DYSPHAGIA
47
DYSPHAGIA
-
Upload
nur-khairah-amalina -
Category
Documents
-
view
7 -
download
0
description
dysphagia ppt
Transcript of DYSPHAGIA

DYSPHAGIA
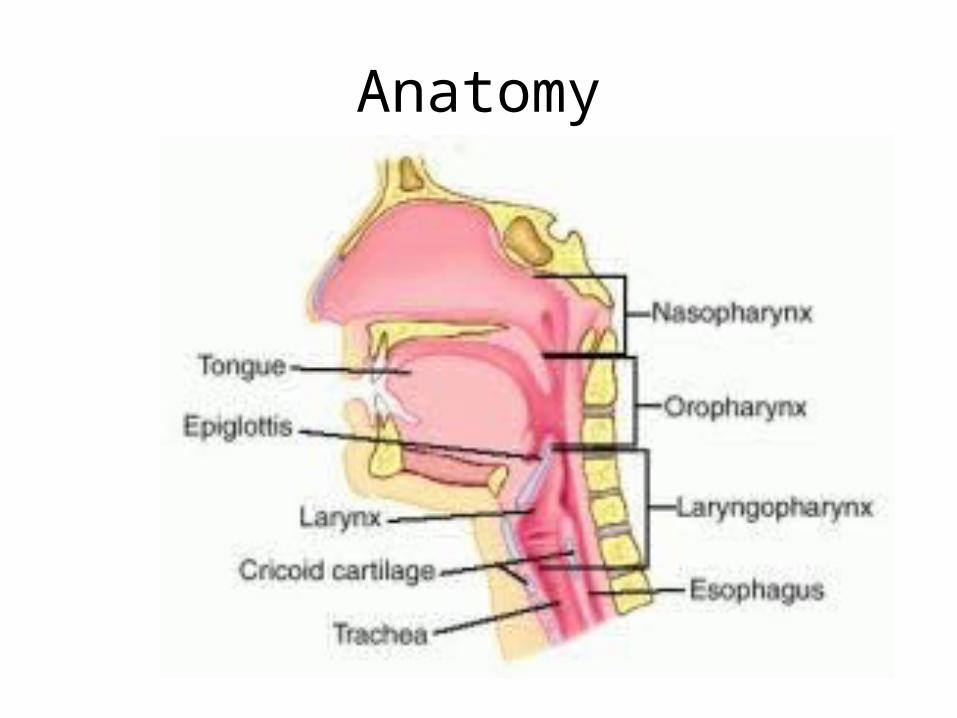
Anatomy
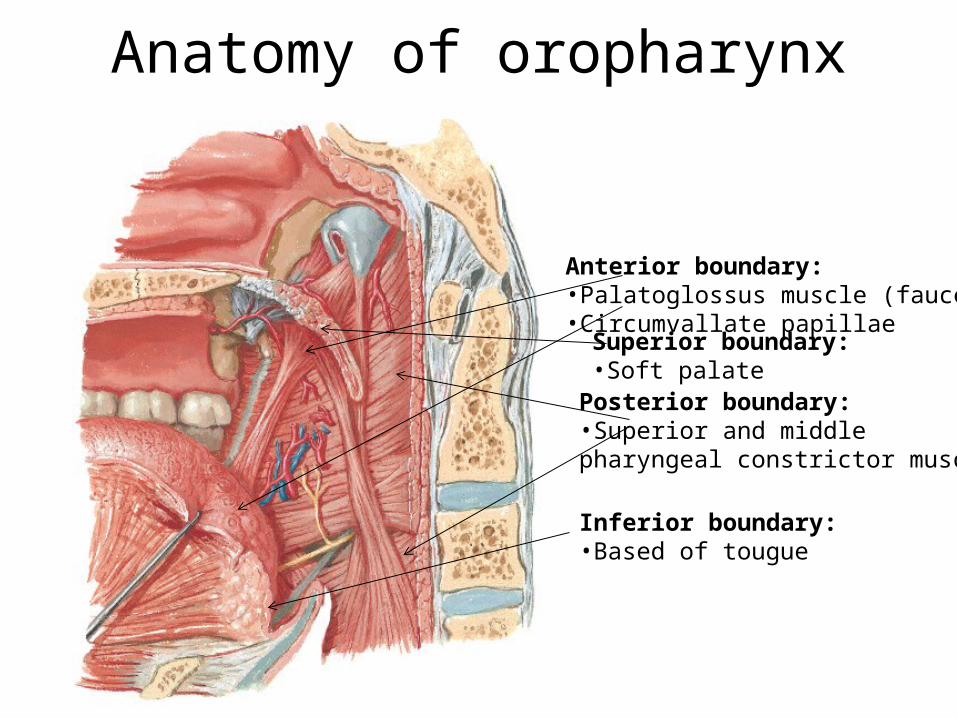
Anatomy of oropharynx
Posterior boundary:•Superior and middle pharyngeal constrictor muscle
Anterior boundary:•Palatoglossus muscle (fauces)•Circumvallate papillae
Inferior boundary:•Based of tougue
Superior boundary:•Soft palate
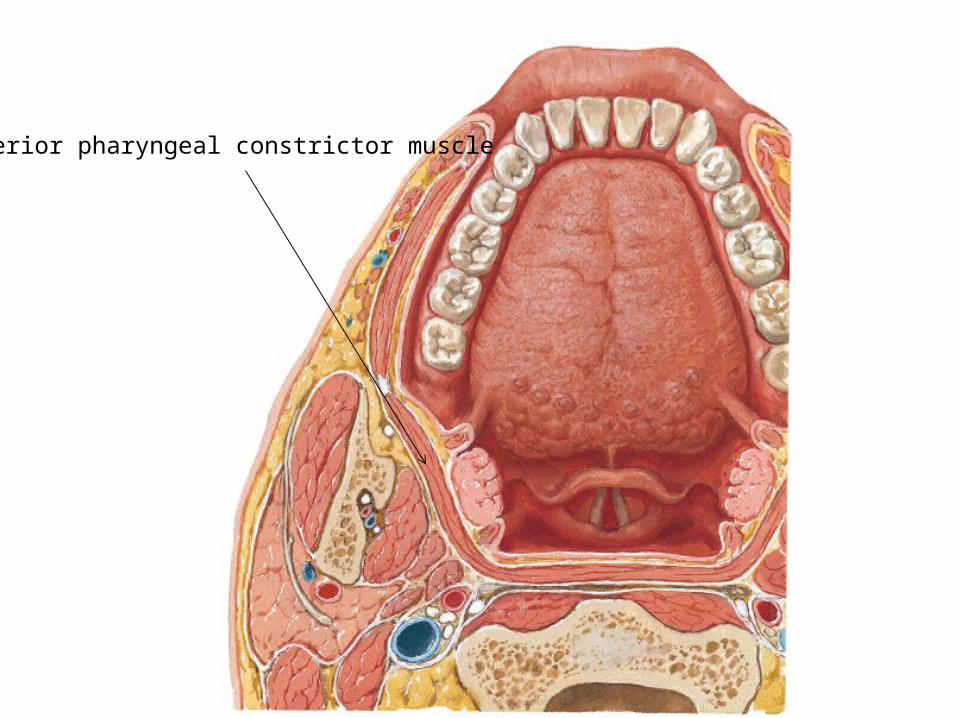
Superior pharyngeal constrictor muscle
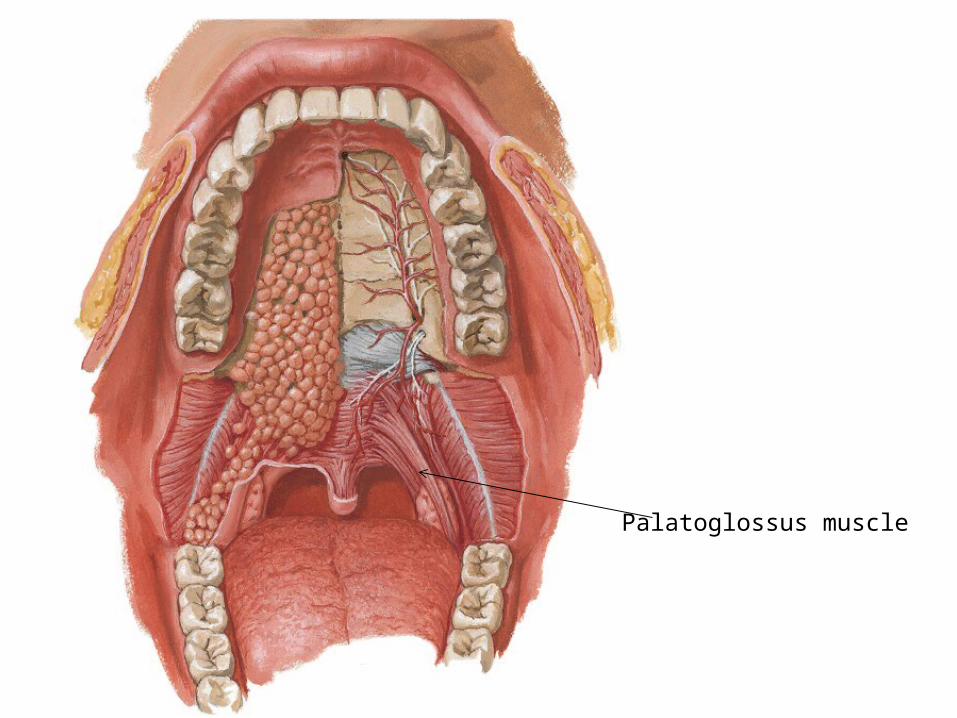
Palatoglossus muscle

Anatomy of hypopharynx
Piriform recess
Posterior pharyngeal wallOropharynx
Hypopharynx

Anatomy of oropharynx
• Neural control is motor nuclei of CN V, VII, IX, X and XII
• Structures involved: a) Lipsb) Dentition and muscle of masticationsc) Tongued) Palatee) Salivary glandsf) Pharyngeal muscles

Mechanism of Swallowing
4 phases:1) Oral preparatory2) Oral3) Pharyngeal 4) Esophageal
- Involves lips, tongue, mandible, dentition, soft palate, muscles of the buccal cavity
- Grind and position the food- Transfer phase- tongue arranges the bolus, move it
posteriorly to chew- Reduction phase- food is chewed, ground and mixed
with saliva to form bolus.
Oral Preparatory Phase
- Food bolus is transported via the action of the
tongue, palate and teeth- Bolus is positioned posteriorly on the tongue- Lips and buccal muscles contract to built pressure
and reduce the volume of the oral cavity- Posterior tongue depressed, middle and anterior
tongue elevate, propulsion of bolus into the oropharynx
Oral Phase

- Involuntary phase- Bolus reaches the anterior tonsillar pillars- Initiates automatic pharyngeal muscle contraction
• Soft palate pulled upward to seal nasopharynx• Larynx pulled upward and anteriorly• Epiglottis swing backward over the laryngeal inlet• Relaxation of the upper esophageal sphincter
Pharyngeal Phase

- Peristalsis or sequential contraction of the esophagus and relaxation of the lower sphincter
- Propels food into stomach
Esophageal Phase
Dysphagia is difficulty in swallowing, which may be associated with ingestion of solids or liquids or both.
DEFINITION

AETIOLOGY1) Pre-esophageal a) Oral phase b) Pharyngeal phase
2) Esophageal a) Lumen b) Wall c) Outside the wall
Pre-esophageal (Oral phase)1) Disturbance in
mastication-Trismus, fracture of mandible,
TMJ problem
2) Disturbance in lubrication -Xerostomia
3) Disturbance in mobility of tongue
-Painful ulcer, tongue tumors, tongue paralysis
4) Defects of palate-Cleft palate, oronasal fistula
5) Lesions of buccal cavity and floor of mouth
-Ulcerative lesion, Ludwig’s angina

Xerostomia
• Dry mouth due to lack of saliva
• Difficulty in eating, speaking, halitosis and caries
• Causes: Diabetes, Parkinson's disease and Sjogren's syndrome, radiotherapy, medications
Sjögren's syndrome /Mikulicz disease -systemic autoimmune disease in which immune cells attack and destroy the exocrine glands that produce tears and saliva
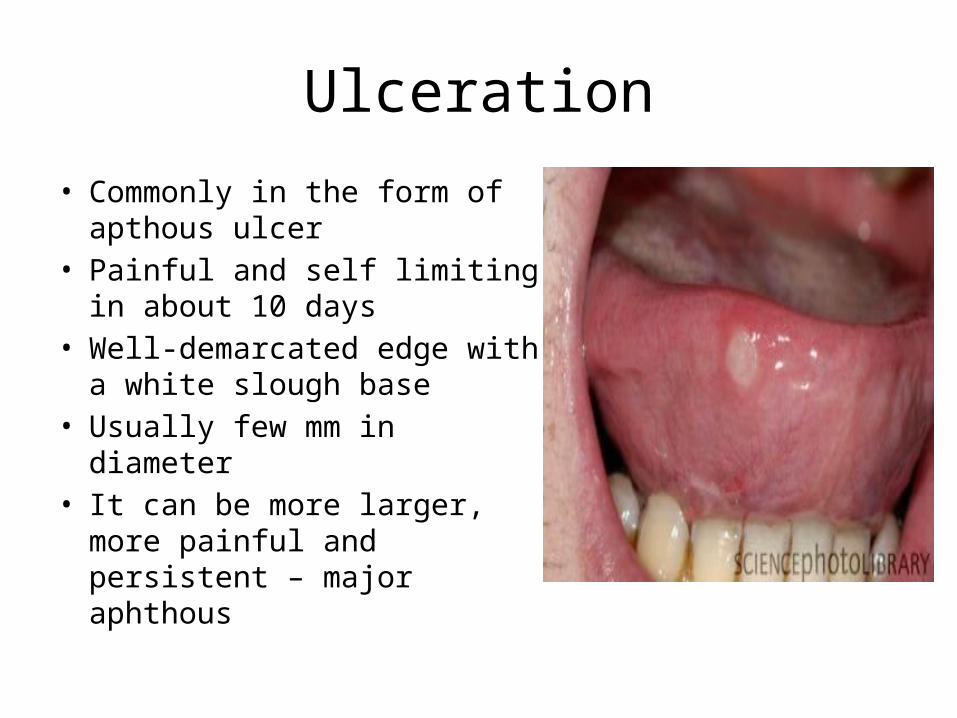
Ulceration
• Commonly in the form of apthous ulcer
• Painful and self limiting in about 10 days
• Well-demarcated edge with a white slough base
• Usually few mm in diameter• It can be more larger, more
painful and persistent – major aphthous
Ludwigs angina
• Cellulitis, usually of odontogenic origin
• Causes : mostly Streptococcal bacteria
• Bilaterally involving the submaxillary, sublingual, and submental spaces
• Painful swelling floor of the mouth, elevation of the tongue, dysphonia, dysphagia, malaise, fever, stridor or difficulty in breathing.
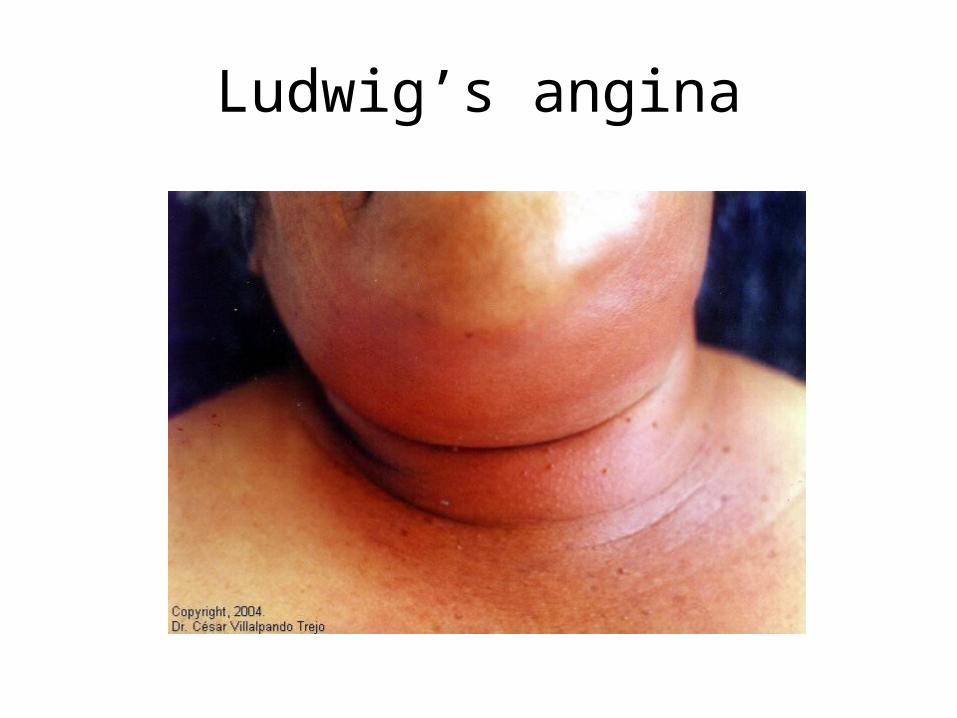
Ludwig’s angina
1) Obstructive lesions of pharynx- Tumours of tonsil, soft palate, pharynx, base of tongue,
supraglottic larynx
2) Inflammatory conditions-acute tonsillitis, acute epiglottitis, retro or para-
pharyngeal abscess
3) Spasmodic conditions-tetanus, rabies
4) Paralytic condition-paralysis of soft palate due to diphteria, bulbar palsy
Pre-esophageal (Pharyngeal phase))
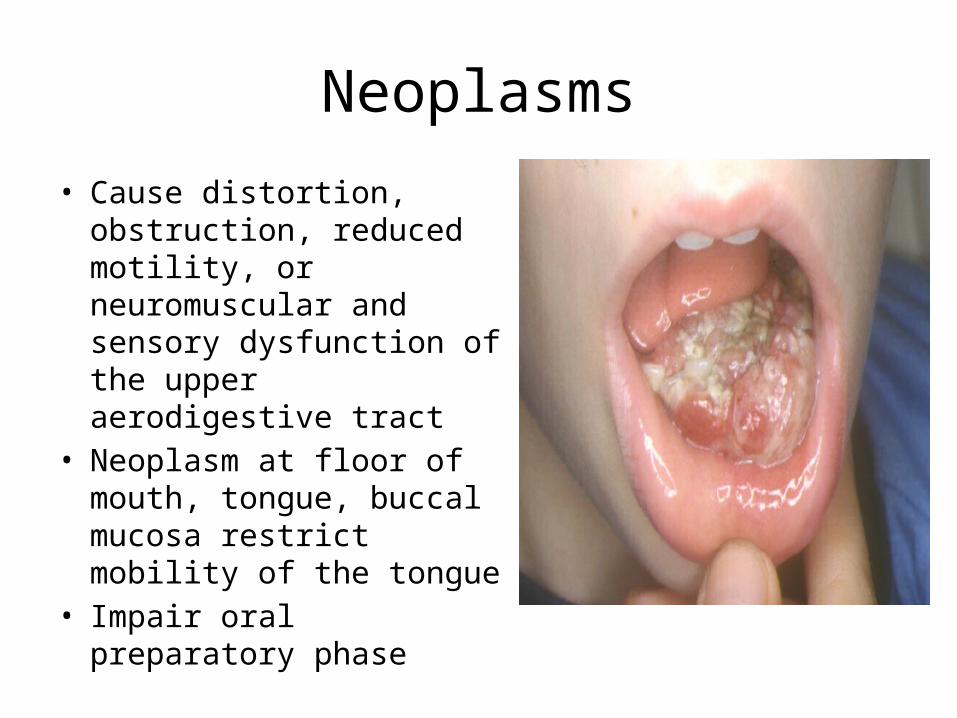
Neoplasms
• Cause distortion, obstruction, reduced motility, or neuromuscular and sensory dysfunction of the upper aerodigestive tract
• Neoplasm at floor of mouth, tongue, buccal mucosa restrict mobility of the tongue
• Impair oral preparatory phase
• Tumor of pharynx interfere with peristalsis/ laryngeal elevation and cause mechanical obstruction
• Invade or destroy larynx- incompetent laryngeal sphincter or sensory denervation- aspiration
Neoplasms
MANAGEMENT
HISTORYPHYSICAL EXAMINATION
INVESTIGATIONTREATMENT
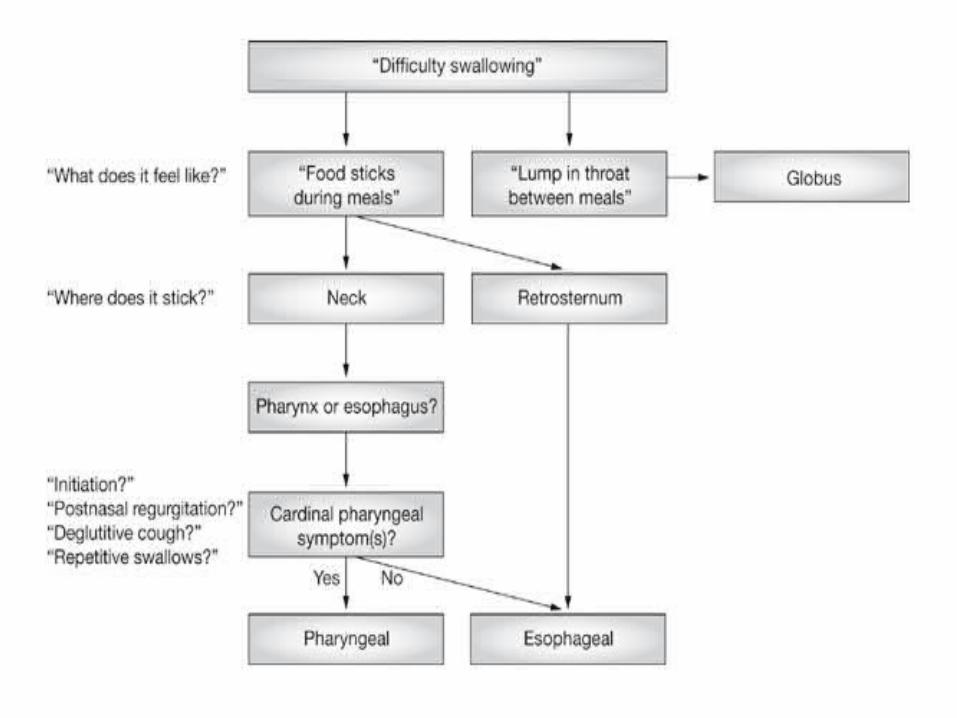
HISTORY
• Detailed history is very important to know :
The anatomic site of problem oesophageal/oropharyngeal
The causes structural/motility
History• Sudden onset– Foreign bodies– Impaction of food on a preexisting stricture or
malignancy– Neurological disorder
• Progressive– Malignancy
• Intermittent– Spasm or spasmodic episodes over an organic lesion
• More to liquids– Paralytic lesion

• More to solid and even progressing even to liquids– Malignancy or stricture
• Intolerance to acid food or fruit juices– Ulcerative lesion
• Associated symptoms - regurgitation and heart burn (hiatus hernia,GORD) - aspiration into lungs (laryngeal paralysis) - aspiration into the nose (palatal paralysis) -any changes in the voice/ dysarthria (restricted tongue
movement)

Predictive symptoms of oropharyngeal dysfunction
• Four symptoms that have high specificity for oropharyngeal dysfunction:
1)delayed or absent oropharyngeal swallow initiation; 2)deglutitive postnasal regurgitation or regress of fluid through the nose
during swallowing3)deglutitive cough indicative of aspiration 4)the need to swallow repetitively to achieve satisfactory clearance of
swallowed material from the hypopharynx.
• If one or more of these four symptoms are present then the cause of dysphagia is probably oropharyngeal, either structural or neuromyogenic
PHYSICAL EXAMINATION
• Full ENT examination is mandatory but special attention is directed to the– Oral cavity– Pharynx– Larynx
• Palpation of any local lesion and the neck is essential
INVESTIGATION
• FBC-anaemia may represent a dietary deficiency secondary to the dysphagia
• Radiography – chest X-ray, barium swallow study, lateral view neck
• Manometry• Oesophageal pH monitoring• Oesophago-gastro-duodenoscopy (OGD)• Fibreoptic Endoscopic Evaluation of Swallowing (FEES).• Others – bronchoscopy, cardiac catetherisation and
thyroid scan
Chest X-ray• To exclude cardiovascular disease,
pulmonary disease and mediastinal disease
Lateral view neck• To exclude cervical osteophytes and any
soft tissue lesion of post-cricoid/retropharyngeal space
Barium swallow study
• Gold standard• Outlines the hypopharynx, oesophagus and
stomach• Suspected obstructive lesion and oesophageal
motility disorder

• Zenker Diverticulum or Pharyngoesophageal Diverticulum
• It is a outpouching of the mucosa of the posterior pharyngeal wall through Killian's triangle(also known as Laimer's triangle, and the Killian-Laimer triangle)an area of weakness between the two parts of the inferior pharyngeal constrictor - the thyropharyngeus and the cricopharyngeus - at their posterior margin
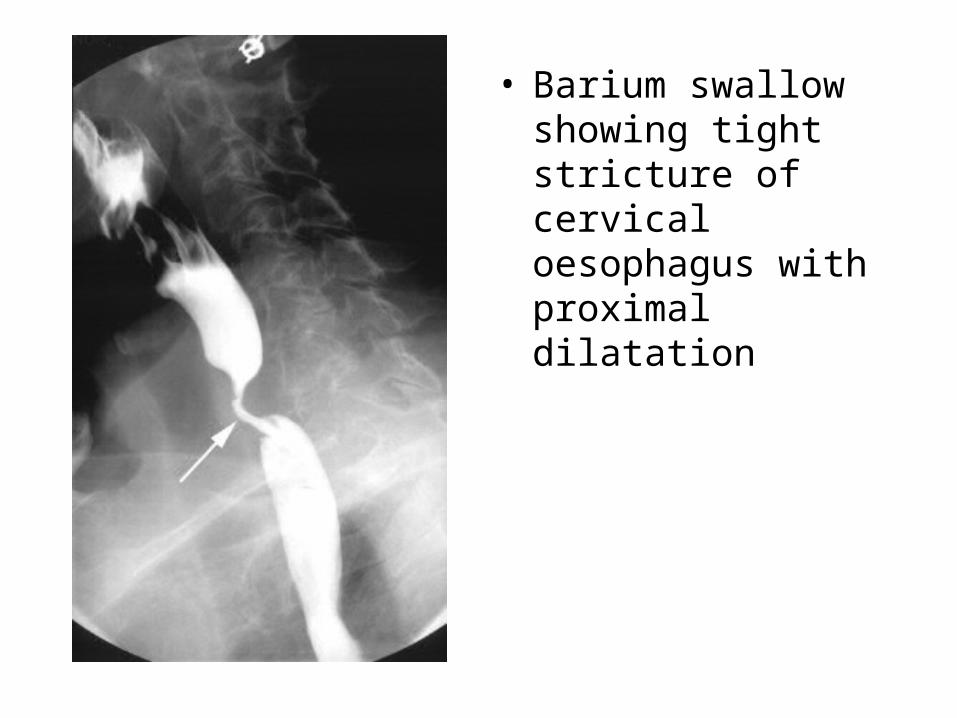
• Barium swallow showing tight stricture of cervical oesophagus with proximal dilatation

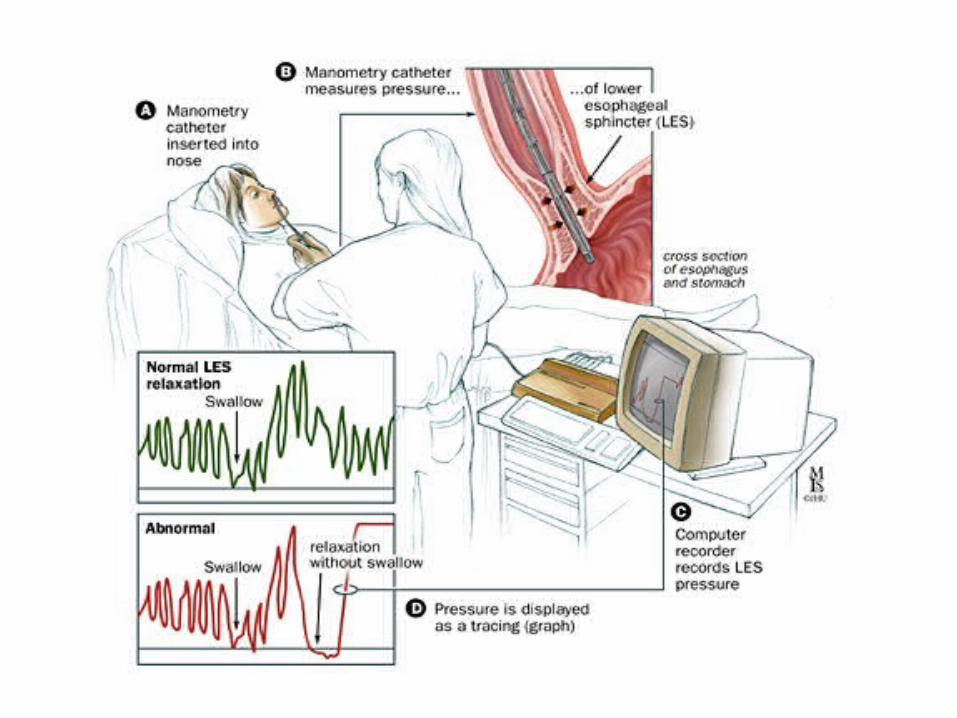
Oesophageal Manometry
• Measures the motility and function of the oesophagus and oesophageal sphincter
• A tube is usually inserted through the nose and passed into the oesophagus
• The pressure of the sphincter muscle is recorded and the contraction waves of swallowing are recorded
Oesophageal pH monitoring• Measures how often and how long stomach acid is entering the
oesophagus• A small thin tube is introduced through the nose mouth and into
the stomach, which is then drawn back up into the esophagus• The tube is attached to a monitor which records the level of
acidity in the esophagus• The patient records symptoms and activity while the tube is left
in place for the next 24 hours• The information from the monitor is compared to the diary the
patient provides• This test is helpful in determining the amount of stomach acid
entering the esophagus

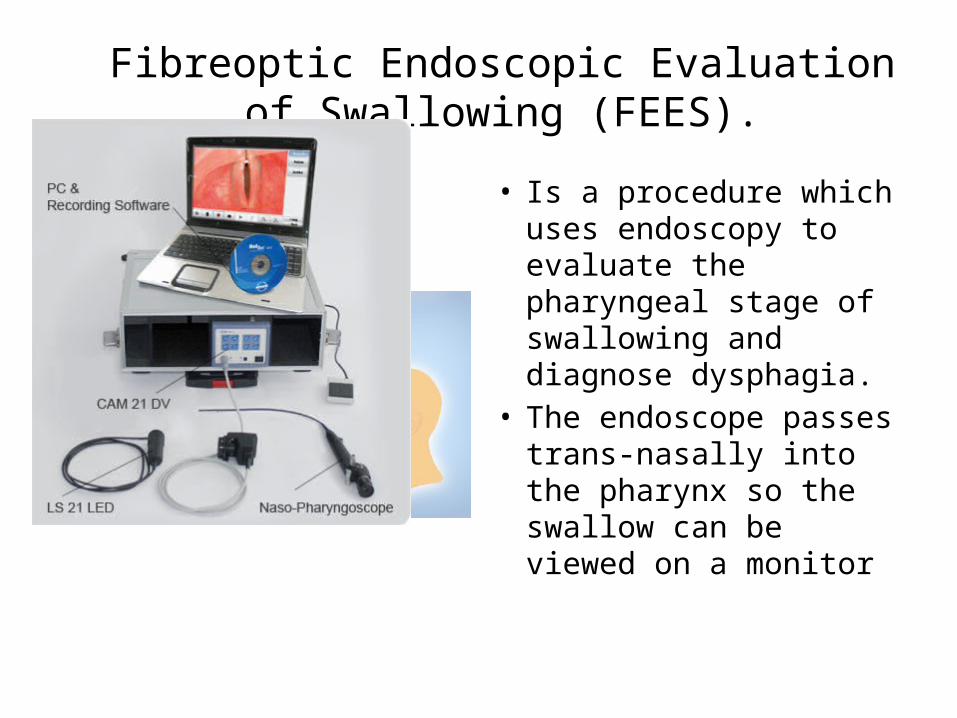
Fibreoptic Endoscopic Evaluation of Swallowing (FEES).
• Is a procedure which uses endoscopy to evaluate the pharyngeal stage of swallowing and diagnose dysphagia.
• The endoscope passes trans-nasally into the pharynx so the swallow can be viewed on a monitor

Other investigations
• Rigid upper GI endoscopy • Bronchoscopy– For bronchial carcinoma
• Cardiac catetherisation– For vascular anomalies
• Thyroid scan– For malignant thyroid
TREATMENT
• Non surgical • Surgical
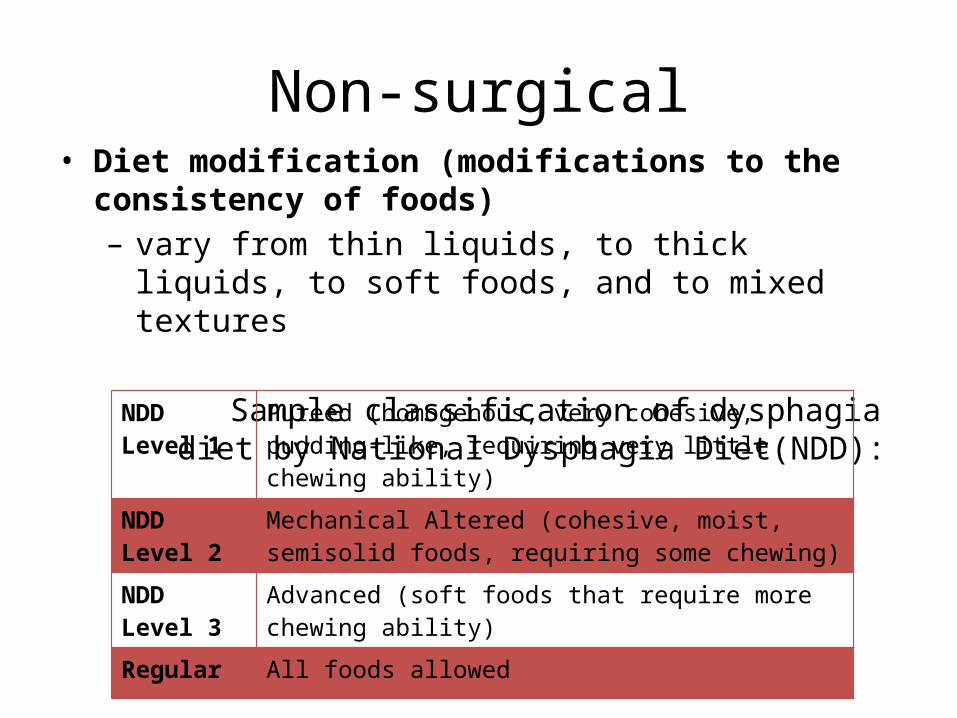
Non-surgical• Diet modification (modifications to the consistency of foods)– vary from thin liquids, to thick liquids, to soft foods, and to
mixed textures
Sample classification of dysphagia diet by National Dysphagia Diet(NDD):
NDD Level 1 Pureed (homogenous, very cohesive, pudding-like, requiring very little chewing ability)
NDD Level 2 Mechanical Altered (cohesive, moist, semisolid foods, requiring some chewing)
NDD Level 3 Advanced (soft foods that require more chewing ability)
Regular All foods allowed
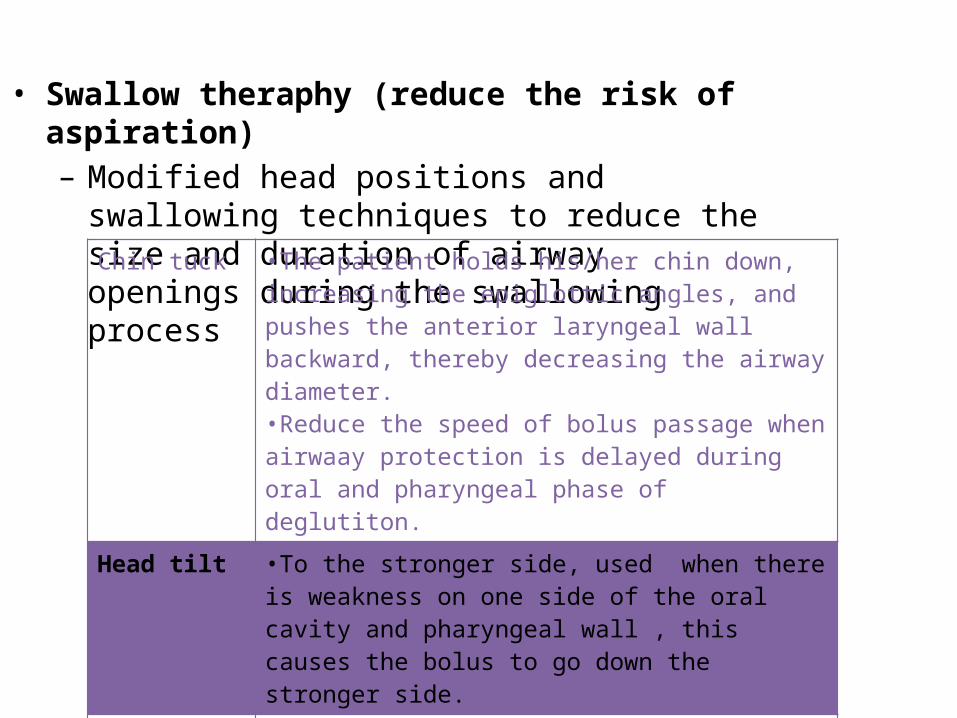
• Swallow theraphy (reduce the risk of aspiration)– Modified head positions and swallowing techniques
to reduce the size and duration of airway openings during the swallowing process
Chin tuck •The patient holds his/her chin down, increasing the epiglottic angles, and pushes the anterior laryngeal wall backward, thereby decreasing the airway diameter.•Reduce the speed of bolus passage when airwaay protection is delayed during oral and pharyngeal phase of deglutiton.
Head tilt •To the stronger side, used when there is weakness on one side of the oral cavity and pharyngeal wall , this causes the bolus to go down the stronger side.
Head rotation •To the damaged or weaker side , used when there is paralysis or paresis on one side of the pharyngeal wall; this causes the bolus to go down the stronger side.
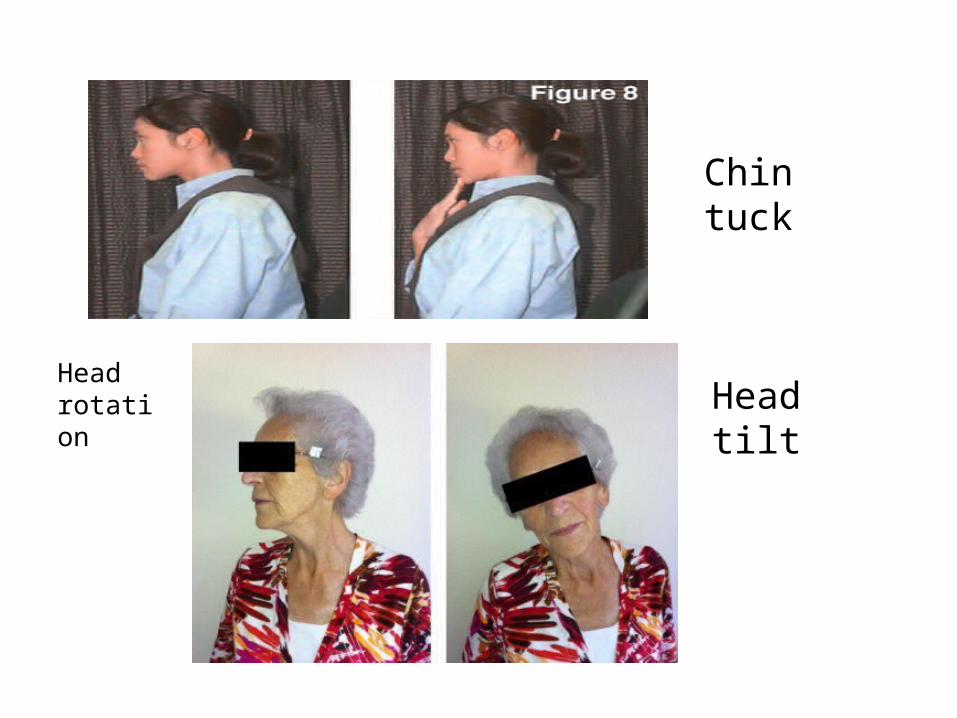
Chin tuck
Head rotation Head tilt
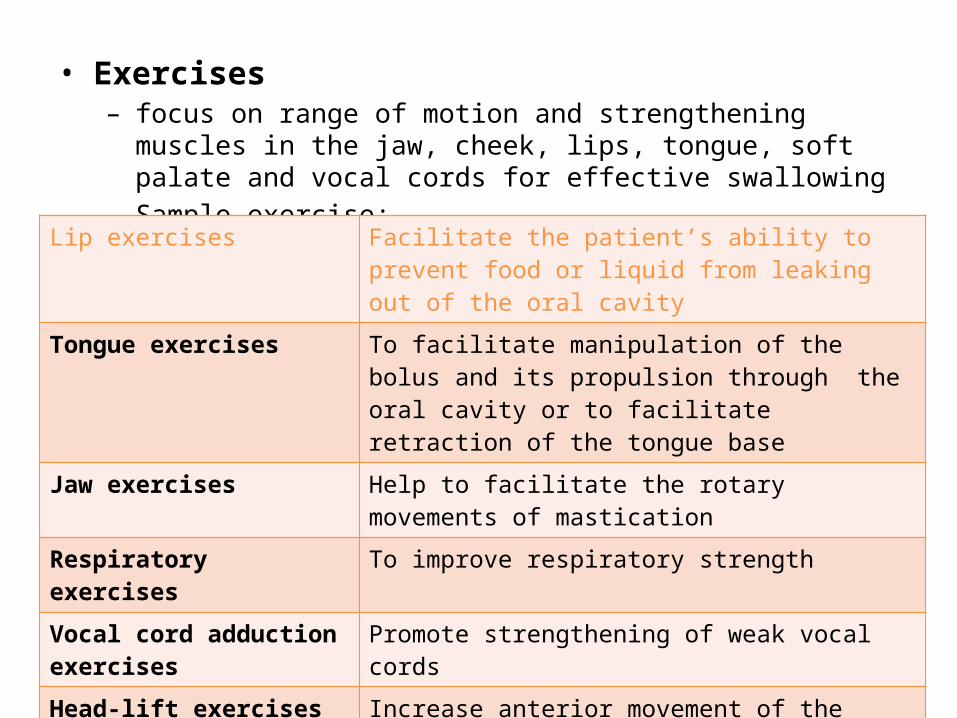
• Exercises– focus on range of motion and strengthening muscles in the jaw, cheek,
lips, tongue, soft palate and vocal cords for effective swallowing – Sample exercise:
Lip exercises Facilitate the patient’s ability to prevent food or liquid from leaking out of the oral cavity
Tongue exercises To facilitate manipulation of the bolus and its propulsion through the oral cavity or to facilitate retraction of the tongue base
Jaw exercises Help to facilitate the rotary movements of mastication
Respiratory exercises To improve respiratory strength
Vocal cord adduction exercises
Promote strengthening of weak vocal cords
Head-lift exercises Increase anterior movement of the hyolaryngeal complex and opening of the upper oesophageal sphincter
Tongue-holding maneuvers Facilitate compensatory anterior movement of the posterior pharyngeal wall
• Nutritional supply– Nasogastric tube feeding– Oroesophageal tube feeding– Oral supplement such as oral liquid supplement
• Hydration – Offering patient preferred liquids or food with high fluid content– I/V fluids or water boluses given via a feeding tube
Surgical
• Usually recommended as the last resort
Cricopharygeal MyotomyTracheostomyMedialization Laryngoplasty