
Drug Interactions - Table of contentsmembers.iif.hu/lakner/download/cikkek/kf/Drug... · Drug...
30
Drug Interactions - Table of contents Dr. Gé za Lakner Drug Interactions - Table of contents Preventable Drug-Related Morbidity (PDRM) Important principles for physicians to consider when prescribing any drug Adverse Drug Reactions (ADR) Adverse Drug Experience Postmarket ADE Reports by Top-10 Ranked Classes of Suspect Drugs (FDA, 1995) Barriers to Improved Monitoring and Reporting of ADEs Essential Antidote Medications Factors affecting serum drug concentration Classification of drug interactions Pharmaceutical interactions Pharmacokinetic Interactions #1/3 Interactions during the absorption phase Protein binding of drugs in human serum Competitive interaction for serum protein binding of clinical significance Pharmacokinetic Interactions #2/3 Frequent parties in drug interactions Role of metabolites CYP-450 system - Substrates Inducers of CYP Enzymes Inhibitors of CYP enzymes Environmental factors affecting the activity of the intestinal monooxigenase systems Drug - Nutrient Interactions Drug - Food Interaction of Grapefruit Juice Monogenic oxydative polymorphism drugs (template drug: debrisoquin) Pharmacogenetic enzyme variations of clinical significance Pharmacokinetic Interactions #3/3 Pharmacodynamic Interactions Drug interaction and renal function Interactions between defibrillators and drugs Factors to consider before prescribing non-sedating antihistamines (terfenadine and astemizole) Drug interactions of ACEIs Pharmacy and Therapeutics Committee Therapeutic Drug Monitoring (TDM) "Red Flag" List and Alternatives PDF created with FinePrint pdfFactory trial version http://www.fineprint.com
Transcript of Drug Interactions - Table of contentsmembers.iif.hu/lakner/download/cikkek/kf/Drug... · Drug...

Drug Interactions - Table of contents
Dr. Gé za Lakner
Drug Interactions - Table of contentsPreventable Drug-Related Morbidity (PDRM)Important principles for physicians to consider when prescribing any drugAdverse Drug Reactions (ADR)Adverse Drug ExperiencePostmarket ADE Reports by Top-10 Ranked Classes of Suspect Drugs (FDA, 1995)Barriers to Improved Monitoring and Reporting of ADEsEssential Antidote MedicationsFactors affecting serum drug concentrationClassification of drug interactionsPharmaceutical interactionsPharmacokinetic Interactions #1/3Interactions during the absorption phaseProtein binding of drugs in human serumCompetitive interaction for serum protein binding of clinical significancePharmacokinetic Interactions #2/3Frequent parties in drug interactionsRole of metabolitesCYP-450 system - SubstratesInducers of CYP EnzymesInhibitors of CYP enzymesEnvironmental factors affecting the activity of the intestinal monooxigenase systemsDrug - Nutrient InteractionsDrug - Food Interaction of Grapefruit JuiceMonogenic oxydative polymorphism drugs (template drug: debrisoquin)Pharmacogenetic enzyme variations of clinical significancePharmacokinetic Interactions #3/3Pharmacodynamic InteractionsDrug interaction and renal functionInteractions between defibrillators and drugsFactors to consider before prescribing non-sedating antihistamines (terfenadine and astemizole)Drug interactions of ACEIsPharmacy and Therapeutics CommitteeTherapeutic Drug Monitoring (TDM)"Red Flag" List and Alternatives
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Preventable Drug-Related Morbidity (PDRM)
• About 3.2% of all hospital admissions in the United States and Europemay be caused to a significant degree by preventable drug-relatedmorbidity (PDRM) in ambulatory care.
• This is the median incidence from seven well-designed studiesconducted between 1986 and 1996
• Incidentally, PDRM represents, on average, about one-half of allmedication-related hospital admissions.
Proximal causes of drug-related morbidity (DRM)• Inappropriate prescribing• Unexpected adverse drug reactions (ADRs)• Patient nonadherence• Overdose or underdose, either in general or for a specific patient• Lack of necessary pharmacotherapy• Failure to recognize symptoms, delay in response, inadequate follow-up
of clinical signs and symptoms• Medication errors
Main components of the strategy• Increase general awareness of the problem of PDRM.• Develop and disseminate a means for health care programs to identify
and assess medication use problems in their own population: developPDRM outcome indicators that could be used to screen populationdatabases
• Develop a means to improve systems found to be unsafe• develop new process indicators for medication use• adapt quality improvement (QI) concepts to use in clinic, hospital,
and community pharmacies• Improve standards for medication use - determine minimum standards
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Important principles for physicians to considerwhen prescribing any drug
• Document all treatments the patient is taking, including over-the-counter therapies (such as appetite suppressants, herbs, and the like).
• Understand the pharmacology of the drugs that you prescribe, includingtheir route of excretion, the type of liver metabolism if it exists, the half-life of the drug, and its bioavailability. The careful use of drugs alsorequires an understanding of the toxic-therapeutic ratio for the drug.
• Minimize the number of prescriptions you write if you can, thusavoiding the probability of drug--drug interactions.
• Be especially vigilant in high risk situations, especially therapy of theelderly, therapy of patients in an intensive care unit, or therapy ofpatients requiring multiple drugs or with co-existing illnesses such asrenal or hepatic impairment.
• If there is an unexpected deterioration or change in the patientcondition, consider drug--drug interactions, which usually present in asubtle manner.
Dr. Jean T. Barbey - 20th Annual Scientific Sessions of the North American Society of Pacing and ElectrophysiologyDay 2 - May 13, 1999
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Adverse Drug Reactions (ADR)
ADR = any unexpected, unintended, undesired, or excessive response to amedicine:• requires discontinuing the medicine (therapeutic or diagnostic),• requires changing the medication therapy,• requires modifying the dose (except for minor dosage adjustments),• necessitates admission to the hospital,• prolongs stay in a healthcare facility,• necessitates supportive treatment,• significantly complicates diagnosis,• negatively affects prognosis, or• results in temporary or permanent harm, disability, or deathAmerican Society of Health-System Pharmacists (ASHP)
• Dose-related reactions• side effect = expected adverse pharmacological effect occurring in the
therapeutic dose range• overdose toxicity = expected toxicity occurring at higher doses than
the therapeutic dose range• Not dose-related reactions
• allergy = changed organic reactivity against a drug molecule whichturned into an antigen upon previous exposition
• idiosyncrasy = unforeseen events unrelated to the pharmacologiceffects of the drug and are not allergic by their nature (e.g.myelotoxicity of chloramphenicol)
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Adverse Drug Experience
ADE = ADR + medication errors
Postmarket ADE Reports byTop-10 Ranked Classes ofSuspect Drugs (FDA, 1995)
Type N %All Suspect Drug Mentions 153,842100 100
Central nervous system agents 42,254 28Hormones & synthetic substitutes 21,173 14
Cardiovascular drugs 15,711 10Anti-infective agents 14,117 9Antineoplastic agents 10,191 7
Skin & mucous membrane agents 9,115 6Autonomic drugs 6,658 4
Gastrointestinal drugs 5,589 4Unclassified 5,436 4
Blood formation & coagulation 3,812 2
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Barriers to Improved Monitoring and Reporting of ADEs
• Fear of personal and organizational liability• Lack of resources for surveillance and reporting• Labor-intensive reporting processes• Ambiguity in interpreting whether the medication was the cause of the
adverse event• Minimal feedback provided to reporters• No incentives or rewards to report• Lack of distinction between significant ADEs and minor ones• Surveillance and reporting functions without a leader
Essential Antidote Medications
• N-Acetyl cysteine (Mucomyst)• Corticosteroid ointments/creams• Dextrose 50%• Digoxin immune Fab (Digibind)• Diphenhydramine (Benadryl)• Epinephrine• Hydrocortisone injection• Methylprednisolone (Medrol) Dosepak• Naloxone• Phytonadione (Vitamin K)• Protamine• Sodium polystyrene sulfonate (Kayexelate)
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Factors affecting serum drug concentration
• properties
• age
• gender
• body weight
• genetic potentials
• inductors
• nutrition
• environment
• conditions
• liver
• kidney
• cardiovascular
• pregnancy
• changes in serum proteins
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Classification of drug interactions
• according to the lifecycle of the drug• extracorporal
• pharmaceutical• intracorporal
• pharmacokinetic = ADME• Absorption• Distribution• Metabolism• Excretion
• pharmacodynamic• synergism , antagonism• additive, potentiating
• according to the playing parties• drug - environment
• drug - nutritient• drug - medical device• drug - drug
• drug - excipient
Pharmaceutical interactions
• potential physical interactions between drugs when they are mixed priorto administration
• intravenous incompatibilities, such as precipitation in a line when twoagents are administered together• drugs may bind to intravenous bags or tubing and
• may interfere with laboratory tests
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Pharmacokinetic Interactions #1/3
Alterations in Absorption• drugs of risk:
• large surface area (antacids)• ability to bind (resins)• ability to chelate (cations such as aluminum)• ability to alter gastrointestinal mobility (metoclopramide or narcotics)• ability to alter gastric pH (ketoconazole)
• management: separate the times of administration• classic examples
• tetracycline - chelated by dairy products• fluoroquinolones - chelated by divalent cations, antacids, iron,
sucralfate, and didanosine;these drugs must also be separated by at least 2 hours -important caveat: fluoroquinolone must be given first !
• drug-excipient interactions: can be actively used to the advantage of theformulator to increase the bioavailability of the druge.g. complexation with cyclodextrins or solid dispersion technology
Protein-Binding Effects• basic mechanism: drugs compete for protein- or tissue-binding sites;
when the drug is freed from a binding site, it may then effect anenhanced pharmacologic action
• drugs of risk• highly protein bound• narrow therapeutic index• occupy most of the available binding sites• small volume of distribution + long half-life• e.g. warfarin and cotrimoxazole, digoxin and quinidine.
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Interactions during the absorption phase
• Change in the GI tract pH
• barbitures - antacids
• warfarin - antacids
• salycylate - antacids
• Na-bicarbonate - tetracyclin
• Change in GI motility (gastric emptying and intestinal peristalsis)
• purgatives
• parasympatholytics
• parasympatholytics - L-DOPA
• antacids - L-DOPA
• griseofulvin - barbiturates
• antibiotics - food
• fat contents of food
• Chelating
• tetracyclin - metals
• cholestyramin
• obstipantia
• desferroxamine - iron
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Protein binding of drugs in human serum
Drug Free % Drug Free %AnticoagulantsWarfarin
Antibioticsdicloxacillincloxacillinoxacillindoxycyclinnafcillin
NSAIDphenoprofenphenylbutazonindomethacinsalycylate
Cardiovascularpropranololdiazoxiddigitoxinchinidin
3
2567
10
113
16
69
1011
CNSdiazepamamitryptilinimipraminchlorpromazinchlordiazepoxidnortryptilinphenytoinmethadonthiopental
OADtolbutamidchlorpropamidtolazamid
Kidneyprobenecidfurosemidchlorothiazidetacrinate
1444569
1313
146
135
10
Competitive interaction for serum protein bindingof clinical significance
Freed drug “ Attacking” drug Consequencewarfarin and otherstrongly protein-boundcoumarins
ClofibrateEtacrinateNalidixatePhenylbutazonTCA (metabolite of
chloralhydrate)
hypoprothrombonaemia,bleeding
Tolbutamid PhenylbutazonSalycylates
hypoglycaemia
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Pharmacokinetic Interactions #2/3
Changes in Drug Metabolism• Cytochrome P-450 (CYP) isoenzymes are important for oxidative
metabolism in the liver• Extrahepatic isoenzymes: small intestine, kidneys, lungs, and brain• More than 30 CYP isoenzymes have been identified• Most commonly involved in drug metabolism are 3A4, 2D6, and 1A2• Good understanding of substrates, inhibitors, and inducers can help
predict the risk for drug interactions in certain drug combinations
Enzyme induction = synthesis of metabolizing enzymes is stimulated;result is reduced plasma concentrations of the substrate agent due to theincreased metabolism; onset and offset is usually gradual and depends,among other factors, on half-life:• Rifampin’s short half-life enables induction of CYP3A4 and CYP2C
within 24 hours (note: rifampin is a self-inducer !)• Phenobarbital, on the other hand, with a half-life of 3 to 5 days, takes up
to a week to induce CYP3A4, CYP1A2, and CYP2C• Other inducers are rifabutin, carbamazepine, primidone, phenytoin
Interactions between CYP isoenzymes and herbal products• Garlic and melatonin may act as inhibitors,• St. John’s wort may be an inducer (observed with: indinavir,
theophylline, cyclosporine, oral contraceptives, digoxin, phencoumoron,and dextromethorphan)
• Grapefruit juice is an inhibitor of e.g. the CYP3A4 pathway, thus themetabolism of dyhydropyridines, saquinavir, cyclosporine, andverapamil.
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com
Frequent parties in drug interactions
• antiarrhytmics
• anticoagulants
• antacides
• anticonvulsives
• antidiabetics
• cytostatics
• H2-receptor antagonists
• psyhotropics (lithium, MAO-inhibitors)
• heart glycosids
• theophyllin
Role of metabolites
• original compound is inactive:
• pro-drug (cyclophosphamid, phenacetin, phenylbutazon, D-vitamin)
• quick metabolism (chloralhydrate, clofibrate)
• original compound and its metabolic are
pharmacologically equivalent:
allopurinol, diazepam, imipramin, lidocain, morphin, nalidixate,
probenecid, procainamid, propranolol, rifampycin, warfarin
• the action of the metabolite differs from the original compound:
codein - morphin, prenylamin - amphetamin
• the metabolite is responsible for toxicity:
INH, paracetamol, acetanilide, furosemid, chloramphenicol
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

CYP-450 system - Substrates
CYP1A2 caffeineclozapineR-warfarintacrinetheophylline
CYP2C9/10 phenytoinS-warfarintolbutamide
CYP2C19 amitriptylineclomipraminediazepamimipramineomeprazolephenytoinpropranolol
CYP2D6 amiodaroneamitriptylineclomipraminecodeinedesipraminedextromethorphanencainide/flecainidefluvoxamineimipraminemetoprololmexilitinenortriptylineperphenazinepropafenonepropranololthioridazinetimolol
CYP2E1 chlorzoxazonehalothanemethoxyflurane
CYP3A3/4 astemizolecarbamazepinecisapridecyclosporinedapsonediltiazemerythromycinfelodipinelidocainelovastatinmidazolamnifedipinequinidinetacrolimustamoxifenterfenadinetestosteronevalproic acidverapamil
Inducers of CYP Enzymes
All phenobarbitalphenytoin
CYP2E1 isoniazidCYP3A1 spironolactoneCYP3A4 carbamazepine
rifampin
Inhibitors of CYP enzymes
CYP1A2 cimetidineciprofloxacinenoxacinerythromycinfluvoxaminegrapefruit juiceritonavir
CYP2C9/10 fluconazoleCYP2C19 fluoxetine
fluvoxamineomeprazole
CYP2D6 cimetidinefluoxetinehaloperidolparoxetinequinidineritonavir
CYP3A3/4 cimetidineclarithromycindiltiazemerythromycinfluconazolefluoxetinefluvoxaminegrapefruit juiceindinaviritraconazoleketoconazolemiconazoleritonavir
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Environmental factors affecting the activity ofthe intestinal monooxigenase systems
Factor Effect
cigarette smoke GG
barbecued meat (steak) GGG
cholesterol GG
iron-poor diet HHH
semi-synthetic diet HH
fasting HH
neutral fat HH
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Drug - Nutrient Interactions
Drug Nutritient InteractionAntihypertensives,Digoxin
Digoxin
Felodipine
Iron Supplements,Sucalfate
Levodopa/Carbidopa
Lithium
MAO Inhibitors-Furazolidone-Isoniazid-Pargyline-Phenelzine-Procarbazine-Selegiline-Tranylcypromine
Quinidine
Quinolones-Ciprofloxacin-Norfloxacin-Ofloxacin
Theophylline,Neuroleptic Drugs
Theophylline
Warfarin
Warfarin
licorice
bran
grapefruit juice
dairy products
high protein meals
dietary sodium
tyramine-containingfoods (aged cheese[*],salted/pickled fish,beef or chicken, liver,alcoholic beverages)
citrus juices
minerals (magnesium,calcium, iron)
dietary caffeine
charcoal-broiled meats
green vegetables, avocado
fried or boiled onions
glycyrrhizic acid (largeamounts) induces hypokalemiaand sodium retention
reduced absorption
increased absorption
complexation resulting inreduced efficacy
reduced absorption
large amounts of dietarysodium can reduce efficacy
flushing, hypertension,cerebrovascular accidents
alkalinization of the urinemay impair elimination
reduction of antibiotic efficacy
excessive CNS stimulation
decrease in elimination halflife
reduction of anticoagulant effect
increase in anticoagulant effect[*] Avoid cheddar, camembert, roquefort cheese.
Processed cheese, cottage cheese, mozzarella and gouda may be eaten in moderation.
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Drug - Food Interaction of Grapefruit Juice
Flavonoids contained in grapefruit juice:• Naringin - a major flavonoid found in grapefruit juice having itself has no
apparent effect on human cytochrome P-450 enzymes - is apparently hydrolyzedin the intestine to naringenin: which is a potent inhibitor of several enzymefamilies, including CYP3A4, CYP1A2, and 11-beta-hydroxysteroiddehydrogenase
• Bergapten, a newly identified furocoumarin was detected in grape-fruit juice andSeville orange (!) juice, and it was found to be a mechanism-based inhibitorof CYP3A4.
Drug Pharmacodynamic EffectsCaffeine -
Cyclosporine -Diltiazem Greater decrease in mean arterial pressure and
prolongation of P--R interval during grapefruit juiceadministration.
Felodipine Concurrent grapefruit juice administration wasassociated with more frequent adverse effects, anincreased heart rate, and decreased diastolic bloodpressure compared with water or orange juice.
Midazolam Psychometric performance tests were significantlyaltered during grapefruit juice administration.
Nifedipine -Nisoldipine Concurrent grapefruit juice administration was
associated with an increased heart rate and minoreffects on systolic and diastolic blood pressures.
Nitrendipine Heart rate increased slightly (10%) with concurrentgrapefruit juice administration.
Quinidine No significant change in QTc interval between waterand grapefruit juice periods.
Terfenadine Increased QTc interval during grapefruit juiceadministration.
Triazolam Increased drowsiness was observed during concurrentgrapefruit juice administration.
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Monogenic oxydative polymorphism drugs(template drug: debrisoquin)
Drug Metabolicpathways
Clinical consequencein PM
Beta-blockersalprenololbufuralolmetoprololpropranololtimolol
AROHAROH, BOHBOH, ODMAROHODA
increased beta-receptorinhibition (metoprolol:loss of cardioselectivity)
Cardiovascularencainidguanoxanindoraminperhexylin
N-propyl-ajmalinpropafenonspartein
ODMAROHAROHALOH
AROH, ALOHBOH, AROHNO
higher dose requiredorthostasisCNS toxicityperipheric neuropathy,
liver damage
CNS toxicityCNS toxicity ,myometrium
contractionPsychotropicsamiflaminamitriptylinclomipramindesipramindextropmetorphanimipraminnortryptilin
NDMNDM, BOHAROHAROHODMAROHBOH
CNS toxicity
Othermetoxiphenaminphenacetinfenformincodein
ODMO-deaethylationAROHODM
NDmethemoglobinaemialactate acidosisdecreased analgetic effect
ALOH alifatic hydroxilationAROH aromatic hydroxilationBOH benzyl hydroxilation
NDM N- demethylationNO N-oxydation
ODM O-demethylationODA O-dealkylation
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Pharmacogenetic enzyme variations of clinical significance
Enzymedefect
Drug of risk Signs Heredity Incidence
cholinesterasedeficiency
suxamethonium postoperative paralysis AR Caucasian: +++Negroid: +
Asian: -paraoxonase
polymorphismparaoxon (parathion) toxicity AR 70% of Caucasians deficient
N-acethyltranferasepolymorphism
INHphenelzinehydralazine
sulphonamidesarylamines
polyneuritispsychosis
carcinogenesis
AR 70% of CaucasiansPM
hydroxilasepolymorphism
phenytoindicoumarolguanoxanphenacetindebrisoquin
spartein
toxicity and decreasedtherapeutic efficacy in
PM
AR rare
Caucasians 6-9% PMAsians 30% PM
G-6-PD deficiency antimalaria drugsFava bean
sulphonamides
haemolytic anaemia XR frequent in Africa andin the Mediterraneum
AR autosomic recessive PM poor metaboliserXR X-chromosome linked recessive
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Pharmacokinetic Interactions #3/3
Alterations in Elimination• Mechanism
• Reduced renal excretion of one drug by another;Example: penicillin-probenecid interaction - probenicid blocksactive secretion of penicillin in the renal tubule
• Alterations in urinary pHExample: alkalinization of urine increases methotrexate elimination
Pharmacodynamic Interactions
• are indicative of the pharmacologic actions of the interacting agents byadditive or synergistic toxicity or, conversely, additive or synergisticactivity; examples:• Drugs used together that depress the central nervous system (CNS)
usually interact, causing synergistic depression of the CNS• Cancer chemotherapy agents• Antihypertensives• St. John’s wort: monoamine oxidase inhibition? + serotonin reuptake
inhibition?• Kava kava - risk for increased central nervous system depression
when combined with other central nervous system depressants, suchas ethanol, conventional sedative hypnotics, and antidepressants
• Methotrexate (used in patients with severe psoriasis, psoriatic arthritisor bullous diseases) and trimethoprim inhibit human dihydrofolatereductase - may cause severe myelosuppression
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Drug interaction and renal function
Primarydrug
Drug causing theinteraction
Mechanism Clinicalconsequence
digoxin chinidin
verapamil
spironolactone
clearence ò
distribution
volume
clearence ò
clearence ò
distribution
volume
digoxin toxicity
methotrexate aspirin renal excretion ò bone marrow
depression
penicillin probenecid renal excretion ò cumulation of
penicillin
chinidin NaHCO3 renal excretion ò chinidin
intoxication
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Interactions between defibrillators and drugs
• Implanted (“ cardioverter” ) defibrillators combined withantiarrhytmic drugs:• beneficial effect: slower ventricular tachycardia may allow increased
ease in pace terminability by implanted defibrillators• deleterious effect: ability of drugs to slow ventricular tachycardia to
below the rate cutoff for the device, thus leading to non-detection• defibrillation threshold (DFT)
• V-W class Ia, Ib antiarrhythmics: either increase or cause no changein defibrillation energy requirements
• V-W class Ic : flecainide increase DFTs, propafenone appears to beneutral - has no effect on DFTs
• V-W class III: acute IV amiodarone has no effects on DFTs, althoughsome studies have shown that it decreases DFTs; chronic amiodaronegenerally tends to increase DFTs; other class III agents, for examplesotalol, decrease defibrillation thresholds.
• Calcium channel blockers increase defibrillation thresholds.• In modern defibrillator technology, there is sufficient safety margin
between the defibrillation threshold measured at implant and themaximum output of the device, that drugs that increase DFT do notusually lead to inability to defibrillate.
Dr. John DiMarco - 20th Annual Scientific Sessions of the North American Society of Pacing and ElectrophysiologyDay 2 - May 13, 1999
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Factors to consider before prescribingnon-sedating antihistamines (terfenadine and astemizole)
• Concurrent use of other medications that prolong the QT interval• Antiarrhythmic Drugs
• Amiodarone• Disopyramide• Ibutilide• Procainamide• Quinidine• Sotalol
• Others• Cisapride• Haloperidol (a structural analogue of terfenadine)• Pentamidine• Phenothiazines (eg, thioridazine)• Probucol• Quinine• Tricyclic antidepressants
• Concurrent use of ketoconazole, itraconazole, fluconazole,erythromycin, clarithromycin, quinine, saquinavir, ritonavir, orindinavir.
• Congenital long-QT syndrome.• Electrolyte disturbances that predispose to torsades de pointes (ie,
hypomagnesemia, hypokalemia, or hypocalcemia).• Recurrent ventricular tachycardia.• Substance abuse (since these patients may be more likely to take
excessive doses).• Liver disease or chronic alcohol abuse (since these patients may have
significant underlying liver disease).
Joette M. Meyer, Keith A. Rodvold : Drug Interactions Between Nonsedating Antihistamines and Anti-InfectiveAgents; in Infect. Med. 13(7):609-613,634 1996
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Drug interactions of ACEIs
Drug Interaction Clinicalsignificance
allopurinol skin rash, Stevens-Johnson sy. Maspirin prostaglandin synthesis é ,
aspirin effect êM
azathioprin risk of anaemia MMCa-channel
blockersslowing the progression of renal
insufficiencyJ
chlorpromazine augmented hypotension M
cyclosporin risk of renal damage M
digoxin digoxin SDC é M
statins ACEI vascular reactivity é J
insulin insulin effect é J
K-depletivediuretics
ACEI effect é JJJ
K-sparing diuretics risk of hyperkalaemia MMM
K-supplementation risk of hyperkalaemia MMM
interferon occasionally granulopenia and/orthrombopenia
M
ISMN increased reactivity for vasodilation J/Mlithium lithium toxicity MMM
moxonidin synergetic antihypertensive effect J
NSAID ACEI effect ê ; acute interstitialnephritis, haematuria, proteinuria,
nephrosis
MMM
rifampycin ACEI effect ê M
sulphanylureaOADs
OAD effect é M
trimethoprim risk of hyperkalaemia M
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Pharmacy and Therapeutics CommitteeFunctions • Reviews all adverse drug reaction (ADR) reports and initiates/approves appropriate modifications to policies, procedures,
protocols, pathways, etc.• Reviews all requests for new formulary medications• Thoroughly evaluates all medications, based on efficacy and toxicity, and if the potential for adverse effects is high, the medication
may be "Reserved" to specific practitioners, indications, or location of use within the institution, or may require specializedmonitoring, labeling, or use of standardized order sheets to minimize the risk of adverse drug events (ADEs)
Adult IV MedicationGuidelines
• Provide information on high-risk medications regarding dose; indication; qualifications of healthcare professional required toadminister medication -- ie, RN, LPN, critical care nurse; location of administration -- ie, critical care, general medical floor;monitoring parameters; and potential adverse effects that can be prevented from becoming actual ADEs.
Adult ChemotherapyGuidelines
• Contain information similar to the above for antineoplastic agents, as this class of medications can be associated with significantrisk for ADEs
Standardized Order Sheets • Antibiotic order sheets ; Antineoplastic order sheets ; Total parenteral nutritional order sheets ;• Standard order sheets based on pathway contents -- ie, MI standing orders based on MI pathway
Standardized Pathways • Developed by multidisciplinary teams to decrease the variability in care.RPh AttendsMultidisciplinary Rounds
• By doing so, the RPh proactively evaluates patient’s medication profile for potential ADEs.
Creatinine ClearanceMonitoring Program
• RPh monitors all renally eliminated medications and makes recommendations for dosage modification to prevent dose-relatedADRs.
Metformin (glucophage)Monitoring Program
• Evaluates renal function to ensure use is in accordance with FDA dosing recommendations to prevent the adverse effect of lacticacidosis
Interaction Monitoring • Monitor drug-drug and food-drug interactions, a preventable type of ADRPharmacy Bulletin • A newsletter distributed to the medical staff that focuses on rationale for drug therapy.
An issue is annually devoted to review of ADRs.Allergy Documentation • Any patient who experiences an ADR due to a hypersensitivity/allergic reaction is evaluated by a pharmacist, and the allergy
information is added to the hospital-wide computer system to prevent the patient from inadvertently receiving the medication at afuture date.
IV Labels • A significant number of cases of vancomycin-induced red-man syndrome were detected via ADR surveillance, leading to theaddition of the warning statement, "Run over 1 hour" to all vancomycin minibags.
FDA Reports • Warfarin/tramadol interaction resulting in prolongation of the prothrombin time was detected and reported to the FDA.This report and others resulted in this drug interaction being added to the package insert
• Subpotent diazepam injection was noted through surveillance. As a result, the institution changed brands of diazepam injection,and this corrected the problem.
• Angioedema associated with sumatriptan was reported to the FDA, and reports were published[26] to inform other healthcarepractitioners of this potentially life-threatening reaction.
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

Therapeutic Drug Monitoring (TDM)
1. profilactic drugs
2. low profile drugs: low therapeutic / toxic concentration ratio
3. doubtful compliance (in silent periods od chronic diseases)
4. desired therapeutic answer not achieved or
therapeutic answer is hard to quantify
5. significant interindividual variations in the effect or
metabolism of the drug
6. overdose , signs of toxicity (paradox intoxication)
7. changes in the pharmacokinetic properties fo the drug due to
secondary diseases (changes in hepatic and renal drug clearance)
8. non-linear pharmacokinetics
9. possibility of drug interaction
(changes in the bound-free fraction of the drug)
10. changes in the physiological state of the patient
(pregnancy, adolescence, elderly)
11. drug treatment should be documented (clinical studies)
12. racem drugs containing a kirality centre if the biological activity /
effect of the enantiomers differ
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

"Red Flag" List and Alternatives1. Cytochrome P-450 inhibitors: impair drug metabolism of other drugs which share the same pathway increase concentrationsof the co-administered drug.
DRUG CLASS LIKELIHOOD OF A DRUG INTERACTION ALTERNATIVESHIV Proteaseinhibitors
Ritonavir (Norvir® ) strongestAmprenavir (Agenerase® ) intermedIndinavir (Crixivan® ) intermedNelfinavir (Viracept® )intermedSaquinavir (Fortovase® / Invirase® ) - weakest
Saquinavir (Invirase® /Fortovase® ) has less potential to cause druginteractions
Macrolides Erythromycin and clarithromycin (Biaxin® ) are both inhibitorsof CYP450, however, the inhibition may be greater witherythromycin
Azithromycin (Zithromax® ) is not metabolized by CYP450 andmay be substituted if clinically warranted
Antifungals Listed by strength of inhibition:Ketoconazole (Nizoral® ) > Itraconazole (Sporanox® ) >Fluconazole (Diflucan® )
Ketoconazole (Nizoral® ) and Itraconazole (Sporanox® ) arepotent inhibitors of CYP450
Fluconazole (Diflucan® ) is associated with less drug interactionswhen dosages of 200 mg or less are used. As dose is increased,there is a greater potential for drug interactions.Topical antifungals such as clotrimazole (Mycelex® ) troches andnystatin may be useful for prophylaxis of thrush or minorinfections. For more severe fungal infections, amphotericin B(Fungizone® , Abelcet® , AmBisome® , Amphotec® ) may be used
Non-nucleosidereversetranscriptaseinhibitors
Delavirdine (Rescriptor® ) is a potent inhibitor of CYP450potentially raising concentrations of other drugs
Efavirenz (Sustiva® ) is a mixed inhibitor/inducer,depending on the concomitant drug
While it may be beneficial in some cases to use delavirdine toincrease concentrations of other drugs (e.g. protease inhibitors),alternatives in this class would be nevirapine and efavirenz(Sustiva® ) or perhaps nucleoside analogs (i.e., didanosine[Videx® ], zidovudine [Retrovir® ]) if clinically appropriate
H2 Antagonists Cimetidine (Tagamet® ) is a CYP450 inhibitor with a highpropensity for causing interactions
Any other H2antagonisti.e. Ranitidine (Zantac® )or Famotidine (Pepcid® )
Charles Flexner, MD and Steven Piscitelli, PharmD: Managing Drug-Drug Interactions in HIV Disease ; MedScape CME
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

2. Cytochrome P-450 Inducers:INDUCING DRUG STRENGTH ALTERNATIVES
Rifamycins:Rifabutin (Mycobutin® ) andRifampin (Rifadin® , Rimactane® )
Potent inducers of CYP450 and maydecrease concentrations of drugsmetabolized by these pathways
For patients receiving protease inhibitors, rifampin should beavoided. However, rifabutin (Mycobutin® ) may be used withindinavir (Crixivan® ), amprenavir (Agenerase® ) and nelfinavir(Viracept® ) at one-half the normal dose (150 mg/day). For ritonavir(Norvir® ), rifabutin (Mycobutin® ) can be used on an every-other-day basis or 3 times weekly at one half the normal dose (150 mg qM-W-F). In patients requiring MAC prophylaxis, azithromycin(Zithromax® ) or clarithromycin (Biaxin® ) may be substituted forrifabutin
HIV Protease inhibitors:Nelfinavir (Viracept® ) andRitonavir (Norvir® )
Moderate inducers of CYP450, potentiallydecreasing concentrations of other drugswhich are metabolized
In this class Alternatives would be:amprenavir (Agenerase® )indinavir (Crixivan® )saquinavir (Fortovase® )delavirdine (Rescriptor® )or perhaps nucleoside analogs, i.e.didanosin e (Videx® )zidovudine (Retrovir® ) could be used if clinically appropriate
Non-nucleoside reversetranscriptase inhibitors:Nevirapine (Viramune® ) andEfavirenz (Sustiva® )
Moderate inducers of CYP450, potentiallydecreasing concentrations of other drugs
Alternatives in this class would be delavirdine or perhaps nucleosideanalogs i.e.didanosine (Videx® )zidovudine (Retrovir® )if clinically appropriate
Anticonvulsants:PhenobarbitalPhenytoin (Dilantin® )Carbamazepine (Tegretol® )
Major / moderate inducers of CYP450,potentially decreasing concentrations ofother drugs.
If clinically warranted, possible alternative anti-epileptics include:valproic acid (Depakene® , Depakote® )gabapentin (Neurontin® )lamotrigine (Lamictal® )topiramate (Topamax® )tigabine (Investigational Tabitril® )
Charles Flexner, MD and Steven Piscitelli, PharmD: Managing Drug-Drug Interactions in HIV Disease ; MedScape CME
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com

3. Metabolized drugs with narrow therapeutic indexes:CATEGORY DRUGS ALTERNATIVES / NOTES
Non-sedatingantihistamines
Terfenadine (Seldane® ) Astemizole (Hismanal® )*although removed from US market, patients maystill have supplies
Newer non-sedating antihistamines such as fexofenadine (Allegra® )and loratadine (Claritin® ) can be safely used with P450 inhibitors, aswell as most over-the counter preparations
Antiarrythmics Flecainide (Tambocor® ) Encainide (Enkaid® )Quinidine
Antiarrhythmic therapy should be closely monitored and used withcaution in patients receiving inhibitors of cytochrome P-450
Long-acting opiateanalgesics
Fentanyl (Sublimaze® , Duragesic® ) Alternative analgesics include hydromorphone, codeine, andNSAIDs, particularly in patients receiving ritonavir (Norvir® )
Promotility agents Cisapride (Propulsid® ) Metoclopramide (Reglan® )Long-actingbenzodiazepines
Midazolam (Versed® ) Triazolam (Halcion® )
Ergotamines anddihydroergotamine
Cafergot® Hydergine® D.H.E. 45®
Illicit drugs Ecstacy/XTC/MDMACoumarin anticoagulants Warfarin (Coumadin® )Oral contraceptives Oral contraceptives should not be given concurrently with P450
inducers, as this can decrease their concentrations and lead tounwanted pregnancy
4. Renally cleared drugs with narrow therapeutic indices:DRUG / NOTES ALTERNATIVESFoscarnet (Foscavir® )Ganciclovir (Cytovene® )
Adjust dose for renal function with these agentsCidofovir (Vistide) may be used if clinically appropriate, but this agent cancause irreversible renal insufficiency
Aminoglycosides:GentamycinTobramycinAmikacin (Any drugs that are nephrotoxic may decrease aminoglycosideclearance and increase likelihood of aminoglycoside toxicity)
Other antibiotics covering gram – bacteria:Aztreonam (Azactram® )Broad Spectrum penicillins and cephalosporins
Charles Flexner, MD and Steven Piscitelli, PharmD: Managing Drug-Drug Interactions in HIV Disease ; MedScape CME
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com
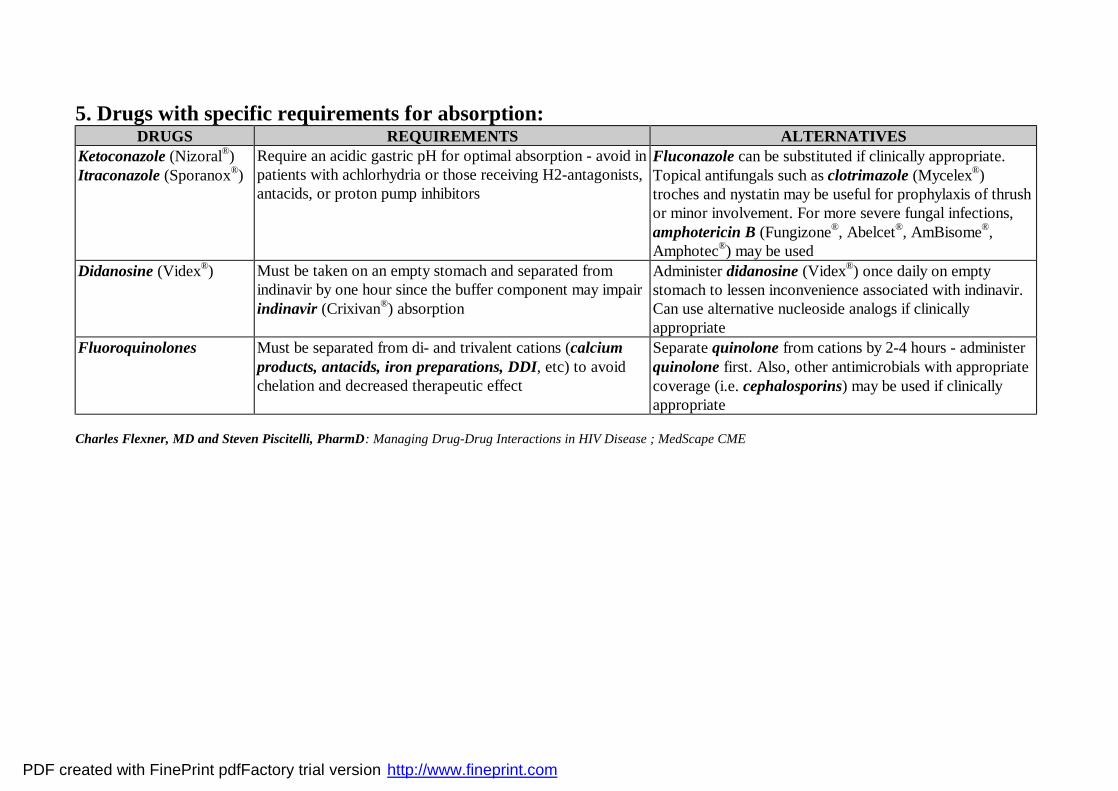
5. Drugs with specific requirements for absorption:DRUGS REQUIREMENTS ALTERNATIVES
Ketoconazole (Nizoral® )Itraconazole (Sporanox® )
Require an acidic gastric pH for optimal absorption - avoid inpatients with achlorhydria or those receiving H2-antagonists,antacids, or proton pump inhibitors
Fluconazole can be substituted if clinically appropriate.Topical antifungals such as clotrimazole (Mycelex® )troches and nystatin may be useful for prophylaxis of thrushor minor involvement. For more severe fungal infections,amphotericin B (Fungizone® , Abelcet® , AmBisome® ,Amphotec® ) may be used
Didanosine (Videx® ) Must be taken on an empty stomach and separated fromindinavir by one hour since the buffer component may impairindinavir (Crixivan® ) absorption
Administer didanosine (Videx® ) once daily on emptystomach to lessen inconvenience associated with indinavir.Can use alternative nucleoside analogs if clinicallyappropriate
Fluoroquinolones Must be separated from di- and trivalent cations (calciumproducts, antacids, iron preparations, DDI, etc) to avoidchelation and decreased therapeutic effect
Separate quinolone from cations by 2-4 hours - administerquinolone first. Also, other antimicrobials with appropriatecoverage (i.e. cephalosporins) may be used if clinicallyappropriate
Charles Flexner, MD and Steven Piscitelli, PharmD: Managing Drug-Drug Interactions in HIV Disease ; MedScape CME
PDF created with FinePrint pdfFactory trial version http://www.fineprint.com


















