Dr Shahna airway management in ICU; 2016
43
Airway Airway management in management in icu icu Dr shahna ali Dr shahna ali
-
Upload
shahnaali -
Category
Health & Medicine
-
view
52 -
download
3
Transcript of Dr Shahna airway management in ICU; 2016

Airway Airway management in icumanagement in icu
Dr shahna aliDr shahna ali

INTRODUCTIONINTRODUCTION• Airway management is a fundamental aspect of emergency Airway management is a fundamental aspect of emergency
and critical care medicineand critical care medicine
• Expertise in airway management – an important skillExpertise in airway management – an important skill
““An experienced EMS provider will tell you that, An experienced EMS provider will tell you that,
when treating a patient, the three most important when treating a patient, the three most important
considerations are airway, airway, airway.”considerations are airway, airway, airway.”

OUR OPTIONSOUR OPTIONS
Anaesthesiology EmergencyPlan in advance
Can’t get airway ….…. Awake patient…. Regroup…. Go for coffee
What will be, will be ………
Can’t get airway ….…. Wipe brow…. Run for help…. Call HOD

WHAT MAKES – DIFFICULT??WHAT MAKES – DIFFICULT??

SCENARIO IS DIFFERENTSCENARIO IS DIFFERENT• PatientsPatients
• Varying degree of acute hypoxemiaVarying degree of acute hypoxemia
• Hemodynamic instabilityHemodynamic instability
• Tolerate poorly any delays in establishing airwayTolerate poorly any delays in establishing airway
• Associated conditions – intracranial hypertension, myocardial Associated conditions – intracranial hypertension, myocardial
ischemia, upper airway bleeding and emesisischemia, upper airway bleeding and emesis
• Co-morbiditiesCo-morbidities

Our patients are differentOur patients are different

They tend to look like thisThey tend to look like this

Or even thisOr even this

And this – after failed And this – after failed intubation attempt intubation attempt

SCENARIO IS DIFFERENTSCENARIO IS DIFFERENT• EvaluationEvaluation
• Inability or lack of time Inability or lack of time
• ConditionsConditions• Not ideal Not ideal
• InstrumentsInstruments• Not working properlyNot working properly• Not sufficientNot sufficient
• Well wishersWell wishers• Not well versed with airway managementNot well versed with airway management

COMPLICATIONSCOMPLICATIONS

Airway management is really easy…Airway management is really easy…
……except when it isn’t… except when it isn’t…

OUR SUCCESS: PLANOUR SUCCESS: PLAN
Drugs
Intubation
Difficult Intubation
Stabilization
Pre-oxygenation
Positioning
Assessment
Preparation
Steps for S
uccess

PreparationPreparationY BAG PEOPLE
Stuart F. Reynolds, John Heffner. Airway Management of the Critically Ill Patient. Chest 2005;127;1397-1412

What NextWhat Next

RememberRemember• Assessment in critically ill patients – does not limit to airwayAssessment in critically ill patients – does not limit to airway
• Assess general and hemodynamic condition of patientAssess general and hemodynamic condition of patient
Prepare for crash landing

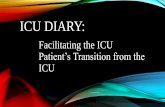
The Montpellier-ICU intubation algorithm
Bundle to limit complications related to intubation.

The Montpellier-ICU intubation algorithmPRE-INTUBATION
1. Presence of two operators2. Fluid loading (isotonic saline 500 ml or starch 250 ml) in absence of cardiogenic edema 3. Preparation of long-term sedation4. Pre-oxygenate for 3 min with NIV in case of acute respiratory failure (FiO2 100 %, pressure support ventilation level between 5 and 15 cmH2O to obtain an expiratory tidal volume between 6 and 8 ml/kg and PEEP of 5 cmH2O)
PER-INTUBATION
5. Rapid sequence induction: - Etomidate 0.2-0.3 mg/kg or ketamine 1.5-3 mg/kg - Succinylcholine 1-1.5 mg/kg (in absence of allergy, hyperkalemia, severe acidosis, acute or chronic neuromuscular disease, burn patient for more than 48 h and medullar trauma) - Rocuronium: 0.6 mg/kg IVD in case of contraindication to succinylcholine or prolonged stay in the ICU or risk factor for neuromyopathy 6. Sellick maneuver
POST-INTUBATION
7. Immediate confirmation of tube placement by capnography8. Norepinephrine if diastolic blood pressure remains < 35 mmHg9. Initiate long-term sedation10. Initial 'protective ventilation': tidal volume 6-8 ml/kg, PEEP < 5 cmH,O and respiratory rate between 10 and 20 cycles/min, FiO2 100 % for a plateau pressure < 30 cmH2O 11. Recruitment maneuver: CPAP 40 cmH2O during 40 s, FiO2 100 % (if no cardiovascular collapse) 12. Maintain intubation cuff pressure from 25-30 cmH2O
NIV: non-invasive ventilation; CPAP: continuous positive airway pressure ; FiO2: inspired fraction of oxygen De Jong et al. Critical Care 2014 18:209 doi:10.1186/cc13776

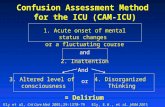
PositioningPositioningSniffing Position “ Magill’s Position”



PRE OXYGENATIONPRE OXYGENATIONTo perform NIV for 3 to 5 min in critically ill patients, the facial mask available in every ICU room is adequate.
The patient should be in the semi-sitting position, FiO2 set at 100 %, inspiratory pressure set to observe a tidal volume of 6 to 10 ml/kg and respiratory rate of 10 to 25 cycles/ min. The duration of the procedure usually corresponds with the time needed to prepare the drugs and equipment for intubation.


ALWAYS REMEMBERALWAYS REMEMBEREmergency Airway Pharmacology
AnaesthesiologyStabilizedOptimizedPlanned
Critically illHypotensiveHypovolemicSympathetic overtoneLow reservesCo – morbiditiesDoes not give time

PHARMACOLOGYPHARMACOLOGY• Proper drug selection:Proper drug selection:
• facilitates laryngoscopyfacilitates laryngoscopy• improves like hood of successful intubationimproves like hood of successful intubation• attenuates the physiological response of intubationattenuates the physiological response of intubation• reduces the risk of aspiration and other complications – 50 to 70%reduces the risk of aspiration and other complications – 50 to 70%
• Depending upon situation combination of :Depending upon situation combination of :• pre-induction drugspre-induction drugs• induction agentinduction agent• paralytic agentparalytic agent
• Muscle relaxants - Muscle relaxants - BewareBeware• compel the physician to ventilate or intubatecompel the physician to ventilate or intubate• CIN or CIMCIN or CIM
Sivilotti ML, Filbin MR, Murray HE, et al. Does the sedative agent facilitate emergency rapid sequence intubation? Acad Emerg Med 2003; 10:612–620

Pre-induction drugsPre-induction drugsPressor response
• Critically ill – hypertensive response may lead to myocardial or Critically ill – hypertensive response may lead to myocardial or
cerbrovascular injurycerbrovascular injury
• Critically ill patients who require emergency intubation – hypoxia, Critically ill patients who require emergency intubation – hypoxia,
hypercarbia and acidosis resulting into extreme sympathetic outflowhypercarbia and acidosis resulting into extreme sympathetic outflow
• Attenuation of theses response – unmask relative hypovolemia and/or Attenuation of theses response – unmask relative hypovolemia and/or
vasodilatation resulting in postintubation hypotensionvasodilatation resulting in postintubation hypotension
Horak J, Weiss S. Emergent management of the airway: new pharmacology and the control of comorbidities in cardiac disease, ischemia, and valvular heart disease. Crit Care Clin 2000; 16:411–427

OpioidsOpioids• Opioids have long history of use in anaesthesiaOpioids have long history of use in anaesthesia
• Fentanyl – most commonly used drugFentanyl – most commonly used drug
• Fentanyl blunts the hypertensive response to intubation (40% incidence Fentanyl blunts the hypertensive response to intubation (40% incidence
of hypertensive response compared with 80% in control subjects), 41 of hypertensive response compared with 80% in control subjects), 41
although it has only marginal effects on attenuating tachycardia although it has only marginal effects on attenuating tachycardia (1)(1)
• Derivatives of fentanyl, sufentanil and alfentanil, are more effective Derivatives of fentanyl, sufentanil and alfentanil, are more effective
blunting both the tachycardic and hypertensive responses to intubation blunting both the tachycardic and hypertensive responses to intubation (2)(2)
1. Feng CK, Chan KH, Liu KN, et al. A comparison of lidocaine, fentanyl, and esmolol for attenuation of cardiovascular response to laryngoscopy and tracheal intubation. Acta Anaesthesiol Sin 1996; 34:61–67
2. Wadbrook PS. Advances in airway pharmacology: emerging trends and evolving controversy. Emerg Med Clin North Am 2000; 18:767–788

OpioidsOpioids• Fentanyl is used in dose of 2 to 3 µmg/kg over 1 to 2 minsFentanyl is used in dose of 2 to 3 µmg/kg over 1 to 2 mins
• Opioids-induced chest wall rigidityOpioids-induced chest wall rigidity
• Caution - in patients who are in severe shock statesCaution - in patients who are in severe shock states
• Opioids can block the sympathetic compensatory response to Opioids can block the sympathetic compensatory response to
hypotension, resulting in cardiovascular collapsehypotension, resulting in cardiovascular collapse

LidocaineLidocaine• Lidocaine, a class 1B antiarrhythmic drug used:Lidocaine, a class 1B antiarrhythmic drug used:
• to diminish the hypertensive responsediminish the hypertensive response• to reduce airway reactivityto reduce airway reactivity• to prevent intracranial hypertension to prevent intracranial hypertension • to decrease the incidence of dysrrhythmiasto decrease the incidence of dysrrhythmias
• Lidocaine should be administered 3 min prior to intubation Lidocaine should be administered 3 min prior to intubation at a dose of 1.5 mg/kgat a dose of 1.5 mg/kg
Lev R, Rosen P. Prophylactic lidocaine use preintubation: a review. J Emerg Med 1994; 12:499–506

Inducing agentsInducing agents• Used to facilitate intubation by rapidly inducing Used to facilitate intubation by rapidly inducing
unconsciousnessunconsciousness
• Various inducing agents commonly used:Various inducing agents commonly used:• MidazolamMidazolam
• PropofolPropofol
• EtomidateEtomidate
• KeatmineKeatmine
• ThiopentoneThiopentone

MidazolamMidazolam• Midazolam is one of most commonly used inducing agent in Midazolam is one of most commonly used inducing agent in
critically ill patientscritically ill patients
• Advantage – less hypotension and respiratory distress than Advantage – less hypotension and respiratory distress than
propofol and thiopentonepropofol and thiopentone
• Disadvantage – onset is slowDisadvantage – onset is slow
• Dose – 0.05 to 0.01 mg/kgDose – 0.05 to 0.01 mg/kg

PropofolPropofol• RRapid-acting, lipid-soluble induction drug apid-acting, lipid-soluble induction drug
• Advantages :Advantages :• short half-life and duration of activity and rapid onset of actionshort half-life and duration of activity and rapid onset of action• anticonvulsive propertiesanticonvulsive properties• antiemetic effectsantiemetic effects• reduces intracranial pressurereduces intracranial pressure• produces profound relaxation of laryngeal musculatureproduces profound relaxation of laryngeal musculature
• DisadvantagesDisadvantages• drug induced hypotensiondrug induced hypotension• allergiesallergies• no analgesic effectno analgesic effect
• Dose – 0.5 to 2 mg/kgDose – 0.5 to 2 mg/kg

EtomidateEtomidate• Advantages :Advantages :
• short half-life and duration of activity and rapid onset of actionshort half-life and duration of activity and rapid onset of action• predictably does not affect BPpredictably does not affect BP• cerebral-protective effectscerebral-protective effects
• DisadvantagesDisadvantages• does not attenuate the pressor responsedoes not attenuate the pressor response• nausea, vomitingnausea, vomiting• myoclonic movements and lowering of the seizure thresholdmyoclonic movements and lowering of the seizure threshold• adrenal suppressionadrenal suppression
Bergen JM, Smith DC. A review of etomidate for rapid sequence intubation in the emergency department. J Emerg Med 1997; 15:221–230Schenarts CL, Burton JH, Riker RR. Adrenocortical dysfunction following etomidate induction in emergency department patients. Acad Emerg Med 2001; 8:1–7

EtomidateEtomidate• Concern in septic shock patients - study by Concern in septic shock patients - study by David Charles RayDavid Charles Ray – –
Etomidate caused less cardiovascular depression than other induction Etomidate caused less cardiovascular depression than other induction
agents in patients with septic shockagents in patients with septic shock
• Dose – 0.1 to 0.2 mg/kgDose – 0.1 to 0.2 mg/kg
• In the future, the investigational drug methoxycarbonyl-etomidate, which In the future, the investigational drug methoxycarbonyl-etomidate, which
lacked prolonged suppressive effects on steroid production in animal lacked prolonged suppressive effects on steroid production in animal
models, might be a safer alternative in critically ill patientsmodels, might be a safer alternative in critically ill patients

Muscle RelaxantsMuscle Relaxants• Use outside operation room in emergency department Use outside operation room in emergency department
remains controversialremains controversial
• Pro:Pro:• Improves intubation conditionsImproves intubation conditions• Makes bag mask ventilation betterMakes bag mask ventilation better• Intubating without muscle relaxants carries significant risk of Intubating without muscle relaxants carries significant risk of laryngeal and vocal-cord morbiditylaryngeal and vocal-cord morbidity
• Cons:Cons:• Unexpected difficult intubationUnexpected difficult intubation
When neuromuscular blocking agents are used for emergency intubation, rapid onset is
crucial to allow quickly securing the airway

Muscle RelaxantsMuscle Relaxants
Booij LH. Is succinylcholine appropriate or obsolete in the intensive care unit? Crit Care 2001; 5:245–246
Perry JJ, Lee J, Wells G. Are intubation conditions using rocuronium equivalent to those using succinylcholine?
Acad Emerg Med 2002; 9:813–823

INTUBATIONINTUBATION


Crash AirwayAlgorithm

Failed AirwayAlgorithm

POST INTUBATION POST INTUBATION STABILIZATIONSTABILIZATION
• Maintain adequate ventilation and oxygenationMaintain adequate ventilation and oxygenation
• Maintain hemodynamic stabilityMaintain hemodynamic stability
• Maintain acid-base and electrolyte balanceMaintain acid-base and electrolyte balance
• Need for sedation or paralysisNeed for sedation or paralysis
• Oral/eye/skin careOral/eye/skin care

TAKE HOME MESSAGETAKE HOME MESSAGE• Maintaining and securing a patent airway is primary goal in any Maintaining and securing a patent airway is primary goal in any
emergency and difficult airway situationemergency and difficult airway situation
• It’s a challengeIt’s a challenge
• But not impossible if we know correct techniquesBut not impossible if we know correct techniques
• Recognize the difficult airwayRecognize the difficult airway
• How much time do you have?How much time do you have?
• Who else is around?Who else is around?
• What is your backup procedureWhat is your backup procedure
• Know both old and new methodsKnow both old and new methods
• Choose backups based on skillsChoose backups based on skills