Dr ranjith mp,ventricular tachycardia in abnormal heart dr ranjith mp
111
Dr Ranjith MP Senior Resident Department of Cardiology Government Medical college Kozhikode
-
Upload
drranjithmp -
Category
Education
-
view
1.295 -
download
3
Transcript of Dr ranjith mp,ventricular tachycardia in abnormal heart dr ranjith mp

Dr Ranjith MP
Senior Resident
Department of Cardiology
Government Medical college
Kozhikode

Mechanisms of VT
VT arises distal to the bifurcation of the His bundle in the specialized conduction system, ventricular muscle, or combinations of both
Disorders of impulse formation
Enhanced automaticity
Triggered activity
Disorders of impulse conduction
Re-entry (circus movements)

Mechanisms of VTDisorders of impulse formation
Enhanced automaticity Can occur in virtually all cardiac tissues
Occurs due to increasing the rate of diastolic depolarization or changing the threshold potential
Can arise from cells that have reduced maximum diastolic potentials, often at membrane potentials positive to −50 mV

Mechanisms of VTDisorders of impulse formation
Automatic ventricular arrhythmias
Premature ventricular complexes
Ventricular tachycardia associated with:
Acute myocardial infarction or ischemia
Electrolyte and acid-base disturbances, hypoxemia
Increased sympathetic tone

Mechanisms of VTDisorders of impulse formation
Triggered activity
Pause-dependent triggered activity
Early afterdepolarization (phase 3)
Polymorphic ventricular tachycardia
Catechol-dependent triggered activity
Late afterdepolarizations (phase 4)
Idiopathic right ventricular tachycardia

Mechanisms of VTDisorders of impulse formation
Triggered activity
Figure A :- Early afterdepolarizations in phase 3 of the AP
Figure B :- Late afterdepolarizations seen in late phase 3 or phase 4 of the AP

Mechanisms of VTDisorders of impulse conduction
Fast Conduction PathSlow Recovery
Slow Conduction PathFast Recovery
Electrical Impulse Cardiac Conduction Tissue
Two distinct pathways that come together at beginning and end to form a loop
A unidirectional block in one of those pathways
Slow conduction in the unblocked pathway
Re-entry (circus movements)

Mechanisms of VTDisorders of impulse conduction
Fast Conduction PathSlow Recovery
Slow Conduction PathFast Recovery
Premature Beat Impulse Cardiac Conduction Tissue
An arrhythmia is triggered by a premature beat
The fast conducting pathway is blocked because of its long refractory period so the beat can only go down the slow conducting pathway
Repolarizing Tissue (long refractory period))

Mechanisms of VTDisorders of impulse conduction
The wave of excitation from the premature beat arrives at the distal end of the fast conducting pathway, which has now recovered and therefore travels retrogradely (backwards) up the fast pathway
Fast Conduction PathSlow Recovery
Slow Conduction PathFast Recovery
Cardiac Conduction Tissue
Re-entry (circus movements)

Mechanisms of VTDisorders of impulse conduction
On arriving at the top of the fast pathway it finds the slow pathway has recovered and therefore the wave of excitation ‘re-enters’ the pathway and continues in a ‘circular’ movement. This creates the re-entry circuit
Fast Conduction PathSlow Recovery
Slow Conduction PathFast Recovery
Cardiac Conduction Tissue
Re-entry (circus movements)

Mechanisms of VTDisorders of impulse conduction
Reentrant ventricular arrhythmias
Premature ventricular complexes
Idiopathic left ventricular tachycardia
Bundle branch reentry
Ventricular tachycardia and fibrillation when associated with chronic heart disease:
Previous myocardial infarction
Cardiomyopathy

Coronary Artery Disease
Dilated Cardiomyopathy
Bundle Branch Re-entry Ventricular Tachycardia
Arrhythmogenic Right Ventricular Cardiomyopathies
Hypertrophic Cardiomyopathy
After Surgery for Congenital Heart Disease

Coronary Artery Disease
Dilated Cardiomyopathy
Bundle Branch Re-entry Ventricular Tachycardia
Arrhythmogenic Right Ventricular Cardiomyopathies
Hypertrophic Cardiomyopathy
After Surgery for Congenital Heart Disease

Healed MI is the most frequent clinical setting for the development of sustained VT
The first episode of VT can occur years after infarct healing
Clinical presentation- tolerated sustained VT to SCD
Incidence reduced from 3% to 1%

Focal activation by abnormal automaticity in the ischemic
border zone
a/c ischemia activates KATP channels causing an increase in
extracellular K along with acidosis and hypoxia in the cardiac
muscle
Minor increases in extracellular K depolarize the
myocardiocyte’s RMP , which can increase tissue excitability
in early phases of ischemia

Focal discharge by Ca overload & triggered activity in the
form of delayed or early after-depolarizations - not been
proven experimentally

Reentry is the mechanism underlying the VT associated with
healed or healing MI (>95%)
The ability to reproducibly initiate and terminate VT with programmed ventricular extrastimuli- the sine qua non of reentry
Induction of VT in coronary disease is stimulation site specific
An inverse relationship of the extrastimulus coupling interval to the onset of the first tachycardia beat is observed in many VTs

Important determinants of arrhythmia risk after MI
The extent of myocardial necrosis
Presence of septal involvement
Degree of left ventricular dysfunction
Anatomic substrate – extensive scar
VT consistently arises from surviving myocytes within extensive areas of infarction
Conduction is slow & discontinuous, owing to fibrosis and abnormalities in gap junction distribution & function

Electrophysiologic substrate for VT develops in the first 2 weeks after MI - remain indefinitely
Triggers – Acute ischemia
– Surges in the autonomic tone
– Heart failure
Once sustained monomorphic VT occurs, risk continues indefinitely, even if acute ischemia & heart failure are adequately controlled
Josep Brugada et al JACC Vol. 37, No. 2, 2001:529–33

Reentry – macro/ micro reentry
Repolarization of individual myocardial cells not
homogenous. Some cells excitable, some refractory



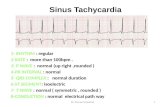
Sinus rhythm mapping in a patient with VT in the setting of extensive healed anterior infarction. The map is color-coded to represent bipolar electrogram voltage: red (representing dense scar) denotes = 0.5 mV, purple = 1.5 mV, and the intervening colors represent voltagevalues in between. Multiple inducible VTs of varied morphology were localized tocircuits within the scar

In the setting of an old MI, the ECG during VT is affected by
The size of infarction
The region of infarction
The region within the scar where the circuit is located
The proximity to the His-Purkinje system
The influence of concomitant pharmacological agents

Presence of Q waves (qR, QR or Qr) in related leads
Notched or wide QRS complexes
Low QRS voltage
Multiple ventricular tachycardia morphologies
Paroxysmal sustained episodes

Surface ECG tends to locate the reentry circuit exit rather than
the VT origin
Location should be defined in 3 axes:
septal vs lateral walls
superior vs inferior walls
apical vs basal regions
Bundle branch block patterns -sequence of ventricular activation

Lateral wall VT
RBBB pattern
Wider QRS complexes
Septal VT
LBBB pattern
Narrower QRS complexes

The QRS axis in inferior leads indicates the sequence of activation between the superior and inferior walls
Inferior MI
Superior axis (80%)
Anterior MI
Superior axis (55% )
Inferior axis (45%)

Predominant polarity of QRS complexes in precordial leads can help discriminate between VTs from the basal or the apical regions
VT from the apex
Negative concordant R progression
VT from the basal
Positive concordant R progression







The key determinant of hemodynamic tolerance
Tachycardia rate
Left ventricular function
Development of ischemia, and mitral insufficiency
Hemodynamic collapse – cardioversion
Intravenous procainamide, sotalol, and amiodarone have
been demonstrated to have superior efficacy

Goal of long-term therapy- prevention of SCD &
recurrence of symptoms
Asymptomatic NSVT with NLVEF- no treatment
Symptomatic NSVT in pts with NLVEF- betablockers
Cardiac arrest survivors / SUS VT in ↓LVEF- ICD
Primary pvt - ICD > Amiod- pvt of SCD

subendocardial resection of arrhythmogenic focus
Cryoablation
Laser vaporization
Photocoagulation





Patients resuscitated from VF when coronary revascularization is not possible, and there is evidence of prior MI and significant LV dysfunction
LV dysfunction due to MI who present with hemodynamically unstable VT
Primary prevention - LV dysfunction due to prior MI who are at least 40 days post-MI and have an LVEF 30%-40% & NYHA II or III
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

Primary prevention ICD is reasonable in patients with LV dysfunction due to prior MI who are at least 40 days post-MI, and have an LVEF 30%-35% & NYHA I
ICD implantation is reasonable in patients with post-MI with normal LV function and recurrent VT
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIII
\
IIaIIaIIa IIbIIbIIb IIIIIIIII

Coronary Artery Disease
Dilated Cardiomyopathy
Bundle Branch Re-entry Ventricular Tachycardia
Arrhythmogenic Right Ventricular Cardiomyopathies
Hypertrophic Cardiomyopathy
After Surgery for Congenital Heart Disease

Coronary Artery Disease
Dilated Cardiomyopathy
Bundle Branch Re-entry Ventricular Tachycardia
Arrhythmogenic Right Ventricular Cardiomyopathies
Hypertrophic Cardiomyopathy
After Surgery for Congenital Heart Disease

DCM has a propensity to the development of ventricular arrhythmias and sudden death
Incidence of DCM - 4 to 8 cases per 100,000 population
Incidence of VT – 50-60% DCM, resp for 8-50% deaths
Genetics - Relationship between individual genotypes and arrhythmogenicity is poorly understood

Multiple factors responsible for VT in DCM

Myocardial fibrosis/scar - may act as sites for reentry
At autopsy, extensive subendocardial scarring in the LV in 33% & multiple patchy areas of replacement fibrosis in 57%
Sustained stretch-induced shortening of refractory period
and AP duration, predisposing to reentry
Short, pulsatile, stretch-induced after depolarizations

Diastolic Ca overload caused by decreased sacrcoplasmic
reticulum Ca2+–adenosine triphosphatase pump
Afterdepolarizations induced by increased Na+-Ca2+ exchanger
activity
Hypokalemia, hypomagnesemia (often related to diuretic use)
Increased circulating catecholamines

Increased sympathetic tone
Purkinje system conduction delay
Increased endocardial surface area in dilated atrium or
ventricle
Drugs (antiarrhythmics, digoxin, sympathomimetic)

Macro reentry - dominant mechanism
Bundle branch reentry ventricular tachycardia (BBRVT) is the most characteristic
BBRVT - Responsible for VT in up to 41% of DCM
Macro-reentrant circuit involving the His-Purkinje system, usually with antegrade conduction over the RBB and retrograde conduction over the LBB

Severity of LV dysfunction - most powerful predictor
SCD is significantly greater in patients with syncope
Laboratory values - low serum sodium and increased plasma norepinephrine, renin, and ANP,BNP
LBBB & of first- and second-degree AV block has been associated with poor outcome

Vesnarinone Trial (VEST) showed a significant association between the degree of QRS prolongation and mortality
Gottipaty V, et al. J Am Coll Cardiol 33:145A, 1999

ACEI – reduction in SCD due to VT (37% vs 46%)
new VT developed less frequent at 1,2 yrs in enalapril group (VHeFT-II trial)

Amiodarone
Used only on specific arrhythmic indications
Reduces ICD shock frequency , without worsening heart failure (SCDHeFT)
Implantable Cardioverter-Defibrillators
AMIOVIRT- No difference in mortality ( amio vs ICD)
SCD-HeFT - Significant reduction in total mortality in ICD group
Catheter ablation

Biventricular pacing- severe drug refractory heart failure , in elderly
Improve systolic function by shortening the duration of mechanical systole and increasing dP/dt
Improve diastolic function by prolonging diastolic filling time
Reduce presystolic MR by earlier activation of the lateral papillary muscle without the adverse effect on the sympathetic nervous system seen with inotropic agents

Coronary Artery Disease
Dilated Cardiomyopathy
Bundle Branch Re-entry Ventricular Tachycardia
Arrhythmogenic Right Ventricular Cardiomyopathies
Hypertrophic Cardiomyopathy
After Surgery for Congenital Heart Disease

Coronary Artery Disease
Dilated Cardiomyopathy
Bundle Branch Re-entry Ventricular Tachycardia
Arrhythmogenic Right Ventricular Cardiomyopathies
Hypertrophic Cardiomyopathy
After Surgery for Congenital Heart Disease

Commonly occurs in disease with severe LV dysfunction like DCM & conduction abnormalities in the HPS
BBR VT may also be seen in:
Myotonic dystrophy
Hypertrophic cardiomyopathy
Ebstein anomaly
Following valvular surgery
Proarrhythmia due to Na channel blockers
Presyncope, syncope or sudden death - VT with fast rates > 200 bpm

Macro re-entrant circuit employing
His Bundle
Both bundle branches
Ramifications of left bundle
Transeptal myocardium

May present with LBBB or RBBB morphology depending on the antegrade conduction
LBBB morphology is common
BBR –LBBB: - antegrade direction -RB & reterograde LB
BBR –RBBB:- antegrade direction-LB & reterograde RB

VT QRS
Morphology
Activation
Sequence
LBBB LB-H-RB-V
RBBB RB- H-LB-V

Surface ECG in sinus rhythm - non-specific or typical bundle branch block patterns with prolonged QRS duration
Total interruption of conduction in one of the BB would theoretically prevent occurrence of reentry
Can occur in patients with relatively narrow QRS complex - functional conduction delay

Electrophysiologic features
During tachy QRS morphology is commonly LBBB type
His electrograms precede each V
HV interval during tachycardia > HV in baseline
Changes in V–V interval follow the changes in H–H
Delay in HPS conduction facilitates induction

Electrophysiologic features

Electrophysiologic features
Block in Bundle branches or HPS will terminate the tachy
Ablation of RB renders tachycardia noninducible
VT of myocardial origin mimics BBR-LB pattern VT – can be differentiated by the presence of rapid intrinsicoid deflection due to initial ventricular activation through the HPS in the later

The reentrant circuit involves superior and inferior division of the left bundle
RBBB and anterior or posterior fascicular block is present during sinus rhythm
usually has RBBB morphology
Antegrade - LAF & retro – LPF –RAD
Antegrade- LPF & retro – LAF- LAD

HV interval shorter than sinus rhythm
LB potential before HIS deflections

High recurrence rate after drugs
RFA - first line therapy
Treatment of choice for BBR VT is ablation of the RB
A PPI should be implanted if the post-ablation HV interval is 100 ms or longer
ICD implant should be considered if myocardial VT occur spontaneously or are inducible or if EF < 35%

Coronary Artery Disease
Dilated Cardiomyopathy
Bundle Branch Re-entry Ventricular Tachycardia
Arrhythmogenic Right Ventricular Cardiomyopathies
Hypertrophic Cardiomyopathy
After Surgery for Congenital Heart Disease

Coronary Artery Disease
Dilated Cardiomyopathy
Bundle Branch Re-entry Ventricular Tachycardia
Arrhythmogenic Right Ventricular Cardiomyopathies
Hypertrophic Cardiomyopathy
After Surgery for Congenital Heart Disease

Most frequent – ARVD
Extensive myocardial fibrosis - substrate for reentry
RV outflow tractRV apexRV inflow segments
Marcus fi et al.Circulation 1982; 65:384–398

1. Prolonged QRS duration ≥ 110 ms in V1-V3 (Sens-55%, Spec-100%)
2. T wave inversion in right precordial leads (Seen in 60%)
3. Epsilon wave (Seen in 30%)
4. Low-voltage QRS amplitude
(Indicate severe cases)
ECG in sinus rhythm

Ventricular arrhythmias are usually exercise-related
Sensitive to catecholamines
Most Common- LBBB morphology VT
Up to 12 VT morphologies have been reported in a single patient
RBBB VT - LV involvement or a left septal breakthrough site


VT in ARVD may be confused with RVOT VT
O’Donnell D ET et al. Eur Heart J. 2003;24:801-810, 2003.

High Risk Features
Younger patients
Recurrent syncope
History of cardiac arrest or sustained VT
Clinical signs of RV failure or LV involvement
Patients with or having a family member with the high risk ARVD gene (ARVD2)
Increase in QRS dispersion ≥ 40 msec
QRS dispersion = max measured QRS minus min measured QRS

Documented VT/VF on c/c OMT, have reasonable expectation of survival- ICD to prevent SCD
Severe disease LV inv, FH of SCD, undiagnosed syncope, on c/c OMT
Amiodarone or sotalol effective , when ICD not feasible
Ablation can be adjunctive
EP testing might be useful for risk assessment
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIII
B
IIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIII
C
IIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIII
CIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIII
C
IIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIII
C
IIaIIaIIa IIbIIbIIb IIIIIIIII

Coronary Artery Disease
Dilated Cardiomyopathy
Bundle Branch Re-entry Ventricular Tachycardia
Arrhythmogenic Right Ventricular Cardiomyopathies
Hypertrophic Cardiomyopathy
After Surgery for Congenital Heart Disease

Coronary Artery Disease
Dilated Cardiomyopathy
Bundle Branch Re-entry Ventricular Tachycardia
Arrhythmogenic Right Ventricular Cardiomyopathies
Hypertrophic Cardiomyopathy
After Surgery for Congenital Heart Disease

SCD in adults with asymptomatic HCM- 1%
NSVT – 8%
On 24-hr Holter -90% have ventricular arrhythmias
J Am Coll Cardiol 45:697-704, 2005
Prevalence of ventricular and supraventricular arrhythmias on24-hour Holter recording in 178 patients from a community-based population of patients with hypertrophic cardiomyopathy

In LVH action potential prolongation is due to a decrease in Ito. This results in nonhomogeneous repolarization and propensity for EAD
Hypertrophied myocytes may produce DAD due to an increase in Ca load
Abnormal pacemaker current (If) has been reported in LVH. Intensity of this current increases with beta adrenergic stimulation
In LVH the density of Ito is reduced. The density of ICaLand IK is unchanged and density of If is increased

Pharmacologic Treatment
Beta-blockers, verapamil, amiodarone
Long term prophylactic pharmacologic therapy now not recommended in high-risk population
ICD implantation is reasonable for patients who have 1 or more major risk factor for SCD. (Level of Evidence: C)

1. Family history of premature HCM-related death
2. Unexplained syncope, particularly in young patients, or if demonstrated to be arrhythmia-based
3. Frequent, multiple, or prolonged episodes of NSVT
4. Hypotensive or attenuated BP response to exercise
5. Extreme LVH with maximum wall thickness ≥ 30 mm
Presence or magnitude of LVOT obstruction has not proved to be a consistently strong independent risk factor for SCD in HCM and therefore does not constitute a sole justification for prophylactic ICD implantation

Coronary Artery Disease
Dilated Cardiomyopathy
Bundle Branch Re-entry Ventricular Tachycardia
Arrhythmogenic Right Ventricular Cardiomyopathies
Hypertrophic Cardiomyopathy
After Surgery for Congenital Heart Disease

Coronary Artery Disease
Dilated Cardiomyopathy
Bundle Branch Re-entry Ventricular Tachycardia
Arrhythmogenic Right Ventricular Cardiomyopathies
Hypertrophic Cardiomyopathy
After Surgery for Congenital Heart Disease

Ventricular Tachycardia in Patients after Surgery for Congenital Heart Disease
Most information concerning patients with VT and congenital heart disease pertains to TOF
VT in these patients are due to the effect of
Years of chronic cyanosis
Presence of a ventriculotomy
Elevation of RV pressures
Severe pulmonic regurgitation with RV dysfunction
These factors lead to myocardial fibrosis, resulting reentrant circuits

Ventricular Tachycardia in Patients after Surgery for Congenital Heart Disease
Mechanism of VT is reentry involving the RVOT, either at the site of anterior rt. ventriculotomy or at VSD patch
The incidence of VT significantly higher in patients with RVSP >60 mm Hg and RVEDP > 8 mm Hg
Zeltser et al showed RV volume overload is the most important predictor of inducible ventricular arrhythmias
J Thorac Cardiovasc Surg 130:1542-1548, 2005

Ventricular Tachycardia in Patients after Surgery for Congenital Heart Disease
The risk of VT can be assessed by QRS duration
Syncope & VT- squares Sudden death- trianglesSyncope with Afl- star
Gatzoulis MA et al. Circulation 95:401-404, 1997

Ventricular Tachycardia in Patients after Surgery for Congenital Heart Disease
Treatment
Antiarrhythmics medication
Radiofrequency catheter ablation
Surgical Cryoablation
ICD implantation
A combined approach of correcting significant structural abnormalities with intra-operative EP-guided ablation may reduce the potential risk of deterioration in ventricular function

References- Journal1. Relationship between the 12-lead electrocardiogram during ventricular tachycardia
and endocardial site of origin in patients with coronary artery disease. John M. et al. Circulation 77, No. 4, 759-766, 1988.
2. Coronary Artery Revascularization in Patients With Sustained Ventricular Arrhythmias in the Chronic Phase of a Myocardial Infarction: Effects on the Electrophysiologic Substrate and Outcome. Josep Brugada et al JACC Vol. 37, No. 2, 2001:529–33
3. Ventricular Tachycardia in Coronary Artery Disease . B. Benito, M.E. Josephson / Rev Esp Cardiol. 2012;xx(x):xxx–xxx
4. Role of Ablation Therapy in Ventricular Arrhythmias. Mithilesh K. Das et al. Cardiol Clin26 (2008) 459–479
5. Ventricular Arrhythmias in Heart Failure Patients Ronald Lo, Henry H. Hsia. Cardiol Clin26 (2008) 381–403

References- Journal5. A Comprehensive Approach to Management of Ventricular Arrhythmias, Fred
Kusumoto. Cardiol Clin 26 (2008) 481–496
6. Relationship between the 12-lead electrocardiogram during ventricular tachycardia and endocardial site of origin in patients with coronary artery disease, J M Miller et al. Circulation. 1988;77:759-766
7. Arrhythmogenic right ventricular cardiomyopathy: A cause of sudden death in young people, A. Thomas mcrae et al, Cleveland clinic journal of medicine volume 68 ,No.5, 2001:459-467
8. Ventricular arrhythmias in idiopathic dilated cardiomyopathy K Von Olshausen et al. Br Heart J 1984; 51: 195-201
9. Non-Sustained Ventricular Tachycardia in Hypertrophic Cardiomyopathy: An Independent Marker of Sudden Death Risk in Young Patients. Lorenzo Monserrat et al, Vol. 42, No. 5, 2003:873–9
10. Sustained Ventricular Tachycardia in Adult Patients Late After Repair of Tetralogy of Fallot. David A. Harrison et al. JACC Vol. 30, No. 5,November 1, 1997:1368–73

References – Text Books
1. Zipes 5th ed. Cardiac Electrophysiology From Cell to Bedside
2. Basic Cardiac Electrophysiology for the Clinician .2nd ed. José Jalife, MD
3. Clinical arrhythmology and electrophysiology: a companion to Braunwald’s heart disease 8th ed.
4. Handbook of Cardiac Electrophysiology. Andrea Natale MD.
5. Management of Cardiac Arrhythmias, edited by Leonard I. Ganz, MD, 2002

THANK YOU

MCQ-1
True statement regarding AVRD
A. Ventricular arrhythmias are usually exercise-related
B. Sensitive to catecholamines
C. Most Common- LBBB morphology VT
D. All are true

MCQ-1
True statement regarding AVRD
A. Ventricular arrhythmias are usually exercise-related
B. Sensitive to catecholamines
C. Most Common- LBBB morphology VT
D. All are true

MCQ-2
12 lead ECG of BBR-VT is given below. The antegrade conduction through------------
A. Right bundle branch
B. Left bundle branch
C. Left posterior fascicle
D. Left anterior fascicle

MCQ-2
12 lead ECG of BBR-VT is given below. The antegrade conduction through------------
A. Right bundle branch
B. Left bundle branch
C. Left posterior fascicle
D. Left anterior fascicle

MCQ-3
Exists site of the VT circuit given below is ?
A. LV lateral wall
B. Septum
C. Right ventricle
D. Both B & C

MCQ-3
Exists site of the VT circuit given below is ?
A. LV lateral wall
B. Septum
C. Right ventricle
D. Both B & C

MCQ-4
A 45yr old smoker with past history of hospitalization for chest pain presented to causality with palpitation and hypotension. Patient was stabilized with DC cardio version and taken to echo lab. His presentation ECG shown below. Echo likely to show?
A. LV apical aneurysm
B. RWMA anterior wall
C. RWMA Inferior wall
D. RV outflow aneurysm

MCQ-4
A 45yr old smoker with past history of hospitalization for chest pain presented to causality with palpitation and hypotension. Patient was stabilized with DC cardio version and taken to echo lab. His presentation ECG shown below. Echo likely to show?
A. LV apical aneurysm
B. RWMA anterior wall
C. RWMA Inferior wall
D. RV outflow aneurysm

MCQ-5
A 39 yr old smoker with hypotension in ED was stabilized with DC cardio version and his echo is shown below(Left side) . His presentation ECG is most likely to be ?
AB
C D

MCQ-5
A 39 yr old smoker with hypotension in ED was stabilized with DC cardio version and his echo is shown below(Left side) . His presentation ECG is most likely to be ?
AB
C D

MCQ-6
All are true about BBR- VT except?
A. High recurrence rate after drugs
B. Treatment of choice for BBR VT is ablation of the RB
C. Usually has LBBB morphology
D. V precede each his electrograms

MCQ-6
All are true about BBR- VT except?
A. High recurrence rate after drugs
B. Treatment of choice for BBR VT is ablation of the RB
C. Usually has LBBB morphology
D. V precede each his electrograms

MCQ-7
VT in post TOF repair patients are due to the effect of all except?
A. Years of chronic cyanosis
B. Presence of a ventriculotomy
C. Elevation of RV pressures
D. Severe pulmonic regurgitation with RV dysfunction
E. None

MCQ-7
VT in post TOF repair patients are due to the effect of all except?
A. Years of chronic cyanosis
B. Presence of a ventriculotomy
C. Elevation of RV pressures
D. Severe pulmonic regurgitation with RV dysfunction
E. None

MCQ-8
Sudden death risk factors in HCM are all except?
A. Family history of premature HCM-related death
B. Unexplained syncope, particularly in young patients, or if demonstrated to be arrhythmia-based
C. Hypotensive or attenuated BP response to exercise
D. Presence or magnitude of LVOT obstruction

MCQ-8
Sudden death risk factors in HCM are all except?
A. Family history of premature HCM-related death
B. Unexplained syncope, particularly in young patients, or if demonstrated to be arrhythmia-based
C. Hypotensive or attenuated BP response to exercise
D. Presence or magnitude of LVOT obstruction