Dr. Quillin on Office Emergencies at TAPA 2014
21
Robert L. Quillin, MD, FAAP
-
Upload
rlquillin -
Category
Health & Medicine
-
view
205 -
download
0
Transcript of Dr. Quillin on Office Emergencies at TAPA 2014

Robert L. Quillin, MD, FAAP

Disclosures
Speaker and consultant for VayaPharma, makers of Vayarin
Previous research support provided by PernixTherapeutics

Presentation Outline
Emergencies in the outpatient clinic setting
Making “quick look” assessments
Triage, treat or transfer approach to the sick patient
Office staff and practical management of patient
Parent/caregiver in the treatment plan

This is an emergency . . .

This is sNOT!
Fever
Cough
Vomiting
Stomach and abdominal
pain
Skin rash
Earaches
Sore throat
Injury, head, neck or face
Headache
Facial laceration
Somewhere in between
National Hospital Ambulatory Medical Care Survey:
2010 Emergency Department Summary Tables

What are we talking about then?
Asthma
Fracture
Appendicitis
Seizure
Anaphylaxis
Concussion
Rash
Laceration
Cancer


Definitions
What providers perceive
“to become aware of, to know, or identify by means of the senses”
What parents believe
“to have confidence in the truth, the existence, or the reliability of something, although without absolute proof that one is right in doing so”
What grandmothers know
“to perceive or understand as fact or truth; to apprehend clearly and with certainty”
Behind door number 1 . . .
Check pulse
Call 911
Remember ABC’s
Direct staff, reassure parents
Make a decision
Triage, Treat, or Transfer
Know limits of parents
Know limitations of staff
Know your own limitations
Know your hospital/ER limitations


Case #1: Fever
6mo fever to 104 over last two days. No sick contacts, no daycare, vaccines UTD
VS: T 101.2
PE: Feeding on bottle, PE wnl
Labs: CBC with WBC 18.7, 57%G, UA not collected
Triage, treat and/or transfer?PEARL: DON’T FORGET THE UA

Case #2: Fall
4mo unrestrained rolls out of carrier from counter to tile floor
VS: T 98.2, P 120
PE: Being held by father, smiling, looking around
Crepitus R parietal skull
Labs/image: None, CT Head
Triage, treat and/or transfer?
PEARL: BUCKLE UP!

Case #3: Wheezing
7yo with known h/o wheezing, fever 101. Had RSV as infant.
VS: T 99, pulse ox 88%
PE: Quiet, retrax present, no wheezing?
Labs: None, CXR?
Triage, treat and/or transfer? PEARL: SAY YOUR ABC’s?

W61.92 Struck by other birdsZ63.1 Problems in relationship with in-lawsW45.8XXA Other foreign body or object entering though
skin, initial encounterV52.2XXA Person on outside of pick-up truck or van
injured in collision with two or three-wheeledmotor vehicle in nontraffic accident
V00.32 Snow-ski accidentX92.0 Assault by drowning and submersion while in
bathtubW00.1 Fall from stairs and steps due to ice and snowV97.33XD Sucked into jet engine, subsequent encounter
ICD-10 FOLLIES
David Pittman, Med Page Today

Case #4: Foreign body
18 mo swallowed a nickel, no vomiting, no cough
VS: T 98.7
PE: waddling around exam room, NAD
Labs/image: CXR/KUB
Triage, treat and/or transfer? PEARL: NICKELS ARE GOOD, BATTERIES AND MAGNETS ARE BAD
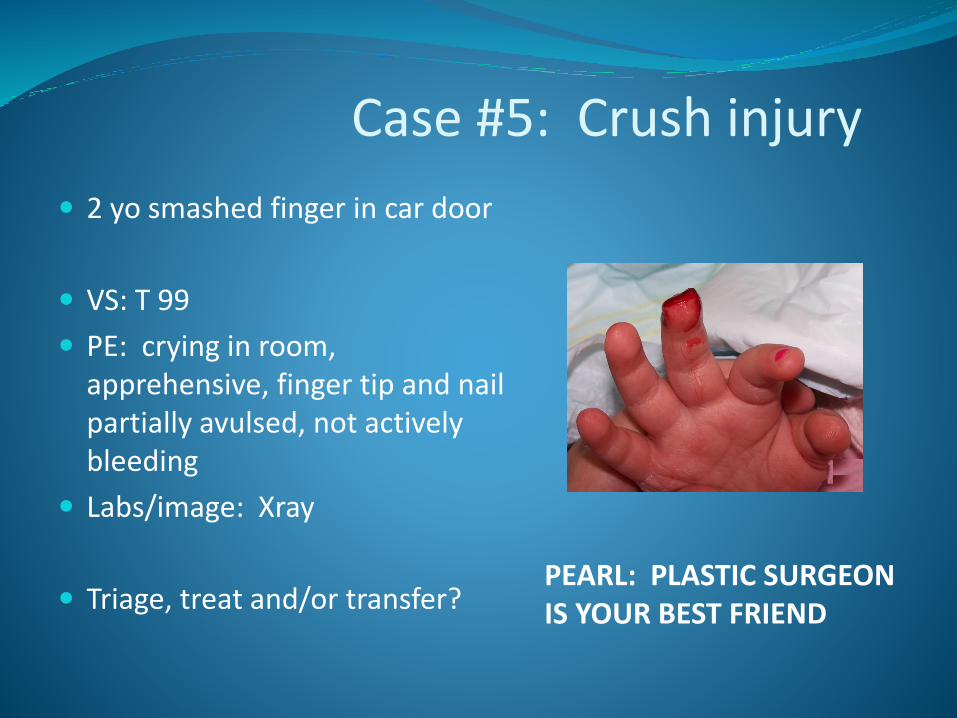
Case #5: Crush injury
2 yo smashed finger in car door
VS: T 99
PE: crying in room, apprehensive, finger tip and nail partially avulsed, not actively bleeding
Labs/image: Xray
Triage, treat and/or transfer?PEARL: PLASTIC SURGEON IS YOUR BEST FRIEND

Case #6: Nodes 5yo with recurrent fever to 102,
swollen glands, recent dx of mono after 5 days of fever
VS: T 101.8, P 100
PE: pale, diffuse cervical LAD, guarding RUQ, bruising
Labs/image: WBC 52K, H/H wnl, plts 30,000
Triage, treat and/or transfer?PEARL: BEWARE OF NODES

Don’t forget the patient comes first!

Thank you TAPAand
safe travels!



![WELCOME [tapa.memberclicks.net]...13 15 4 CONTENTS TaPa Editorial MunIES PILLAI, Editor editor@tapa-apac.org LEO WAn LInG wanling@tapa-apac.org Marketing DERICk DInG derick.ding@tapa-apac.org](https://static.fdocuments.in/doc/165x107/60e205162f6a6046c35127c1/welcome-tapa-13-15-4-contents-tapa-editorial-munies-pillai-editor-editortapa-apacorg.jpg)