Dysmorphology Congenital Anomalies Combi Oct 20
20
CHAPTER 35 1034 DYSMORPHOLOGY & HUMAN EMBRYOLOGY Birth defects are the leading cause of death in the first year of life. They are evident in 2–3% of newborn infants and in up to 7% of adults. Many are now detected by ultrasound prior to birth. Clinical investigation of the causes and conse- quences of birth defects is called dysmorphology. MECHANISMS Developmental Biology Cell proliferation and programmed cell death (apoptosis) both contribute to embryonic structural formation. The genes that control these processes are being identified. Products of other genes establish regulatory pathways in which positive and negative signaling loops initiate and maintain cell differentiation with precise timing. Cell biology now provides techniques that allow experimental access to developmental pathways. Embryology has become more experimental than descriptive and practitioners can expect systems biology to soon begin to inform them about the ori- gins of specific birth defects. This level of understanding will open the door to interventions that may well prevent birth defects or treat them prenatally. Cellular Interactions The picture emerging from experimental studies of morpho- genesis is one of a hierarchy of gene expression during devel- opment. Morphogenesis begins with expression of genes encoding transcription factors. These proteins bind to DNA in undifferentiated embryonic cells and recruit them into developmental fields, groups of cells primed to respond to specific signals later in development. This recruitment also establishes spatial relationships and orients cells with respect to their neighbors. As fields differentiate into identifiable tis- sues (eg, ectoderm, mesoderm, and endoderm), cellular pro- liferation, migration, and further differentiation are mediated through genes encoding cell signaling proteins. Signaling proteins include growth factors and their recep- tors, cellular adhesion molecules, and extracellular matrix proteins that both provide structure and position signals within developing structures. During morphogenesis groups of primed cells repeatedly proliferate, migrate, and then dif- ferentiate in response to locally expressed growth factors or signaling proteins. Within these interactions are keys to understanding not only many human birth defects but also cancer. The genes that organize cell proliferation and differ- entiation during development are often precisely those that mutate during carcinogenesis. Environmental Factors The effects of exogenous agents during development are also mediated through genetically regulated pathways. At the cel- lular level, xenobiotics (compounds foreign to nature) cause birth defects either because they disrupt cell signaling and thereby misdirect morphogenesis, or because they are cyto- toxic and lead to cell death in excess of the usual develop- mental program. In general, drug receptors expressed in embryos and fetuses are the same molecules that mediate pharmacologic effects in adults. However, effector systems may be different, reflecting incomplete morphogenesis and differences between fetal and postnatal physiology. These circumstances allow prediction of dose-response relationships during development on the one hand, but call for caution about pre- dicting effects on the other. Xenobiotics must traverse the placenta to affect embry- onic and fetal tissues. The human placenta is a relatively good barrier against microorganisms, but it is ineffective at excluding drugs and many chemicals. The physicochemical properties (eg, molecular size, solubility, and charge) that allow foreign chemicals to be absorbed into the maternal cir- culation also allow them to cross the placenta. The placenta can metabolize some xenobiotics but it is most active against steroid hormones and low-level environmental contami- nants than drugs. The timing of xenobiotic exposures is an important determinant of their effects. Morphogenic processes express so-called critical periods, during which developing organs they produce are particularly susceptible to maldevelopment. Critical periods of susceptibility are not all confined to early gestation. In particular, the developing brain is susceptible to toxicity throughout pregnancy. As discussed, over-the-counter, prescribed, and abused drugs that are pharmacologically active in mothers will be active across the placenta. Exposure to agents achieving cyto- toxic levels in adults are likely to be teratogenic (ie, cause birth defects). Abused substances such as alcohol that are toxic to adults are predictably toxic to embryos and fetuses. Drugs generally safe in adults will be generally safe for fetuses. However, keeping in mind that embryonic and fetal physiol- ogy may differ from that of an adult with respect to drug action, some risk for abnormal development must always be considered. Risk assessment requires continuous monitoring of populations exposed to drugs during pregnancy. Effects of toxic environmental contaminants on the embryo and fetus are also dose-dependent. Thus, the level of exposure to a toxin frequently becomes the primary determi- nant of its risk. Exposures producing symptoms in mothers can be assumed to be potentially toxic to the fetus. Environmental mutagens present a special problem. Animal experiments indicate that high levels of exposure to mutagenic agents are also teratogenic. Most effects are medi- ated through increased apoptosis responding to DNA dam- age. This is especially true for the developing brain. At lower doses attempts to repair DNA damage in embryonic or fetal cells may lead to somatic mutations that can contribute to carcinogenesis or be expressed as mosaic organ dysgenesis. Transplacental pharmacologic effects can also be thera- peutic. The potential for embryonic and fetal drug therapies during pregnancy is increasing. For example, folic acid
-
Upload
okenabirhie -
Category
Documents
-
view
237 -
download
6
description
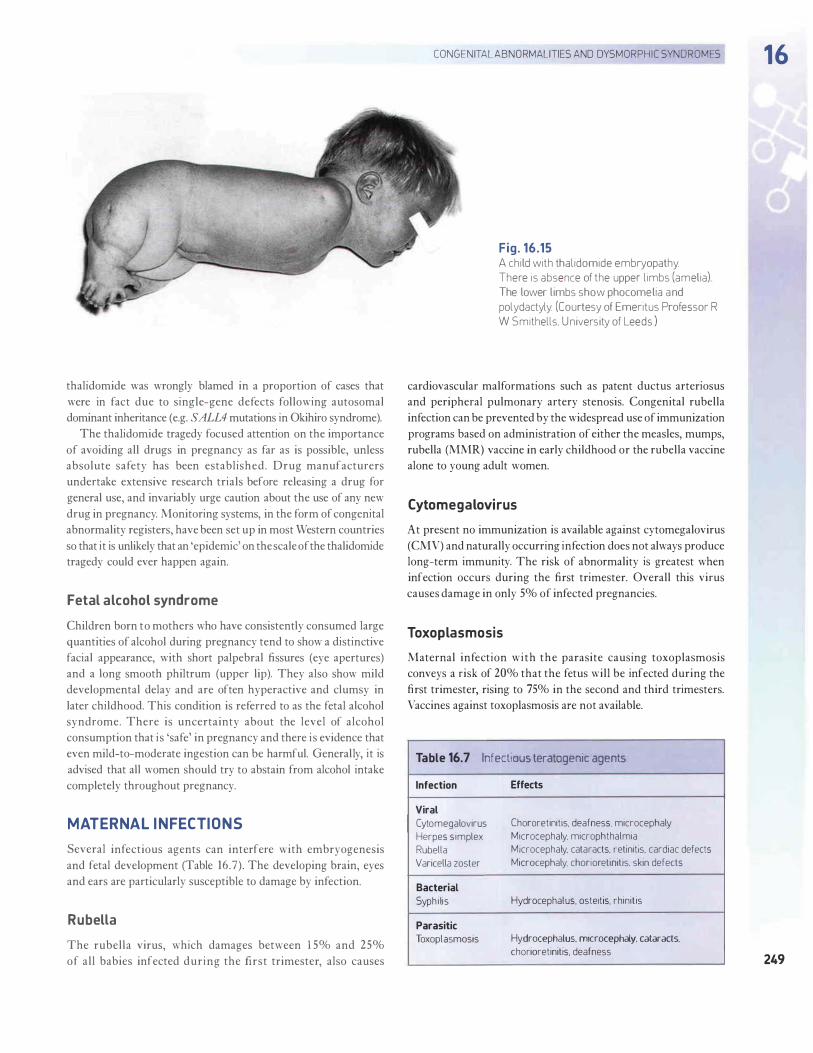
congenital abnormalities explained in detail...
Transcript of Dysmorphology Congenital Anomalies Combi Oct 20

� CHAPTER 351034
DYSMORPHOLOGY & HUMAN EMBRYOLOGYBirth defects are the leading cause of death in the first year oflife. They are evident in 2–3% of newborn infants and in upto 7% of adults. Many are now detected by ultrasound priorto birth. Clinical investigation of the causes and conse-quences of birth defects is called dysmorphology.
MECHANISMS
Developmental BiologyCell proliferation and programmed cell death (apoptosis)both contribute to embryonic structural formation. Thegenes that control these processes are being identified.Products of other genes establish regulatory pathways inwhich positive and negative signaling loops initiate andmaintain cell differentiation with precise timing. Cell biologynow provides techniques that allow experimental access todevelopmental pathways. Embryology has become moreexperimental than descriptive and practitioners can expectsystems biology to soon begin to inform them about the ori-gins of specific birth defects. This level of understanding willopen the door to interventions that may well prevent birthdefects or treat them prenatally.
Cellular InteractionsThe picture emerging from experimental studies of morpho-genesis is one of a hierarchy of gene expression during devel-opment. Morphogenesis begins with expression of genesencoding transcription factors. These proteins bind to DNAin undifferentiated embryonic cells and recruit them intodevelopmental fields, groups of cells primed to respond tospecific signals later in development. This recruitment alsoestablishes spatial relationships and orients cells with respectto their neighbors. As fields differentiate into identifiable tis-sues (eg, ectoderm, mesoderm, and endoderm), cellular pro-liferation, migration, and further differentiation aremediated through genes encoding cell signaling proteins.
Signaling proteins include growth factors and their recep-tors, cellular adhesion molecules, and extracellular matrixproteins that both provide structure and position signalswithin developing structures. During morphogenesis groupsof primed cells repeatedly proliferate, migrate, and then dif-ferentiate in response to locally expressed growth factors orsignaling proteins. Within these interactions are keys tounderstanding not only many human birth defects but alsocancer. The genes that organize cell proliferation and differ-entiation during development are often precisely those thatmutate during carcinogenesis.
Environmental FactorsThe effects of exogenous agents during development are alsomediated through genetically regulated pathways. At the cel-lular level, xenobiotics (compounds foreign to nature) causebirth defects either because they disrupt cell signaling and
thereby misdirect morphogenesis, or because they are cyto-toxic and lead to cell death in excess of the usual develop-mental program.
In general, drug receptors expressed in embryos andfetuses are the same molecules that mediate pharmacologiceffects in adults. However, effector systems may be different,reflecting incomplete morphogenesis and differencesbetween fetal and postnatal physiology. These circumstancesallow prediction of dose-response relationships duringdevelopment on the one hand, but call for caution about pre-dicting effects on the other.
Xenobiotics must traverse the placenta to affect embry-onic and fetal tissues. The human placenta is a relatively goodbarrier against microorganisms, but it is ineffective atexcluding drugs and many chemicals. The physicochemicalproperties (eg, molecular size, solubility, and charge) thatallow foreign chemicals to be absorbed into the maternal cir-culation also allow them to cross the placenta. The placentacan metabolize some xenobiotics but it is most active againststeroid hormones and low-level environmental contami-nants than drugs.
The timing of xenobiotic exposures is an importantdeterminant of their effects. Morphogenic processes expressso-called critical periods, during which developing organsthey produce are particularly susceptible to maldevelopment.Critical periods of susceptibility are not all confined to earlygestation. In particular, the developing brain is susceptible totoxicity throughout pregnancy.
As discussed, over-the-counter, prescribed, and abuseddrugs that are pharmacologically active in mothers will beactive across the placenta. Exposure to agents achieving cyto-toxic levels in adults are likely to be teratogenic (ie, cause birthdefects). Abused substances such as alcohol that are toxic toadults are predictably toxic to embryos and fetuses. Drugsgenerally safe in adults will be generally safe for fetuses.However, keeping in mind that embryonic and fetal physiol-ogy may differ from that of an adult with respect to drugaction, some risk for abnormal development must always beconsidered. Risk assessment requires continuous monitoringof populations exposed to drugs during pregnancy.
Effects of toxic environmental contaminants on theembryo and fetus are also dose-dependent. Thus, the level ofexposure to a toxin frequently becomes the primary determi-nant of its risk. Exposures producing symptoms in motherscan be assumed to be potentially toxic to the fetus.
Environmental mutagens present a special problem.Animal experiments indicate that high levels of exposure tomutagenic agents are also teratogenic. Most effects are medi-ated through increased apoptosis responding to DNA dam-age. This is especially true for the developing brain. At lowerdoses attempts to repair DNA damage in embryonic or fetalcells may lead to somatic mutations that can contribute tocarcinogenesis or be expressed as mosaic organ dysgenesis.
Transplacental pharmacologic effects can also be thera-peutic. The potential for embryonic and fetal drug therapiesduring pregnancy is increasing. For example, folic acid
Hay_CH35_p1020-1053.qxd 6/18/10 12:40 PM Page 1034

�GENETICS & DYSMORPHOLOGY 1035
supplementation can lower risks for birth defects such asspina bifida, and maternally administered corticosteroids caninduce fetal synthesis and secretion of pulmonary surfac-tants prior to delivery.
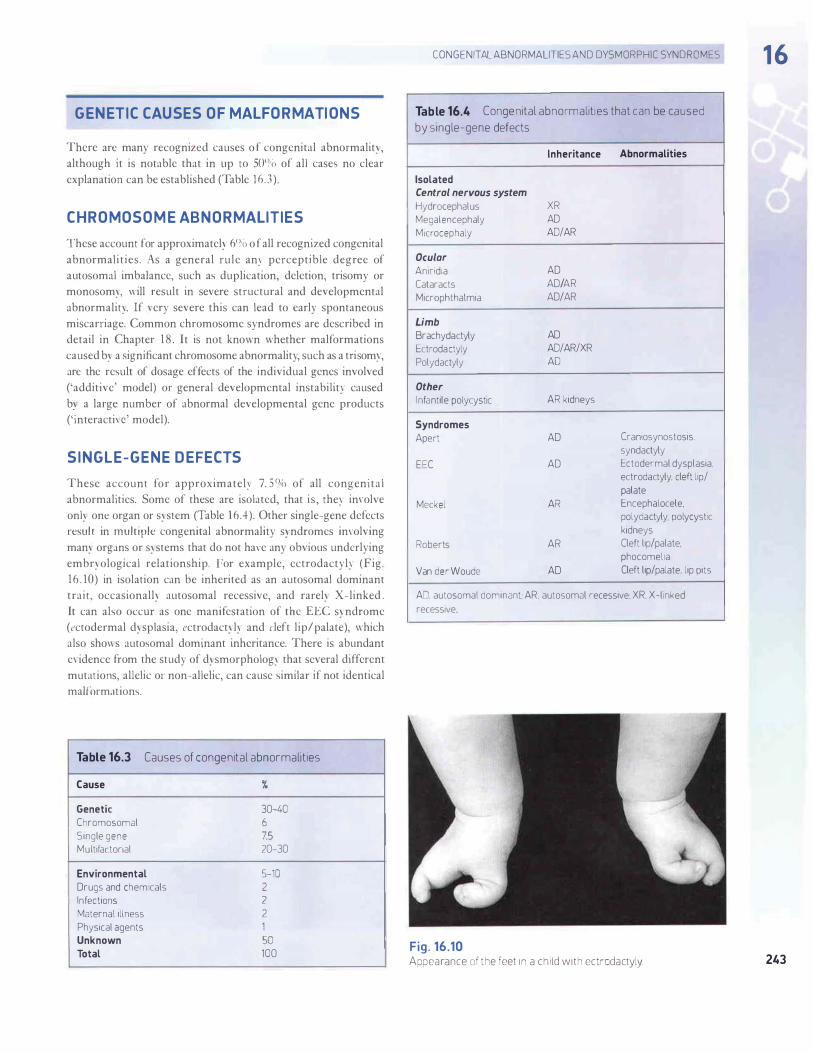
Mechanical FactorsMuch of embryonic development and all of fetal growthoccurs normally within the low pressure and space providedby amniotic fluid. Loss or inadequate production of amnioticfluid can have disastrous effects, as can disruption of placen-tal membranes. Disruption of placental membranes in earlygestation leads to major structural distortion and most oftenlethal. Later, deformation or even amputation of fetalextremities (amniotic band sequence) can occur.
Movement is also important for morphogenesis. Fetalmovement is necessary for normal development of joints andis the principal determinant of folds and creases present atbirth in the face, hands, feet, and other areas of the body.Clubfoot is an etiologically heterogeneous condition inwhich the foot is malpositioned at birth. It more often resultsfrom mechanical constraint secondary to intrauterinecrowding, weak fetal muscles, or abnormal neurologic func-tion than from primary skeletal maldevelopment.
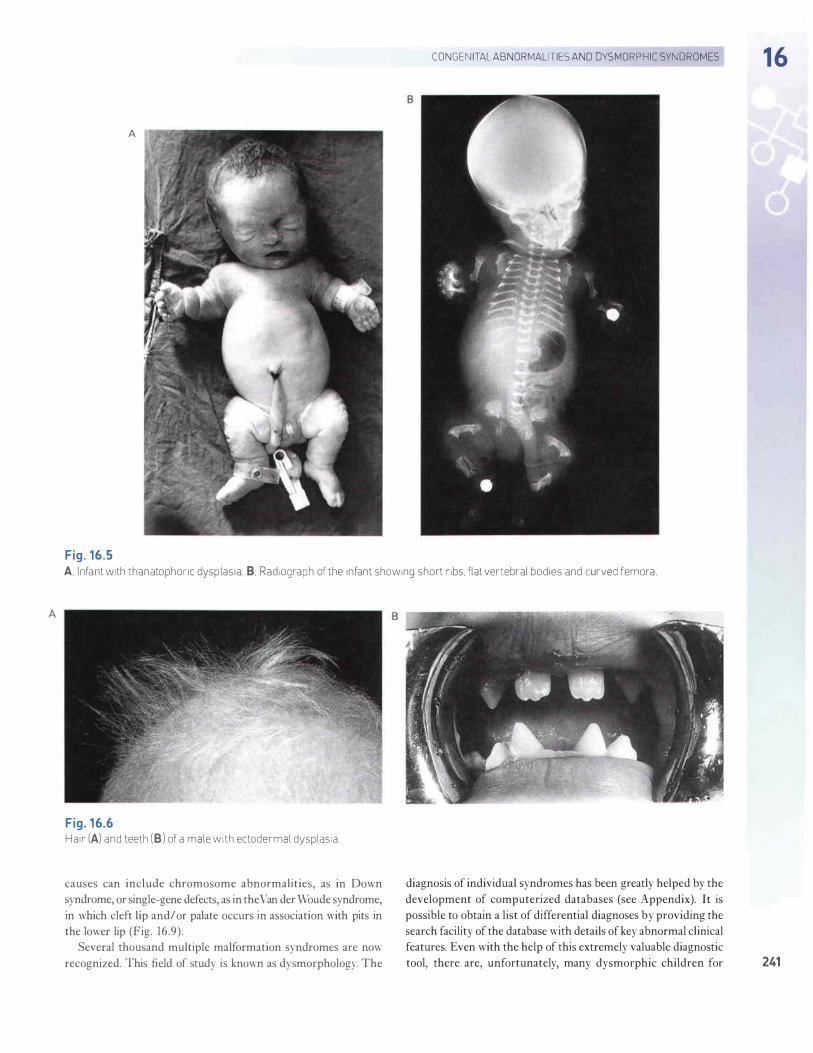
Lung and kidney development are particularly sensitiveto mechanical forces. Constriction of the chest throughmaldevelopment of the ribs, lack of surrounding amnioticfluid, or lack of movement (fetal breathing) leads to varyingdegrees of pulmonary hypoplasia in which lungs are smallerthan normal and develop fewer alveoli. Mechanicallyinduced pulmonary hypoplasia is a common cause of respi-ratory distress at birth and may be lethal.
Cystic renal dysplasia is frequently associated withobstruction ureters or bladder outflow. As pressure withinobstructed renal collecting systems increases it distorts cellinteractions and alters histogenesis. Developing kidneysexposed to increased internal pressures for long periodseventually become nonfunctional.
CLINICAL DYSMORPHOLOGYThe most important task for the clinician presented with aninfant with a birth defect is to determine whether the prob-lem is isolated or part of a larger embryopathy (syndromic).
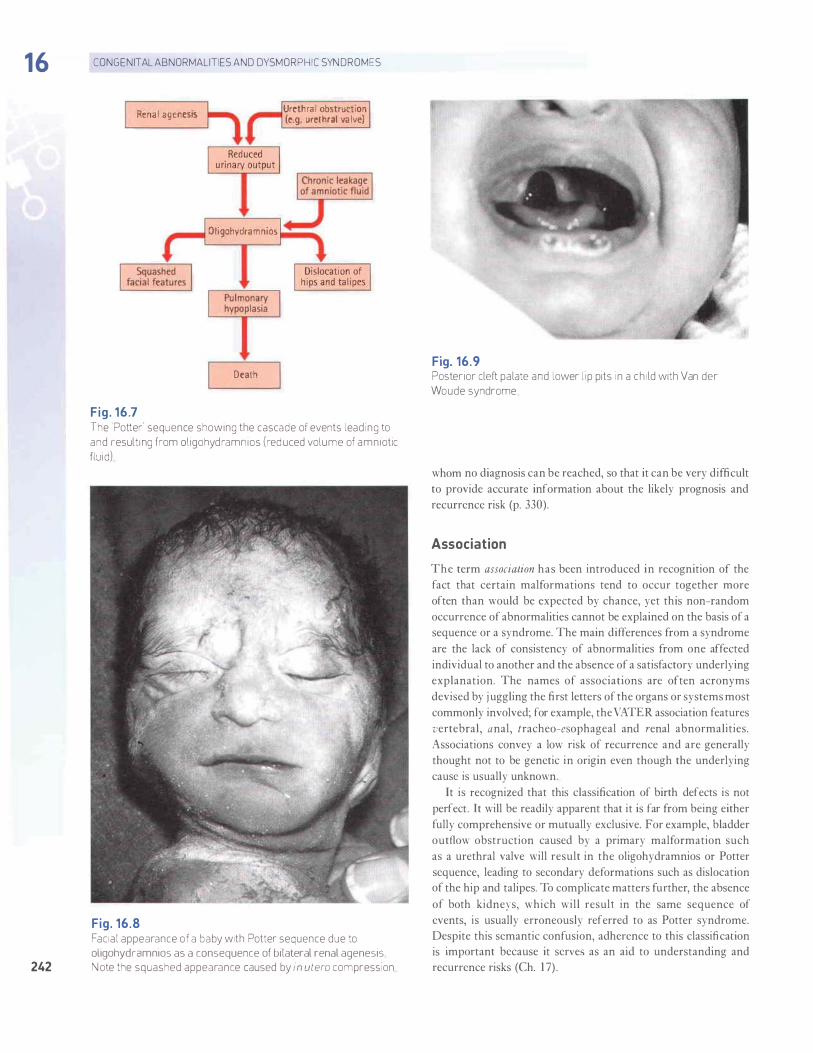
TerminologyClassification of dysmorphic features strives to reflect mech-anisms of maldevelopment. However, much of the terminol-ogy that describes abnormal development in humansremains historical and documents recognition of patternsprior to understanding of their biology. For example, birthdefects are referred to as malformations when they resultfrom altered genetic or developmental processes. When phys-ical forces interrupt or distort morphogenesis, their effectsare termed disruptions and deformations, respectively.The term dysplasia is used to denote abnormal histogenesis.
Malformations occurring together more frequently than wouldbe expected by chance alone may be classified as belonging toassociations. Those in which the order of maldevelopment isunderstood may be referred to as sequences. For example,Robin sequence (or Pierre Robin anomalad) is used to describecleft palate that has occurred because poor growth of the jaw(retrognathia) has displaced the tongue and prevented poste-rior closure of the palate. Syndromes are simply recurrent pat-terns of maldevelopment, which have in many cases a knowngenetic cause.
Evaluation of the Dysmorphic InfantCaring for infants with birth defects can be very stressful.The extent of an infant’s abnormalities may not be immedi-ately apparent, and parents who feel grief and guilt are oftendesperate for information. However, as with any medicalproblem the history and physical examination provide mostof the clues to diagnosis. Special aspects of these proceduresare outlined in the following sections.
A. History
Pregnancy histories nearly always contain important cluesto the diagnosis. Parental recall after delivery of an abnor-mal infant is better than recall after a normal birth. Anobstetric wheel can help document gestational age andevents of the first trimester: the last menstrual period, theonset of symptoms of pregnancy, the date of diagnosis of thepregnancy, the date of the first prenatal visit, and the physi-cian’s impressions of fetal growth at that time. Family histo-ries should always be reviewed. Environmental historiesshould include descriptions of parental habits and work set-tings in addition to medications and use of drugs, tobacco,and alcohol.
B. Physical Examination
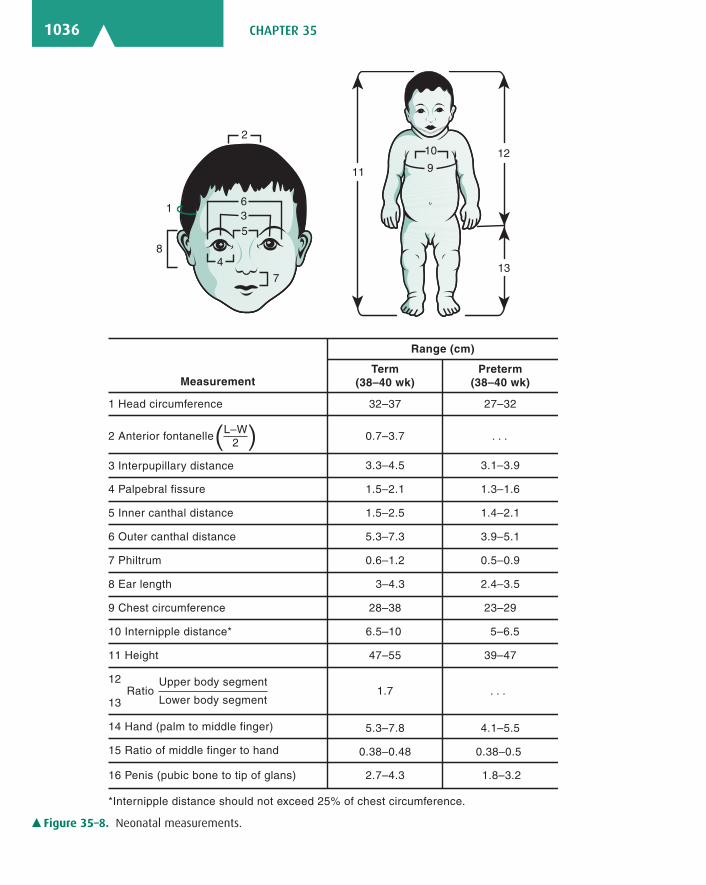
Meticulous physical examination is crucial for accurate diag-nosis in dysmorphic infants and children. In addition to theroutine procedures described in Chapter 1, special attentionshould be paid to the neonate’s physical measurements(Figure 35–8). Photographs are helpful and should include aruler for reference.
C. Imaging and Laboratory Studies
Radiologic and ultrasonographic examinations can beextremely helpful in the evaluation of dysmorphic infants.Films of infants with apparent limb or skeletal anomaliesshould include views of the skull and all of the long bones inaddition to frontal and lateral views of the axial skeleton.Chest and abdominal films should be obtained when indi-cated. The pediatrician should consult a radiologist for fur-ther workup. Computed tomography (CT), magneticresonance imaging (MRI), and ultrasonography are all usefuldiagnostic tools, but their interpretation in the face of birthdefects may require considerable experience.
Hay_CH35_p1020-1053.qxd 6/18/10 12:40 PM Page 1035
� CHAPTER 351036
12
13
11
8
2
9
4
7
6
5 3
10
1
Range (cm)
Measurement Term
(38–40 wk)Preterm
(38–40 wk)
1 Head circumference
2 Anterior fontanelle
3 Interpupillary distance
4 Palpebral fissure
5 Inner canthal distance
6 Outer canthal distance
7 Philtrum
8 Ear length
9 Chest circumference
10 Internipple distance*
11 Height
12 Upper body segment
13 Lower body segment
14 Hand (palm to middle finger)
32–37
*Internipple distance should not exceed 25% of chest circumference.
15 Ratio of middle finger to hand
16 Penis (pubic bone to tip of glans)
0.7–3.7
3.1–3.9
1.3–1.6 1.5–2.1
1.5–2.5
5.3–7.3
0.6–1.2
3–4.3
28–38
3.3–4.5
. . .
Ratio
6.5–10
47–55
1.7
5.3–7.8
0.38–0.48
1.4–2.1
3.9–5.1
0.5–0.9
2.4–3.5
23–29
5–6.5
39–47
. . .
4.1–5.5
0.38–0.5
2.7–4.3 1.8–3.2
27–32
L–W2( )
� Figure 35–8. Neonatal measurements.
Hay_CH35_p1020-1053.qxd 6/18/10 12:40 PM Page 1036

�GENETICS & DYSMORPHOLOGY 1037
Traditional cytogenetic analysis provides specific diag-noses in approximately 5% of dysmorphic infants who sur-vive the neonatal period. Chromosomal abnormalities arerecognized in 10–15% of infants who die. With the availabil-ity of Chromosomal microarray at least 10–15% additionalsubtle chromosomal anomalies has been identified. Of note,many copy number variations (CNV) exist in different indi-viduals, therefore, interpretation is sometimes difficult andmay require parental samples for clarification. Common dis-orders such as trisomies 21 and 18 can be determined rapidlythrough use of FISH, but this technique should always beaccompanied by a complete karyotype. A normal karyotypedoes not rule out the presence of significant genetic disease.Any case requiring rapid diagnosis should be discussed withan experienced clinical geneticist.
D. Perinatal Autopsy
When a dysmorphic infant dies, postmortem examination canprovide important diagnostic information. The pediatricianshould discuss the case thoroughly with the pathologist, andphotographs should always be taken. Radiologic imagingshould be included whenever limb anomalies or dispropor-tionate growth is present. Tissue, most often skin, should besubmitted for cytogenetic analysis. Fibroblasts from these stud-ies should routinely be frozen and preserved for future studies.The pediatrician and the pathologist should also considerwhether samples of blood, urine, or other tissue should beobtained for biochemical analyses. Placental as well as fetaltissue can be used for viral culture.
Hudgins L, Cassidy SB: Congenital anomalies. In RJ Martin et al(editors): Fanaroff and Martin’s Neonatal-Perinatal Medicine—Diseases of the Fetus and Infant, 8th ed. Elsevier Mosby,Philadelphia, 2006: 561–582.
� CHROMOSOMAL DISORDERS: ABNORMAL NUMBER
TRISOMIES
1. Trisomy 21 (Down Syndrome)
ESSENT IALS OF D IAGNOS I S & TYP I CAL F EATURES
� Characteristic features include upslanting palpebral fis-sures, epicanthal folds, midface hypoplasia, and small,dysplastic pinnae.
� Generalized hypotonia.� Cognitive disabilities (usually mild to moderate).� Associated with congenital heart disease and gastroin-
testinal anomalies.
Down syndrome occurs in about 1:760 newborns. Cognitivedisabilities are characteristic of Down syndrome, as is gener-alized hypotonia. The affected newborn may have prolongedphysiologic jaundice, polycythemia, and a transient leuke-moid reaction. Feeding problems are common duringinfancy. Problems which may be seen during childhoodinclude thyroid dysfunction, hearing loss, celiac disease, andatlanto-occipital instability. Leukemia is 12–20 times morecommon in Down syndrome patients.
� Clinical FindingsThe principal physical findings include a flattened occiput,characteristic facies (up-slanting palpebral fissures, epican-thal folds, midface hypoplasia, and small, dysplastic pinnae),and minor limb abnormalities. About one-third to one-halfof children with Down syndrome have congenital heart dis-ease, most often endocardial cushion defects or other septaldefects. Anomalies of the gastrointestinal tract, includingesophageal and duodenal atresias, are seen in about 15%of cases.
Information regarding health care guidelines for patients withDown syndrome: http://www.downsyn.com/guidelines/health-care.html
2. Trisomy 18 SyndromeThe incidence of trisomy 18 syndrome is about 1:4000 livebirths, and the ratio of affected males to females is approxi-mately 1:3. Trisomy 18 is characterized by prenatal and postna-tal growth retardation that is often severe, and hypertonicity.Complications are related to associated birth defects. Death isoften caused by heart failure or pneumonia and usually occursin infancy or early childhood, although a small percentage ofpatients reach adulthood. Surviving children show significantcognitive disabilities.
� Clinical FindingsInfants with trisomy 18 are often small for gestational ageand have dysmorphic features including a characteristicfacies and extremities (overlapping fingers and rockerbottomfeet), and congenital heart disease (often ventricular septaldefect or patent ductus arteriosus). To see clinical picturesof patients with trisomy 18, visit the following web site:http://medgen.genetics.utah.edu/photographs/pages/trisomy_18.htm.
3. Trisomy 13 SyndromeThe incidence of trisomy 13 is about 1:12,000 live births, and60% of affected individuals are female. Most infants with tri-somy 13 have congenital anomalies that are incompatible withsurvival. Surviving children demonstrate failure to thrive, cog-nitive disabilities, apneic spells, seizures, and deafness. Death
Hay_CH35_p1020-1053.qxd 6/18/10 12:40 PM Page 1037