![Paclitaxel-coated PTA Balloon Catheter IN.PACT™ Admiral™ · The IN.PACT Admiral paclitaxel-coated PTA balloon catheter is an over-the-wire [OTW] balloon catheter with a drug-coated](https://static.fdocuments.in/doc/165x107/60409071edb91f0df1529500/paclitaxel-coated-pta-balloon-catheter-inpacta-admirala-the-inpact-admiral.jpg)
Drug-Coated Balloon Technologies I: …summitmd.com/pdf/pdf/2026_Granada.pdfDrug-Coated Balloon...
24
Drug Drug Coated Coated Balloon Balloon Drug Drug-Coated Coated Balloon Balloon Technologies I: Technical Technologies I: Technical Technologies I: Technical Technologies I: Technical Considerations and Considerations and Considerations and Considerations and Controversies Controversies Juan F. Granada, MD Juan F. Granada, MD Juan F. Granada, MD Juan F. Granada, MD Executive Director and Chief Scientific Officer Executive Director and Chief Scientific Officer Skirball Center for Cardiovascular Research Skirball Center for Cardiovascular Research Cardiovascular Research Foundation Cardiovascular Research Foundation Columbia University Medical Center, New York Columbia University Medical Center, New York
Transcript of Drug-Coated Balloon Technologies I: …summitmd.com/pdf/pdf/2026_Granada.pdfDrug-Coated Balloon...

DrugDrug CoatedCoated BalloonBalloonDrugDrug--Coated Coated Balloon Balloon Technologies I: TechnicalTechnologies I: TechnicalTechnologies I: Technical Technologies I: Technical
Considerations andConsiderations andConsiderations and Considerations and ControversiesControversies
Juan F. Granada, MDJuan F. Granada, MDJuan F. Granada, MDJuan F. Granada, MDExecutive Director and Chief Scientific OfficerExecutive Director and Chief Scientific OfficerSkirball Center for Cardiovascular ResearchSkirball Center for Cardiovascular Research
Cardiovascular Research FoundationCardiovascular Research FoundationColumbia University Medical Center, New YorkColumbia University Medical Center, New York

Disclosure Statement of Financial InterestDisclosure Statement of Financial Interest
Within the past 12 months, I or my spouse/partner have had a Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with thefinancial interest/arrangement or affiliation with thefinancial interest/arrangement or affiliation with the financial interest/arrangement or affiliation with the organization(s) listed below.organization(s) listed below.
Affiliation/Financial RelationshipAffiliation/Financial Relationship CompanyCompany•• Grant/Research SupportGrant/Research Support•• Consulting Fees/HonorariaConsulting Fees/Honoraria•• Major Stock Shareholder/EquityMajor Stock Shareholder/Equity
•• BSCI, Abbott, BSCI, Abbott, MedradMedrad, Caliber, Caliber•• MedradMedrad•• VNTVNT
Affiliation/Financial RelationshipAffiliation/Financial Relationship CompanyCompany
Major Stock Shareholder/EquityMajor Stock Shareholder/Equity•• Royalty IncomeRoyalty Income•• Ownership/FounderOwnership/Founder•• Intellectual Property RightsIntellectual Property Rights
VNTVNT
p y gp y g•• Other Financial BenefitOther Financial Benefit

Mechanism of Mechanism of Drug Delivery and Drug Delivery and Restenosis PreventionRestenosis PreventionRestenosis PreventionRestenosis Prevention
Can a drug delivered locally onlyCan a drug delivered locally onlyCan a drug delivered locally, only Can a drug delivered locally, only one time and without a controlled one time and without a controlled delivery system achieve longdelivery system achieve long--termtermdelivery system achieve longdelivery system achieve long term term
biological efficacy? biological efficacy?

Mechanism of Drug Delivery and Mechanism of Drug Delivery and Restenosis PreventionRestenosis PreventionRestenosis PreventionRestenosis Prevention
DEB 10sBMS
Effect of Carrier on Effect of Carrier on Paclitaxel TransferPaclitaxel Transfer
Cremers B. Thromb Haemost. 2009 Jan;101(1):201-6
TaxusCoated
“Hydrophilic Carriers “Hydrophilic Carriers I P lit lI P lit l
TaxusCoated Balloon
Increase Paclitaxel Increase Paclitaxel Transfer”Transfer”
Cremers B. Cath Cardiov Int. April 2012
Long Term HealingLong Term Healing

PACCOCATH PACCOCATH ISRISR–– F/U F/U 5 Years Follow Up5 Years Follow UpLongLong Term FollowTerm Follow Up AfterUp AfterLongLong--Term FollowTerm Follow--Up After Up After Treatment of Coronary InTreatment of Coronary In--Stent Stent Restenosis With a PaclitaxelRestenosis With a Paclitaxel
ISRRestenosis With a PaclitaxelRestenosis With a Paclitaxel--Coated Balloon CatheterCoated Balloon Catheter
Target Lesion Revascularization
Scheller B, JACC Scheller B, JACC IntvIntv 2012;5:3232012;5:323--3030
4 Years F/u37 37
38.935
40
45
Target Lesion Revascularization
37 37
20
25
30
35
rcen
tage
PCB
69.3
5
10
15
20
Per
Control
4 60
12 Months 2 Years 5 Years

PCB Efficacy in BMSPCB Efficacy in BMS--ISR is ISR is ReproducibleReproducible in FIH Clinical Trialsin FIH Clinical Trials
0.9
ReproducibleReproducible in FIH Clinical Trials in FIH Clinical Trials 86% RRR PEPPER Study (Biotronik)
0.7
0.8
0.9
s (%
) PCB Control0.80±0.79 • 81 patients
• 47% DES-ISR.• LL: 0.07 mm.
0.5
0.6
Res
teno
si
0.45±0.68
(Taxus)
55% RRR 126 PatientsBMS-ISR= 52% DES-ISR= 48% ISR + SV (< 2 5mm) 54%
0.3
0.4
t Bin
ary
R
0.31±0.22
ISR + SV (< 2.5mm) 54%ISR + Bifurcation 29%
0.1
0.2
-Seg
men
t
0.11±0.44
0 02 0 0
0.20±0.450.16±0.40
N 54 N 54N= 23
-0.1
0PACOCCATH I/II INPACT ISR PEPCAD II PERVIDEO I Spanish Registry
In- -0.02±0.50N=54 N=54 N=66 N=65 N=39 N=34
(Medrad) (Medtronic) (BBraun) (Lutonix) (Eurocor)

Impact of Drug Retention (PK) on Impact of Drug Retention (PK) on Vascular Toxicity and EfficacyVascular Toxicity and EfficacyVascular Toxicity and EfficacyVascular Toxicity and Efficacy
T
Paclitaxel-Eluting Stents in Clinical Trials)
TOXI
C
EFFE
CT
100Typical DEB
clita
xel
n (n
g/m
g)
PEU
TIC
DO
WIMPROVE IMPROVE EFFICACYEFFICACY
ypCurve
rter
ial P
acce
ntra
tion
THER
AP
WIN
DFormulation BDESFormulation A
DES5
Ar
Con
c
ECT
1
NO
EFF
E
25 10050 75
REDUCE REDUCE COMPLICATIONSCOMPLICATIONS
00
Time (Days)25 10050 750

Local Local Tissue Effects (Safety)Tissue Effects (Safety)Vascular Healing According to DosVascular Healing According to Dosee
1= Minimal
Vascular Healing According to DosVascular Healing According to Dosee
Delayed Endothelialization2.17
1.75
1 5
2
2.5
core
Fibrin (Endothelial + Medial)
1.2
1.71.95
1.5
2
2.5
Scor
e
2= Slight3= Moderate4= Marked
1 1
0
0.5
1
1.5M
ean
Sc 11.2
0
0.5
1
Mea
n S5= Massive
UncoatedControl 2x 4x 6x Control 2x 4x 6x
IEL Rupture Presence Amorphous Material
Uncoated
IEL Rupture
2 21.62
2.5
1.52
2.53
n Sc
ore
2.87
1.8722.5
33.5
Scor
e
Cotavance(1x)
00.5
1
Control 2x 4x 6x
Mea
n
0
1
00.5
11.5
Mea
n Cotavance
(6x)
Control 2x 4x 6x Control 2x 4x 6x
Histology picture obtained from CVPath

Mechanism Mechanism of Action of of Action of DCB: Impact DCB: Impact on Drugon Drug Retention and EmbolizationRetention and Embolizationon Drug on Drug Retention and EmbolizationRetention and Embolization
1000
mg
Luminal Surface Vessel Acute Drug Transfer
0
1 H 24 H 7 D 28 D
ng/mMicro-Particles
Macro-Particles
1 Hour 24 Hour 7 Day 28 Day
•• Most of Paclitaxel remains on the vessel Most of Paclitaxel remains on the vessel surfacesurface
Acute Drug Transfer
Distal Circulation*~60 to 70%
surfacesurface•• This “drugThis “drug--reservoir” creates a gradient reservoir” creates a gradient and serves as the source for sustained and serves as the source for sustained drug deliverydrug delivery
Tissue Transfer*~1 to 10%
drug deliverydrug delivery•• Once the drug is transferred to the media Once the drug is transferred to the media of the vessel, tissue clearance depends on of the vessel, tissue clearance depends on well described PK curveswell described PK curveswell described PK curves well described PK curves

Distal Washout of Paclitaxel Coating Distal Washout of Paclitaxel Coating
Distal Tissue Effect Distal Tissue Effect (Embolization)(Embolization)•• Acute Ischemic Events (CLIAcute Ischemic Events (CLI))
Ch i Ti Eff tCh i Ti Eff t•• 120 x 7 mm120 x 7 mm•• Paclitaxel Coated BalloonPaclitaxel Coated Balloon•• ?% of Systemic Concentration?% of Systemic Concentration
•• Chronic Tissue EffectsChronic Tissue Effects•• Other Organs ToxicityOther Organs Toxicity
•• % of Drug Clearance?% of Drug Clearance?•• % Chronic Tissue Retention?% Chronic Tissue Retention?

Paclitaxel Formulation TypesPaclitaxel Formulation TypesImpact on Biological PerformanceImpact on Biological PerformanceImpact on Biological PerformanceImpact on Biological Performance
Coating “B” AmorphousCoating “B” AmorphousCoating “A” CrystallineCoating “A” CrystallineCrystalline Amorphous
Particles Released +++ ++Uniform Coating ++ +++Drug Transfer to Vessel +++ ++Drug Transfer to Vessel +++ ++Drug Retention vs. Time +++ +Biological Effectiveness +++ ?g

Tissue Transfer and RetentionTissue Transfer and RetentionCrystalline versus Amorphous CoatingsCrystalline versus Amorphous CoatingsCrystalline versus Amorphous CoatingsCrystalline versus Amorphous Coatings
Tissue Drug Concentration (%)Tissue Drug Concentration (%)
100.00EFFECTIVE
50.00
25.00
12.50
Crystalline Coating 1: higher uptake, higher retention
Crystalline Coating 2: lower uptake, higher retention
6.25
3.13
3.06
1h 24h 7d 28d
3.06
1.53
0.77
0 38
Amorphous Coating 3: higher uptake, lower retention
1h 24h 7d 28d
Time
0.38
0.19
0.10
SAFE

Second Generations CoatingsSecond Generations CoatingsPaclitaxel Coated Balloon TechnologiesPaclitaxel Coated Balloon TechnologiesPaclitaxel Coated Balloon TechnologiesPaclitaxel Coated Balloon Technologies
First generation DCBFirst generation DCBFirst generation DCB First generation DCB technologies have already technologies have already migrated into their secondmigrated into their second•• Manual dipping processManual dipping process migrated into their second migrated into their second generation providing more generation providing more precise coatings, tissue drug precise coatings, tissue drug
•• Automated and controlled Automated and controlled drug coatingdrug coating
delivery and lower delivery and lower particulate count… particulate count…
•• Inconsistent D:E mixtureInconsistent D:E mixture•• Improved coating mixture Improved coating mixture and uniformityand uniformityand uniformityand uniformity
••Limited scale productionLimited scale production••Large scale reproducibilityLarge scale reproducibility••Large scale reproducibilityLarge scale reproducibility

Fact#1:Fact#1: Limited Evidence Based Limited Evidence Based Medicine Leading to Clinical PracticeMedicine Leading to Clinical Practice
RCT of PCB for the Treatment of De Novo SFA Disease (ITT= PTA Only)RCT of PCB for the Treatment of De Novo SFA Disease (ITT= PTA Only)
Medicine Leading to Clinical PracticeMedicine Leading to Clinical Practice
0.61-0.05
PACIFIER(Medtronic)(Medtronic)
N=45“Still less than “Still less than
0.461.09LEVANT I
POBAN=35N=39(Lutonix)(Lutonix)
( )( )several several hundred hundred
0.30.8Fem-PAC PCBN=34
N=31(Medrad)(Medrad)patients having patients having 6 month 6 month
0.41.7Thunder N=48
N=41(Medrad)(Medrad)angiographic angiographic data and long data and long
-0.5 0 0.5 1 1.5 2
Angiographic Late Loss (mm)
term follow up” term follow up”

Fact #2:Fact #2: PCB May Have Limited PCB May Have Limited Efficacy in DESEfficacy in DES ISRISR
BMS ISR 157 P ti t
Efficacy in DESEfficacy in DES--ISR ISR
• DIOR II PCB Technology (3 µg/mm2)
BMS-ISR: 157 Patients.DES-ISR: 83 Patients.Frequency of Stent Implantation 4.9%DIOR II PCB Technology (3 µg/mm )
• 40.6% Diffuse ISR• Length Covered by PCB 24±9.1 mm• Follow Up: 228 ± 44 days (97.6% of Patients)
1214 13,4
12,2
q y p %• In.Pact Falcon (Medtronic)• 75 patients, 122 lesions
ISR 62 7%
4681012
9,8
5,97,2
9,8
BMS
• ISR 62.7%• Diffuse disease 34.7%
• Death/MI/TVR: 13.3%Angiographic Follow Up (63 9%):
024 2
1,32,6
01,2 1,2 1,2 1,2
BMS
DES• Angiographic Follow Up (63.9%):
• Restenosis 30.8%• DES-ISR: 47.5%• BMS ISR: 0%• BMS-ISR: 0%• De Novo: 16.1%
J Shannon, TCT-14, TCT2011

Fact #3:Fact #3: A PTA Balloon is Not An Ideal A PTA Balloon is Not An Ideal Platform (A Stent May Be Needed!)Platform (A Stent May Be Needed!)
PTA study (2002)PTA study (2002)
Platform (A Stent May Be Needed!)Platform (A Stent May Be Needed!)PTA study (2002)PTA study (2002)
74 patients74 patients43% major dissections43% major dissections32% residual stenosis >30%32% residual stenosis >30%
ABSOLUTE: Stent vs. PTA (2006)ABSOLUTE: Stent vs. PTA (2006)104 patients, 1:1 randomization104 patients, 1:1 randomization32%32% insufficient PTA result led to insufficient PTA result led to cross cross over to stentover to stentover to stentover to stent
RESILIENT: Stent vs. PTA (2008)RESILIENT: Stent vs. PTA (2008)206 patients 2:1 randomization 206 patients 2:1 randomization 40% PTA 40% PTA cross over to stentcross over to stent due to flow limiting due to flow limiting
Expansion in path of least resistanceExpansion in path of least resistanceSignificant shear stress and traumaSignificant shear stress and trauma
Expansion mechanism leads to:Expansion mechanism leads to:
ggdissections and residual stenosisdissections and residual stenosis
Pacifier: DEB vs. PTA (2011)Pacifier: DEB vs. PTA (2011)91 patients, 1:1 randomization91 patients, 1:1 randomization
Significant shear stress and traumaSignificant shear stress and traumaHigh dissection rateHigh dissection rateElastic recoilElastic recoilAbrupt closureAbrupt closure
21% and 35%21% and 35% bail out stenting due to bail out stenting due to flow limiting dissections and residual flow limiting dissections and residual stenosisstenosis
Abrupt closureAbrupt closure
Acute failure reported in ~30 - 40% of PTA case requiring additional treatment
Slide (modified) courtesy of Eitan KonstantinoSlide (modified) courtesy of Eitan Konstantino
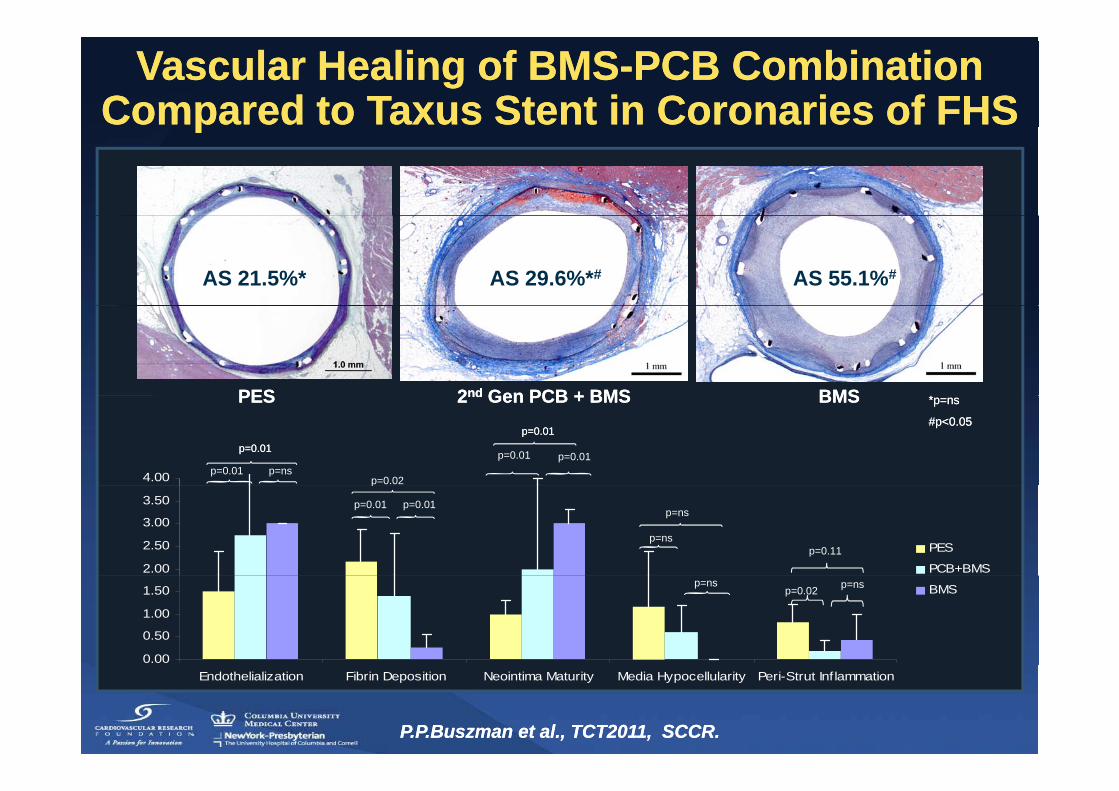
Vascular Healing of BMSVascular Healing of BMS--PCB Combination PCB Combination Compared to Taxus Stent in Coronaries of FHSCompared to Taxus Stent in Coronaries of FHSpp
AS 21.5%* AS 29.6%*# AS 55.1%#
PESPES 22ndnd Gen PCB + BMSGen PCB + BMS BMSBMS **PESPES 22ndnd Gen PCB + BMSGen PCB + BMS BMSBMS
p=nsp=0.01
p=0.01p=0.01
p=0.02
p=0.01
p=0.01p=0.01
p=0.01
4.00
*p=ns*p=ns
#p<0.05#p<0.05
p=0.01p=0.01
p
p=ns
p=nsp=0.11
2.00
2.50
3.00
3.50
PES
PCB+BMSp=ns
p=0.02 p=ns
0.00
0.50
1.00
1.50 BMS
P.P.BuszmanP.P.Buszman et alet al., TCT2011, SCCR. ., TCT2011, SCCR.
Endothelialization Fibrin Deposition Neointima Maturity Media Hypocellularity Peri-Strut Inflammation

Primary Effectiveness Outcomes Provisional BMS versus DESy
“It is possible that in selected cases and due to the scaffolding effect, peripheral DES may be more effective g , p p y
than PCB…then if we are obliged to migrate into a combined approach (PCB + BMS), PCB use will be
restricted to longer lesions and smaller vascular territories”
Dake M D et al. Circ Cardiovasc Interv 2011;4:495Dake M D et al. Circ Cardiovasc Interv 2011;4:495--504504

Fact #4: Fact #4: SirolimusSirolimus AnaloguesAnalogues• Rapalogs provide well-established therapeutic benefit• Rapalogs provide high level of safety – DES “drug of choice”• PTX chosen for DEB because tissue transfer/absorption is far simpler• So why we do not use them?
19

Paclitaxel Irreversibly Inhibits Arterial SMC
Tissue Distribution and Retention of Paclitaxel Make
Proliferation and Migration Using a Single Dose
it an Ideal Agent for Local Drug Delivery
Control (hSMC)(+) anti–ß-tubulin
Sirolimus
P lit l (hSMC)
Sirolimus
PaclitaxelPaclitaxel (hSMC)
(+) anti–ß-tubulin Dextran
A L i t l P N tl A d S i USA 2004 101
Axel DI. Circulation. 1997;96:636-645
A. Levin et al., Proc Natl Acad Sci USA, 2004, 101, 9463-9467.

Drug Eluting Balloon Nanoparticle Based Drug Eluting Balloon Nanoparticle Based ((Si liSi li ) B ll Dil t ti S t) B ll Dil t ti S t((SirolimusSirolimus) Balloon Dilatation System) Balloon Dilatation System
Nanoparticle delivery technology• Enhanced tissue penetration• Protection from rapid degradation
Angioplasty balloon dilation systemAngioplasty balloon dilation system•• Fully integrated combination deviceFully integrated combination device•• SemiSemi--compliant ballooncompliant balloonp g
• Controlled and sustained release• Complete degradation
pp•• Full range of sizes and diametersFull range of sizes and diameters
Regular dilatation pressures plus Sirolimus
nanoparticle delivery
21 Slide courtesy (modified) of Caliber TherapeuticsSlide courtesy (modified) of Caliber Therapeutics

Elution Control and Dose FeasibilityElution Control and Dose FeasibilitySirolimusSirolimus Delivery Using a Porous BalloonDelivery Using a Porous BalloonSirolimusSirolimus Delivery Using a Porous BalloonDelivery Using a Porous Balloon
Tissue PK at 28 Days Following Sirolimus Delivery
Slide courtesy (modified) of Caliber TherapeuticsSlide courtesy (modified) of Caliber Therapeutics

Opportunities for ImprovementOpportunities for ImprovementB ll S f M difi tiB ll S f M difi tiSIROLIMUSSIROLIMUS
DEB Nanoparticle Based DEB Nanoparticle Based Balloon Dilatation System Balloon Dilatation System
(CALIBER)(CALIBER)
Balloon Surface ModificationBalloon Surface ModificationTechnologiesTechnologies
(AVIDAL)(AVIDAL)(CALIBER)(CALIBER)
DCB Microcrystalline Coating DCB Microcrystalline Coating (MICELL)(MICELL)
Dedicated DCB Platforms Dedicated DCB Platforms (QUATRO)(QUATRO)(MICELL)(MICELL) (QUATRO)(QUATRO)
Illustrative spot analysis by TOF‐SIMS
DCB Nanocrystalline Coating DCB Nanocrystalline Coating (CMI)(CMI)
Niche DCB Platforms Niche DCB Platforms (CONIC)(CONIC)( )( )

DCB ConclusionsDCB Conclusions•• PCB are technological suited to become the ideal interventional PCB are technological suited to become the ideal interventional
tool for the treatment of ISR and SFA diseasetool for the treatment of ISR and SFA disease•• Although efficacious for the treatment of BMSAlthough efficacious for the treatment of BMS ISR its overallISR its overall•• Although efficacious for the treatment of BMSAlthough efficacious for the treatment of BMS--ISR, its overall ISR, its overall
efficacy to treat DESefficacy to treat DES--ISRISR needs to be further studied needs to be further studied •• The DCB+BMS combination may lead to similar DESThe DCB+BMS combination may lead to similar DES--like clinical like clinical
outcomes (i eoutcomes (i e stent thrombosisstent thrombosis)) Then the synergistic use ofThen the synergistic use ofoutcomes (i.e., outcomes (i.e., stent thrombosisstent thrombosis)). Then, the synergistic use of . Then, the synergistic use of these devices deserves further investigation in a prospective these devices deserves further investigation in a prospective manner manner
•• Second generation PCBs appear to offer impro ed coatingSecond generation PCBs appear to offer impro ed coating•• Second generation PCBs appear to offer improved coating Second generation PCBs appear to offer improved coating platforms providing more precise drug transfer to the tissueplatforms providing more precise drug transfer to the tissue
•• However, there is still a lot of room for improvement in regards However, there is still a lot of room for improvement in regards p gp gto dosing, method of transfer and PK behaviorto dosing, method of transfer and PK behavior
•• Emerging data involving competitive devices (i.e., DES) will Emerging data involving competitive devices (i.e., DES) will determine the clinical applicability of DCB in thedetermine the clinical applicability of DCB in the cathcath--lablabdetermine the clinical applicability of DCB in the determine the clinical applicability of DCB in the cathcath lablab
•• However, the DCB field has reached a feasibility phase, is However, the DCB field has reached a feasibility phase, is rapidly evolving and is here to stay for the long runrapidly evolving and is here to stay for the long run