Dr P V Kotecha
62
Child Anemia Feasibility Study: Approaches and Lessons Learnt S R Nagar – Uttar Pradesh Presentation at XIII Annual Conference of Indian Association of Preventive & Social Medicine UP & Uttarakhand Chapter Dehradun – Uttarakhand 31st October, 2010 Prof Prakash V Kotecha Country Representative, A2Z, the USAID Micronutrient Project, New Delhi, India Ex Professor and Head, PSM Dept, Medical College, Baroda, Gujarat [email protected]/[email protected]
-
Upload
iapsmupukcon2010 -
Category
Education
-
view
1.676 -
download
4
description
Transcript of Dr P V Kotecha

Child Anemia Feasibility Study: Approaches and Lessons LearntS R Nagar – Uttar Pradesh
Presentation at XIII Annual Conference of
Indian Association of Preventive & Social Medicine
UP & Uttarakhand Chapter Dehradun – Uttarakhand
31st October, 2010Prof Prakash V Kotecha
Country Representative,
A2Z, the USAID Micronutrient Project, New Delhi, India
Ex Professor and Head, PSM Dept, Medical College, Baroda, Gujarat

Iron: The Scope of the ProblemThe World Health Organization (WHO) has categorized iron deficiency as one of the top ten most serious health problems in the modern world. Iron deficiency anemia (IDA):– Impairs the mental development of over 40% of the
developing world's infants and reduces their chances of attending or finishing primary school
– Decreases the health and energy of approximately 500 million women and leads to approximately 50,000 deaths in childbirth each year
– Is complex because it requires increased iron intake at critical stages of the life- cycle - before and during pregnancy and throughout early childhood
.
Source: http://www.micronutrient.org/english/view.asp?x=579

Iron: The Scope of the Problem
– Iron deficiency has assumed even greater importance as evidence accumulates linking iron deficiency with mental impairment.
– Various tests of cognitive and psychomotor skills associate lack of iron during infancy and early childhood with significant levels of disadvantage, affecting IQ scores by as much as 5 to 7 points.
– Millions of children might be unable to complete primary school due to the impeded cognitive development they sustained as newborns and young children who couldn't get enough iron and iodine.
Source: http://www.micronutrient.org/english/view.asp?x=579

• Reducing anemia will decrease maternal and perinatal mortality, improve cognitive development and schooling in children, and increase physical capacity and work productivity in adults.
• About 42 percent of pregnant women and 47 percent of preschool children worldwide are anemic.
• The most common cause of anemia is iron deficiency, which is associated with 115,000 maternal deaths and 591,000 perinatal deaths each year (Stolzfus et al., 2004).
Dr. Prakash V. Kotecha
4
Iron: The Scope of the Problem

5
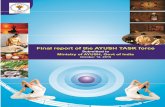
Anemia in Children
74.279.2
73.8
85.1
0
20
40
60
80
100
India UP
NFHS II 1998-99 NFHS III 2005-06
Anemia failed to decrease…and at present highest ever
Dr. Prakash V. Kotecha

6
Current GOI Guidelines: April 2007Relevant to children
• Current GOI Guidelines: April 2007Relevant to children
• Children 6-60 months to be given IFA syrup• Dose is 20 mg iron and 100 microgram folic acid in one ml
per day• Total dose/days not mentioned (as per IMNCI)• For safety reason to be dispensed in bottles so designed
that only one ml can be dispensed at a time • DFS, Sprinkles, dispersible tablets, fortified rice and other
alternatives need to be explored as additional/alterative therapy
• Source: No Z.28020/50/2003-CH GOI 23rd April 2007
Dr. Prakash V. Kotecha

Dr. Prakash V. Kotecha
7
Current Program guideline for anemia control for young children
• Screening of all children for anemia• Those found clinically suffering from anemia appropriate
treatment be given • This has come with 10th five year plan objectives and
goals.• However actually what is followed at present is
screening by ANM and those found anemic are given IFA when available
• Calculation of IFA small tablets (and currently provided IFA syrup bottles) also based on this criteria, they are not sufficient in number if and when all eligible children will receive them.

Dr. Prakash V. Kotecha
8
Source: http://pariwarkalyan.up.nic.in/mch-intro.htm 17/09/2010

Policy on Anemia Control: 1991
• Acknowledges importance and consequences of anemia in mothers and children
• Recommends integrated approach (ICDS-PHC)• Stresses on diet first (with lists) and on counseling• Recommends 100 small IFA for ALL children/year• Recommends controlling worm and other infections• Screening and special attention to severe anemia
9
Dr. Prakash V. Kotecha

NFHS III (2005-06) India Data
Age in Months
10
Dr. Prakash V. Kotecha

Anemia by Age Group
11
Dr. Prakash V. Kotecha

12
Child Anemia Feasibility Study Why UP?
Source: DLHS III (2007-08) Much Larger Sample Size90,000+ HH UP
38
7
23
0
20
40
60
80
100
Have electricity Use piped drinkingwater
Live in a puccahouse
UP

What is this study about ?• Child anemia control requires a package of
services not just iron alone.• Is it FEASIBLE to provide this package of
services to children in rural UP?• Is it possible to implement the program within
the existing system?• Do front line workers have the capacity to grasp
and deliver what is necessary to control child anemia?
Dr. Prakash V. Kotecha
13

Gyanpur
14
Study area
Dr. Prakash V. Kotecha
Handia

15
Study areaDistrict
State
S. R. Nagar,
UP
Block Gyanpur
Total population 2,65,678
No. of Sub-centers 32
No. of ANM 29
No. of AWC 187
Children 6-23 14000
Control block Handia, Allahabad districtDr. Prakash V. Kotecha

16
Child Anemia Feasibility Study: Steps• Formative Research• Based on the findings and recommendation of TAG
– Comprehensive package of services for intervention – Attempted through the system within system guidelines
• Training and Capacity building of AWW/ANM/ASHA and others providing services
• Enhanced Monitoring and evaluation– Anemia Prevalence– Worm prevalence– IFA syrup stock and distribution– Morbidity data for study and control area to check for morbidity in study area with
reference to iron supplementation if any
• Follow up with AWW/ANM for distribution and tracking the supply of IFA syrup
• Post training support (mentoring) by ICDS sector meeting and joint block meeting facilitation by field staff
• Ensuring anemia control and worm control in mothers

17
Comprehensive Package of Interventions• Improving nutritional status by addressing complementary
feeding practices appropriate to the age and ensuring energy rich dense food adequate in quality and quantity.
• Increasing iron intake of the target population through – Iron supplementation in form of syrup one ml twice a week
(GOI policy) using dropper only (discontinue when sick)– Improving breast feeding practices
• Control of infections – Hookworm by deworming and improved hygiene practice – Malaria (EDPT)
• Increasing iron stores at birth by improving the iron status of pregnant women with better ANC and IFA
Dr. Prakash V. Kotecha

Scenario at the Start of the Feasibility Study in Gyanpur Block
Dr. Prakash V. Kotecha
18

19
Dr. Prakash V. KotechaSource: NFHS III & A2Z study 2007-08
Anemia Prevalence at the starting of the Feasibility Study (6-23 m)

20
54.4
14.2 11
74.6
0102030405060708090
100
Ascariasis TrichurisTrichirura
Hook worm Any Infection
Helminthes Study Children in UP
N=472 (Gyanpur Block)
Source: Awasthi et al, 2008Dr. Prakash V. Kotecha

21
IFA Consumption at the starting time 2008 Baseline study
2 40
20
40
60
80
100
Intervention Block Non Intervention Block
Uttar Pradesh
Consumed Iron
Dr. Prakash V. KotechaSource: A2Z study 2007-08

22
Capacity Building of Frontline Providers• ALL ANM (33), AWW (209), ASHA (203) Supervisors of
ICDS (6) and LHV (Supervisors of ANM) (6) total 493• 3 day, highly interactive training that covered (March 08 to
Sept 08 total 22 trainings)– tracking pregnant women, – early and complete registration, IFA for every pregnant mother with
counseling for consumption and reasons to continue consumption– identify target children, – Counseling for IFA syrup, (how, when, where and why, how to
preserve, what precaution to take, where to store), for IYCF (energy dense adequate quality and quantity to be fed timely and responsively)
– Deworming when and how to dose (1yr onwards six monthly)– How to prevent malaria and protect form malaria and advocacy for
early diagnosis and prompt treatment for fever/malaria
Dr. Prakash V. Kotecha

23
Capacity Building of Frontline Providers• Follow up with AWW/ANM for distribution and tracking
the supply of IFA syrup– From District to Block– From Block to sub-health center and AWC– From AWC to beneficiary
• Post training support (mentoring) by ICDS sector meeting and joint block meeting facilitation by field staff
• IEC Material (for HW and beneficiary)and Training to use them
Dr. Prakash V. Kotecha

24
Anemia Status of Health workers
68.20% 65.70%
56.10%50.00%
61.10%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
ANM ASHA AWW SUPERVISOR Total
N=288

Dr. Prakash V. Kotecha
25

Dr. Prakash V. Kotecha
26IEC
Material in form
of calendar











IFA Syrup Supply Tracking all the way…
• Assumption was to give IFA in the month of May and follow up children for 9-12 months for their regular consumption
• Continuous monitoring only can improve the situation and detect issues
Dr. Prakash V. Kotecha
37
100
21.6
80
20.6
6.9
67.4
32.6
17.5 19
81
69
0
10
20
30
40
50
60
70
80
90
100
May
June Ju
ly
Augus
t
Supply and Distribution of IFA syrup staus from May to August 2008 in Gyanpur
Stock at Block Supply to ANM Distribution to ben.

Program Period
• Started Training for the program Feb 2008. IFA syrup was supplied in May 2008 and repeat supply was required after one year. 15000 IFA syrup bottles were supplied each time
• A2Z Program Support continued till Dec 2009. End line study was conducted in January 2010.
Dr. Prakash V. Kotecha
38

On going Monitoring LQAS
39
FOCUS
LQAS I (Sept. 08)
LQAS II (Feb. 09)
LQAS III (Aug. 09)
Advice on Anemia 46 34 75
IFA syrup Received 66 45 73
Benefits Explained 44 33 65
IFA consumed in last 7 days 59 15 50
Complementary Feeding Advice 28 51
Complementary Feeding Practice 14 11
Anemia Prevalence 95 87 86
Dr. Prakash V. Kotecha

RESULTS OF THE END LINE STUDY
Dr. Prakash V. Kotecha
40

End Line Study Children
Dr. Prakash V. Kotecha
41
District BlockNumber of mothers of
children aged 6-23 months (total sectors)
Sant Ravi Das Nagar Gyanpur 304
Allahabad Handia 331
Total 635

Religion & Caste of children studied
Dr. Prakash V. Kotecha
42
CharacteristicsProject Block
(Gyanpur)Comparison Block
(Handia)Religion Endline Baseline Endline Baseline
Hindu 93.4 93.8 93.4 94.2Muslim 6.3 6.2 6.3 5.8
Scheduled caste 24.3 30.8 24.3 22.6
Scheduled tribe 2.6 0.0 2.6 1.3
Other backward caste 44.7 41.6 44.7 55.5
Total N304 305 331 310

Standard of living & Literacy
Dr. Prakash V. Kotecha
43
Standard of living
Percent Households
Project Block (Gyanpur)
Comparison Block (Handia)
Low80.6 25.7
Medium14.8 33.5
High 4.6 40.8
Illiteracy
Illiterate54.3 37.8
Total N 304 331

ANC Coverage of Mothers
Dr. Prakash V. Kotecha
44

IFA Received by Mothers of children 6-23 months during their pregnancy
2 4
79
61
0
20
40
60
80
100
Gyanpur Handia
Baseline
Endline
Dr. Prakash V. Kotecha
45

IFA Consumption by Mothers
Dr. Prakash V. Kotecha
46

Anemia among children IFA Consumption by Mothers
Dr. Prakash V. Kotecha
47

IFA Syrup Received by Children 6-23 months
Dr. Prakash V. Kotecha
48

IFA Syrup Knowledge among mothers of children who received syrup
Dr. Prakash V. Kotecha
49

IFA Syrup Consumption & Side effect
• 92.6 % of children who received iron consumed it. 94% of these children were administered doses by the mother
• Only 13% had consumed more than 50 doses; while 35% consumed less than 10 doses and 36% consumed between 10 and 50 doses !
• Only 21% of children’s mother complained about side effects; 4/5th of these were black color stool and 1/5th had nausea as side effects.
Dr. Prakash V. Kotecha
50

IFA Syrup Consumption in last 7 days
Dr. Prakash V. Kotecha
51

Deworming Medicine Received by the Children
Dr. Prakash V. Kotecha
52
11.8
2
9.9
1.50
7
14
Gyanpur Handia
Children Mothers
87% children & 73% of mothers consumed the
medicine

Benefits explained by ASHA
Dr. Prakash V. Kotecha
53
“Child becomes weak and pale due to lack of blood in the body. It is advisable to take iron rich diet and other iron preparation
to prevent anemia. Iron increases blood and help fight
infection.”

Complementary Feeding
Dr. Prakash V. Kotecha
54

Hygiene Practices observed
Dr. Prakash V. Kotecha
55

Hemoglobin Study • 31 cluster sampled PPS and then 10 children
from each cluster was planned with expected design effect of 2.
• HemoCue Machine (301) was used for measuring hemoglobin level.
• Children were pricked either at the toe or heel using lancet needle provided by Hemocue
• All precuations were taken for aseptic and antiseptic measures and children were pricked after consent from the parents
Dr. Prakash V. Kotecha
56

Anemia Prevalence Difference13% Reduction of
Anemia2% Reduction of
Anemia
84% Increase in non anemic children

Level of Malnutrition
39.8
34.435.3
33.5
30
35
40
45
Gyanpur Handia
Baseline
Endline
Dr. Prakash V. Kotecha
58

Achievements• Complete Package delivery is feasible to be delivered
within the system
• It is possible to build the capacity of front line workers to deliver IFA syrup and provide counseling within the system
• Through the system, we can reach to children for IFA syrup to young age group that is not part of vaccination. ICDS also usually does not cover this age group at the center.
• IFA to mothers is also attended to and improved when importance is emphasized
• Complementary feeding is discussed
• Deworming medicine to children is being advised.
59
Dr. Prakash V. Kotecha

Dr. Prakash V. Kotecha
60

Challenges
• Coverage for every child remains a challenge• IFA supply and logistics and monitoring• Compliance for IFA syrup• Reduction of anemia to a larger proportion• Deworming medicine• Complimentary food advice and practice• Health Workers themselves are anemia…
61
Dr. Prakash V. Kotecha

Age profile of mothers
Dr. Prakash V. Kotecha
62