Dr. Saleh M. Aldaqal MBBS, FRCSI,SBGS Assistant Professor and Consultant General And laparoscopic...
28
Endocrine surgery Dr. Saleh M. Aldaqal MBBS, FRCSI,SBGS Assistant Professor and Consultant General And laparoscopic Surgery(france), Department of Surgery, Faculty of Medicine, King Abdulaziz University.
-
Upload
jean-stevens -
Category
Documents
-
view
222 -
download
1
Transcript of Dr. Saleh M. Aldaqal MBBS, FRCSI,SBGS Assistant Professor and Consultant General And laparoscopic...

Endocrine surgery
Dr. Saleh M. Aldaqal MBBS, FRCSI,SBGS
Assistant Professor and Consultant General And laparoscopic
Surgery(france), Department of Surgery, Faculty of
Medicine, King Abdulaziz University.www.dr-aldaqal.com

Endocrine surgeryParathyroid - hyper and hypo parathyroidismAdrenal tumors - cushing syndrome - conn`s disease - pheochromocytomas - adrenocortical carcinoma - incidentilenomaPancreatic endocrine tumorsCarcinoid tumors

ParathyroidSuperior parathy. 4 th branchial pouchInferior parathy. 3 rd branchial pouch (
50% ectopic)90% 4 glands, 10% 5-6 glands.Both receive blood supply from inferior
thyroid artery.Direct feedback by Ca level, no pituitaty
control.PTH has direct effect on bone ( osteoclast)
and kidneys ( tubular reabsorption) and indirect effect on the GIT ( renal vitam. D ).

Hyper parathyrodismPrimary : due to disease in the gland as adenoma
(80%), hyperplasia ( 15%), carcinoma (5%) ( high ca. and PTH ) treatment : surgery
Secondary : compensatory response to hypoca. - CRF ( hyperphosphatemia, reduction in vitam. D ) - intestinal malabsorption syndrom ( ca. level at lower normal, high PTH ) treatment : calcium, vitam. D, phosphate binder Indication of surgery : sever renal osteodystrophy
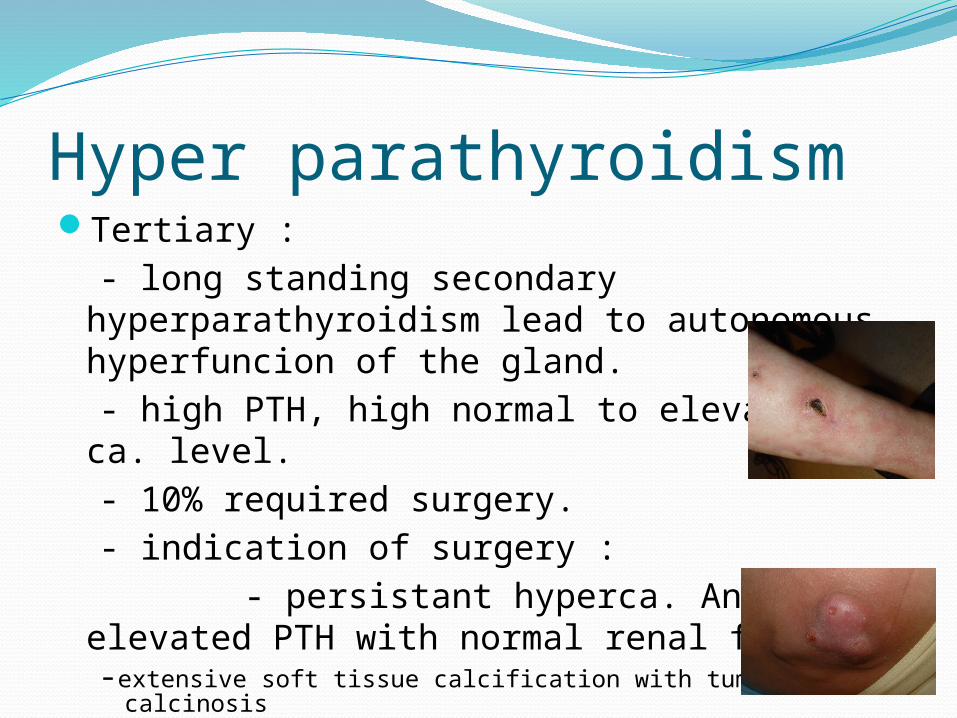
Hyper parathyroidismTertiary : - long standing secondary
hyperparathyroidism lead to autonomous hyperfuncion of the gland.
- high PTH, high normal to elevated ca. level. - 10% required surgery. - indication of surgery : - persistant hyperca. And elevated PTH
with normal renal function -extensive soft tissue calcification with tumoral calcinosis -calciphylaxis

Hypo parathyroidism Secondary to thyroidictomy90% dut to ischemia to the gland10% accidental removal of the glandSigns and symptomsTreatment asymptomatic, mild symptoms, sever
symptoms

Adrenal gland80% cortex - zona glomerulosa…..aldosteron
(mineralocorticoid) - zona fasciculata, reticularis ….cortison,
androgen (glucocorticoid) under ACTH control
20% medulla - adrenalin, noradrenalin

Normal Anatomy, Abdominal-pelvic CT
Liver Spleen
Inferior vena cava
aorta
Stomach
Vertebra
Ribs
Vertebra
Left kidney
Right kidney
Left portal vein
Left adrenal

Cushing syndromeDefenition Causes : - 90% iatroginc exogenous - 10% endogenous ( 70% pituitary adenoma, 29% adrenal
causes, 1% ectopic production due to carcinoma as ca. lung)
Adrenal causes : most commonly due to adenoma, followed by
carcinoma and rarly due to hyperpasia.

Cushing syndromeDiagnosis : - 24 h urinary free cortisol - to confirm the diagnosis , low dose
dexamethasone suppression test. - then ACTH level, if low, adrenal causes - if ACTH level high, then high dose
dexamethasone suppression test ( pituitary or ectopic ).

Conn`s disease ( primary hyperaldosteronism)
Aldosteron secretion is under control of renin-angiotensin system, serum potassium.
Sustained hypertension , Hypokalemia.
95% adrenal adenoma ( surgical)
5% adrenal hyperplasia (medical )

Pheochromocytomas Adrenal medulla10% tumor - 10% bilateral - 10% malignant - 10% extra adrenal ( paraganglia cells in
abdomen, carotid body, urinary bladder) - younger than 20 years of age - 10% MEN II

Pheochromocytomas Symptoms : headache, paroxysmal hypertensive
episode, palpitations, sweating..)Diagnosis - 24 h urinary catecholamines and metabolites ( metanephrines, VMA ) - CT- scan - MIBG isotop scan ( monoiodobenzylguanidine )Treatment : surgical - pre operative preparation with alph-
blocker as phenoxybenzamine , fluid…

Carcinoid tumorArise from neural crest cells.Site : - GIT : any site, most common is appendix,
ileum, rectum. - extraintestinal : bronchus and ovary.Prognosis depend on the size ; < 1 cm 20-
30% L.N metastasis. > 2 cm 80% L.N metastasis.
Lead to extensive fibrosis, fixation and kinking of the bowel.

Carcinoid tumorCan lead to carcinoid syndrome. - flushing, diarrhea, asthma, valvular heart
disease. - secret serotonin. - diagnosis : 24h urinary 5-HIAA - developed when there is extensive liver
metastasis, or extra intestinal tumor. - treatment : surgery, somatostatin

Pancreatic endocrine tumorInsulinomaWhipple`s triad - symtoms of fasting hypoglcemia. - fasting hypoglycemia < 50 mg/dl. - relieved by glucose administration.Single, benign tumor.Treatment : surgical

Gastrinoma Zollinger-Ellison syndrom.
Increase secretion of gastrin.
recuurant peptic ulcer and diarrhea.
Could associated with MEN I.

Glucagon-secreting tumor
DiabetsAnemiaWeight lossDVTCutaneous lesion ( necrolytic migratory
erythema)
THANK YOU



























