DRUG DISCOVERY & DEVELOPMENT Antibody-drug ......DRUG DISCOVERY & DEVELOPMENT R&D Solutions for...
8
SUMMARY Antibody-drug conjugates (ADCs) take advantage of the specificity of antibodies to deliver bioactive payloads directly to disease sites. Due to their modularity, ADCs offer almost endless possibilities for treating various cancers, but optimizing these very complex combinations brings many challenges. Antibody-drug conjugates: Converting our expanding knowledge base into successful immunotherapeutics DRUG DISCOVERY & DEVELOPMENT R&D Solutions for PHARMA & LIFE SCIENCES
Transcript of DRUG DISCOVERY & DEVELOPMENT Antibody-drug ......DRUG DISCOVERY & DEVELOPMENT R&D Solutions for...
-
SUMMARYAntibody-drug conjugates (ADCs) take advantage of the specificity of antibodies to deliver bioactive payloads directly to disease sites. Due to their modularity, ADCs offer almost endless possibilities for treating various cancers, but optimizing these very complex combinations brings many challenges.
Antibody-drug conjugates: Converting our expanding knowledge base into successful immunotherapeutics
DRUG DISCOVERY & DEVELOPMENT
R&D Solutions for PHARMA & LIFE SCIENCES
-
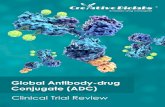
Antibody-drug conjugates (ADC) represent an exciting new dimension in the fight against cancer and is one of many different approaches that utilize the patients own immune system (Figure 1). ADCs take advantage of the specificity of antibodies to deliver bioactive payloads directly to disease sites. This targeted delivery strategy enables the use of highly cytotoxic payloads that cannot be used systemically. Achieving a therapeutic dose at the disease site requires a small amount of the cytotoxic agent, keeping systemic exposure low and safe.
Due to their modularity, ADCs offer almost endless possibilities for treating various cancers, but optimizing these very complex combinations brings many challenges. Powerful tools and methods to address these challenges are in development, and to effectively implement these and propel ADC development forward, we must capture and leverage everything we have learned to date – both our successes and our failures.
Two ADCs are currently used in patients: Adcetris for treating certain relapsed or refractory lymphomas and Kadcyla for treating Her2-positive breast cancer. The rapidly expanding field has over 40 more ADCs currently in clinical development and many more showing preclinical promise.1–3
Learning from our failuresEarly ADCs failed in the clinic, because we did not fully understand how interactions of tumor cell targets with the antibody
vehicles and drug payloads influenced therapeutic outcomes and toxicities. Murine antibody vehicles caused patients to develop immune responses against the foreign antibodies.4,5 Poor efficacy was common due to low potency payloads, unstable linkers, low levels of antigen expression on the tumor cells, and failure of the tumor cells to internalize the conjugates.5
In 2000, Mylotarg became the first ADC approved by the FDA, but it was removed from the market due to problems with efficacy and toxicity.3 We later learned that patients with tumors overexpressing P-glycoprotein were resistant to treatment because the cytotoxic metabolites were substrates for P-glycoprotein and were easily transported back out of the cells.3 The linker had a short half-life and released the payload in healthy tissues. Furthermore, poor conjugation efficiency produced heterogeneous populations with about half of the antibodies carrying 4-6 payloads each, and the other half carrying none.2,3 These insufficiently conjugated antibodies reduced treatment efficacy by binding the target and blocking antibodies with sufficiently conjugated payloads.
Optimizing individual componentsWe now know how important the choice of target antigen and each individual ADC component are to a successful combination. The antibody vehicle, the bioactive payload, and the linkage between the two each functions in the complex context of the others, and any of the components can contribute to efficacy or toxicity issues.
The understanding of how to successfully combine the right therapeutic payload with the right antibody and target the right patient group continues to grow.
2
-
Anti-tumor antibodies (HER2/neu, CD20)
Immune checkpoint inhibitors (CTLA-4, PD-1/PDL-1)
Adoptive cell transfer (CAR T cells, DCs)
Co-stimulatory agonists (4-1BB)
Vaccines (peptides, viruses)
Antibody-drug conjugates CD30, HER2/neu)
Oncolytic viruses (HSV1716, H101)
Angiogenesis blockers (VEGF)
3
TargetSelecting the tumor antigen target is one of the most critical aspects of ADC development. The target must be expressed at high levels and exclusively on tumor cells to maximize exposure and achieve high concentrations of payload inside the cells.2 Expression on healthy cells increases the likelihood of off-target toxicities. In addition, the target antigen should not be shed or secreted from the tumor cells, as this can also increase the chance of toxicity.2
The heterogeneity and dynamic nature of cancer complicates target selection. As cancerous cells progress over time, they share fewer characteristics with healthy cells and develop unique characteristics influencing their growth rate, invasiveness, and potential to respond to treatment.6 The pathways involved with these differences are good potential therapeutic targets. However, transformation of healthy cells into cancer cells is a nonlinear process, meaning
that the pathways involved are not always predictable or repeatable from tumor to tumor or patient to patient, even for the same type of cancer.6 So a good target in one tumor might not be present in another at the levels required for efficacy. To overcome some of these challenges, we need systems that allow us to quickly assimilate the scientific evidence associated with disease biology. A few solutions do exist that can help us manage the information overload and streamline evidence integration.
AntibodyTraditionally, ADCs have used full IgG monoclonal antibodies (mAbs) as the vehicle due to their high avidity and favorable pharmacokinetic properties. The antibody needs to bind the target antigen with high specificity and moderate affinity and undergo internalization to release the cytotoxic payload inside the cell. Very high affinity antibodies are not favored, because they are rapidly internalized and degraded,
Figure 1. Central to all immune therapies is boosting the anti-cancer response using the patient’s own immune system. This illustration identifies the main categories of immunotherapeutics based on their mechanisms. Each therapeutic has unique benefits and challenges.
Provoking anti-cancer
immune response
-
4
limiting penetration into solid tumors.7 The antibody isotype is also important, as some isotypes elicit effector functions such as antibody-dependent cellular cytotoxicity (ADCC) or complement-dependent cytotoxicity (CDC). In some cases, these may be advantageous and contribute to efficacy. One example is the antibody trastuzumab. Alone, this antibody targets and kills HER2-positive breast cancer by flagging the cells for attack via ADCC. But this same antibody serves as the vehicle for the ADC Kadcyla, which, in addition to the ADCC, delivers a cytotoxic payload directly to the cancer cells.8 However, if an ADC is supposed to only kill actively dividing cells, cytotoxicity mediated by the antibody vehicle could potentially lead to the death of normal, quiescent tissues as well.2
Around twenty ADCs currently in development use bispecific mAb vehicles, which target two tumor antigens instead of one.2 This approach has potential to increase efficacy and safety, but adds the challenge of identifying two good target antigens instead of one. Also under investigation are engineered antibody fragments such as diabodies for use as the antibody vehicle, with the goal to further improve pharmacokinetic properties.2 Even antibodies with high selectivity for tumor tissues accumulate in tumors with poor efficiency, and presumably, a significant portion of an ADC dose is catabolized outside of the tumor site, potentially exposing healthy tissues to toxic products.9 In murine models, an anti-CD30 diabody-drug conjugate accumulates in tumor tissue faster than the IgG conjugate counterpart9, but whether this observation translates into
increased efficacy in patients remains to be seen.
PayloadMost ADC research to date has used cytotoxic payloads, which elicit their effects by targeting tubulin, DNA, or RNA. Tubulin-binding payloads inhibit microtubule assembly, causing cell cycle arrest and apoptosis.1 These payloads kill dividing cells very efficiently, but can lead to drug resistance in non-dividing cells.10 DNA damaging agents kill both dividing and non-dividing cells, and although there is risk to harm healthy tissues, they are attractive for de-bulking solid tumors that contain high percentages of non-dividing cells.2 RNA-targeting payloads bind to RNA polymerase II, inhibiting mRNA synthesis and protein synthesis, ultimately leading to apoptosis.1,2
Other classes of payloads are also being considered for use in ADCs. Pro-inflammatory cytokines are of particular interest, since they can provoke strong anti-tumor immune responses. Their systemic use has been challenging due to toxicity issues, such as the systemic inflammatory response and multiorgan failure associated with systemic recombinant human tumor necrosis factor (TNF) treatment.11 However, targeting tumors directly using antibody-drug conjugates can potentially limit these effects and increase the therapeutic window for these powerful molecules.12
ConjugationAlthough common payload types have been extensively characterized, there is still much to learn regarding how conjugation variations affect stability
Figure 2. Illustration of a theoretical antibody- drug conjugate showing antibody, linker, and drug.
-
5
and interactions with cellular targets. Most ADCs in development involve conjugating the payload to cysteine or lysine residues on the antibody, generating a heterogeneous ADC population with varying numbers of payloads per antibody.1–3 It is possible that future FDA regulations will require homogeneous ADC production since the purity and potency of the preparation affects the pharmacokinetics and safety profiles of these agents. Uncontrolled conjugation and high ratios of drug to antibody can also negatively influence efficacy, so extensive efforts are underway to control site-specific conjugation using antibody engineering or chemo-enzymatic bioconjugation methods.2
Around 2–4 payloads per antibody is the optimal ratio for efficacy and pharmacokinetics,13 although higher ratios using hydrophilic linker-payload combinations have recently shown success in preclinical models.14,15 Systematic assessment of conjugation sites with different linkers shows that payload positions also affect the linker stability and influence pharmacokinetics differently in mouse and rat models, highlighting again the importance of good predictive models for pre-clinical testing.15
Linker The antibody vehicle is connected to the payload via a linker molecule. Cleavable linkers release the payload upon exposure to lysosomal proteases or low pH environments, while non-cleavable linkers rely on proteolytic degradation of the antibody.1 Payload release can produce antibodies or payloads with residual chemical structures, which may affect
efficacy or toxicity, so use of “traceless” linkers is also under investigation.16
Although the best choice of linker depends on the particular payload and target, the most efficacious combination cannot really be predicted.2 New methods using radiolabeled linkers and payloads may provide a better understanding of ADC metabolism and a systematic approach for linker selection.17
Significant advances for optimizing each of these parameters individually have been made in recent years, and scientists can now design very elaborate ADCs based on our expansive knowledge base. However, successfully developing these great ideas into therapeutics with maximum efficacy and minimum toxicity is still encumbered by a number of challenges.
Challenges and future perspectivesGood in vitro and in vivo models for predicting ADC efficacy or toxicity are limited due to our incomplete knowledge of disease biology and drug action as well as differences between animals and humans. As a result, candidates that work well in preclinical studies are often ineffective or toxic in the clinic.1 Plus the inability to quantify localization of an ADC in tumor and healthy tissue or assess release of the payload makes it impossible to determine the mechanism of action or make adaptations to decrease off-target activity.1 However, new methods for dual-labeling both the antibody and the payload may help solve some of these issues in the future.18
Converting the wealth of known data into actionable insights will improve optimization of these complex combinations and help shift the risk of failure to earlier stages in the development pipeline.
-
6
Furthermore, traditional clinical trials designed for testing small molecule drugs are poorly suited for ADCs and other immunotherapeutics and must evolve to meet special challenges.19,20 Due to disease heterogeneity, not all patients will respond to a particular immunotherapy, so developing predictive biomarkers and methods to determine expression levels of target antigens is critical to identify the correct patient population for testing.21 Dosing is another problem, since determining dose-limiting toxicities is usually not possible after one treatment round, so markers to predict adverse events early are needed for adequate management.19,20
Overcoming all of these challenges to fulfill the exciting potential of ADCs requires developing new technologies and solutions and using our learnings from the past to bridge the gap between our current capabilities and what is yet to come. Creating ADCs is a rapidly evolving technology, and
we are continuously accruing new knowledge from pre-clinical and clinical studies. Every success and every failure is information that can not only open new exploratory and development paths but can also improve decisions about new development paths. Converting this wealth of data into actionable insights will improve optimization of these complex combinations and help shift the risk of failure to earlier stages in the development pipeline. As the understanding of how to successfully combine the right payload with the right antibody and target the right patient group grows so do the possibilities of these intricate therapies.
-
7
Works Cited1. Gébleux, R. & Casi, G. Pharmacology & Therapeutics Antibody-drug conjugates: Current
status and future perspectives. Pharmacol. Ther. (2016). doi:10.1016/j.pharmthera.2016.07.0122. Kim, E. G. & Kim, K. M. Strategies and advancement in antibody-drug conjugate optimization
for targeted cancer therapeutics. Biomol. Ther. 23, 493–509 (2015).3. Bornstein, G. G. Antibody Drug Conjugates: Preclinical Considerations. AAPS J.
17, 525–34 (2015).4. Petersen, B. H., Deherdt, S. V, Schneck, D. W. & Bumol, T. F. The Human Immune Response
to KSl/4-Desacetylvinblastine (LY256787) and KSl/4-Desacetylvinblastine Hydrazide (LY203728) in Single and Multiple Dose Clinical Studies. Cancer Res. 51, 2286–2290 (1991).
5. Tolcher, A. et al. Randomized phase II study of BR96-doxorubicin conjugate in patients with metastatic breast cancer. J Clin Oncol. 17, 478–484 (1999).
6. Grizzi, F. et al. Cancer initiation and progression: an unsimplifiable complexity. Theor. Biol. Med. Model. 3, (2006).
7. Rudnick, S. I. et al. Influence of Affinity and Antigen Internalization on the Uptake and Penetration of Anti-HER2 Antibodies in Solid Tumors. Cancer Res. 71, 2250–2259 (2011).
8. Junttila, T. T., Li, G., Parsons, K., Phillips, G. L. & Sliwkowski, M. X. Trastuzumab-DM1 (T-DM1) retains all the mechanisms of action of trastuzumab and efficiently inhibits growth of lapatinib insensitive breast cancer. Breast Cancer Res. Treat. 128, 347–356 (2011).
9. Kim, K. et al. Anti-CD30 diabody-drug conjugates with potent antitumor activity. Mol. Cancer Ther. 7, (2008).
10. Borst, P. Cancer drug pan-resistance: pumps, cancer stem cells, quiescence, epithelial to mesenchymal transition, blocked cell death pathways, persisters or what? Open Biol. 2, (2012).
11. Lejeune, F. J., Liénard, D., Matter, M. & Rüegg, C. Efficiency of recombinant human TNF in human cancer therapy. 6, 1–17 (2006).
12. Hemmerle, T. et al. The antibody-based targeted delivery of TNF in combination with doxorubicin eradicates sarcomas in mice and confers protective immunity. Br J Cancer 109, 1206–1213 (2013).
13. Hamblett, K. J. et al. Effects of drug loading on the antitumor activity of a monoclonal antibody drug conjugate. Clin. Cancer Res. 10, 7063–7070 (2004).
14. Lyon, R. et al. Self-hydrolyzing maleimides improve the stability and pharmacological properties of antibody-drug conjugates. Nat. Biotechnol. 33, 733–735 (2015).
15. Strop, P. et al. Location matters: Site of conjugation modulates stability and pharmacokinetics of antibody drug conjugates. Chem. Biol. 20, 161–167 (2013).
16. Bernardes, G. J. L. et al. A Traceless Vascular-Targeting Antibody–Drug Conjugate for Cancer Therapy. Angew. Chemie Int. Ed. 51, 941–44 (2011).
17. Kitson, S. L., Moody, T. L., Rozzell, D. & Caswell, J. Antibody-Drug Conjugates (ADCs): Carbon-14 Labelling Requirements. Curr. Opin. Drug Discov. Devel. (2013). at
18. Cohen, R. et al. Development of Novel ADCs: Conjugation of Tubulysin Analogues to Trastuzumab Monitored by Dual Radiolabeling. Cancer Res. 74, 5700–5710 (2014).
19. Postel-Vinay, S. et al. Challenges of phase 1 clinical trials evaluating immune checkpoint-targeted antibodies. Ann. Oncol. 27, 214–224 (2016).
20. Menis, J., Litière, S., Tryfonidis, K. & Golfinopoulos, V. The European Organization for Research and Treatment of Cancer perspective on designing clinical trials with immune therapeutics. Ann. Transl. Med. 4, 267–267 (2016).
21. Diamantis, N. & Banerji, U. Antibody-drug conjugates - an emerging class of cancer treatment. Br. J. Cancer 114, 362–367 (2016).
-
ASIA AND AUSTRALIATel: + 65 6349 0222 Email: [email protected]
JAPANTel: + 81 3 5561 5034 Email: [email protected]
KOREA AND TAIWANTel: +82 2 6714 3000 Email: [email protected]
EUROPE, MIDDLE EAST AND AFRICATel: +31 20 485 3767 Email: [email protected]
NORTH AMERICA, CENTRAL AMERICA AND CANADATel: +1 888 615 4500 Email: [email protected]
SOUTH AMERICATel: +55 21 3970 9300 Email: [email protected]
Copyright© 2017 Elsevier B.V. February 2017
LEARN MORE
To learn more about Elsevier’s R&D Solutions, visit: www.elsevier.com/rd-solutions/pharma-and-life-sciences or contact your nearest Elsevier office.
R&D Solutions for Pharma & Life Sciences
Elsevier’s R&D Solutions is a portfolio of tools that integrate data, analytics and technology capabilities to help pharmaceutical & life sciences customers realize the potential of data-driven drug discovery and development.