Dr Tharani Nitkunan, consultant urologist Dr Alison Tree ...€¦ · hormone therapy for prostate...
97
Consequences of prostate cancer treatment Dr Tharani Nitkunan, consultant urologist Dr Alison Tree, consultant oncologist
Transcript of Dr Tharani Nitkunan, consultant urologist Dr Alison Tree ...€¦ · hormone therapy for prostate...

Consequences of
prostate cancer
treatment Dr Tharani Nitkunan, consultant urologist
Dr Alison Tree, consultant oncologist

COI
Alison Tree
• Honoraria from Ferring (Degarelix), Astellas, Janssen and
Bayer
• Research funding from Elekta, MSD and Accuray
Tharani Nitkunan
• Honoraria from Astellas, Allergan and Contura International

Overview of this session
• Brief summary of the logistics of radiotherapy, surgery and
hormone therapy for prostate cancer
• How to manage the consequences of treatment (case studies)
1. Lower urinary tract consequences
2. Bowel consequences
Break for questions
3. Erectile dysfunction
4. Androgen deprivation therapy side effects and management
strategies

When to treat prostate cancer
Low-risk Intermediate-risk High-risk
PSA <10ng/ml 10-20ng/ml >20ng/ml
Gleason score/ISUP Gleason < 7/ISUP Grade 1
Gleason 7/ISUP Grade 2/3
Gleason >7/ISUP Grade 4/5
Clinical stage cT1-2a cT2b cT2c
ISUP (International Society of
Urological Pathology 2014 grades)
Gleason
1 2-6
2 7 (3+4)
3 7 (4+3)
4 8 (4+4 or 3+5 or 5+3)
5 9-10

Radiotherapy- myth busting
• Equivalent to surgery for cancer cure

Radiotherapy myth-busting

Logistics
• Start ADT first
• Once PSA has dropped to around 1, start planning
radiotherapy
• For prostate radiotherapy insert gold seeds into prostate for
image guidance (like TRUS but faster)

Risks
• Pain
• Bleeding (GI, GU, Haematospermia)
• Infection
• Rectal swab, targeted antibiotics
• IF FEVER – STRAIGHT TO A +E, NEED IV Abx (risk 0.3%)
8

• CT scan (possibly MR scan) 1 week after seeds inserted)
• Whole radiotherapy planning pathway takes around 4 weeks,
but patient only needed twice

Daily treatment – used to be 7.5 weeks,
now mostly 4 weeks, ??soon 5 days 10

Quick discussion
• If you were going to have prostate radiotherapy, what would
you be most worried about?

Daily treatment
• Fill bladder, may use enema
• Change into gown
• Patient lies on the couch
• Radiographers line up to pin-point tattoos
• Mini-CT (called cone beam CT)
• Shift patient to ensure prostate exactly aligned
• Radiographers leave the room – patient is alone
• Treat – takes about 2 minutes with VMAT
• Patient goes home, no restrictions on lifestyle

1 slide on PSA follow up
• PSA should be checked 6 monthly until 5 years after
radiotherapy
• Annually thereafter
• After radiotherapy, PSA “failure” occurs at nadir PSA+2 ng/ml
• Actually easier to say 2 ng/ml in general
• Off ADT Testosterone will usually return to normal, PSA will rise
a little. Don’t panic.
• Any questions about PSA – please write to us or call us. If
unsure, repeat PSA in 3 months.

Surgery

Surgery
Eradicate cancer
Preserve continence
Preserve potency
RALP = robot-
assisted laparoscopic
prostatectomy

Surgery – pre-operative preparation
Surgical counselling
Patient seminar

Surgery – pre-operative preparation
Pelvic floor muscle training
• hammock of muscles
• 10 squeezes 3x/d
Exercise
• 30mins 5x/week
Avoid driving 2-4 weeks after surgery
No high impact exercises for 6 weeks
Ensure no constipation

Surgery
Apical dissection
Posterior Reconstruction
Anatomy- Membranous urethral length
Previous LUTS
Experience
Retzius Sparing
Nerve-sparing
• Contraindicated in high risk of extracapsular disease
• cT2c or cT3 PCa,
• any GS > 7 on biopsy

Surgery – Post-operative care
Home at 24-48 hours
Catheter for 7-10 days
Analgesia
Ensure bowels opening
VTE prophylaxis
• Low molecular weight heparin
• TED stocking 28 days

Surgical complications – BAUS
• No semen all
• Erectile dysfunction (incl penile shortening) almost all
• Incontinence 3-5%
• Bleeding req transfusion or further surgery 2-10%
• Urinary leak 2-10%
• Pain, infection or hernia of port sites 2-10%
• Lymph node collection 2-10%
• Anaesthetic complications 0.5-2%
• Conversion to open surgery 1%
• Rectal injury 0.5-2%

Surgical complications - Potency
• Bilateral nerve sparing and good prior erectile function
• Men <60 yrs - 75% recovery
• Men >60yrs – 50% recovery
• Negative factors – obesity, diabetes, hypertension, poor pre-
operative erections
Cahill personal communication

Surgical complications - Continence
Causes
• Stress urinary incontinence 32-100%
• Sphincter incompetence 40-92%
• Urethral sphincter length >15mm – less incontinence
• Detrusor overactivity 4-40%
• Detrusor compliance 12-82%
• Stricture 24-67%

Surgical complications - Continence
• 4-8% rates of incontinence
• Better with time
• 12months

PSA follow-up post radical surgery
• 2 consecutive PSA rises >0.2ng/ml
• PSA should be undetectable within six weeks post surgery
• Rapidly increasing PSA suggests distant metastases
• Slowly increasing PSA suggests local recurrence.

ADT


When do we give ADT?
• With radiotherapy – increases cure rates
• In metastatic disease – prolongs survival

Castration
28


LHRH Agonists/analogues eg
Zoladex/Prostap/Decapeptyl
• Castrate testosterone levels achieved in around 2 weeks
• May raise testosterone in first 1-2 weeks (potential for tumour
flare). Co-treatment with Bicalutamide for first month necessary.
• Equivalent efficacy to castration in trials
• Licensed preparation
Goserelin (Zoladex) 3.6mg q 4w or 10.8mg q 12w
Leuprorelin (Prostap) 3.75mg q 4w or 11.25mg q 12w
Triptorelin (Decapeptyl) monthly, 3 or 6 monthly
• Nearly everyone responds

How to start ADT - usually
• Bicalutamide 150mg od for 28 days
• LHRH analogue injections starting 7-14 days after starting
Bicalutamide
• Start monthly, can switch to 3 monthly preparations if long term
ADT is required
• Caution
– Uncontrolled cardiac disease (ischaemic or failure)
– Diabetics with poor control

When 1 month and when 3 month
depots?
• Total length of ADT in localised disease depends on risk
• 3 month depots – 9 months to testosterone recovery
• Good risk – 6 months
• Locally advanced/node positive – 3 years
• Metastatic – lifelong

Side effects of LHRH analogues
• Hot flushes
• Fatigue
• Loss of muscle bulk
• Loss of libido and ED
• Mood change
• Insulin resistance
• Cardiac effects?
• Osteoporosis
• Acupuncture, MPA,
Tamoxifen
• Exercise
• Exercise
• Not much ?vacumn pumps
• Monitor BM
• BP, cholesterol, Exercise
• Start Alendronate

NICE guidance on Osteoporosis

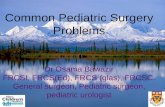
Degarelix effect on testosterone levels
Van Poppel EU (54) 805-815, 2008

Overall survival
Klotz et al, Eur Urol 66, 1101-1108, 2014
37 deaths in
all, 4 due to
prostate cancer

Patients with a history of CV disease (n=708)
Risk of cardiac event or death
Degarelix
6.5%
LHRHa
14.7 %

NICE guidance
“Degarelix is recommended as an option for treating advanced
hormone- dependent prostate cancer in people with spinal
metastases, only if the commissioner can achieve at least the
same discounted drug cost as that available to the NHS in June
2016.”
Reality in my experience – Degarelix started in hospital for those
with spinal mets, switched to random LHRH, often without
Bicalutamide cover, in the community.


LUTS management

Urinary incontinence

LUTS management
• When do you talk about LUTS in your patient cohort– Pre- treatment
– Post-treatment
• History
• Investigations
• Management
• Cases

History - LUTS
• Storage
– Frequency
– Nocturia
– Urgency
– Urge incontinence
Voiding–Hesitancy–Straining to void–Stop/start flow–Incomplete emptying
Post-micturition dribbling
Red flag symptoms

History
• Stress incontinence
• Pad use
• How much does this affect your life?
• Fluid intake - caffeine
• Bowels

Assessment
Frequency/volume chart
Uroflowmetry
IPSS or EPIC

IPSS/EPIC
• EPIC
• expanded prostate cancer index composite
• 5 questions on urinary symptoms
• Other domains – bowel function/ sexual function
• IPSS
• 7 questions on symptoms + 1 quality of life question

EPIC
1. Over the past 4 weeks, how often have you leaked urine?
More than once a day/About once a day/More than once a week/About once a week/Rarely or never
2. Which of the following best describes your urinary control during the last 4 weeks?
No urinary control whatsoever/Frequent dribbling/Occasional dribbling/Total control
3. How many pads or adult diapers per day did you usually use to control leakage during the last 4 weeks?
None/1 pad per day/2 pads per day/3 or more pads per day
4. How big a problem, if any, has each of the following been for you during the last 4 weeks?
Dripping or leaking urine /Pain or burning on urination/Bleeding with urination/ Weak urine stream or incomplete emptying/ Need to urinate frequently during the day
5. Overall, how big a problem has your urinary function been for you during the last 4 weeks?
No problem/Very small problem/Small problem/ Moderate problem/Big problem

IPSS
Score:
1-7 mild
8-19 moderate
20-35 severe

IPSS
Quality of life question
If you were to spend the rest of your life with your urinary
condition just the way it is now, how would you feel
about that?
0 delighted, 1 pleased, 2 mostly satisfied, 3 mixed, 4
mostly dissatisfied, 5 unhappy, 6 terrible

Urine dipstick
Signs of UTI – wcc and nitrites
Haematuria – to follow haematuria pathway

Diagnosis
History Anatomy
Storage Bladder• Bladder compliance
• Detrusor overactivity
Voiding Urethra
• Stricture
• Stress urinary incontinence

Voiding
• Tamsulosin 400mcg od
• Offer finasteride or a 5alpha reductase inhibitor to men
with prostate volumes >30g or PSA >1.4ng/ml

Management of storage symptoms
Bladder training, caffeine reduction
Antimuscarinics
Mirabegron
Combinaton
Botox

Management of storage symptoms
- bladder training

Antimuscarinics
NICE guidelines
• Offer one of the following
oxybutynin immediate release or
tolterodine immediate release or
darifenacin
• If the first treatment is not effective or well tolerated, offer
another drug with the lowest acquisition cost.
• Do not offer oxybutynin immediate release to frail elderly

Antimuscarinics – per NICE
• Offer one of the following
oxybutynin immediate release or £1.76 to £1.06
tolterodine immediate release or £1.18
darifenacin. £30.58
• If the first treatment is not effective or well tolerated, offer
another drug with the lowest acquisition cost.
Trospium chloride XL (Regurin XL 60mg) £23
Fesoterodine (Toviaz 4 and 8mg) £28.62
Solifenacin (5 and 10mg) £29.70 to £38.64

Antimuscarinics
Risks
• Increase in cognitive impairment
• OR=1.45, 95% CI 1.16 to 1.73
• Increase in falls
• all-cause mortality relative to score on the Anticholinergic
Cognitive Burden (ACB) scale
• a system that scores drugs with anticholinergic effects from 1 (possible
anticholinergic effects based on in vitro data) to 3 (known anticholinergic
effects that may cause delirium).
• an increase of 1 point on the scale approximately doubling risk (OR=2.06,
95% CI 1.82 to 2.33)

Mirabegron
• Beta 3 adrenoceptor agonist
• Enables bladder relaxation
• £27.06
• SCORPIO - RCT comparing mirabegron to tolterodine XL
4mg and placebo for 12 weeks4
• Reduced number of incontinence episodes and micturition
episodes
• contraindicated in severe uncontrolled hypertension (systolic
blood pressure ≥180 mm Hg or diastolic blood pressure ≥110
mm Hg, or both)

Investigations – flow rate and scan

Flow rate and scan

Urodynamics


Urinary incontinence - management
History Anatomy Management
Storage Bladder• Bladder compliance
• Detrusor overactivity
Intradetrusor Botox
Clam cystoplasty
Urinary diversion
Voiding Urethra Urethral stricture Optical urethrotomy
Stress urinary
incontinence
Pelvic floor muscle training
Sling
Artificial urinary sphincter

Case 1
Mr AK 76
Locally advanced CaP, DXT (ProSpare Trial) in 2011
Hypertension, NIDDM
Referred in April 2014
Storage LUTS and penile tip pain
Solifenacin 20mg od and on tamsulosin
Voids 2 hly day and nigh
GA cystoscopy 2013 normal.

Case 1
Changed to regurin
Some improvement
Changed to Mirabegron
Urodynamics

Case 1
Not obstructed on CMG, DO only
Reflux bilaterally to mid ureter at 90mls
MDT
Combination treatment – mirabegron + Regurin
Ensure regular USKUB
Content with LUTS

Case 2
Mr RR 77
DXT for CaP 2011 Gleason 4+5 5/12 T2N0, PSA
7.3
Urgency and Frequency
Urodynamics
Botox
Worked well
Botox Nov 2012, Sept 2015, Nov 2016

Case 3
Mr AW 84
Prostate brachytherapy 2006
LHRH analogues since 2009
Bicalutamide 2013
Dexamethasome Nov 2013- Aug 2015
CRPC
Frequency, urgency, weak stream, urge incontinence
D – 15, N- 4
IPSS QoL 5/6

Started on Tamsulosin at RMH – helped Sx
Started on Fesoterodine
Bladder diary and uroflowmetry
Residual
166ml

Case 3
TURP March 2016
Less frequent and urgent but more
incontinence
Urodynamics
Cystoscopy + urethral dilation Nov 2016
Rigid small prostate
Short bulbar stricture
Normal bladder

Case 4
Mr AP 67
RARP
Stress urinary incontinence
Pelvic floor muscle training
Male sling or artificial urinary sphincter
Boston Scientific

Bowel symptoms

Case history
• 72 year old man
• PSA 18, Gleason 4+4 (Grade group 4), T3a (capsular invasion)
N0M0 prostate cancer
• Radical radiotherapy 2 years ago – 60 Gy in 20 fractions
• PSAs well controlled around 0.5 ng/ml
• Now in GP PSA follow up
• Comes to see you with a 6 week history of flecks of blood on
the toilet paper
• Since radiotherapy minor increase in bowel frequency (2/day).
• No other symptoms

Please discuss – 5 minutes
• Correct investigation and management of this
• Most likely causes
• Appropriate treatments for these

2 week rule always applies (first time
round)
• Use usual referral criteria
• Most likely he has rectal telangiectasia from previous
radiotherapy
• Often require no treatment
• If persistent or heavy bleeding, can use sucralfate enemas,
formalin application.


Severe rectal telangiectasia

Same patient comes back 2 years later
• Bleeding has spontaneously improved, but now has loose
stools 3-4 times per day coming on gradually over the last 12
months.
• Some faecal urgency
What do you do?

5 min break and/or
questions

Erectile dysfunction


Erectile dysfunction
Pre-procedural potency is important
History
• Sexual function using IIEF (International Index of Erectile
Function)
• Medical history
• Assess cardivascular risk

Erectile dysfunction – cardiovascular
risk
Low risk – treat ED
High risk – refer to cardiologist

Erectile dysfunction
Diagnostic tests
• Glucose-lipid profile
• Testosterone
Management
• Lifestyle changes and risk factor modification
• manage hypertension, diabetes, weight

Erectile dysfunction – PDE5 inhibitors
• Viagra (Sildenafil), Levitra (Vardenafil), Cialis (Tadalafil)
• Cause smooth muscle relaxation – vasodilation
• How to take them
• Take at lease 30 minutes before sexual activity (45 mins for Viagra).
• Avoid heavy meals 2 hours prior to taking Viagra (not a problem with Cialis).
• Will require sexual stimulation / intimacy to acquire an erection.
• May require up to 8 doses to gain optimum effect (on separate days).

Side effects

Vacuum constriction device
• Blood drawn into the penis using a vacuum device and
constriction ring
• Blood drawn into the penis using a vacuum device and
constriction ring
• Works within 5-6 minutes
• Effective in patients that cannot have PDE5 inhibitors
• Advantages – suitable for most patients,

Intracavernosal injection therapy
• Alprostadil (Caverejct)
• Relaxes smooth muscle increasing blood flow to the penis
• As the penis engorges it compresses venules preventing outflow
of blood
• Erection occurs in about 10 minutes

Intraurethral therapy
MUSE (Alprostadil)
Insert stem into urethra after urination

Erectile rehabilitation
Cialis 5mg daily (2.5-5mg) or with injection or urethral therapy
2x/week or daily vacuum therapy
Starts 6-8 weeks post-op
Patients are allowed 4 PDE5i tablets per month on NHS

ADT side effects

Further information

62 year old man, metastatic prostate
cancer, on ADT for 3 years
• Comes to see you with several complaints:
• Hot flushes waking him at night, embarrassing in the day
• Fatigue – affecting QOL
• Loss of strength (can’t dig the garden any longer)
• Reduced penile length
• Reduced self-worth, feeling low
What would you do? 5 minutes

Serenity prayer – what can we change?
God grant me the serenity to accept the
things I cannot change, the courage to
change the things I can and the wisdom
to know the difference
What side effects can we actually help
with?

Hot flushes
• Randomised trial venlafaxine 75mg od vs cyproterone acetate
100mg od vs medroxyprogesterone acetate 20mg od. MPA and
cyproterone better than venlafaxine, MPA favoured but…
• Acupuncture

Reduced penile length, reduced libido
• A side effect of ADT – no known way to improve this whilst on
LHRH analogues.
Reduced self worth, feeling low• I have a question for you here – what should I be telling the
patient to do?

Questions?