Drug Interactions in TB / HIV Co-infected...
43
Presented at the 3 rd Intl. Workshop on Clinical Pharmacology of TB Drugs 11 September 2010, Boston USA Drug Interactions in TB / HIV Co-infected Patients Saye Khoo HIV Pharmacology Group University of Liverpool / Biomedical Research Centre in Microbial Diseases Presented at the 3 rd Intl. Workshop on Clinical Pharmacology of TB Drugs 11 September 2010, Boston USA
Transcript of Drug Interactions in TB / HIV Co-infected...

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Drug Interactions in TB / HIV Co-infected Patients
Saye KhooHIV Pharmacology Group
University of Liverpool / Biomedical Research Centre in Microbial Diseases
Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
HIV and TB ‐ prevalence
Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Menu
• HIV‐TB drug interactions
• What we know and don’t know
• Inter‐individual differences in DDIs
• Management of DDIs in different healthcare settings

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Potential to be affected Potential to affect other drugs
ADME Potential Mechanism Potential
NRTIs
NNRTIs CYP2B6, CYP3A4 P450 inducer
PIs CYP3A4, transporters
Inhibits P450Induces UGT
Integrases UGT1A1
maraviroc CYP3A4
T20
ARV and TB drugs have great potential for interactions – comprising some of the most ‘therapeutically risky’ drugs for DDIs

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Potential to be affected Potential to affect other drugsADME Potential Mechanism Potential
Rifampicin* CYP3A4, SLCO1B Induce CYPs, transporters Isoniazid* Acetylation Pyrazinamide* POA; renal Ethambutol renal (75%) Streptomycin renal Rifabutin CYP P450 Rifapentine esterase Induces 3A4, 2C8/9 Moxifloxacin Phase II Gatifloxacin Renal (77%) Capreomycin renal Ethionamide* SulphoxidePAS Renal (>80%) Linezolid Renal MAO inhibitor Cycloserine Renal (65%)
TMC207 CYP3A4 PA824 SQ109 CYP2D6, 2C19 OPC67683 LL3858 ? ?

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
- 86%
- 35%
- 89%
- 82%
- 82%
- 73%
- 63%
- 80%
- 72%
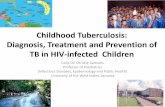
Change (%) in AUC of ARVs when given with rifampicin
www.hiv-druginteractions.org accessed Sept 2010
- 40%
- 26%
- 40%
• No significant interactions – NRTIs and T20• Steady‐state RIF, single or multiple doses HIV drugs• Patients and healthy volunteers• No data on intermittent or high dose RIF regimens
ND ND

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
+53%+4 fold
+2 fold+11 fold
+3 fold+2 fold
+17%- 38%
-17% RBT AUC
Change (%) in AUC of ARVs when given with rifabutin
www.hiv-druginteractions.org accessed Sept 2010
• Studies done in healthy volunteers• HIV/TB patients – RBT exposure with intermittent RBT + LPVr• No data for RPT

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
www.hiv-druginteractions. org
Rif INH PZA Eth Strep RBT RPT Mox Ethio Cyclo Capreo TMC 207
PA 824
OPC 67683
SQ 109
SQV/r RTV IDV
NFV FPV/r LPV/r ATV/r TPV/r DRV/r
NVP EFV ETR ZDV 3TC ddI
d4T ABC ddC FTC TDF ENF MVC RAL
TB-HIV drug interactions

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
What we know What we need to know
ARVs do not completely eliminate TB risk
No substitute for rifamycin in intensive or continuation phases
Interaction potential Rif>RPT>RBT
Plasma exposure of Rif, INH, ethambutol reduced in TB, and HIV patients compared with healthy volunteers
Induction potential with different dosing of Rif
Large datasets of RBT safety and efficacy in HIV+TB coinfection
Optimal RBT dose with bPI
Interaction data for new drugs & RPT
Shorter regimens with greater sterilisation
HIV‐TB Treatment interactionsTB drugs
McIlleron et al AAC 2006;50:1170-77Perlman et al 2005; 41:1638–47Tappero et al. CID 2005;41:461-9Sahai et al. AIM 1997;127:289–293O’Reilly. AIM 1974;81:337
Lawn et al AIDS 2009, 23:1717–1725Jindani et al. Lancet 2004;364:1244Burman et al. CPK 2001;40:327Boulanger CID 2009; 49:1305–11

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Effect of disease on PKEffect on ARVsPIs‐ ATV, others less clear
Effect on TB drugsR, H, E concentrations altered in TB vs healthy volunteersAdditional impact of HIV on Rif & INH ?
RBT PK in HIV/TB co‐infection (n = 10; USA)Cmax targets >0.30 g/mL
TBTC Study 23A: Cmin 0.45 g/mL, AUC >5.2 g.h/mL(<3.2 for ARR)1 patient relapsed with ARR
No below Cmax target
RBT 300mg od 5 / 10
RBT 150mg 3x/w + LPVr 7 / 10
Boulanger CID 2009; 49:1305–11

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
What we know What we need to know
ARVs do not completely eliminate TB risk
No substitute for rifamycin in intensive or continuation phases
Interaction potential Rif>RPT>RBT
Plasma exposure of Rif, INH, ethambutol reduced in TB, and HIV patients compared with healthy volunteers
Induction potential with different dosing of Rif
Large datasets of RBT safety and efficacy in HIV+TB coinfection
Interaction data for new drugs & RPT
Shorter regimens with greater sterilisation
HIV‐TB treatment interactionsTB drugs
McIlleron et al AAC 2006;50:1170-77Perlman et al 2005; 41:1638–47Tappero et al. CID 2005;41:461-9Sahai et al. AIM 1997;127:289–293O’Reilly. AIM 1974;81:337
Lawn et al AIDS 2009, 23:1717–1725Jindani et al. Lancet 2004;364:1244Burman et al. CPK 2001;40:327Boulanger CID 2009; 49:1305–11

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
What we know What we need to know
Integrate ART into TB therapy
NNRTIs preferred: observational data suggest efficacy and safety of EFV > NVP if started during TB therapy
No dose modification of EFV in Africans and Thais
2nd line choices are difficult
How and when to start
NNRTIs‐ prospective trials
How to use NVP ?
Pharmacogenetics – CYP2B6 ?
Safety of bPIs with Rif
LPVr ‘superboosting’ ?
Raltegravir efficacy data
NRTI only regimens ?
Alternatives to a rifamycin ?
HIV‐TB treatment interactionsHIV drugs
Schmidt et al. Arch Drug Info 2009;2:8–16Nijland et al AIDS 2008:22:931;Acosta AAC 2007;51:3104Burger et al. AAC 2006;50:3336Haas CROI 2008 Abst 766bAbdool Karim et al. NEJM 2010;362:697-706Boulle et al. JAMA 2008;300:530-39Stohr. AVT 2008;13:675

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Outcomes in a “smear negative” cohort treated for TB
Hargreaves N, et al, INT J TUBERC LUNG DIS 2001 5(9):847–854
• mortality in smear-positives ~23% [Harries IJTLD 2001]
• higher mortality in smear-negative, HIV-positive
• can early introduction of ARVs modulate this ?
Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
SAPIT
Abdool Karim et al. NEJM 2010;362:697
HIV‐positive, CD4 <500new TB infection
HIV‐positive, CD4 <500new TB infection
Early integrated (IP)Early integrated (IP) Late Integrated (CP)
Late Integrated (CP)
N = 642
Sequential (> 6m)N = 213
Sequential (> 6m)N = 213
Combined IntegratedN = 429
Combined IntegratedN = 429
HIV+ , TB infection in S Africa
CD4 count ≤ 500
Randomised open label
• Early Integrated : intensive phase (within 4w) • Late Integrated: continuation phase (within 4w of completing IP)
• Sequential : within 4w of completing TB therapy
ddI + 3TC + EFV (600mg)

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
SAPIT
Abdool Karim et al. NEJM 2010;362:697
HIV‐positive, CD4 <500new TB infection
HIV‐positive, CD4 <500new TB infection
Early integrated (IP)Early integrated (IP) Late Integrated (CP)
Late Integrated (CP)
N = 642
Sequential (> 6m)N = 213
Sequential (> 6m)N = 213
Combined IntegratedN = 429
Combined IntegratedN = 429

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
CAMELIAANRS1295/1260‐ CIPRA KHOO1/10425
• HIV+ , TB infection in Cambodia
• low CD4 count (median 25)
• Randomised to early (2w) vs late (8w) ART
• d4T + 3TC + EFV(600mg)
• superiority trial• Primary endpoint: survival
• Secondary endpoints: IRIS, virological & immunological response
HIV‐positive, CD4 <200new TB infection
HIV‐positive, CD4 <200new TB infection
Early ART (2w)N = 332
Early ART (2w)N = 332
Late ART (8w)N = 329
Late ART (8w)N = 329
N = 661
Blanc et al. IAS 2010 Vienna THLBB106

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Camelia HIV‐positive, CD4 <200new TB infection
HIV‐positive, CD4 <200new TB infection
Early ART (2w)N = 332
Early ART (2w)N = 332
Late ART (8w)N = 329
Late ART (8w)N = 329
N = 661
Blanc et al. IAS 2010 Vienna THLBB106

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
EFV vs NVP
Khayelitsha observational data (N=2035) suggest inferior outcomes with NVP in patients with concurrent, but not incident TB
Blantyre data (n = 27) suggest 59% NVP ‘plasma levels’ subtherapeutic during lead‐in, vs 14% at weeks 4 & 8
Thai RCT (N2R Study)Prospective RCT (N = 142) EFV (600) vs NVP (400, standard lead‐in)
At w12, C12h < MEC in EFV (3.1%) vs NVP (21.3%)No difference in CD4 & VL responseVariability EFV >> NVP (CV 107% vs 47%)
Boulle et al. JAMA 2008;300:530-39Van Osterhout et al 2008;300:530-39Manosuthi et al CID 2009:48:1752

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
NVP 400 vs 600 mg / day
Thai patients (N = 32) on Rif for 2-6 weeks
Randomised to• NVP 400mg/day: 200mg/day lead-in• NVP 600mg/day: 400mg/day lead-in
PK of NVPProportion C12 below 3.1mg/L at w2NVP400 (79%) vs NVP600 (19%) (P = 0.002)
NVP hypersensitivityNVP600 (4/16) 2 during lead-inNVP400 (1/16)3 /4 were female
Proportion C12 <3.1mg/L
Avihinghasanon et al AVT 2008;13:529
Indian patients (N = 13)• NVP Cmax and Ctrough sampled before & 1 week after Rif• Ctrough <MEC in 8/13 patients• Dose increment to 300mg bd restored NVP troughs to therapeutic
range in 7/7 patientsRamachandran JAIDS 2006, 41:36-41

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
NVP 400mg vs 600mg/day
Elsherbiny et al EJCP 2009;65:71
• S African HIV+ patients taking NVP‐based regimen
• with (n=27) and without (n=26) concurrent TB treatment
• Population PK models: Cl/F by 37.4%
• Simulations suggest 300mg NVP bid achieves adequate concentrations
Predicted NVP 200mg bid
Predicted NVP 300mg bid

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
CARINEMO HIV‐positive, CD4 <250new TB infection
HIV‐positive, CD4 <250new TB infection
EFVEFV NVPNVP
N = 570
• HIV+ , TB infection in Mozambique
• Randomised to EFV versus NVP‐based ART
• started 4‐6w after TB treatment
• no lead‐in dosing of NVP (i.e. starting at 200mg bid)
• PK data presented in 20 patients M:F 11:9
Median weight 52.7 kg
Bonnet et al WAC Cape Town 2009

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
CARINEMO HIV‐positive, CD4 <250new TB infection
HIV‐positive, CD4 <250new TB infection
EFVEFV NVPNVP
N = 570
Bonnet et al WAC Cape Town 2009

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Incident TB on ART
Komati et al AIDS 2010, 24:1849–1855
ART reduces, but does not eliminate TB in high prevalence settings
Different treatment scenario• No lead-in dosing issues• Risk of HSR lower • Induction is taking place over 10-14 days• ? Increase NVP dose• ? If so, when ?
Lawn et al AIDS 2009, 23:1717–1725
PHIDISA Cohort (n = 1771) Gugulethu Cohort (n = 1480)

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
NevRif (Malawi)
• developing incident TB following >4w of NVP-containing ART• N = 20 (M:F 10:10), Mean BMI 19.4• mean 1.5 months on NVP
• AUC0-8h 22% over 2 weeks • Day 3 gave the greatest mean drop in NVP levels of 21.3 %• 30% patients had NVP troughs below MEC
Chaponda et al IWCPHT 2010 Sorrento
Incident TB on ART

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Incident TB
New HIV Diagnosis Not on ARVs
Receiving ARVs(assumes virologically suppressed)
HIV resistance testNNRTI‐ susceptible?
EFV‐containing regimen
Known Drug Interactions ?No
YesContinue regimenNRTI onlyENF containingManageable Interaction ?
Yes‐ EFV or RAL
No / difficult‐ PI, NVP, MVC Continue, dose
modify if appropriate– EFV or RAL‐ containingCan be safely switched to EFV ?
No Yes
Modify TB treatmentSubstitute Rif with RBT+ current regimen
or
Yes No
Modify TB treatmentSubstitute Rif with RBT+ bPI‐containing ART
or Modify ARVs‐ RAL regimen if possible
Less preferable‐ bPI – ‘super‐boosted ‘LPVr‐ RTV at full dose‐ Double dose MVC‐ Switch to ENF‐ NRTI‐only regimen
Modify ARVs‐ RAL regimen if possible
Less preferable‐ bPI – ‘super‐boosted ‘LPVr‐ RTV at full dose‐ Double dose MVC‐ Switch to ENF‐ NRTI‐only regimen
Concurrent TB

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Menu
• HIV‐TB drug interactions
• What we know and don’t know
• Inter‐individual differences in DDIs
• Management of DDIs in different healthcare settings

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Can Rif – EFV interaction differ between people?
Rif tends to increase rather than decrease variability 5 ‐ 55 fold in oral AUC of S‐verapamil, midazolam and theophyllineCV of EFV was 58% without, vs 157% with Rif (n = 19)
Inter‐individual differences in EFV – Rif interaction ?Ethnicity and CYP2B6 PM more than compensates for Rif effect
Non‐genetic factorssmoking (CYP P450 induction), diet, etc
Genetic factorsRif + S‐mephenytoin induction in CYP2C19 EMs, but not PMsRif + Propafenone induction in CYP2D6 PMs, but not EMs
Friedland JAC 2006;58:1299Di Iulio et al Pharmacogenet Genom 2009;19:300Ren et al. JAIDS 2009;50:439Ramachandran AAC 2009;53:863Uttayamakul AIDS Res Ther 2010;7:8Uttayamakul IAS 2010 Vienna WEPE0104
Lin. Ann Rev Pharm Toxicol 2001:41:535Fromm BJCP 1998;45:247Backman CPT 1996;59:7Robson BJCP 1984;18:445Zhou. BJCP 1990;30:471Dilger. Pharmacogenetics 1999;9:551

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
TB coinfection – to dose increase or not ?
020406080
100
020406080
100
white black white black
white black white black
600mg 800mg 600mg 800mg 600mg 800mg 600mg 800mg
600mg 800mg 600mg 800mg 600mg 800mg 600mg 800mg
50kg 60kg
70kg 80kg
EFV < 1000ng/ml EFV 1000-4000ng/ml EFV > 4000ng/ml
%Multivariable regression model: predicted trough (C24h )
Male, aged 41y, on EFV for 12 months, taking TB treatment
Stohr. AVT 2008;13:675

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
020406080
100
020406080
100
white black white black
white black white black
600mg 800mg 600mg 800mg 600mg 800mg 600mg 800mg
600mg 800mg 600mg 800mg 600mg 800mg 600mg 800mg
50kg 60kg
70kg 80kg
EFV < 1000ng/ml EFV 1000-4000ng/ml EFV > 4000ng/ml
%
TB coinfection – to dose increase or not ?Multivariable regression model: predicted trough (C24h )
Male, aged 41y, on EFV for 12 months, taking TB treatment
Stohr. AVT 2008;13:675

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
• 26 TB+ HIV patients from Ghana• Concomitant Rif + EFV (600mg)• CYP2B6 516G>T + haplotypes• Rif did not reverse effects of poor
metaboliser genotype
CYP 2B6 PolymorphismsN=26 Ghanians given EFV + RIF
Kwara et al. JCP 2008;48:1032Kwara BJCP 2009;67:427
• 65 patients from Ghana on EFV• 19 received comitant Rif + EFV (600mg)• CYP2B6 and CYP2A6 PM genotypes
accounted for 36% and 12% population variance
• No significant effect of Rif use

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Variability in Rif – EFV interaction
CYP2B6 PM more than compensates for Rif effect
• S Indian patients (n = 57) receiving EFV + Rif• Full PK with genotyping in n = 19• sparse PK in n = 38• CYP2B6 G516T but not Rif significantly influenced EFV PK
• Thai patients (n = 124) receiving EFV (600mg) + Rif• CYP 2B6 516 GG (38.5%), GT (47.7%) and TT (13.9%) affect C12h concentrations• small effect of Rif on EFV PK in comparison
Ramachandran et al. AAC 2009;53:863Uttayamakul et al. AIDS Res Ther 2010;7:8

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
CYP2B6
CYP2A6
Hom-LOF 2B6 & 2A63A4 _rs46464337
Hom-LOF 2B6Het 3A4 _rs46464337
Di Iulio et al Pharmacogenet Genom 2009;19:300Arab Almeddine et al. CPT 2009;85:485
X X

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
0
5000
10000
15000
20000
25000
on RIF off Rif
EFV
conc
entr
atio
n (n
g/m
L)
CV 157% CV 58%
0
5000
10000
15000
20000
25000
on RIF off Rif
EFV
conc
entr
atio
n (n
g/m
L)
CV 157% CV 58%
Adults (n=19) Durban Children (n=15) Cape Town
Ren et al. JAIDS 2009;50:439Friedland et al JAC 2006;58:1299
Variability in Rif – EFV interaction
• Thai patients (n = 124) receiving EFV (600mg) + Rif• CYP 2B6 516 GG (38.5%), GT (47.7%) and TT (13.9%)• C12h concentrations• small effect of Rif on EFV PK in comparison
Ramachandran et al. AAC 2009;53:863Uttayamakul et al. AIDS Res Ther 2010;7:8

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Overlapping Syndromes
Syndrome Causes
Febrile, generally unwell IRIS, paradoxical reactions, MDR TB
Abnormal LFTs TB drugs, HIV drugs, paradoxical reactions, hepatitis virus ‘flares’
neuropathy d4T, ddI, 3TC, HIV, isoniazid, ethionamide, linezolid
Eye problems Ethambutol, rifabutin, linezolid, ethionamide
CNS Efavirenz, cycloserine
Cardiac PIs, quinolones
Arthropathies HIV, pyrazinamide, quinolones, PAS

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Menu
• HIV‐TB drug interactions
• What we know and don’t know
• Inter‐individual differences in DDIs
• Management of DDIs in different healthcare settings

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Risk for clinically significant interactions
Study
Year Setting N CSDI lower Screening Tool Adverse Notes
de Maat et al
2004 Netherlands (hospital)
115
105
26%
23%
N/A Liverpool website
N/A Pharmacy screening effective, further pharmacy input not
Shah et al
2007 USA (Medicaid)
571
(689)
30%
(15%)
8%
(4%)
Liverpool websiteMicromedex
no VL impact
Audit, and re-audit.
Miller et al 2007 USA (hospital)
153 41% N/A DHHS SPC / PI Micromedex
N/A Age >42y (OR 2.9) >3 conditions (OR 3.0) >3 ARVs (OR 2.4) PI use (OR 11.5)
Kigen et al
2009 Kenya (hospital)
996 34%* 12% Liverpool website
N/A
Marzolini et al
2009 Switzerland(hospital)
1497 40% 4% Liverpool website
no CD4 or VL impact
Antiviral Ther 2010
Evans-Jones et al
2009 UK (hospital)
159 27% 15% Liverpool website
N/A CID 2010Only 36% CSDIs correctly identified
* excludes ARV-ARV interactions

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Risk for clinically significant interactions
Study
Year Setting N CSDI lower Screening Tool Adverse Notes
de Maat et al
2004 Netherlands (hospital)
115
105
26%
23%
N/A Liverpool website
N/A Pharmacy screening effective, further pharmacy input not
Shah et al
2007 USA (Medicaid)
571
(689)
30%
(15%)
8%
(4%)
Liverpool websiteMicromedex
no VL impact
Audit, and re-audit.
Miller et al 2007 USA (hospital)
153 41% N/A DHHS SPC / PI Micromedex
N/A Age >42y (OR 2.9) >3 conditions (OR 3.0) >3 ARVs (OR 2.4) PI use (OR 11.5)
Kigen et al
2009 Kenya (hospital)
996 34%* 12% Liverpool website
N/A
Marzolini et al
2009 Switzerland(hospital)
1497 40% 4% Liverpool website
no CD4 or VL impact
Antiviral Ther 2010
Evans-Jones et al
2009 UK (hospital)
159 27% 15% Liverpool website
N/A CID 2010Only 36% CSDIs correctly identified
* excludes ARV-ARV interactions

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
How common are HIV Drug Interactions ?
Kenya [Kigen et al. HIV8, 2008 Abstract O121; manuscript in preparation]
• 996 consecutive patients receiving ARVs• Moderate / Major drug interactions identified in 34%• 12% (1:3 CSDIs) could have lowered ARV concentrations• Rifampicin > Azoles > Steroids > Antimalarials > PPIs

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Risk for clinically significant interactionsStudy
Year Setting N CSDI lower Screening Tool Adverse Notes
de Maat et al
2004 Netherlands (hospital)
115
105
26%
23%
N/A Liverpool website
N/A Pharmacy screening effective, further pharmacy input not
Shah et al
2007 USA (Medicaid)
571
(689)
30%
(15%)
8%
(4%)
Liverpool websiteMicromedex
no VL impact
Audit, and re-audit.
Miller et al 2007 USA (hospital)
153 41% N/A DHHS SPC / PI Micromedex
N/A Age >42y (OR 2.9) >3 conditions (OR 3.0) >3 ARVs (OR 2.4) PI use (OR 11.5)
Kigen et al
2009 Kenya (hospital)
996 34%* 12% Liverpool website
N/A (in preparation)
Marzolini et al
2009 Switzerland(hospital)
1497 40% 4% Liverpool website
no CD4 or VL impact
(submitted)
Evans-Jones et al
2009 UK (hospital)
159 27% Liverpool website
N/A Only 36% CSDIs correctly identified
* excludes ARV-ARV interactions
Evan Jones et al CID 2010;50:1419

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Interventions which work• Prescriber education
• Pharmacist input [1-2]
• Drug interactions databaseswww.hiv-druginteractions.org, www.clinicalcareoptions.com, etcConcordance is variable [3]
Tendency to over-call – ‘Alert fatigue’ !
• ‘Active vs passive’ identification of interactionsDecision support software for dispensaries / electronic prescribers
Interaction datasheets for patients or prescribers
• Therapeutic Drug Monitoringto manage interactions, or else to discount them
1 Hanlon Am J Med 1996;100;428. 2 de Maat J Clin Pharm Ther 2004;29:1213 Pham. CPT 2008;83:396

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Resource‐limited settings
A Public Health approach to managing DDIs
• Training to improve quality of prescribing
• Regional Drug Information Centres – e.g. ATIC
• Programmatic approach – Integrated, rather than vertical programmes
• Instituting systems for pharmacovigilance
• Incorporate monitoring for serious DDIs within ARV Programmes
• Audit quality of prescribing

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Liverpool HIV Drug Interactions website

Presented at the 3rd Intl. Workshop on Clinical Pharmacology of TB Drugs11 September 2010, Boston USA
Acknowledgements
www.hiv-druginteractions.orgReceives sponsorship from GSK, Abbott, Merck, BMS, Tibotec, Roche, Gilead, Pfizer, Elton John AIDS Foundation, British HIV Association, Glasgow HIV conference.
Editorial content remains independent.
Declaration of Interests
David BackGerry DaviesAndrew OwenSara GibbonsKay Seden
Wolfgang StoehrDavid DunnGabriel KigenLawrence LeeCeppie Merry
… and many others….