Dr Shahid Zaman - King's College London · 2019-02-25 · 17/10/2018 1 Down’s syndrome and...
37
17/10/2018 1 Down’s syndrome and dementia Dr Shahid Zaman Associate Lecturer & Consultant Psychiatrist Cambridge Intellectual and Developmental Disabilities Research Group, Dept. of Psychiatry, University of Cambridge Cambridgeshire & Peterborough NHS Foundation Trust (CPFT) http://www.Dem enti aInDS.com [email protected] Tuesday 16 October 2018 at King’s College London Overview PART-1 • Background – what is dementia; what is Alzheimer’s disease • Why important in Down’s syndrome • Why does it happen • What can we do-prevention-primary & secondary & treatment PART-2 • Video • Case example • Memory clinic
Transcript of Dr Shahid Zaman - King's College London · 2019-02-25 · 17/10/2018 1 Down’s syndrome and...

17/10/2018
1
Down’s syndrome and dementia
Dr Shahid ZamanAssociate Lecturer &
Consultant Psychiatrist
Cambridge Intellectual and Developmental Disabilities Research Group, Dept. of Psychiatry, University of Cambridge
Cambridgeshire & Peterborough NHS Foundation Trust (CPFT)http://www.DementiaInDS.com
Tuesday 16 October 2018 at King’s College London
Overview
PART-1
• Background – what is dementia; what is Alzheimer’s disease
• Why important in Down’s syndrome
• Why does it happen
• What can we do-prevention-primary & secondary & treatment
PART-2
• Video
• Case example
• Memory clinic

17/10/2018
2
Epidemiology
• Improved longevity in ID (1930s, c.18.5 years; 1990s, 66 years)
• By 2020 the number >65years with ID will double
• Ageing and associated conditions more relevant
Comparison of dementia age-specific prevalence rates
BSP & RCPsyh rep 77; 2015

17/10/2018
3
Dementia type
• Alzheimer’s disease commonest (c. 60%)• Others: Vascular dementia, Lewy body dementia,
Fronto-temporal dementia• 50% have AD pathology but others are “mixed
dementia”• Down syndrome -AD commoner; vascular rare• Histopathological process starts well before
symptoms appear
Summary of Diagnostic Criteria
• Cognitive (esp. memory)/adaptive skills decline
• Personality/behavioural changes
• Progressive
• Significantly effect social & occupational functioning
• Exclude other causes -poor environment, medication, delirium, mood disorder, sensory impairment, hypothyroidism, B12, folate, etc

17/10/2018
4
Alzheimer’s disease-risk factors
• Age
• Family history increases risk
• Apolipoprotein E; there are three isoforms e2 (10 to 20%), e3(60%), e4 (20-30%))
• E4e(3 or 2) (x3); e4e4 (x8 to x12): 40 to 65% of AD population
• If e4 earlier onset; e2 “protective”
Alzheimer’s disease-risk factors
• Cardiovascular risk factors- hypertension, hyperlipidaemia, diabetes, obesity, smoking
• Fewer year in education-?cognitive reserve building or socio-economic factors
• Social & cognitive engagement
• Moderate (x2 risk; loss of consciousness or PTA >30min) to severe (x4 risk; >24 hours) traumatic brain injury
• Repeated (even mild TBI) increases risk

17/10/2018
5
Wikipedia 2015
CORONAL SECTIONS:
( A) Ant. pole of temporal lobe ( B) Amygdala & entorhinal cortex ( C) Body of hippocampus ( D) Calcarina in the occiptal pole
D. A. Devenny et al., 2005
Alzheimer’s disease neuropathology in DS

17/10/2018
6
Alzheimer’s disease pathology in DS-Cored amyloid plaque components
Other components:•B: Microglia (CD45)•C: Astrocytes
(GFAP)•D: Phosphorylated
tau (Tau-1)
D. A. Devenny et al., 2005
Thioflavin-T

17/10/2018
7
Amyloid Precursor Protein metabolism & potential drug targets
L.M.Shaw et al., 2007
Cummings NEJM 2004
Amyloid cascade hypothesis
DS
AB42 Tau AB42 Tau DAPI
AD

17/10/2018
8
Alzheimer’s disease pathology in DS-Cored amyloid plaque components
Other components:•B: Microglia (CD45)•C: Astrocytes
(GFAP)•D: Phosphorylated
tau (Tau-1)
D. A. Devenny et al., 2005
Thioflavin-T
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
90.00
100.00
0 5 15 25 35 45 55 65
% A
ffecte
d
(adapted from Mann et al., 1989)
AD neuropathology & dementia diagnosis in Down syndrome versus age
Age (years)

17/10/2018
9
Alzheimer’s disease in Down syndrome (trisomy 21)
• By 40-yrs., pathological hallmarks of
Alzheimer’s disease almost universally
• Not all over the age of 40 years have a
clinical diagnosis of dementia
Photo from Down’s Syndrome Association
Down syndrome-the APP gene
Photo from Down’s Syndrome Association
Link with Alzheimer’s disease:
An extra copy of the gene, Amyloid
Precursor Protein (APP)
Gene dosage effect
APP breaks down to produce Amyloid-
beta-central to dementia

17/10/2018
10
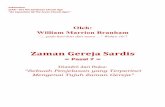
PiB-PET in Down syndrome with or without dementia
Annus et al., 2016 Alzheimers Dement. 2016 May; 12(5): 538–545.
Total cortical binding (using PiB) versus age in Down syndrome

17/10/2018
11
Age (years)
No
n-D
isp
lace
able
Bin
din
g P
oten
tial
Non-displaceable binding potential versus age in the 14 healthy non-DS volunteers
Landt et al., 2011 Arch Neurol.
Bal lard et al., The Lancet Neurology 2016 15, 622-636DOI: (10.1016/S1474-4422(16)00063-6)

17/10/2018
12
What prospects for treatments?
By the time a clinical diagnosis is made-it’s probably too late!
The clinical phenotype ‘lags behind’ the neuropathology by 10 to 15 years-the histopathology is necessary but not sufficient
This creates a problem when considering early interventions
Ballard et al., The Lancet Neurology 2016 15, 622-636DOI: (10.1016/S1474-4422(16)00063-6)
Intervention ?
Primary prevention-when safe to intervene?

17/10/2018
13
Non disease-modifying dementia drugs
• Cholinesterase inhibitors and memantine
• Others: vitamin E in DS
• May slow cognitive decline; evidence of improved quality of life for patients and carers
• May help behavioural/psychological problems: irritability, aggression, mood, hallucinations
Disease-modifying or preventativedementia drugs
• Monoclonal antibodies directed against various domains of Ab (e.g. solanezumab –targets soluble Ab crenezumab-targets soluble and fibrillar Ab, gantenerumab-targets fibrillar Ab; aducanumab)
• Active antibodies: directed against Ab
• Reduce production by BACE inhibitor (e.g MERC MK-8931 or verubecestat)

17/10/2018
14
Any clinical drug trials in Down syndrome?
•Immunotherapy (passive or active) to remove Ab – a feasibility trial in USA
•No BACE inhibitor trials yet•No gamma-secretase modulator trials yet
•No tau targets tried yet

17/10/2018
15
Research methods in our current study
CT and MRI/PET brain scans
Blood tests
Neuropsychologicaltests
Physical exam
Ethical tensions for research with vulnerable adults
DISCRIMINATION IF PARTICIPANTS ARE EXCLUDED
LIMITING THE DEVELOPMENT OF TREATMENTS FOR THIS POPULATION
UNETHICAL INCLUSION OF VUNERABLE ADULTS
POTENTIALLY EXPLOTING PARTICIPANTS WITH A LACK OF CAPACITY
d’Abera et al, 2013

17/10/2018
16
Positive feedback
I support people with DS to take part…as once they understand what it’s about andwhy they are needed, they want to help and make a difference..
Summary
• Alzheimer’s disease (AD) neuropathology occurs almost universally in adults with Down syndrome (40 s)
• Clinical symptoms manifest many years after pathology established, by which time treatment options less likely to modify disease process
• Aim is to discover biological and other measurable features to help identify the “pre-symptomatic” and “prodromal” condition of AD and ultimately those individuals likely to benefit from disease modifying interventions
• Treatments based on: amyloid cascade hypothesis: triplication of the APP gene on chromosome 21 leads to overproductionof amyloid-beta (Ab) that initiates and drives the disease

17/10/2018
17
PART II
Video clip

17/10/2018
18
CASE
Background-1
• RN 51 year old with DS• Singe man, never married
• living in supported accommodation since 2003
• Full programme of activities-including day centres
• Prior to 2003, living with his mother in council home

17/10/2018
19
Background-2
• Only child
• Mother – AD diagnosed 3 years-farm labourer
• Father – died 15 years ago-?Cause of death- bus conductor
• Maternal Aunt – 100 years visits
• Aunt- 70 – carcinoma of breast
• Moved to supported living in 2003
Background-3
• Moderate Intellectual disability (IQ: 36 to 49)
• Good vocabulary but in conversation some difficulty in putting together coherent sequences of sentences. Understands level of a 5 year old
• Fully mobile, independent with e.g. personal care, laundry, make basic meals
• Requires help: organising day, budgeting, travel

17/10/2018
20
Background-4
• Non smoker
• No alcohol or substance misuse
• Not hypertensive
• No FH of IHD
Background-5
• 20 years: Diabetes Mellitus type I
• 27 years: Hypothyroidism
• 29 years: Bilateral cataracts
• 39 years: Hypercholesterolaemia
• 45 years: Bilateral mild non-proliferative diabetic retinopathy
• 47 years: DKA - admitted x3
• 43 years: Bilateral diabetic macular oedema
• 49 years: Microalbuminuria-urine alb:creat ratio, 4.1 mg/mmol

17/10/2018
21
Presented with…
Mr RN, in 2009
• appeared more confused or disorientated
• unable to remember where his bedroom was when onholiday; unable to remember where he has put his keys
• talking about the past as if it was happening now (familymembers who were deceased as if alive)

17/10/2018
22
Mr RN, in 2009
• unsure when crossing the road
• puts on 2 jumpers and no coat
• shoes the wrong way round
• unable to shave; unable to do laundry
• hoarding food
Mr RN, in 2009
• Signs of irritability-hit a co-resident; shouting and angry more often
• No deterioration in language
• No deterioration in sleep
• No change in appetite or weight
• Good diabetic control

17/10/2018
23
Mr RN, in 2009
• Simvastatin 40 mg OD
• Aspirin 75 mg OD
• Levothyroxine 125 mcg OD
• Novorapid/Levemir
Mr RN a 51 year old
• Feb 2010: on donepazil for 4 months;
• Been suspicious; no improvement in memory; no improvements in functional skills; believed he was a member of staff and wanted to administer insulin to others.
• Shaving the back of his neck & abdomen
• Tearful

17/10/2018
24
Mr RN a 51 year old
• April 2010: Hoarding others’ personal belongings and items e.g. socks, wet wipes, deodorants; flushed a phone down the toilet
• Withdrawn, more tearful, less enjoyment living at his home but enjoyed other activities
Mr RN a 51 year old
• Aug/Sept 2010: following the introduction of fluoxetine, mood improved; no aggression; further deterioration in skills

17/10/2018
25
Mr RN a 51 year old
• Nov 2010: following the introduction of fluoxetine, mood improved; no aggression; further deterioration in skills; language deteriorated-less able to understand taking more time to process
• Retrograde amnesia – at least 2 years back. No further decline in functional skills.
Mr RN a 51 year old
• Sept 2011: 3 aggressive outbursts-mostly stable
• June 2012: Staff training for dementia being well observed

17/10/2018
26
Summary
A 51 year old male with DS and moderate ID, who presents with typicalfeatures of AD. He was managed by training his support staff withtraining in dementia, donepazil and fluoxetine.

17/10/2018
27
Intellectual Disability and Dementia-Memory Clinic
PerspectiveRebecca Ford and Rachel Spitzer
Senior Community Nurses
East Learning Disability Team
Memory clinic
• We have used the GP LES lists to identify everyone with Downs Syndrome within our area.
• Memory clinic is a multi professional session once a month
• Clients attend with their carers and/or family

17/10/2018
28
Assessments
• DLD
• CAMCOG
• CAMDEX
• Communication assessment
• Sensory assessment
• OT skills assessment
• Eating and drinking assessment
Monitoring medication
• One of our roles is to support families and carers to understand and identify medications and possible side effects.
• We provide easy read information to clients and carers.
• We look for signs of stabilisation of cognitive abilities.

17/10/2018
29
Non-Drug Treatments
• Cognitive Stimulation – encourage
activities that will maintain memory, problem-solving skills and language
• Occupational Activities – seek meaningful activities for individuals as their needs change e.g.massage, aromatherapy
• Behavioural Therapy – work with Psychologist/Nurse to develop strategies to reduce behavioural problems associated with dementia e.g.aggression
• Exercise and Nutrition – exercise and a well balanced diet can improve mobility and benefit mental function and mood.
Behaviour monitoring
• Provide support and advice to carers and families regarding changes in behaviour.
• Monitor charts and records kept by support staff.
• Refer to behaviour clinic if needed.
• Refer to SCIP advisor if needed.

17/10/2018
30
Staff training
• Provided to an individual staff team so very client focused.
• Opportunity for staff to discuss any concerns.
• Provide practical ways of working with dementia.
• Advice and support
• Provide reassurance to staff team and family
Communication
• Communication may already be a difficulty for someone with a learning disability
• Communication skills will gradually decrease as dementia progresses
• The individual might become frustrated, exhibiting aggression and/or challenging behaviours
• Non-verbal communication becomes even more important to aid understanding

17/10/2018
31
Communication• It may appear that the individual is talking “rubbish”
or refusing to interact
• You need to believe that the individual wants to communicate
• Use very short sentences with fewer key information carrying words
• You will need to ensure your body language and intonation are clear and relate to what you are saying
• You will need to give extra time and be patient
CommunicationProblems might include:
• Reduction in, and possible total loss of speech eventually
• Word finding difficulties
• Reduced ability to understand
• Poor articulation
• Unusual speech patterns
• Repetition
• Decreased ability to use sign language
• Increase in non-verbal communication
• Difficulty knowing when to speak

17/10/2018
32
• Life story work which is a record of past life e.g.
box/book with photo’s and other familiar objects (Good practice for all service users throughout life)
• Reminiscence work (involve individual in activities that remind them of their youth e.g music)
• Picture time-table, photo staff rota, photos of activities and objects of reference
• Lay out clothes in the correct order
• Prompt about days of the week using activities /t.v programmes
• Use a calendar
• Talking Mats
• Easy Read information
Memory Aids
Eating and Drinking• Eating, drinking and swallowing skills will gradually
decrease as the dementia progresses
• Decreasing ability to control and manipulate food and drink in the mouth
• Swallowing may become more difficult and a safety issue
• Visual perception and spatial awareness difficulties

17/10/2018
33
Eating and DrinkingThe individual may present with the following:
• Difficulties recognising when hungry or thirsty and not remembering if they have eaten
• Deterioration in ability to control and manipulate food using crockery/cutlery
• Environmental distraction
• Difficulties recognising food and eating utensils
• Difficulties remembering how to eat
• Change in taste
• Difficulties getting food or drink to mouth
• May appear to resist attempts to feed
• Return of reflex actions e.g. sucking, biting, tongue movements
• Weight loss and dehydration are common
Assistive Technology
• Assistive technology can be very helpful at different stages in diagnosis and management
• Bed monitors• Door alarms• Seizure monitoring
• Colourful cutlery and plates• Lipped plates• Colourful toilet seats• Mobile phone tracking• Call alarms• Dosset boxes

17/10/2018
34
EpilepsyAt least 80% of individuals with Down syndrome will develop late onset
epilepsy due to the dementia
This is often the first time carers have thought about dementia
Staff are often anxious when a client has a seizure for the first time.
We provide epilepsy training
We have an epilepsy clinic
Seizure diaries/records are kept by staff and monitored in epilepsy clinic
Continence
• Continence skills will gradually decrease as the dementia progresses
• Urinary incontinence often occurs because the individual may• Be unable to recognise the “urge” sensation
• Forget to use the toilet regularly
• Be unable to find the toilet
• Be unable to undo buttons and zips quickly enough
• Have a UTI?
Consider a referral to continence service

17/10/2018
35
General Health Changes
• Having a learning disability and dementia reduces the ability to communicate pain and discomfort
• A change in behaviour or sudden deterioration in skills may be an indicator of ill health
• Always refer any possible physical illness to the GP
• It is important that you know how the individual communicates when they are in pain
Environment
We often recommend some subtle changes to the home environment to aid cognitive memory and independence for as long as possible
• Similar flooring in all areas, good lighting, red detail on toilet seats and doors and plain walls and carpets (perceptual problems)
• Signs on bathroom, cloakroom and bedroom doors at eye level (disorientation problems)
• Consideration of noise levels e.g. does the television and radio need to be on at the same time (concentration & over stimulation problems)
• Cover up mirrors at night (lack of recognition of own reflection)
• Make minor physical adaptations e.g. handrails (mobility problems)
• Safety – the individual’s home should be secure but not restrictive e.g exit doors could be monitored and fitted with alarms. You may need to consider a DOLs referral.

17/10/2018
36
Philosophy of Care
• Keep the individual at the centre (person centred not task orientated)
• Individuals with dementia need to have, or be
• Stress free
• Failure free
• Individualised care
• Cons istency without time pressures
• Staff need to
• Understand and know the person
• Understand dementia
• Think ahead and predict stressors
• Adopt a flexible approach
• Use what you a lready know
End of Life Care
• Our philosophy is to keep the client in their own home wherever possible.
• Best interest meeting to discuss how we can achieve this.
• Possible referrals to advocacy/IMCA.
• District nurse involvement (Gold Standard Framework).
• Involvement with primary health services.

17/10/2018
37
End of Life Care
• Discussions around the timing of DNAR. The reason for DNAR is not related to the LD.
• Dysphagia assessment.
• Referral to continuing care for assessment.
• Referral to OT/Physio regarding appropriate seating and beds.
• Emotional support for staff and families.
• Reassurance that staff are doing all they can.