Dr Susan Russell - Haemophilia Foundation Australia 2007... · – labour, episiotomy, caesarian...
24
SCH Management of Delivery in Management of Delivery in Carriers of Carriers of Haemophilia Haemophilia & & Care of their Newborn Care of their Newborn Dr Susan Russell Dr Susan Russell Head, Clinical Head, Clinical Haematology Haematology Programme Programme & & Haemophilia Haemophilia Treatment Centre Treatment Centre Sydney Children Sydney Children ’ ’ s Hospital s Hospital HFA Meeting Canberra HFA Meeting Canberra October 2007 October 2007
Transcript of Dr Susan Russell - Haemophilia Foundation Australia 2007... · – labour, episiotomy, caesarian...
SCH
Management of Delivery in Carriers of Haemophilia &
Care of their Newborn
Management of Delivery in Management of Delivery in Carriers of Carriers of HaemophiliaHaemophilia & &
Care of their Newborn Care of their Newborn
Dr Susan RussellDr Susan RussellHead, Clinical Head, Clinical HaematologyHaematology ProgrammeProgramme & &
HaemophiliaHaemophilia Treatment CentreTreatment CentreSydney ChildrenSydney Children’’s Hospitals Hospital
HFA Meeting CanberraHFA Meeting CanberraOctober 2007October 2007
SCH
Carriers of HaemophiliaCarriers of HaemophiliaCarriers of Haemophilia
Delivery & neonatal period (1Delivery & neonatal period (1stst 28 days) is a high 28 days) is a high risk time for both baby & carrier motherrisk time for both baby & carrier motherIn 1/3 of cases there is no family historyIn 1/3 of cases there is no family history35% of carriers agree to prenatal testing35% of carriers agree to prenatal testing31% of carriers with a +31% of carriers with a +veve family history not family history not aware of their carrier status at delivery*aware of their carrier status at delivery*Knowledge of carrier status has some impact on Knowledge of carrier status has some impact on the method of delivery & management of the babythe method of delivery & management of the baby–– Mothers unaware of their status were more likely to Mothers unaware of their status were more likely to
have instrumental deliveries*have instrumental deliveries*
*Maclean Haemophilia 2004; 10: 560-4

SCH
Carriers of HaemophiliaCarriers of HaemophiliaCarriers of Haemophilia
Factor VIII levels in carriers rise during pregnancyFactor VIII levels in carriers rise during pregnancy–– Majority are normal; some low at termMajority are normal; some low at term
Postpartum, Factor VIII levels drop rapidly and Postpartum, Factor VIII levels drop rapidly and excessive PV bleeding can occur excessive PV bleeding can occur Factor IX carriers levels do not increase during Factor IX carriers levels do not increase during pregnancypregnancyCarriers of haemophilia A & B are potentially at Carriers of haemophilia A & B are potentially at increased risk of bleeding if Factor levels are < 50% increased risk of bleeding if Factor levels are < 50% with with –– invasive procedures invasive procedures egeg CVS, amniocentesis, TOP CVS, amniocentesis, TOP –– labourlabour, episiotomy, caesarian section , episiotomy, caesarian section –– postpartumpostpartum
SCH
Babies with HaemophiliaBabies with HaemophiliaBabies with Haemophilia
1515--33% of newborns with inherited 33% of newborns with inherited bleeding disorders present with bleeding in bleeding disorders present with bleeding in neonatal periodneonatal periodMajority of newborns with haemophilia are Majority of newborns with haemophilia are diagnosed after a bleeddiagnosed after a bleedDiagnosis often delayed Diagnosis often delayed especially if no especially if no family historyfamily history::–– median 7median 7--9 mo, average 6 mo9 mo, average 6 mo
Greatest risk is to babies where there is no family history
SCH
Potential Problems at BirthPotential Problems at BirthPotential Problems at Birth
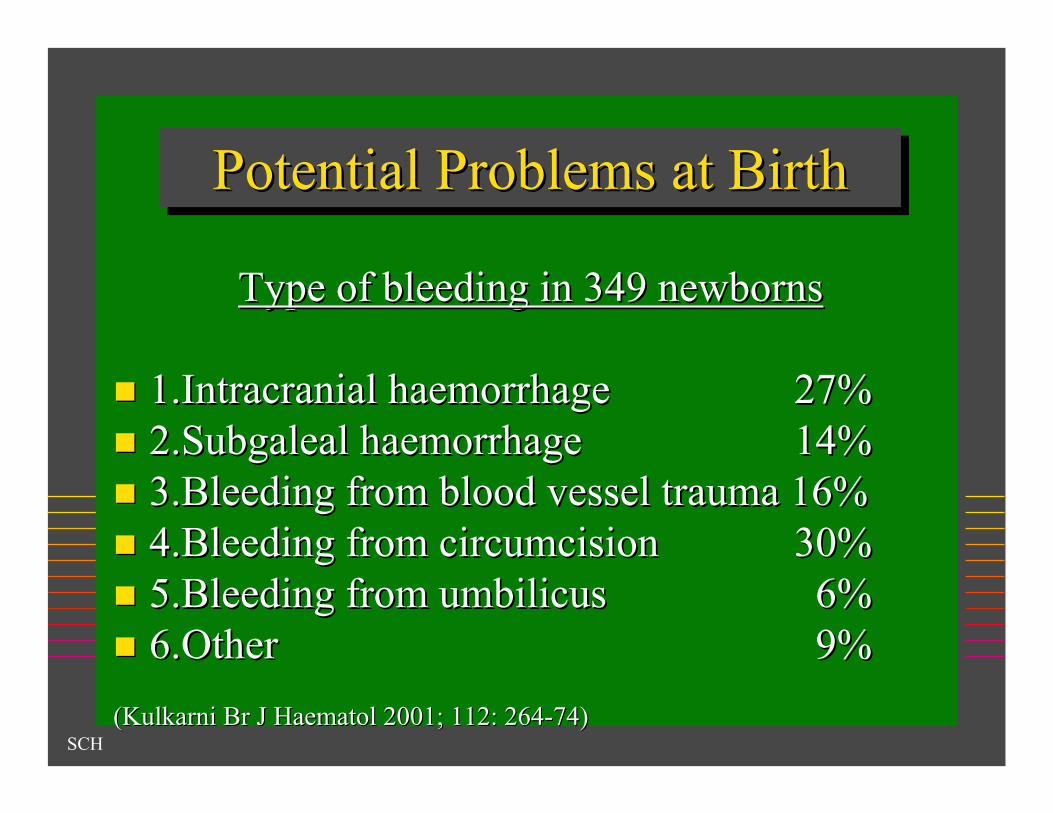
Type of bleeding in 349 newbornsType of bleeding in 349 newborns
1.Intracranial 1.Intracranial haemorrhagehaemorrhage 27%27%2.Subgaleal 2.Subgaleal haemorrhagehaemorrhage 14%14%3.Bleeding from blood vessel trauma 16%3.Bleeding from blood vessel trauma 16%4.Bleeding from circumcision4.Bleeding from circumcision 30%30%5.Bleeding from umbilicus5.Bleeding from umbilicus 6%6%6.Other6.Other 9%9%
((KulkarniKulkarni Br J Br J HaematolHaematol 2001; 112: 2642001; 112: 264--74)74)
SCH
Intracranial HaemorrhageIntracranial Intracranial HaemorrhageHaemorrhage
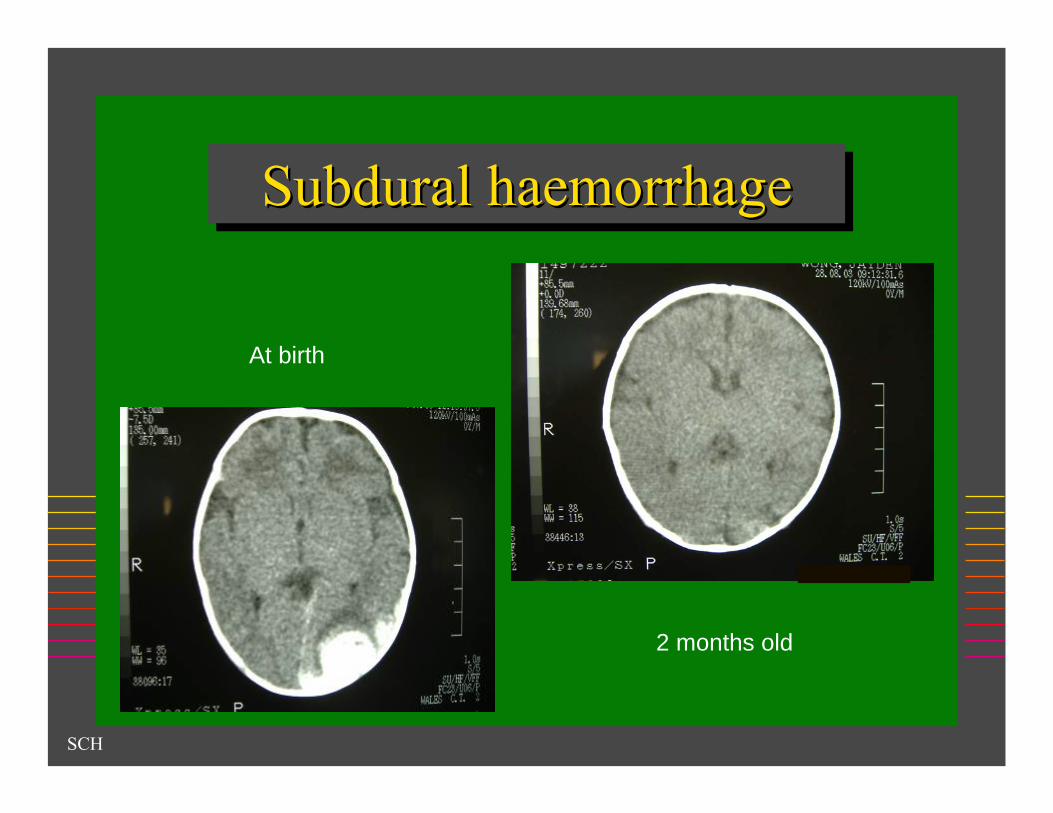
Sites:Sites:–– SubduralSubdural haemorrhagehaemorrhage: most common: most common–– ParenchymalParenchymal haemorrhagehaemorrhage–– Spinal cord Spinal cord haematomahaematoma
Leading cause of morbidity & mortalityLeading cause of morbidity & mortalityCan occur regardless of mode of deliveryCan occur regardless of mode of delivery–– Risk is not zero with a caesarian section*Risk is not zero with a caesarian section*
Can occur regardless of severity of haemophiliaCan occur regardless of severity of haemophiliaIncidence 1Incidence 1--4% male babies with haemophilia4% male babies with haemophilia50% of all ICH in haemophilia occur in the neonatal 50% of all ICH in haemophilia occur in the neonatal periodperiod
Ljung Acta Paediatr 1994; 83: 609-611
SCH
Subdural haemorrhageSubduralSubdural haemorrhagehaemorrhage
At birth
2 months old

SCH
Intracranial HaemorrhageIntracranial Intracranial HaemorrhageHaemorrhage
Prevalence of haemophilia in ICH in Prevalence of haemophilia in ICH in premature neonates is unknownpremature neonates is unknownPresentation:Presentation:–– pallor, lethargy, irritabilitypallor, lethargy, irritability–– vomiting, poor feeding & sucking, vomiting, poor feeding & sucking, –– tense tense fontanellefontanelle, seizure, unequal pupils, seizure, unequal pupils–– hypotension, shockhypotension, shock
Investigation:Investigation:–– ultrasound but poor for ultrasound but poor for subduralsubdural sitesite–– CT scan/MRI scan CT scan/MRI scan –– no LPno LP

SCH
Intracranial HaemorrhageIntracranial Intracranial HaemorrhageHaemorrhage
Treatment: As soon as clinically diagnosedTreatment: As soon as clinically diagnosed–– Factor level to 100% for Factor level to 100% for ≥≥ 2 weeks then proceed to 2 weeks then proceed to
prophylaxis prophylaxis –– ±±Neurosurgery to remove blood Neurosurgery to remove blood
Outcome:Outcome:–– death death –– neurological neurological sequelaesequelae (38%(38%--59%)59%)
»» retardation, cerebral palsyretardation, cerebral palsy»» seizure seizure
–– recurrence of bleedingrecurrence of bleeding–– higher incidence of inhibitorshigher incidence of inhibitors–– decreased quality of lifedecreased quality of life
SCH
Subgaleal Haemorrhage/ Cephalohaematoma
SubgalealSubgaleal HaemorrhageHaemorrhage/ / CephalohaematomaCephalohaematoma
Babies at increased risk:Babies at increased risk:–– ventouseventouse assisted delivery, assisted delivery, –– use of forcepsuse of forceps–– fetal blood samplingfetal blood sampling–– scalp electrodescalp electrode
May be associated with intracranial bleedMay be associated with intracranial bleedShock & DIC can hide the diagnosis of Shock & DIC can hide the diagnosis of haemophiliahaemophilia

SCH
Massive SubgalealHaemorrhage at BirthMassive Massive SubgalealSubgaleal
HaemorrhageHaemorrhage at Birthat Birth

SCH
Bleeding from VenepunctureBleeding from Bleeding from VenepunctureVenepuncture
Risk of compartment syndrome from bleed Risk of compartment syndrome from bleed into into cubitalcubital fossafossa
Chalmers Blood Reviews 2004; 18: 85-92

SCH
Other TraumasOther TraumasOther Traumas
Bleeding from a circumcision (or any Bleeding from a circumcision (or any other operation)other operation)–– 100 reported cases in literature100 reported cases in literature–– Blood transfusion may be required for Blood transfusion may be required for
shockshock
NonNon--stop bleeding from a heel prickstop bleeding from a heel prickMuscle Muscle haematomahaematoma from IM injectionsfrom IM injections

SCH
Recommendations for Management of Possible
& Known Carriers of Haemophilia A & B
Recommendations for Recommendations for Management of Possible Management of Possible
& Known Carriers of & Known Carriers of Haemophilia A & BHaemophilia A & B
SCH
CarriersCarriersCarriersConsider Consider preconceptualpreconceptual genetic genetic counsellingcounsellingGenetic Genetic counsellingcounselling to discuss antenatal diagnosis and to discuss antenatal diagnosis and gene mutation analysisgene mutation analysisReferral to an adult Referral to an adult haematologisthaematologistFactor VIII level be done at booking, 28 & 36 weeks, Factor VIII level be done at booking, 28 & 36 weeks, during during labourlabour & prior to invasive procedures& prior to invasive proceduresArrange for provision of recombinant factor for the Arrange for provision of recombinant factor for the mother, if necessary (mother, if necessary (egeg FVIII < 50%) for FVIII < 50%) for –– invasive procedures invasive procedures –– epidural epidural anaesthesiaanaesthesia–– delivery and post partumdelivery and post partum
Lee Haemophilia 2006; 12: 301-336
SCH
CarriersCarriersCarriers
Ideally, carriers be delivered in Ideally, carriers be delivered in centrescentres with access towith access to–– an an ““adultadult”” haematologisthaematologist for care of the motherfor care of the mother–– a high risk obstetric unit & a neonatology unita high risk obstetric unit & a neonatology unit–– a a ““paediatricpaediatric”” haematologisthaematologist–– specialisedspecialised anaesthestistanaesthestist–– a blood bank with Factor a blood bank with Factor –– laboratory to measure factor levelslaboratory to measure factor levels
Barriers to achieving the ideal:Barriers to achieving the ideal:–– country patients: large distances country patients: large distances –– personal choicepersonal choice
Regardless of where delivery occurs: communication Regardless of where delivery occurs: communication between all of the above health professionals is between all of the above health professionals is paramountparamount & a delivery plan must be established in & a delivery plan must be established in advanceadvance
Lee Haemophilia 2006; 12: 301-336
SCH
DeliveryDeliveryDelivery
Method of delivery at discretion of the obstetricianMethod of delivery at discretion of the obstetricianRequires careful considerationRequires careful consideration–– Safest method of delivery for a baby at risk is controversialSafest method of delivery for a baby at risk is controversial–– Principle: deliver by the least traumatic methodPrinciple: deliver by the least traumatic method
»» Avoid Avoid ventouseventouse, , midcavitymidcavity forceps and prolonged forceps and prolonged labourlabour»» May be via caesarian section in some circumstancesMay be via caesarian section in some circumstances
Consider factor replacement for mother if necessary Consider factor replacement for mother if necessary during during labourlabour–– Check FBC, APTT, platelets, factor levels + XCheck FBC, APTT, platelets, factor levels + X--matchmatch
Have a Have a paediatricianpaediatrician present with a recombinant present with a recombinant Factor vial in his handFactor vial in his hand
Lee Haemophilia 2006; 12: 301-336

SCH
PostpartumPostpartumPostpartum
Carriers are at increased risk of Carriers are at increased risk of postpartum postpartum haemorrhagehaemorrhage (>500 ml)(>500 ml)Check Factor level daily after deliveryCheck Factor level daily after deliveryKeep >50% for 3 days (5 if C/S)Keep >50% for 3 days (5 if C/S)
Lee Haemophilia 2006; 12: 301-336
SCH
Recommendations for Management of the Baby
Born to a Possible or Known Carrier of
Haemophilia
Recommendations for Recommendations for Management of the Baby Management of the Baby
Born to a Possible or Born to a Possible or Known Carrier of Known Carrier of
HaemophiliaHaemophilia
SCH
BabiesBabiesBabies
1. Babies at risk not have fetal scalp electrodes placed 1. Babies at risk not have fetal scalp electrodes placed or fetal blood sampling performedor fetal blood sampling performed2. Collect cord blood or perform careful 2. Collect cord blood or perform careful venepuncturevenepuncture for testing of all males at riskfor testing of all males at risk3. Consider 3. Consider venepuncturevenepuncture to confirm initial resultto confirm initial result4. Give Vitamin K to prevent 4. Give Vitamin K to prevent HaemorrhagicHaemorrhagic Disease Disease of the Newbornof the Newborn5. Give hepatitis B vaccination 5. Give hepatitis B vaccination 6. Circumcision not be performed until status 6. Circumcision not be performed until status determined determined –– Note: circumcision in general is a controversial Note: circumcision in general is a controversial
topictopic
Kulkarni Br J Haematol 2001; 112: 264-74
SCH
The Giving of Factor at BirthThe Giving of Factor at BirthThe Giving of Factor at BirthGiving a dose of Factor VIII/IX empirically at birth to all boysGiving a dose of Factor VIII/IX empirically at birth to all boysborn to known carriers has been advocated by some* but not born to known carriers has been advocated by some* but not widely practiced widely practiced
Possible increased risk of inhibitor development from Possible increased risk of inhibitor development from ““earlyearly””exposure to factor VIIIexposure to factor VIII
CANAL study concluded that it is the intensity of treatment at aCANAL study concluded that it is the intensity of treatment at asoso--called called ““peak momentpeak moment”” rather than age at first exposure that rather than age at first exposure that increases the risk of inhibitor developmentincreases the risk of inhibitor development
Giving a dose of Factor VIII/IX is recommended if Giving a dose of Factor VIII/IX is recommended if –– baby had a traumatic birthbaby had a traumatic birth–– there is an obvious bleeding problemthere is an obvious bleeding problem–– baby is very ill at birth & requiring intubation & ventilationbaby is very ill at birth & requiring intubation & ventilation–– ICH is suspectedICH is suspected
(*Buchanan J (*Buchanan J PediatrPediatr HematolHematol OncolOncol 1999; 21: 2541999; 21: 254--66

SCH
Imaging of the HeadImaging of the HeadImaging of the Head
Imaging of the head must be performed in Imaging of the head must be performed in all babies at risk who are:all babies at risk who are:–– symptomatic of ICHsymptomatic of ICH–– had a traumatic deliveryhad a traumatic delivery–– prematurepremature
Types of imaging: ultrasound, CT scan, Types of imaging: ultrasound, CT scan, MRIMRI
SCH
In ConclusionIn ConclusionIn Conclusion
Prompt recognition of bleeding & early diagnosis of Prompt recognition of bleeding & early diagnosis of haemophiliahaemophilia in any baby is crucial to proper managementin any baby is crucial to proper managementAny unexplained or prolonged bleeding in a newborn Any unexplained or prolonged bleeding in a newborn should raise the suspicion of should raise the suspicion of haemophiliahaemophilia and testing and testing should be done immediately (especially ICH)should be done immediately (especially ICH)All (male) newborns delivered by possible and known All (male) newborns delivered by possible and known haemophiliahaemophilia carriers should be tested at birthcarriers should be tested at birthThe pregnancy and delivery of a baby by a The pregnancy and delivery of a baby by a haemophiliahaemophiliacarrier should be regarded as a potentially high risk carrier should be regarded as a potentially high risk situation for both and be managed accordinglysituation for both and be managed accordinglyA multidisciplinary approach to & establishment of A multidisciplinary approach to & establishment of guidelines for the management of carriers, the delivery guidelines for the management of carriers, the delivery and their newborns is highly recommendedand their newborns is highly recommended

SCH
ConclusionsConclusionsConclusions
Prenatal testing of females with a family Prenatal testing of females with a family history of history of haemophiliahaemophilia, to determine carrier , to determine carrier status may influencestatus may influence–– Reproductive optionsReproductive options–– Where the pregnancy is managedWhere the pregnancy is managed–– Management of the motherManagement of the mother–– Management of Management of labourlabour–– Method of delivery Method of delivery ieie avoid traumatic avoid traumatic
procedures that may place the baby at risk of procedures that may place the baby at risk of ICHICH
–– Management of the baby Management of the baby