fig. 3 Timing of onset of
muscle group activity relative to
submental activity during the
swallow. The three participant
groups are shown. Group 1,
dysphagic DMD participants;
Group 2, nondysphagic DMD
participants; Group 3, healthy
controls. The symbols represent
means and the lines represent
95 % confidence intervals
196 S. K. Archer et al.: Dysphagia in Duchenne Muscular Dystrophy Assessed Objectively
123

While a consistent method for peak identification was used,
it increased the subjective element of the analysis. Further
studies examining the sEMG trace with simultaneous direct
visualisation of the swallow with either FEES or video-
fluoroscopy would enable identification of sEMG mea-
surements that are most clinically meaningful.
Conclusion
This is the first investigation of the clinical usefulness of
sEMG for the assessment of swallowing function in
patients with DMD. The technique was well tolerated and
quick to administer, enabling easy and objective recording
of data. Compared to controls, dysphagic DMD patients
produced a greater proportion of their maximum voluntary
muscle activity when swallowing, indicating muscle
weakness. Furthermore, characteristic differences were
present in the pattern of activity during swallowing
between DMD patients and healthy controls, indicative of
myopathic changes in the muscle groups tested. However,
distinct differences between DMD patients with dysphagia
and those DMD patients with intact swallow function were
not found, indicating that there are subclinical physiolog-
ical changes to the muscles for swallowing in DMD, which
is consistent with previous studies of limb muscles. While
this finding limits the value of the sEMG technique for
diagnosing dysphagia in DMD, this study has shown that
sEMG provides useful physiological information about
changes to swallowing muscles in DMD, justifying further
study.
Acknowledgments This work was performed as part of a MRes in
Biomedical Sciences at St George’s, University of London. The
authors acknowledge with gratitude the help given by Mr. David
Crick at Cambridge Electronic Design (Cambridge) who wrote the
script ‘‘Swallow EMG’’ for the Spike 2 data analysis programme. The
authors acknowledge the help given by Prof. Di Newham from King’s
College London in reviewing the manuscript. The authors acknowl-
edge financial support from the Department of Health via the National
Institute for Health Research (NIHR) comprehensive Biomedical
Research Centre award to Guy’s & St Thomas’ NHS Foundation
Trust in partnership with King’s College London and King’s College
Hospital NHS Foundation Trust.
Conflict of Interest The authors report no conflicts of interest
concerning the materials or methods used in this study or the findings
reported in this paper.
References
1. Manzur AY, Muntoni F. Diagnosis and new treatments in mus-
cular dystrophies. J Neurol Neurosurg Psychiatry. 2009;80(7):
706–14.
2. Hill M, Hughes T, Milford C. Treatment for swallowing diffi-
culties (dysphagia) in chronic muscle disease. Cochrane Database
Syst Rev. 2004;2:CD004303.
3. Shinonaga C, Fukuda M, Suzuki Y, Higaki T, Ishida Y, Ishii E,
Hyodo M, Morimoto T, Sano N. Evaluation of swallowing
function in Duchenne muscular dystrophy. Dev Med Child
Neurol. 2008;50(6):478–80.
4. Nozaki S, Umaki Y, Sugishita S, Tatara K, Adachi K, Shinno S.
Videofluorographic assessment of swallowing function in patients
with Duchenne muscular dystrophy. Clin Neurol. 2007;47(7):407–12.
5. Hanayama K, Liu M, Higuchi Y, Fujiwara T, Tsuji T, Hase K,
Ishihara T. Dysphagia in patients with Duchenne muscular dys-
trophy evaluated with a questionnaire and videofluorography.
Disabil Rehabil. 2008;30(7):517–22.
6. Aloysius A, Born P, Kinali M, Davis T, Pane M, Mercuri E.
Swallowing difficulties in Duchenne muscular dystrophy: Indi-
cations for feeding assessment and outcome of videofluoroscopic
swallow studies. Dysphagia. 2009;24(1):123–4.
7. Crary MA, Carnaby GD, Groher ME. Biomechanical correlates
of surface electromyography signals obtained during swallowing
by healthy adults. J Speech Lang Hear Res. 2006;49(1):186–93.
8. Crary MA, Carnaby GD, Groher ME. Identification of swallow-
ing events from sEMG signals obtained from healthy adults.
Dysphagia. 2007;22(2):94–9.
9. Palmer PM, Luschei ES, Jaffe D, McCulloch TM. Contributions
of individual muscles to the submental surface electromyogram
during swallowing. J Speech Lang Hear Res. 1999;42(6):
1378–91.
10. Vaiman M. Standardization of surface electromyography utilized
to evaluate patients with dysphagia. Head Face Med. 2007;3:26.
11. Vaiman M, Eviatar E, Segal S. Surface electromyographic studies
of swallowing in normal subjects: A review of 440 adults. Report
3. Qualitative data. Otolaryngol Head Neck Surg. 2004;131(6):
977–85.
12. O’Kane L, Groher ME, Silva K, Osborn L. Normal muscular
activity during swallowing as measured by surface electromy-
ography. Ann Otol Rhinol Laryngol. 2010;119(6):398–401.
13. Armijo-Olivo S, Gadotti I, Kornerup M, Lagravere MO, Flores-
Mir C. Quality of reporting masticatory muscle electromyogra-
phy in 2004: a systematic review. J Oral Rehabil. 2007;34(6):
397–405.
14. Liguori R, Fuglsang-Frederiksen A, Nix W, Fawcett P, Andersen
K. Electromyography in myopathy. Clin Neurophysiol. 1997;
27:200–3.
15. Emeryk-Szajewska B, Kopec J. Electromyographic pattern in
Duchenne and Becker muscular dystrophy. Part I. Electromyo-
graphic pattern in subsequent stages of muscle lesion in Duchenne
muscular dystrophy. Electromyogr Clin Neurophysiol. 2008;
48:265–77.
16. Fuglsang-Frederiksen A. The role of different EMG methods in
evaluating myopathy. Clin Neurophysiol. 2006;117:1173–89.
17. Crary MA, Carnaby MGD, Groher ME. Initial psychometric
assessment of a functional oral intake scale for dysphagia in
stroke patients. Arch Phys Med Rehabil. 2005;86(8):1516–20.
18. Johnson SW, Lynn PA, Miller JSG, Reed GA. Miniature skin-
mounted preamplifier for measurement of surface electromyo-
graphic potentials. Med Biol Eng Comput. 1997;15:710–1.
19. Crary MA, Baldwin BO. Surface electromyographic character-
istics of swallowing in dysphagia secondary to brainstem stroke.
Dysphagia. 1997;12(4):180–7.
20. O’Dwyer NJ. Control of speech muscles in normal and cerebral-
palsied speakers: an electromyographic analysis. Kensington:
University of New South Wales; 1988.
21. Ding R, Larson CR, Logemann JA, Rademaker AW. Surface
electromyographic and electroglottographic studies in normal
S. K. Archer et al.: Dysphagia in Duchenne Muscular Dystrophy Assessed Objectively 197
123

subjects under two swallow conditions: normal and during the
Mendelsohn manuever. Dysphagia. 2002;17(1):1–12.
22. Bland JM, Altman DG. Multiple significance tests: the Bonfer-
roni method. BMJ. 1995;310:170.
23. Burkhead LM, Sapienza CM, Rosenbek JC. Strength-training
exercise in dysphagia rehabilitation: principles, procedures, and
directions for future research. Dysphagia. 2007;22:251–65.
24. Ono T, Iwata H, Hori K, Tamine K, Kondoh J, Hamanaka S,
Maeda Y. Evaluation of tongue-, jaw-, and swallowing-related
muscle coordination during voluntarily triggered swallowing. Int
J Prosthodont. 2009;22(5):493–8.
25. Logemann JA. Swallowing disorders. Baillieres Best Pract Res
Clin Gastroenterol. 2007;21:563–73.
26. Monaco A, Cattaneo R, Spadaro A, Giannoni M. Surface elec-
tromyography pattern of human swallowing. BMC Oral Health.
2008;8:6.
27. Humbert IA, Poletto CJ, Saxon KG, Kearney PR, Crujido L,
Wright-Harp W, Payne J, Jeffries N, Sonies BC, Ludlow CL. The
effect of surface electrical stimulation on hyolaryngeal movement
in normal individuals at rest and during swallowing. J Appl
Physiol. 2006;101:1657–63.
28. Martin-Harris B, Michel Y, Castell DO. Physiologic model of
oropharyngeal swallowing revisited. Otolaryngol Head Neck
Surg. 2005;133:234–40.
29. Eeg-Olofsson KE. Dystrophinopathies. In: Stalberg E, editor.
Clinical neurophysiology of disorders of muscle and neuromus-
cular junction. Amsterdam: Elsevier; 2003. p. 429–41.
30. Hogrel JY. Clinical applications of surface electromyography
in neuromuscular disorders. Neurophysiol Clin. 2005;35(2–3):
59–71.
31. Vaiman M. Surface electromyography in preoperative evaluation
and postoperative monitoring of Zenker’s diverticulum. Dys-
phagia. 2006;21(1):14–20.
32. Kennedy D, Kieser J, Bolter C, Swain M, Singh B, Waddell JN.
Tongue pressure patterns during water swallowing. Dysphagia.
2010;25:11–9.
33. Huckabee ML, Steele CM. An analysis of lingual contribution to
submental surface electromyographic measures and pharyngeal
pressure during effortful swallow. Arch Phys Med Rehabil.
2006;87(8):1067–72.
Sally K. Archer MRes, BMedSci (Hons), MRCSLT
Rachel Garrod PhD, MSC, MCSP
Nicholas Hart MBBS, BSc, MRCP, PhD
Simon Miller PhD
198 S. K. Archer et al.: Dysphagia in Duchenne Muscular Dystrophy Assessed Objectively
123