Drugs and the kidney
71
Drugs and the Kidney www.freelivedoctor.com
description
Transcript of Drugs and the kidney

Drugs and the Kidney
www.freelivedoctor.com

Drugs and the Kidney
1 Renal Physiology and Pharmacokinetics
2 Drugs and the normal kidney
3 Drugs toxic to the kidney
4 Prescribing in kidney disease
www.freelivedoctor.com

Normal Kidney Function
• 1 Extra Cellular Fluid Volume control• 2 Electrolyte balance• 3 Waste product excretion• 4 Drug and hormone elimination/metabolism• 5 Blood pressure regulation• 6 Regulation of haematocrit• 7 regulation of calcium/phosphate balance
(vitamin D3 metabolism)
www.freelivedoctor.com

Clinical Estimation of renal function
• Clinical examinationpallor, volume status, blood pressure measurement, urinalysis
• Blood tests• Routine Tests• haemoglobin level• electrolyte measurement (Na ,K , Ca, PO4)• urea• creatinine normal range 70 to 140 μmol/l
www.freelivedoctor.com

Serum Creatinine and GFR
• Muscle metabolite - concentration proportional to muscle mass– High: muscular young men– Low: conditions with muscle wasting
• elderly• muscular dystrophy• Anorexia• malignancy
• “Normal” range 70 to 140 μmol/litrewww.freelivedoctor.com

Serum Creatinine and GFR
Seru
m
creatinin
e
Glomerular filtration rate (GFR)
www.freelivedoctor.com

GFR Estimation
• Cockroft-Gault FormulaCrCl=Fx(140-age)xweight/CreaP
F♀=1.04F♂=1.23Example85♀, 55kg, Creatinine=95CrCl=33ml/min
• MDRD Formula
www.freelivedoctor.com

Tests of renal function cont.
• 24h Urine sample-Creatinine clearance
• chromium EDTA Clearance
• gold standard Inulin clearance
www.freelivedoctor.com

Na+ 60%K+
2%
Na+ -K+, H+
Liddle’s syndromePseudohypoaldosteronismtype-IAmiloride sensitive
1%
Na+-Cl-
Gitelman's syndromeThiazide sensitive
7%
30%
Na-K-2ClROMKBartter's syndromeBumetanidesensitive
The nephron and electrolyte handling
www.freelivedoctor.com

www.freelivedoctor.com

Pharmacokinetics
• Absorption
• Distribution
• Metabolism
• Elimination– filtration– secretion
www.freelivedoctor.com

Diuretics
• Loop
• Thiazide
• Aldosterone antagonist
• Osmotic
www.freelivedoctor.com

Diuretics
• Indications for use– heart failure ( acute or chronic )
– pulmonary oedema
– hypertension
– nephrotic syndrome
– hypercalcaemia
– hypercalciuria
www.freelivedoctor.com

Loop diuretics
Frusemide, BumetanideIndication
– Fluid overload– Hypertension– Hypercalcaemia
Mechanism of actionBlockade of NaK2Cl (NKCC2) transporter in the thick ascending loop of Henle
www.freelivedoctor.com

www.freelivedoctor.com

Loop diuretics
• Frusemide– oral bioavailability between 10 and 90%– Acts at luminal side of thick ascending
limb(NaK2Cl transporter)– Highly protein bound– Rebound after single dose– Half-life 4 hours
www.freelivedoctor.com

Loop diuretics continued
• Caution– Electrolyte imbalance - hypokalaemia– Volume depletion (prerenal uremia)– Tinitus (acts within cochlea – can synergise
with aminoglycoside antibiotics)
www.freelivedoctor.com

Thiazide diuretics
Bendrofluazide, Metolazone
Site of action distal convoluted tubule
blocks electroneutral Na/Cl exchanger (NCCT)
Reaches site of action in glomerular filtrate– Higher doses required in low GFR
(ineffective when serum creatinine >200μM)
– T ½ 3-5 hours
www.freelivedoctor.com

www.freelivedoctor.com

Thiazides
• Indications– Antihypertensive: especially in combination
with ACE inhibitor/ARB (A+D)– In combination with loop diuretic for profound
oedema– Cautions
• Metabolic side effects – hyperuricaemia, impaired glucose tolerance & electrolyte disturbance (hypokalaemia and hyponatraemia)
• Volume depletion
www.freelivedoctor.com

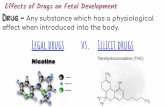
Major Outcomes in High Risk Hypertensive Patients Randomized to
Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs
DiureticThe Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial
(ALLHAT)The ALLHAT Collaborative Research Group
Sponsored by the National Heart, Lung, and Blood Institute (NHLBI)www.freelivedoctor.com

Years to CHD Event0 1 2 3 4 5 6 7
Cum
ula
tive
CH
D E
vent
Rat
e
0
.04
.08
.12
.16
.2
Number at Risk: Chlorthalidone 15,255 14,477 13,820 13,102 11,362 6,340 2,956 209 Amlodipine 9,048 8,576 8,218 7,843 6,824 3,870 1,878 215 Lisinopril 9,054 8,535 8,123 7,711 6,662 3,832 1,770 195
Cumulative Event Rates for the Primary Outcome (Fatal CHD or Nonfatal MI) by ALLHAT Treatment Group
RR (95% CI) p value
A/C 0.98 (0.90-1.07) 0.65
L/C 0.99 (0.91-1.08) 0.81
ChlorthalidoneAmlodipineLisinopril
www.freelivedoctor.com

Overall Conclusions
Because of the superiority of thiazide-type diuretics in preventing one or more major forms of CVD and their lower cost, they should be the drugs of choice for first-step antihypertensive drug therapy.
www.freelivedoctor.com

Amiloride and Spironolactone
• Amiloride – Blocks ENaC (channel for Na secretion in
collecting duct under aldosterone control)• Spironolactone
– Aldosterone receptor antagonist – Reaches DCT via blood stream (not
dependent on GFR)• Often Combined with loop or thiazides to
capitalise on K-sparing action
www.freelivedoctor.com

www.freelivedoctor.com

Nephrotoxic Drugs
• Dose dependant toxicity– NSAIDs including COX 2– Aminoglycosides– Radio opaque contrast materials
• Idiosyncratic Renal Damage– NSAIDs– Penicillins– Gold, penicillamine
www.freelivedoctor.com

NSAIDs (Non-steroidal anti inflammatory drugs)
• Commonly used– Interfere with prostaglandin production,
disrupt regulation of renal medullary blood flow and salt water balance
• Chronic renal impairment– Habitual use– Exacerbated by other drugs ( anti-
hypertensives, ACE inhibitors)– Typical radiological features when advanced
www.freelivedoctor.com

www.freelivedoctor.com

Aminoglycosides
• Highly effective antimicrobials– Particularly useful in gram -ve sepsis– bactericidal
• BUT– Nephrotoxic – Ototoxic – Narrow therapeutic range
www.freelivedoctor.com

Prescribing Aminoglycosides
• Once daily regimen now recommended in patients with normal kidneys
– High peak concentration enhances efficacy
– long post dose effect– Single daily dose less nephrotoxic
• Dose depends on size and renal function– Measure levels!
www.freelivedoctor.com

Intravenous contrast• Used commonly
– CT scanning, IV urography, Angiography– Unsafe in patients with pre-existing renal impairment– Risk increased in diabetic nephropathy, heart failure
& dehydration– Can precipitate end-stage renal failure– Cumulative effect on repeated administration
• Risk reduced by using Acetylcysteine ?– see N Engl J Med 2000; 343:180-184
www.freelivedoctor.com

Prescribing in Kidney Disease
• Patients with renal impairment
• Patients on Dialysis
• Patients with renal transplants
www.freelivedoctor.com

Principles
• Establish type of kidney disease• Most patients with kidney failure will already be
taking a number of drugs • Interactions are common• Care needed to avoid drug toxicity
• Patients with renal impairment and renal failure
• Antihypertensives• Phosphate binders
www.freelivedoctor.com

Dosing in renal impairment
• Loading dose does not change (usually)• Maintenance dose or dosing interval does
T ½ often prolonged– Reduce dose OR– Increase dosing interval
– Some drugs have active metabolites that are themselves excreted renally
– Warfarin, diazepam
www.freelivedoctor.com

Spironolactone
• Class• Potassium sparing diuretic
• Mode of action• Antagonises the effect of aldosterone at levels MR• Mineralocorticoid receptor (MR)–aldosterone complex
translocates to nucleus to affect gene transcription
• Indication• Prevent hypokalaemia in patients taking diuretics or digoxin• Improves survival in advanced heart failure (RALES 1999
Randomised Aldactone Evaluation Study)• Antihypertensive (adjunctive third line therapy for
hypertension or first line for conns patients)• Ascites in patients with cirrhosis
www.freelivedoctor.com

Spironolactone
• Side effects– Antiandrogenic effects through the antagonism of DHT
(testosterone) at its binding site. – Gynaecomastia, impotence, reduced libido
• Interactions– Other potassium sparing drugs e.g. ACE inhibitors/ARBs
& potassium supplements (remember ‘LoSalt’ used as NaCl substitute in cooking)
www.freelivedoctor.com

Amphotericin
• Class• Anti fungal agent for topical and systemic use
• Mode of action• Lipid soluble drug. Binds steroid alcohols
(ergosterol) in the fungal cell membrane causing leakage of cellular content and death. Effective against candida species
• Fungistatic or fungicidal depending on the concentration
• Broad spectrum (candida, cryptosporidium)
www.freelivedoctor.com

Amphotericin• Indications
– iv administration for systemic invasive fungal infections– Oral for GI mycosis
• Side effects– Local/systemic effects with infusion (fever)– Chronic kidney dysfunction
» Decline in GFR with prolonged use» Tubular dysfunction (membrane permeability)» Hypokalaemia, renal tubular acidosis (bicarb wasting
type 1/distal), diabetes insipidus, hypomagnesaemia» Pre hydration/saline loading may avoid problems
Toxicity can be reduced substantially by liposomal packing of Amphotericin
www.freelivedoctor.com

Lithium toxicity
• Lithium carbonate - Rx for bipolar affective disorder
• Toxicity closely related to serum levels• Symptoms
– CVS arrhythmias (especially junctional dysrrythmias)– CNS tremor – confusion - coma
• Treatment• Supportive - Haemodialysis and colonic irrigation for severe
levels• Inadvertent intoxication from interaction with ACEI &
loop/thiazide diuretic• Carbamezepine and other anti epileptics increase
neurotoxicity
www.freelivedoctor.com

Digoxin toxicity
• Incidence – High levels demonstrated in 10% and toxicity
reported in 4% of a series of 4000 digoxin samples
• Kinetics – large volume of distribution (reservoir is skeletal
muscle)– about 30% of stores excreted in urine/day
www.freelivedoctor.com

Treatment of digoxin toxicity
• Supportive– Correction of electrolyte imbalances– Atropine for bradycardia avoid cardio stimulants because
arrythmogenic
• Limitation of absorption– Charcoal effective within 8 hours (or cholestyramine)
• Specific measures– DIGIBIND Fab digoxin specific antibodies. Binds plasma
digoxin and complex eliminated by kidneys (used when OD is high/near arrest)
• Enhanced elimination– Dialysis is ineffective. Charcoal/cholestyramine interrupt
enterohepatic cycling.
www.freelivedoctor.com

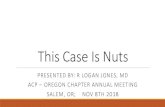
From Knauf & Mutschler Klin. Wochenschr. 1991 69:239-250
70%
20%
5%
4.5%
0.5%Volume 1.5 L/dayUrine Na 100 mEq/LNa Excretion 155 mEq/day
100%GFR 180 L/day Plasma Na 145 mEq/LFiltered Load 26,100 mEq/day
CA InhibitorsProximal tubule
Loop DiureticsLoop of Henle
ThiazidesDistal tubule
Antikaliuretics
Collecting duct
Thick Ascending Limb
www.freelivedoctor.com

Principles important for understanding effects of diuretics
• Interference with Na+ reabsorption at one nephron site interferes with other renal functions linked to it
• It also leads to increased Na+ reabsorption at other sites
• Increased flow and Na+ delivery to distal nephron stimulates K + (and H +) secretion
www.freelivedoctor.com

• Diuretics act only if Na+ reaches their site of action. The magnitude of the diuretic effect depends on the amount of Na+ reaching that site
• Diuretic actions at different nephron sites can produce synergism
• All, except spironolactone, act from the lumenal side of the tubular cellular membrane
Principles important for understanding effects of diuretics
www.freelivedoctor.com

N NSO2
NH2
SO2NH2NH2
NH2
NH2
SO2NH2Cl
Cl
SO2NH2
SO2NH2
Cl
SO2NH2
N C
N
SO2
Prontosil
Sulfanilamide
p-chlorobenzene sulfonamide
1,3 disulfonamide 6 cholrobenzene
Cholrothiazide www.freelivedoctor.com

THIAZIDE DIURETICS
• Secreted into the tubular lumen by the organic acid transport mechanisms in the proximal tubule
• Act on the distal tubule to inhibit sodium and chloride transport and result in a modest diuresis
• Increase renal excretion of potassium, magnesium• Reduce calcium and urate excretion• Not effective at low glomerular filtration rates• Impair maximal diluting but not maximal concentrating
ability
www.freelivedoctor.com

General Structure of Thiazide Diureticswww.freelivedoctor.com

Ion % Control
NaF 143±9
LiCl 4±1
NaCl 20±0.5
KCl 44±2
Choline chloride 36±7
NaBr 24±2
NaI 25±1
KI 12±2
Na acetate 82±5
K acetate 95±5
Disodium sulfate 152±22
Dipotassium sulfate 118±12
Trisodium citrate 112±5
Inhibition of high-affinity 3H-metolazone binding by ions
www.freelivedoctor.com

Correlation of the daily clinical doses of thiazide diuretics with their affinity for high-affinity 3H-metolazone binding sites in rat kidney. Correlation coefficient r=0.7513.
www.freelivedoctor.com

Thiazides - Pharmacokinetics
• Rapid GI absorption• Distribution in extracellular space• Elimination unchanged in kidney• Variable elimination kinetics and therefore
variable half-lives of elimination ranging from hours to days.
www.freelivedoctor.com

CLINICAL USES Of THIAZIDES-1
1) HYPERTENSION
• Thiazides reduce blood pressure and associated risk of CVA and MI in hypertension
• they should be considered first-line therapy in hypertension (effective, safe and cheap)
• Mechanism of action in hypertension is uncertain – involves vasodilation that is not a direct effect but a consequence of the diuretic/natriuretic effect
www.freelivedoctor.com

Schematic drawing of temporal changes in mean arterial pressure (MAP), total peripheral vascular resistance (TPR), cardiac output (CO) and plasma volume (PV) during thiazide treatment of a hypertensive subject
www.freelivedoctor.com

www.freelivedoctor.com

www.freelivedoctor.com

CLINICAL USES OF THIAZIDES-2
2) EDEMA (cardiac, liver renal)
3) IDIOPATHIC HYPERCALCIURIA• condition characterized by recurrent stone
formation in the kidneys due to excess calcium excretion
• thiazide diuretics used to prevent calcium loss and protect the kidneys
4) DIABETES INSIPIDUS
www.freelivedoctor.com

ADVERSE EFFECTS OF THIAZIDES-1
Initially, they were used at high doses which caused a high
incidence of adverse effects. Lower doses now used cause
fewer adverse effects. Among them are:• HYPOKALEMIA• DEHYDRATION (particularly in the elderly) leading to
POSTURAL HYPOTENSION• HYPERGLYCEMIA possibly because of impaired insulin
release secondary to hypokalemia• HYPERURICEMIA because thiazides compete with urate
for tubular secretion
www.freelivedoctor.com

ADVERSE EFFECTS OF THIAZIDES-2
• HYPERLIPIDEMIA; mechanism unknown but cholesterol increases usually trivial (1% increase)
• IMPOTENCE
• HYPONATREMIA due to thirst, sodium losloss, inappropriate ADH secretion (can cause confusion in the elderly), usually after prolonged use
www.freelivedoctor.com

Less common problems
• HYPERSENSITIVITY - may manifest as interstitial nephritis, pancreatitis, rashes, blood dyscrasias (all very rare)
• METABOLIC ALKALOSIS due to increased sodium load at the distal convoluted tubule which stimulates the sodium/hydrogen exchanger to reabsorb sodium and excrete hydrogen
• HYPERCALCEMIA
ADVERSE EFFECTS OF THIAZIDES-3
www.freelivedoctor.com

LOOP DIURETICS• Secreted in proximal tubule by acid mechanisms• Act on the ascending loop of Henle to inhibit
sodium and chloride transport• Cause a greater natriuresis than thiazides• Effective at low glomerular filtration rates (as occur
in chronic renal failure), where thiazides are ineffective
• Increase potassium, calcium and magnesium excretion
• Decrease urate excretion• Impair maximal concentrating and diluting capacity
www.freelivedoctor.com

www.freelivedoctor.com

LOOP DIURETICS
• Additional non-tubular effects1. Renal Vasodilation and
redistribution of blood flow2. Increase in renin release3. Increase in venous capacitance
These effects mediated by release of prostaglandins from the kidney.
www.freelivedoctor.com

www.freelivedoctor.com

Loop Diuretics - Pharmacokinetics
• Rapid GI absorption. Also given i.m. and i.v.
• Extensively protein bound in plasma
• Short half-lives in general
• Elimination: unchanged in kidney or by conjugation in the liver and secretion in bile.
www.freelivedoctor.com

www.freelivedoctor.com

CLINICAL USES OF LOOP DIURETICS
• EDEMA due to CHF, nephrotic syndrome or cirrhosis
• Acute heart failure with PULMONARY EDEMA
• HYPERCALCEMIA• not in widespread use for the treatment of
hypertension (except in a few special cases e.g. hypertension in renal disease)
www.freelivedoctor.com

• Hypokalemia, metabolic alkalosis, hypercholesterolemia, hyperuricemia, hyperglycemia, hyponatremia
• Dehydration and postural hypotension• Hypocalcemia (in contrast to thiazides)• Hypersensitivity• OTOTOXICITY (especially if given by rapid IV
bolus)
Adverse Effects of Loop Diuretics similar to thiazides in many respects
www.freelivedoctor.com

Edema: Therapeutic Considerations
• Therapy is palliative (except with pulmonary edema).
• Need a mild sustained response. • Specific consideration to potassium
homeostasis, i.e. supplement with K-salt or use K-sparing diuretic.
• Therefore, in most cases start with a thiazide.• If resistant, move to Loop diuretic.
www.freelivedoctor.com

www.freelivedoctor.com

Conditions treated with Diuretics
• Edema
• Hypertension
• Nephrogenic Diabetes Insipidus
• Syndrome of Inappropriate ADH Secretion (SIADH)
• To increase or decrease Ca++, K+ or H+ ion excretion.
www.freelivedoctor.com

Diuretic Resistance
1. Compensatory Mechanisms (RAAS, SNS)2. Failure to reach tubular site of action
a - Decreased G.I. absorptionb - Decreased secretion into tubular lumen (e.g. uremia, decreased kidney perfusion)c - Decreased availability in tubular lumen (e.g. nephrotic syndrome)
3. Interference by other drugs (e.g. NSAID’s)4. Tubular adaptation (chronic Loop diuretic use)
Can Use Combination of Diuretics to Induce a Synergistic Effect
www.freelivedoctor.com

Clinical Condition Dose of furosemide (mg)
intravenous Oral
Renal Insufficiency 0 < ClCr < 50 80 160
Renal Insufficiency ClCr < 20 200 400
Nephrotic Syndrome 120 240
Cirrhosis 40 80Congestive Heart
Failure 40-80 80-160
Maximum Doses of Loop Diuretics
www.freelivedoctor.com