DSM5& Development · ii. Failure&to ... •&Mixed&Anxiety/Depression&&...
7
3/07/13 1 American Psychiatric Associa5on DSM5 Development Towards DSM5 • Publica5on of the fi>h edi5on of Diagnos5c and Sta5s5cal Manual of Mental Disorders (DSM5) occurred in May 2013. • The review and revision process for DSM5 has taken 12 years. • Field trials were conducted in large academic seMngs and select clinical prac5ces around the world (2010 2012). American Psychiatric Associa5on DSM5 Development 1. General Issues in DSMV Development: 1.1 Classifica5on issues under discussion 1.2 CrossCuMng dimensional assessment in DSM5 1.3 Diagnoses proposed by outside sources 1.4 Defini5on of a Mental Disorder
Transcript of DSM5& Development · ii. Failure&to ... •&Mixed&Anxiety/Depression&&...

3/07/13
1
American Psychiatric Associa5on
DSM-‐5 Development
Towards DSM-‐5
• Publica5on of the fi>h edi5on of Diagnos5c and Sta5s5cal Manual of Mental Disorders (DSM-‐5) occurred in May 2013.
• The review and revision process for DSM-‐5 has taken 12 years. • Field trials were conducted in large academic seMngs and select
clinical prac5ces around the world (2010 -‐ 2012).
American Psychiatric Associa5on
DSM-‐5 Development
1. General Issues in DSM-‐V Development: 1.1 Classifica5on issues under discussion 1.2 Cross-‐CuMng dimensional assessment in DSM-‐5 1.3 Diagnoses proposed by outside sources 1.4 Defini5on of a Mental Disorder

3/07/13
2
American Psychiatric Associa5on
DSM-‐V Development • 1.3 Diagnoses proposed by outside sources
• Apathy Syndrome • Body Integrity Iden5ty Disorder • Complicated Grief Disorder • Developmental Trauma Disorder • Disorders of Extreme Stress Not Otherwise Specified • Foetal Alcohol Syndrome • Internet Addic5on • Male-‐to-‐Eunuch Gender Iden5ty Disorder • Melancholia • Parental Aliena5on Disorder • Seasonal Affec5ve Disorder • Sensory Processing Disorder
American Psychiatric Associa5on
DSM-‐5 Development
1. General Issues in DSM-‐V Development: 1.1 Classifica5on issues under discussion 1.2 Cross-‐CuMng dimensional assessment in DSM-‐5 1.3 Diagnoses proposed by outside sources 1.4 DefiniDon of a Mental Disorder
American Psychiatric Associa5on
DSM-‐5 Development
1.4 Defini5on of a Mental Disorder Proposed Features of a Mental Disorder: A. A behavioural or psychological syndrome or paXern that occurs in an individual B. That reflects an underlying psychobiological dysfunc5on C. The consequences of which are clinically significant distress (e.g., a painful symptom) or disability (i.e., impairment in one or more important areas of func5oning) D. Must not be merely an expectable response to common stressors and losses (for example, the loss of a loved one) or a culturally sanc5oned response to a par5cular event (for example, trance states in religious rituals) E. That is not primarily a result of social deviance or conflicts with society
American Psychiatric Associa5on
DSM-‐5 Development Other Considera.ons:
F. That has diagnos5c validity on the basis of various diagnos5c validators (e.g., prognos5c significance, psychobiological disrup5on, response to treatment) G. That has clinical u5lity (for example, contributes to beXer conceptualiza5on of diagnoses, or to beXer assessment and treatment) H. No defini5on perfectly specifies precise boundaries for the concept of either “medical disorder” or "mental/psychiatric disorder” I. Diagnos5c validators and clinical u5lity should help differen5ate a disorder from diagnos5c “nearest neighbours” J. When considering whether to add a mental/psychiatric condi5on to the nomenclature, or delete a mental/psychiatric condi5on from the nomenclature, poten5al benefits (for example, provide beXer pa5ent care, s5mulate new research) should outweigh poten5al harms (for example, hurt par5cular individuals, be subject to misuse)
3/07/13
3
American Psychiatric Associa5on
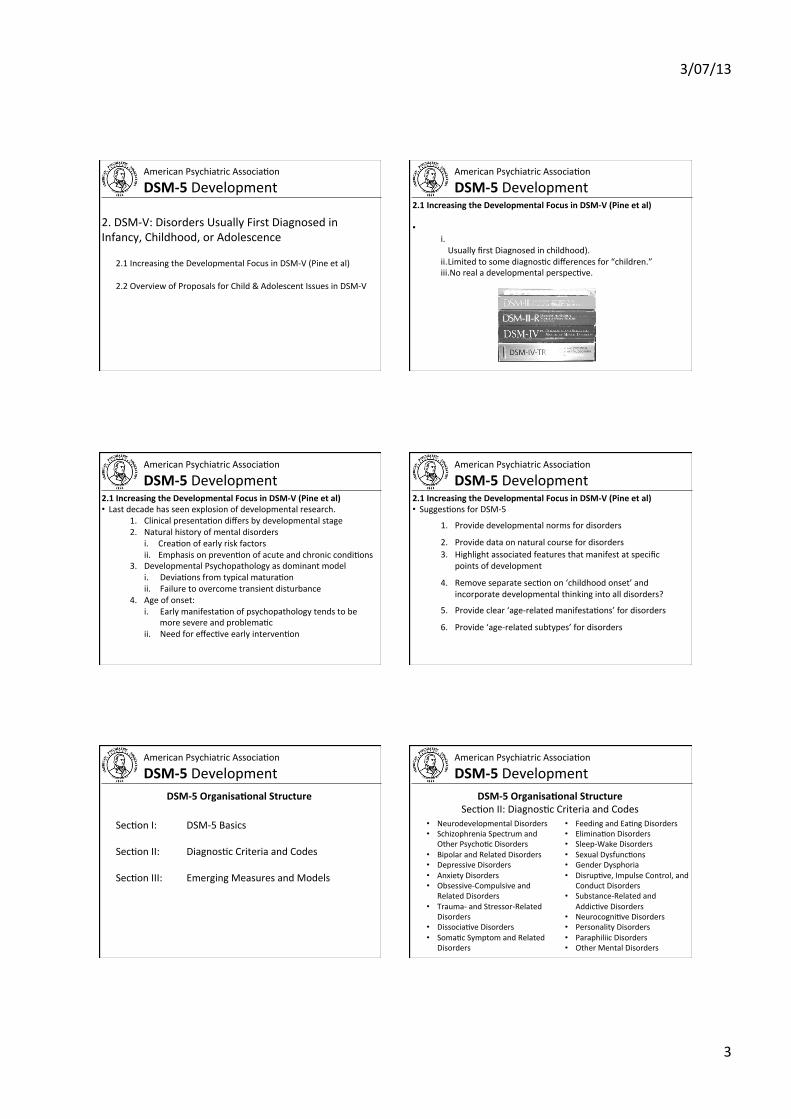
DSM-‐5 Development 2. DSM-‐V: Disorders Usually First Diagnosed in Infancy, Childhood, or Adolescence
2.1 Increasing the Developmental Focus in DSM-‐V (Pine et al)
2.2 Overview of Proposals for Child & Adolescent Issues in DSM-‐V
American Psychiatric Associa5on
DSM-‐5 Development 2.1 Increasing the Developmental Focus in DSM-‐V (Pine et al) • DSM-‐III, DSM-‐III-‐R and DSM-‐IV have limited developmental focus.
i. Limited to age of onset (thus producing chapter on Disorders Usually first Diagnosed in childhood).
ii. Limited to some diagnos5c differences for “children.” iii. No real a developmental perspec5ve.
American Psychiatric Associa5on
DSM-‐5 Development 2.1 Increasing the Developmental Focus in DSM-‐V (Pine et al) • Last decade has seen explosion of developmental research.
1. Clinical presenta5on differs by developmental stage 2. Natural history of mental disorders
i. Crea5on of early risk factors ii. Emphasis on preven5on of acute and chronic condi5ons
3. Developmental Psychopathology as dominant model i. Devia5ons from typical matura5on ii. Failure to overcome transient disturbance
4. Age of onset: i. Early manifesta5on of psychopathology tends to be
more severe and problema5c ii. Need for effec5ve early interven5on
American Psychiatric Associa5on
DSM-‐5 Development 2.1 Increasing the Developmental Focus in DSM-‐V (Pine et al) • Sugges5ons for DSM-‐5
1. Provide developmental norms for disorders
2. Provide data on natural course for disorders 3. Highlight associated features that manifest at specific
points of development
4. Remove separate sec5on on ‘childhood onset’ and incorporate developmental thinking into all disorders?
5. Provide clear ‘age-‐related manifesta5ons’ for disorders
6. Provide ‘age-‐related subtypes’ for disorders
American Psychiatric Associa5on
DSM-‐5 Development
Sec5on I: DSM-‐5 Basics Sec5on II: Diagnos5c Criteria and Codes Sec5on III: Emerging Measures and Models
DSM-‐5 OrganisaDonal Structure
American Psychiatric Associa5on
DSM-‐5 Development
• Neurodevelopmental Disorders • Schizophrenia Spectrum and
Other Psycho5c Disorders • Bipolar and Related Disorders • Depressive Disorders • Anxiety Disorders • Obsessive-‐Compulsive and
Related Disorders • Trauma-‐ and Stressor-‐Related
Disorders • Dissocia5ve Disorders • Soma5c Symptom and Related
Disorders
• Feeding and Ea5ng Disorders • Elimina5on Disorders • Sleep-‐Wake Disorders • Sexual Dysfunc5ons • Gender Dysphoria • Disrup5ve, Impulse Control, and
Conduct Disorders • Substance-‐Related and
Addic5ve Disorders • Neurocogni5ve Disorders • Personality Disorders • Paraphiliic Disorders • Other Mental Disorders
DSM-‐5 OrganisaDonal Structure Sec5on II: Diagnos5c Criteria and Codes

3/07/13
4
American Psychiatric Associa5on
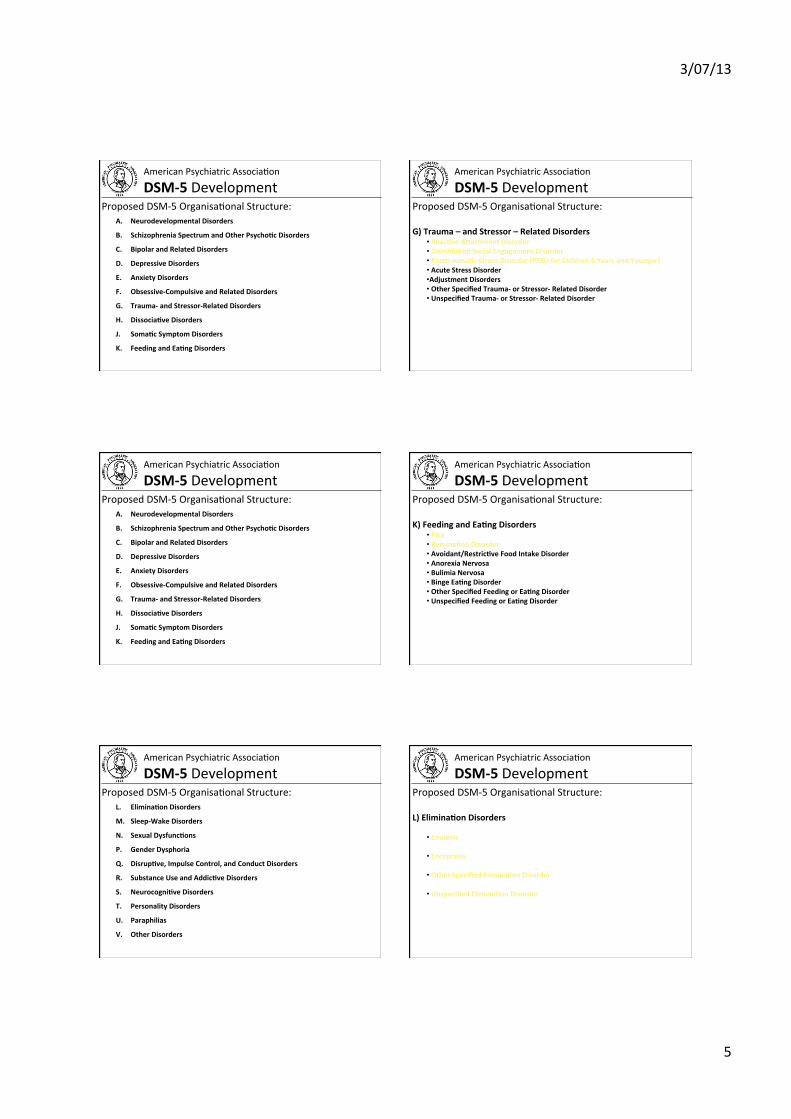
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure:
A. Neurodevelopmental Disorders
B. Schizophrenia Spectrum and Other PsychoDc Disorders
C. Bipolar and Related Disorders
D. Depressive Disorders
E. Anxiety Disorders
F. Obsessive-‐Compulsive and Related Disorders
G. Trauma-‐ and Stressor-‐Related Disorders
H. DissociaDve Disorders
J. SomaDc Symptom Disorders
K. Feeding and EaDng Disorders
American Psychiatric Associa5on
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure: A) Neurodevelopmental Disorders
• Intellectual DisabiliDes
• CommunicaDon Disorders
• AuDsm Spectrum Disorder
• AXenDon Deficit/HyperacDvity Disorder
• Specific Learning Disorder
• Motor Disorders
• Other Neurodevelopmental Disorders
American Psychiatric Associa5on
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure:
A. Neurodevelopmental Disorders
B. Schizophrenia Spectrum and Other PsychoDc Disorders
C. Bipolar and Related Disorders
D. Depressive Disorders
E. Anxiety Disorders
F. Obsessive-‐Compulsive and Related Disorders
G. Trauma-‐ and Stressor-‐Related Disorders
H. DissociaDve Disorders
J. SomaDc Symptom Disorders
K. Feeding and EaDng Disorders
American Psychiatric Associa5on
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure: D) Depressive Disorders
• DisrupDve Mood DysregulaDon Disorder • Major Depressive Disorder, Single Episode • Major Depressive Disorder, Recurrent • Chronic Depressive Disorder (Dysthymia) • Premenstrual Dysphoric Disorder • Mixed Anxiety/Depression • Substance-‐Induced Depressive Disorder • Depressive Disorder Associated with a Known General Medical CondiDon • Other Specified Depressive Disorder • Unspecified Depressive Disorder
American Psychiatric Associa5on
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure:
A. Neurodevelopmental Disorders
B. Schizophrenia Spectrum and Other PsychoDc Disorders
C. Bipolar and Related Disorders
D. Depressive Disorders
E. Anxiety Disorders
F. Obsessive-‐Compulsive and Related Disorders
G. Trauma-‐ and Stressor-‐Related Disorders
H. DissociaDve Disorders
J. SomaDc Symptom Disorders
K. Feeding and EaDng Disorders
American Psychiatric Associa5on
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure: E) Anxiety Disorders
• SeparaDon Anxiety Disorder • Panic disorder • Agoraphobia • Specific Phobia • Social Anxiety Disorder (Social Phobia) • Generalized Anxiety Disorder • Substance-‐Induced Anxiety Disorder • Anxiety Disorder associated with a Known General Medical CondiDon • Other Specified Anxiety Disorder • Unspecified Anxiety Disorder
3/07/13
5
American Psychiatric Associa5on
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure:
A. Neurodevelopmental Disorders
B. Schizophrenia Spectrum and Other PsychoDc Disorders
C. Bipolar and Related Disorders
D. Depressive Disorders
E. Anxiety Disorders
F. Obsessive-‐Compulsive and Related Disorders
G. Trauma-‐ and Stressor-‐Related Disorders
H. DissociaDve Disorders
J. SomaDc Symptom Disorders
K. Feeding and EaDng Disorders
American Psychiatric Associa5on
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure: G) Trauma – and Stressor – Related Disorders
• ReacDve AXachment Disorder • Disinhibited Social Engagement Disorder • PosXraumaDc Stress Disorder (PTSD for Children 6 Years and Younger) • Acute Stress Disorder • Adjustment Disorders • Other Specified Trauma-‐ or Stressor-‐ Related Disorder • Unspecified Trauma-‐ or Stressor-‐ Related Disorder
American Psychiatric Associa5on
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure:
A. Neurodevelopmental Disorders
B. Schizophrenia Spectrum and Other PsychoDc Disorders
C. Bipolar and Related Disorders
D. Depressive Disorders
E. Anxiety Disorders
F. Obsessive-‐Compulsive and Related Disorders
G. Trauma-‐ and Stressor-‐Related Disorders
H. DissociaDve Disorders
J. SomaDc Symptom Disorders
K. Feeding and EaDng Disorders
American Psychiatric Associa5on
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure: K) Feeding and EaDng Disorders
• Pica • RuminaDon Disorder • Avoidant/RestricDve Food Intake Disorder • Anorexia Nervosa • Bulimia Nervosa • Binge EaDng Disorder • Other Specified Feeding or EaDng Disorder • Unspecified Feeding or EaDng Disorder
American Psychiatric Associa5on
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure:
L. EliminaDon Disorders
M. Sleep-‐Wake Disorders
N. Sexual DysfuncDons
P. Gender Dysphoria
Q. DisrupDve, Impulse Control, and Conduct Disorders
R. Substance Use and AddicDve Disorders
S. NeurocogniDve Disorders
T. Personality Disorders
U. Paraphilias
V. Other Disorders
American Psychiatric Associa5on
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure: L) EliminaDon Disorders
• Enuresis
• Encopresis
• Other Specified EliminaDon Disorder
• Unspecified EliminaDon Disorder

3/07/13
6
American Psychiatric Associa5on
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure:
L. EliminaDon Disorders
M. Sleep-‐Wake Disorders
N. Sexual DysfuncDons
P. Gender Dysphoria
Q. DisrupDve, Impulse Control, and Conduct Disorders
R. Substance Use and AddicDve Disorders
S. NeurocogniDve Disorders
T. Personality Disorders
U. Paraphilias
V. Other Disorders
American Psychiatric Associa5on
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure: Q) DisrupDve, Impulse Control, and Conduct Disorders
• OpposiDonal Defiant Disorder • IntermiXent Explosive Disorder • Conduct Disorder (Specify if with Limited Prosocial EmoDons) • AnDsocial Personality Disorder • Pyromania • Kleptomania • Other Specified DisrupDve or Impulse Control Disorder • Unspecified DisrupDve or Impulse Control Disorder
American Psychiatric Associa5on
DSM-‐5 Development Proposed DSM-‐5 Organisa5onal Structure:
L. EliminaDon Disorders
M. Sleep-‐Wake Disorders
N. Sexual DysfuncDons
P. Gender Dysphoria
Q. DisrupDve, Impulse Control, and Conduct Disorders
R. Substance Use and AddicDve Disorders
S. NeurocogniDve Disorders
T. Personality Disorders
U. Paraphilias
V. Other Mental Disorders
American Psychiatric Associa5on
DSM-‐5 Development
• Assessment Measures • Cultural FormulaDon • Alternate DSM-‐5 Model for Personality Disorders • CondiDons for Further Study
• AXenuated Psychosis Syndrome • Depressive Episodes with Short-‐DuraDon Hypomania • Persistent Complex Bereavement Disorder • Caffeine Use Disorder • Internet Gaming Disorder • Neurobehavioral Disorder Associated with Parental Alcohol Exposure • Suicidal Behaviour Disorder • Nonsuicidal Self Injury
DSM-‐5 OrganisaDonal Structure Sec5on III: Emerging Measures and Models
American Psychiatric Associa5on
DSM-‐5 Development DSM-‐5 AuDsm Spectrum Disorder
Must meet criteria A,B,C and D: A. Persistent deficits in social communicaDon and social interacDon across contexts, as manifested by the following, currently or by history:
1. Deficits in social-‐emoDonal reciprocity; ranging from abnormal social approach and failure of normal back and forth conversa5on through reduced sharing of interests, emo5ons or affect, to failure to ini5ate or respond to social interac5ons. 2. Deficits in nonverbal communicaDve behaviours used for social interacDon; ranging from poorly integrated-‐ verbal and nonverbal communica5on, through abnormali5es in eye contact and body-‐language, or deficits in understanding and use of gestures, to total lack of facial expression and nonverbal communica5on. 3. Deficits in developing, maintaining and understanding relaDonships; ranging from difficul5es adjus5ng behaviour to suit different social contexts through difficul5es in sharing imagina5ve play and in making friends to an apparent absence of interest in peers.

3/07/13
7
B. Restricted, repeDDve paXerns of behaviour, interests, or acDviDes as manifested by at least two of the following, currently or by history:
1. Stereotyped or repeDDve motor movements, use of objects, or speech; (such as simple motor stereotypies, lining up toys or flipping objects, echolalia, or idiosyncra5c phrases).
2. Insistence on sameness, inflexible adherence to rouDnes, or ritualized paXerns of verbal or nonverbal behaviour; (extreme distress at small changes, difficul5es with transi5ons, rigid thinking paXerns, gree5ng rituals, need to take same route or eat same food ever day).
B. Restricted, repeDDve paXerns of behaviour, interests, or acDviDes as manifested by at least two of the following:
3. Highly restricted, fixated interests that are abnormal in intensity or focus; (such as strong aXachment to or preoccupa5on with unusual objects, excessively circumscribed or persevera5ve interests). 4. Hyper-‐or hypo-‐reacDvity to sensory input or unusual interest in sensory aspects of environment; (such as apparent indifference to pain/temperature adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascina5on with lights or movement).
C. Symptoms must be present in early childhood (but may not become fully manifest un5l social demands exceed limited capaci5es, or may be masked by learned strategies in later life). D. Symptoms together cause clinically significant impairment in social, occupaDonal, or other important areas of funcDoning.
Towards the Future
DSM-‐5 Proposal for AuDsm Spectrum Disorder (2)
ASD Severity Level Social CommunicaDon Restricted interests & RepeDDve behaviours
Level 3 ‘Requiring very substan5al support’
Severe deficits in verbal and nonverbal social communica5on skills cause severe impairments in func5oning; very limited ini5a5on of social interac5ons and minimal response to social overtures from others.
Preoccupa5ons, fixated rituals and/or repe55ve behaviours markedly interfere with func5oning in all spheres. Marked distress when rituals or rou5nes are interrupted; very difficult to redirect from fixated interest or returns to it quickly.
Level 2 ‘Requiring substan5al support’
Marked deficits in verbal and nonverbal social communica5on skills; social impairments apparent even with supports in place; limited ini5a5on of social interac5ons and reduced or abnormal response to social overtures from others.
RRBs and/or preoccupa5ons or fixated interests appear frequently enough to be obvious to the casual observer and interfere with func5oning in a variety of contexts. Distress or frustra5on is apparent when RRB’s are interrupted; difficult to redirect from fixated interest.
Level 1 ‘Requiring support’
Without supports in place, deficits in social communica5on cause no5ceable impairments. Has difficulty ini5a5ng social interac5ons and demonstrates clear examples of atypical or unsuccessful responses to social overtures of others. May appear to have decreased interest in social interac5ons.
Rituals and repe55ve behaviours (RRB’s) cause significant interference with func5oning in one or more contexts. Resists aXempts by others to interrupt RRB’s or to be redirected from fixated interest.
DSM-‐5 Social CommunicaDon Disorder A. Persistent difficulDes in the social use of verbal and nonverbal communicaDon as manifested by all of the following:
1. Deficits in using communica5on for social purposes, such as gree5ng and sharing informa5on, in a manner that is appropriate for the social context.
2. Impairment of the ability to change communica5on to match context or the needs of listener, such as speaking differently in a classroom than on a playground, talking differently to a child than to an adult, and avoiding use of overly formal language.
3. Difficul5es following rules for conversa5on and storytelling, such as taking turns in conversa5on, rephrasing when misunderstood, and knowing how to use verbal and nonverbal signals to regulate interac5on.
4. Difficul5es understanding what is not explicitly stated (e.g., making inferences) and nonliteral or ambiguous meanings of language (e.g., idioms, humor, metaphors, mul5ple meanings that depend on the context for interpreta5on).
DSM-‐5 Social CommunicaDon Disorder A. Persistent difficulDes in the social use of verbal and nonverbal communicaDon as manifested by all of the following:
B. The deficits result in func5onal limita5ons in effec5ve communica5on, social par5cipa5on, social rela5onships, academic achievement, or occupa5onal performance, individually or in combina5on.
C. The onset of symptoms is in the early developmental period (but deficits may not become fully manifest un5l social communica5on demands exceed limited capaci5es).
D. The symptoms are not aXributable to another medical or neurological condi5on or to low abili5es in the domains of word structure and grammar, and are not beXer explained by ASD, ID, GDD, or another mental disorder).
American Psychiatric Associa5on
DSM-‐5 Development
Ques5on & Answer Session