Dub Fer Undip
52
DYSFUNCTIONAL UTERINE BLEEDING Oleh : Adi Setyawan Prianto Program Pendidikan Konsultan Fertilitas dan Endokrinologi Reproduksi Bagian/SMF Obstetri dan Ginekologi Fakultas Kedokteran Universitas Diponegoro SEMARANG Revised 2010
-
Upload
nurul-arsy-m -
Category
Documents
-
view
235 -
download
1
Transcript of Dub Fer Undip
-
DYSFUNCTIONAL UTERINE BLEEDINGOleh :Adi Setyawan PriantoProgram Pendidikan Konsultan Fertilitas dan Endokrinologi ReproduksiBagian/SMF Obstetri dan GinekologiFakultas Kedokteran Universitas DiponegoroSEMARANGRevised 2010
-
Dysfunctional Uterine Bleeding :The spectrum of abnormal menstrual bleeding patterns that may occurin anovulatory women who have no medical illness, or pelvic pathology.
Medical treatment based on sound physiologic concepts. Designed to achieve 2 specific goals : 1. to reverse the abnormalities of endometrial growth and development. 2. to induce or restore cyclic predictable menses of normal volume and duration.DEFINITIONLeon Speroff et al : Clinical Gynecologic Endocrinology and Infertility 7 ed 2005
-
REGULATION OF THE MENSTRUAL CYCLEMenstruation is the response of the endometrium to the withdrawal of progesterone (and estrogen) that occurs with the demise of the corpus luteum in the absence of pregnancy(Fig. 1). Involves complex interactions between the endocrineand immune system are the component blood vessels and the dynamic population of leukocytes that influx at this time (Fig. 2).FIG. 2. Distribution of CD56ve uNK cells in endometrium during the secretory phase of the cycle. This shows the close clustering of the uNK cells (solid arrow). The spiral vessels are indicated by openarrows.Jabbour et al. Regulation of Menstrual Function Endocrine Reviews, February 2006, 27(1):1746 19
-
FIG. 1. Illustration of the alternatives for a progesterone-primed endometrium. The progesterone induced changes that characterize the endometrium primed for implantation also bring about progesterone dependency of the tissue. On the demise of the corpus luteum, falling progesterone levels initiate an inflammatory process that starts in the stromal compartment but involves leukocyte immigration and metalloproteinase (MMP) activation. Eventual shedding of the functional layer of the endometrium opens the way for estrogen-dependent regrowth of the tissue.
18 Endocrine Reviews, February 2006, 27(1):1746 Jabbour et al. Regulation of Menstrual FunctionDownloaded from edrv.endojournals.org at Indonesia:Endo Jnls Sponsored
-
Figure 1. Molecular and cellular events occurring after progesterone withdrawal (Critchley et al., 2001). Coincident events of progesterone withdrawal and hypoxia. Progesterone withdrawal results in an up-regulation of inflammatory mediators, production of MMPs, a leucocyte influx and expression of stromal KDR in the upper endometrial zones. There is coincident hypoxia and an up-regulation of VEGF. VEGF binds to its type 2 receptor, KDR, and there is a paracrine/autocrine action on the up-regulation of MMP production in the same endometrial upper zone stromal cells. Menstrual sloughing takes place from the superficialregions of the endometrium. KDR, kinase insert domaincontaining receptor or VEGF receptor 2; PGF2a, prostaglandin F2a.
-
There are three classic phases of the menstrual cycle: An estrogen-dominated preovulatory phase, a postovulatory and progesterone-dominated secretory phase, 3. And a menstrual phase following progesterone withdrawal that accompanies demise of the corpus luteum.
The endometrium is composed of two layers and is a target tissue for steroid hormones. The upper functional layer is shed at menstruation. The endometrium regenerates after menstrual shedding from an underlying basal layer.Parameters of normal menstruationThe menstrual cycle is generally defined in the context of its length, regularity, frequency, and pattern of menstrual blood loss. Studies have indicated that the mean menstrual cycle length in the mid-reproductive years is between 28 and 30 d.The duration of the period of menstruation is commonly 45 d, with the period of heaviest bleeding reported in the first 2 d of menses, whereas the volume of blood loss varies between 25 and 35 ml.
by Fraser and Inceboz (287).
-
The progesterone-dominated latter half of the menstrual cycle is constituted by an early, mid, and late secretory phase.The pattern of sex steroid receptor expression in the endometrium across the secretory phase reflects the fact that theearly secretory phase is regulated by both estrogen and progesterone.The mid secretory phase is regulated by progesterone alone as estrogen receptor (ER) is down-regulated in the glands and stroma at this time (9); and the late secretoryphase is associated with progesterone withdrawal and,consequently, menstruation.FIG. 4. Progesterone withdrawal activates many pathways; prominent among these are those releasing vasoactive agents. Chemotactic agents,which synergize with vasoactive agents, are also expressed. There is no doubt that MMPs, which degrade the interstitial matrix of the endometrium, play a major role in the menstruation process, but their origin is uncertain.MMPs can be released from both resident endometrium stromal cells and invading leukocytes.
-
Mechanisms Involved in ONSET and CESSATION of Normal Menstruation ONSET Menstruation : Basically, menstruation was envisioned as ischaemic necrosis of the endometrium caused by vasoconstriction spiral arterioles in the basal layer, trigerred by withdrawal of estrogen and progesterone. Initiation of menstruation is an enzymatic autodigestion of the functioal layer of the endometrium with its subsurface capillary plexus, possibly extending to the spiral arteriol system in the basal layer.
CESSATION Menstruation: Similarly, the end of menses was explained by longer and more intense waves of vaso constriction, combine with coagulation mechanisms activated by vascular stasis and endometrial collaps, aided by rapid reepithelization mediated by estrogen derived from the emerging new follicular cohort. The end normal menstruation is Coagulation mechanisms, Local vasocontriction, and Re-epithelization all contribute to hemostasis.
-
The enzymatic degradation of the endometrium i.e. the release of intracellular lysosomal enzymes, proteases from inflitrating inflammatory cells, and the actions of matrix metallo-proteinases.
Progesterone withdrawal also stimulates an inflammatory response in the endometrium.The inflammatory inflitrate ( i.e. neutrophils, eosinophils and macrophage or monocytes)is drawn by chemokines (interleukin 8; IL 8),some of which are down regulated by progesterone.
Matrix metalloproteinases are family a proteolitic enzymes that degrade components of the extra cellular matrix and basement membrane.
Progressive enzymatic degradation of the endometrium eventually disrups the subsurface capillary and venous vascular system, causing interstitial hemorrhage; dissolution of the surface membrane allow blood to escape into the endometrial cavity.Desquamation begins in the fundus and gradually extends toward the isthmus.
-
The menstrual fluid is composed of an autolysed endometrium rich in inflamatorry exudates, red blood cells, and proteolytic enzymes. PLASMIN, has potent fibrinolityc action that help to prevent clotting of menstrual fluid and to facilitate the expulsion of degenerated tissue.
To some extent, the amount of menstrual bleeding is controlled by the local balance between fibrinolysis and clotting Endometrial stromal cells tissue factor and plasminogen activator inhibitor (PAI)-I promote clotting and help to balance fibrinolytic processes. Early in menstruation, intravascular platelet plugs, and later thrombi from at shedding surface, helping to limit blood loss. Myometrial contractions are not important for control of menstrual bleeding.
STROMAL REGENERATION : Matrix metalloproteinases present in the menstrual endometrium may be important mediators of the release and activation of growth factors needed for endometrial repair. VEGF is an important promoter of endometrial mitosis and can be induced by TNF , TGF and IGF-1. The endometrium is not repaired, but completely remodeled at regular intervals.
-
Figure 2. Breakdown and restoration in the endometrium. Tissue is shed as a result of the action of MMP. Re-epithelialization is very rapid and occurs from theopen mouths of the glands and from the unshed portions of the luminal epithelium. Leucocyte products and a variety of other factors derived from the epithelium itself are postulated to play a role in re-epithelialization. Subsequent restoration of the underlying stroma includes proliferation of cells associated with blood vessels and endometrial stromal cells, along with the laying down of the extracellular matrix. These events are postulated to occur under the influence of increasing estrogenconcentrations and are probably locally regulated by a number of growth factors and other regulatory factors (Salamonsen, 2003). MT1, membrane type 1; ET-1, endothelin 1; BMP-6, bone morphogenetic protein 6; BV, blood vessel; FGFs, fibroblast growth factors.The ESHRE Capri Workshop Group 424
-
Endometrial Responses to Steroid Hormones : Physiologic and Pharmacologic Normal menstrual bleeding at the end of an ovulatory cycle results from estrogen- progesterone withdrawal. Other examples : include the bleeding that follows discontinuiton of both estrogen and progestin in women receiving cyclic postmenopausal hormone therapy and oral contraceptives. Under these circumstance, bleeding generally is regular, predictable, and consistent in volume and duration.
However, estrogen-progesterone withdrawal is not the only pattern of steroid hormone signals that can provoke endometrial bleeding. Bleeding can also result from : 1. Estrogen withdrawal, 2, Estrogen breakthrough, 3. Progesterone withdrawal, and 4. Progesterone breakthrough.
-
ESTROGEN WITHDRAWAL BLEEDING :
One clinical sample of estrogen withdrawal bleeding is that bilateral ooforectomy during follicular phase of the cycle. Other examples include cyclic estrogen only hormone therapy in castrate ,or post menopausal women and midcycle bleeding that coincides with the transient , but abrupt fall estrogen levels immediately before ovulation.ESTROGEN BREAKTHROUGH BLEEDING : The best examples of estrogen breakthrough bleeding are different patterns of bleeding observed in women with chronic anovulation. Relatively low levels of chronic estrogen exposure typically result in intermittent spotting or staining that is generally light in volume but may be prolonged. In contrast, sustained high level estrogen stimulation commonly results in long intervals of amenorrhea punctuated by acute episodes of often profuse bleeding that vary in duration.
-
PROGESTERONE WITHDRAWAL BLEEDING :
Progesterone withdrawal bleeding is observed when treatment with exogenous progesterone, or synthetic progestin is discontinued.
It usually occurs only when endometrium has first been primed with endogenous or exogenous estrogen.
The amount and duration of bleeding can vary widely and generally corelates with the level and duration previous estrogen stimulated endometrial prolifertaion.
In women receiving cyclic hormone therapy with exogenous estrogen and progestin, bleeding follows withdrawal of progesterone, even if estrogen treatment continues
Progestin withdrawal bleeding can be delayed, but only if estrogen levels are increased 10-20 fold.
-
PROGESTERONE BREAKTHROUGH BLEEDING :
Progesterone breakthrough bleeding occurs when the ratio of progesterone to estrogen is unfavorably high. Clinical examples of progesterone breakthrough bleeding are the bleeding observed in women using the progestin-only contraceptive mini-pill or other long acting progestin only conraceptive methodes (progestin implants, depot medroxyprogesterone acetates),
Also women using combination estrogen-progestin oral contraceptives, in which net effect of oral contraceptives on the endometrium is profoundly progestational.
-
Abnormal Uterine Bleeding with Combination OCPs
-
TABLE 4 Treatment Options for Abnormal Uterine Bleeding in Women Using Hormonal Contraception
TreatmentDosageNonsteroidal anti-inflammatory drug such as ibuprofen (e.g., Advil, Motrin) 800 mg three times daily for 1 to 2 weeks or until bleeding stopsSupplemental estrogen Conjugated equine estrogens (Premarin) 0.625 to 1.25 mg per day for 1 to 2 weeksEthinyl estradiol (Estinyl)20 mcg per day for 1 to 2 weeks Estradiol (Estrase) 0.5 to 1 mg per day for 1 to 2 weeks
-
Abnormal Uterine Bleeding with Progestin-Only Contraceptions
Abnormal Uterine Bleeding with Progestin-Only Contraception
Abnormal Uterine Bleeding with Progestin-Only Contraception
Abnormal Uterine Bleeding with Progestin-Only Contraception
-
Presumed Dysfunctional Uterine Bleeding in Women of Childbearing Age: Evaluation Based on Risk Factors for Endometrial Cancer
-
ANOVULATORY BLEEDING Anovulatory bleeding can represent : 1. Estrogen withdrawal bleeding : reflecting the transient fall in estrogen levels resulting from regression of the most recent follicular cohort. 2. Estrogen breakthrough bleeding :due to focal breakdown of an overgrown and structurally fragile endometrium under continous estrogen stimulation. Tend to occur in women with : 1.Polycystic ovarian syndrome. 2. Obese women. 3. Postmenarcheal adolescent 4. Perimenopausal women To older women who is deeply concerned that she may have CANCER.
-
Session IIDYSFUNCTIONAL UTERINE BLEEDING LECTURE11 Oktober 2010 Revised
-
ANOVULATORY BLEEDINGANOVULATORY BLEEDINGEstrogen withdrawal bleedingTransient fall estrogen levelRegression of most follicular cohortEstrogen breakthrough bleeding1. Focal breakdown 2. Structurally fragile endometriumUnder continous estrogen stimulationClinical examples :1.Polycystic ovary syndrome2. Obese women.3. Postmenarcheal adolescents.4. Perimenopausal women
-
Characterizes Anovulatory WomanAlways in the follicular phase of the ovarian cycle.In the proliferative phase of the endometrial cycle.There is no luteal or secretory phase, because there is no cycle.The only ovarian steroid signal the endometrium receives is estrogen.Estrogen level constanly fluctuate, rising and falling as each grow of cohort follicles and later into atresia.
-
DIFFERENTIAL DIAGNOSISAccident or complicationof pregnancyPossibility of underlying pathologyThyroid disordersCoagulopathyMedicationsPost tubal ligation syndrome1. Threatened or incomplete abortion2. Ectopic pregnancy.1. Uterine neoplasia2. Cervical and endometrial polyps3. Adenomyosis.1. Hypothyroidism 2. Hyperthyroidism.1. A hystory of postpartum hamorrhage or 2. Excessive bleeding with surgery,3. Dental procedurs,or trauma1. Glucocorticoids, tamoxifen, and anticoagulants.2. Herbs have estrogenic activity.Affects ovarian blood supply, increased after sterilization by electrocautery.1.2.3.4.5.6.
-
DIAGNOSTIC EVALUATION OF ABNORMAL BLEEDINGTrue anovulatory bleeding1. Without additional laboratory evaluation2.Infrequent, irregular, unpredictable menstrual bleedingAnatomical lesion Regular monthly periods that heavy and prolonged1.Serum progesterone > 3 ng/mL : ovulation.2. TSH3. BIOPSI : Biopsi (-) : endometrial thickness < 5 mm. Biopsi (+), if the clinical history suggests long-term unopposed estrogen exposure and endometrial thickness > 12 mmLaboatory test :
-
PROGESTIN THERAPYProgestins arepowerful antiestrogensAndrogenEstradiolEstradiol sulfateAndrogenEstroneEstrone sulfateAromataseSulfotransferaseAromataseSulfataseSulfotransferase17-hydroxysteroiddehidrogenase1. Progestin stimulate 17-hydroxysteroid dehidrogenase and sulfotransferase activity.2. Estrogen receptor replenishment.3. Suppress estrogen mediated transcription of oncogens.The ANTIMITOTIC growth-limiting effects on endometriumPrevention and reversal hyperplasia.Arrest of growth secretory phase (pregnancy and oral contraceptive combination.)
-
Continued Progestin Therapy ..Oligomenorrheic anovulatory womenWith episodic abnormal bleedingMedroxyprogesterone acetate(5-10 mg daily for 2 weeks every month)Self-limited progesterone withdrawal bleedingWhen menses (-)Possibility of a more profoundovulatory dysfunction due to grossly low estrogen levels.Anovulatory with metrorrhagia/polymenorrheaProgestin treatment for 14 daysInduce stabilizing predecidual changes in a vascular and fragile endometriumand withdrawal medical curettageFailed progestin treatmentDiagnostic evaluation12.3.
-
ORAL CONTRACEPTIVE THERAPYProlonged episodes of heavy anovulatory bleedingUniformly increased endometrial thicknessTransvaginal ultrasound examinationMinimize the risk of unsuccessful treatmentWith continued heavy blood loss.Higher doses progestin therapy(medroxyprogesterone acetate 20 mg , orNorethindrone acetate 5 mg daily)Low dose monophasic combination oral contraceptive (one pill twice daily)Bleedings stop expected within 24 48 hours.Continue for at least5-7 days even when bleeding stopIf oral contraceptive cannot be usedDiagnostic evaluation
-
ESTROGEN THERAPYIntermitten vaginal spottingFrankly low levels of estrogen stimulation(estrogen breakthrough bleeding)Transvaginal ultrasound1. Defining endometrial thickness 2. Anatomic abnormality of the uterine cavity.Estrogen levels are insufficient to stimulste the growth asfondation of actions of progesteroneEndometrium is attenuated and bleeding is acute and heavy1,25 mg conjugated estrogensTappering tp once daily dose for 7-10 days afterbleeding is controlledFollowed by treatment with progestinTo stabilize the estrogen-stimulated endometrial growthInitial treatment strategyA very thin and denuded endometriumDiagnostic evaluation
-
Continued Estrogen Therapy..Episodic progesterone breakthrough bleeding1. Women with low-dose combination edtrogen-progestin contraceptives2. Depot progestin contraceptives.Insufficient endogenous estrogen to balance progestin effectsProgestin attenuates the endometriumInducing pseudoathropyThe light spotting, staining, or bleeding may occurEstrogen TherapyLogical and best choice.
-
ENDOMETRIAL HYPERTPLASIA AND NEOPLASIAEndometrial hyperplasia without atypia1. Regress spontaneously2. After curettage3. With progestin therapyIn contrast, Quite resistant curettage or prolongred high dose progestational therapyRisk 10 30 % progression to adenocarcinomaCyclic progestin therapy(medroxyprogesterone acetate 10 mg daily for 14 days orOral contraceptives.Hyperplasia with atypiaBest treated surgically.
-
ENDOMETRIAL ABLATIONPersistent bleeding despite treatmentBoth frustating and concerningHysterectomyEndometrial ablationHysteroscopic techniqueNon- hysteroscopy techniqueA bipolar vaporizing electrodeHydrothermal techniqueCirculates heated water (87 5 C) inside in ballonUsing electrodes on the outer surfaceAnd radiofrequency-induced thermal destructionResult better, if:1 Performed during the early follicular phase2. After endometrium is first attenuated for 4-6 weeks by progestin, danazol, GnRHaLower riskFewer complicationMore rapid recoveryMore satisfied with the outcome
-
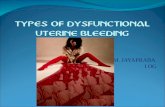
By definition, the anovulatory woman is always in the follicular phase of the ovarian cycle, and in the proliferative phase of the endometrial cycle. There is no luteal or secretory phase because there is no cycle. The only ovarian steroid signal the endometrium receives is estrogen. Epithel repair is focal, in the areas of breakdown, not universal; The results is a constantly changing patchwork of small repairs, instead of an organized and well structured remodeling.
-
Normal endometrium. (2) Sagittal transvaginal US scan of the uterus shows the menstrual-phase endometrium (arrowheads) (normal thickness, 1-4 mm). (3) Transverse transvaginal US scan shows the proliferative-phase endometrium (arrows) (normal thickness, 4-6 mm). (4) Sagittal transvaginal US scan obtained during the periovulatory phase (day 15) shows the trilaminar endometrium with a thickness of approximately 11 mm (arrows). (5) Sagittal transvaginal US scan shows the secretory-phase endometrium (cursors) (normal thickness, 8-16 mm).
-
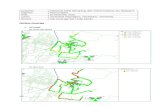
Figures 8, 9. (8) Polyp in a 47-year-old woman with excessive bleeding. (a) Sagittal transvaginal US scan shows the endometrium with a thickness of 15 mm. (b) Sagittal sonohysterogram shows a single polyp (arrowheads) with a catheter. The endometrium is normal. (9) Polyps in a 56-year-old woman. (a) Sagittal transvaginal US scan shows the endometrium with a thickness of 12 mm. (b) Sagittal sonohysterogram shows three polyps (P) with an otherwise thin (1-2-mm) endometrium.
-
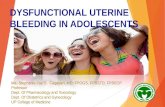
Endometrial carcinoma in a 51-year-old woman with a 4-week history of bleeding. (a) Sagittal transvaginal US scan shows the endometrium with a thickness of 23 mm. (b) Sagittal sonohysterogram shows diffuse thickening secondary to hyperplasia.
-
DIAGNOSTIC EVALUATION OF ABNORMAL BLEEDINGMENSTRUAL HISTORY:
Detail information regarding : 1. Intermenstrual intervals ( number of days, regularit). 2. Volume.(heavy, light, or variable). 3. Duration. (normal or prolonged, consistent or variable) 4. The onset abnormal menses.(perimenarcheal, sudden, gradual) 5. temporal associations (postcoital, postpartum, postpill, weight gain or loss) 6. Associated symptoms (premenstrual molimina, dysmenorrhea,dyspareunia, galactorrhea, hirsutism) 7. Underlying systemic illnesses (renal, hepatic, hematopoeitic, thyroid) 8. Medications.(hormonal, anticoagulants)
-
Regular monthly periods that are heavy or prolonged are more likely related to an anatomical lesion or bleeding disorder than to anovulation.
A sensitive pregnancy test can quickly exclude any realistic possibility that the bleeding related to an accident or complication of pregnancy.
A well-timed serum progesterone determination during what should be the luteal phase of the cycle can help to document ovulation or anovulation.
A serum thyroid-stimulating hormone (TSH) level can quickly exlude any associated thyroid disorders. In adolescents, suspicion of bleeding disorders is sufficient indication for screening coagulation study.
Endometrial hyperplasia and cancer are more commonly detected in older than in younger women, but duration of exposure to unopposed estrogen stimulation is the more critical risk factor.
-
A very thin endometrial stripe (< 5 mm), suggests an attenuated or denuded endometrium, best treated first with estrogen rather than progestin or estrogen-progestin combination.
In perimenopausal and postmenopausal women when the endometrial thickness is < 4-5 mm, endometrial biopsy is considered unnecessary, because the risk of endometrial hyperplasia or cancer is remote.
The biopsy is indicated when the clinical hystory suggests long-term unopposed estrogen exposure even when the endometrial thickness is normal (5-12 mm).ULTRASOUND :
-
EVALUATION TO STRONG EVIDENCE FOR ANATOMIC CAUSE :Regular monthly cycles with increasing volume or duration of bleeding.Regular monthly cycles complicated by intermenstrual bleeding in the absence of vaginal or cervical lesion.3. Abnormal bleeding despite objective evidence of ovulation from measurement of serum progesterone (>3 ng.ml) or from endometrial biopsy (secretory endometrium).4. Failed empirical medical management.
-
PROGESTIN THERAPY In most circumstances, progestin therapy will control anovulatory bleeding once uterine pathology has been excluded. In women who do not ovulate, cyclic progestin therapy restores the normal sequence of endometrial steroid hormone stimulation-estrogen, followed by estrogen plus progesterone, followed by withdrawal.
Mechanisms of progestin action in regimen progestin therapy:
Progestin stimulate 17-hydroxysteroid dehydrogenase and sulfotranferase activity, the enzymes that work in concert to convert estradiol to estrone sulfate (rapidly clear from the body). Progestin antagonize estrogen action by inhibiting estrogens induction of its own receptor Progestin also supress estrogen-mediated transcription of oncogen. Together, these action explain ANTIMITOTIC (prevention and reversal of hyperplasia, arrest growth of secretory phase of the cycle).
-
Self-limited progesterone withdrawal bleeding can be induced by cyclic treatment with an orally active progestin like : MEDROXYPROGESTERONE ACETATE ( 5-10 mg daily for 2 weeks every month ).
The interval therapy can be fixed to the calendaer beginning on the first of every month or to the onset of menses.
In women who likely still ovulate (albeit infrequently) or want to avoid pregnancy; an estrogen-progestin contraceptive is a better choice.
In anovulatory women with metrorrhagia or polymenorrhea : progestin tretment for 14 days can induce stabilizing predecidual changes in a vascular and fragile endometrium and, after withdrawal, so called medical curettage
Failed progestin treatment requires further diagnostic evaluation ????
Continued,.
-
ORAL CONTRACEPTIVE THERAPY : Prolonged episodes of heavy anovulatory bleeding and transvaginal ultrasound examination can confirm the diagnostic of uniformly increased endometrial thickness, usually are treated best with combined estrogen-progestin therapy in the form of combined oral contraceptive.
To respite from heavy bleeding that only recently stopped, oral contraceptive can be continued (one pill per day) until the package of pills is completed. In women wih normal uteri, oral contraceptive reduce menstrual flow by at least 60% from that in natural cycles.
Episodic breakthrough bleeding is relatively common and can be treated with estrogen
Mechanisms of action are :For the short term, the decidual changes induced by treatment, provide some structural stabilityand stop further random breakdown of an overgrown, vascular, and fragile endometrium, butsubstantial amount of tissue remains to be shed upon estrogen-progestin withdrawal.
-
ESTROGEN THERAPY : Endometrium is typically extremely thin with frankly low levels of estrogen stimulation frequently intermittent vaginal spotting (estrogen breakthrough bleeding ), also treatment with progestin, commonly failed and may further aggravate the problem. A similar situation can develop after prolonged episodes of heavy bleeding. In either case, estrogen therapy is most effective as initial treatment strategy. Under such circumstances, transvaginal ultrasound can help guide the choice of treatment by defining the endometrial thickness and revealing any abnormality of uterine cavity.
Estrogen therapy is also the logical and best choice for management of episodic progesterone breakthrough bleeding, that commonly occured in women receiving low-dose combination estrogen-progestin contraceptive, or depot progestin therapy. Progestin inducing pseudo atrophy. Symptom is similar likely ; light spotting, staining or bleeding that similar to the type of estrogen breakthrough bleeding with very low levels of circulating estrogen.
-
In all such cases, a short interval of added estrogen :
Conjugated estrogen 1,25 mg , or micronized estradiol 2,0 mg daily for 7 10 days)
If treatment failed, so..what ??????
Further evaluation can exclude possibilty of a previously unrecognized endometrial polyp, or sub mucous myoma Continued, ..
-
DILATATION AND CURETTAGE Dilatation and curettage is the most expeditious and effective way to stop acute uncontrolled uterine bleeding. Mechanisms of effects of curretage is not entirely clearbut Surgical denudation of basal layer of endometrium is presumed to acutely stimulate all of the normal processes involved in cessation of normal menstrual bleeding, likely ; 1. Local clotting mechanism 2. Vasoconstriction of basal arterioles 3. Rapid reepithelization.
-
NON SPECIFIC TREATMENTS FOR ABNORMAL MENSTRUAL BLEEDING A spesific cause for heavy or prolongrd menstrual bleeding in ovulatory women cannot always be identified; may be local defects in endometrial hemostasis are presumed responsible.
Nonsteroidal Antiinfflamatory Drugs (NSAIDs) :
The concentration of PGE2 and PGF 2 increase progresively in human endometrium during the menstrual cycle. NSAIDs inhibit PG synthesis and decrease menstrual blood loss. NSAIDs might be considered the first line therapy for ovulatory women with heavy menstrual bleeding and no demontrabel pathology. NSAIDs have the added advantage of providing relief from dysmenorrhea.
-
2. The Levonorgestrel IUD :
The LNG-IUD has a reservoir containing 52 mg LNG. Menstrual blood loss can be reduced by 75 95 % LNG-IUD is more effective than cyclic administration of norethindrone LNG_IUD is an atractive option for chronic ilness (renal failure).
-
ENDOMETRIAL ABLATION Indication : Persistent bleeding when medical treatment are rejected, unsuccessful, or poorly tolerated.
Hysteroscopic and non- hysteroscopic techniques Blind techniques for ablation are technically easier to perform, take less time, are more likely to require only local anesthesia, and achived similar results, but equipment problems are more common.
There are legitimate concerns that endometrial carcinomas might be advertantly treated by endometrial ablation, or procedure might obliterate portions of the uterine cavity Endometrial ablation is not recommended for women at high risk for endometrial cancer.
-
Microwave Endometrial Ablation (MEA)