Apollo Training Apollo Spacecraft and Systems Familiarization
Upload
truongkienCategory
view
218download
1
Tropical ID (Update) Dr P Senthur Nambi
Consultant – Infectious DiseasesApollo Hospitals, Chennai Region

Tropical Infections
Common & often consideredEg: Typhoid, Malaria, Dengue, Lepto
Common but considered less oftenEg: Scrub typhus
Not so common but not to be ignoredEg: Meliodosis
Uncommon but not to forgetEg: JE, Rabies, Anthrax
Newer onesEg: WNV, CCHF, Zika

Approach to fever
Differentiated fever
• Pneumonia
• Meningoencephalitis
• UTI
• Intraabdominalinfections
Undifferentiated fever
• Enteric fever
• Leptospirosis
• Malaria
• Dengue
• Scrub typhus

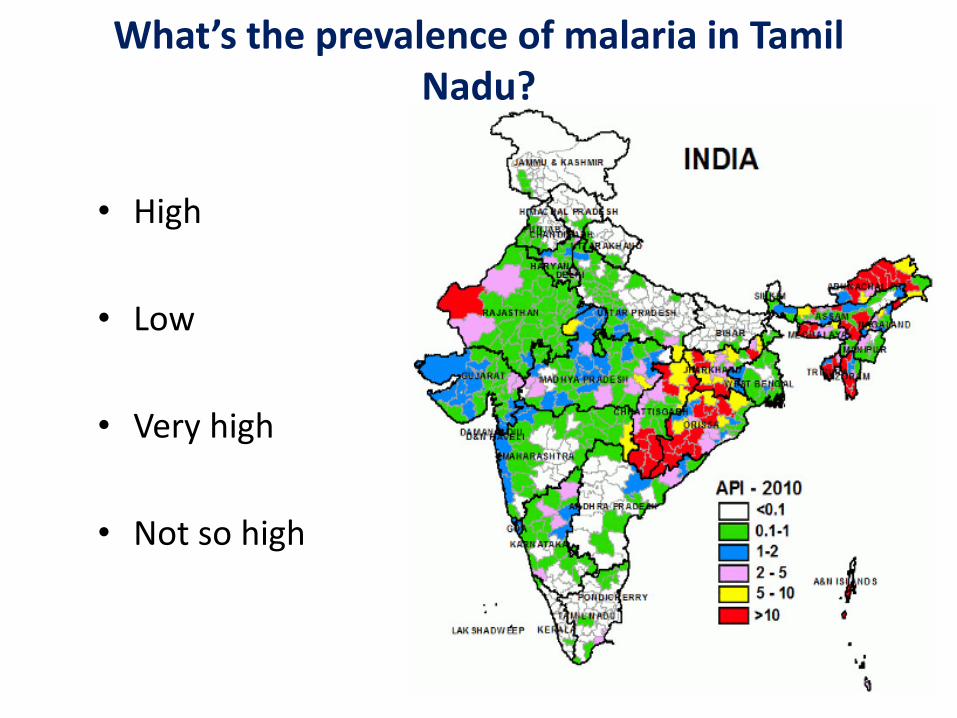
What’s the prevalence of malaria in Tamil Nadu?
• High
• Low
• Very high
• Not so high


How would you diagnose malaria?
1. Clinically
2. Rapid diagnostic test (Card test)
3. Peripheral smear
4. QBC

Blood film examination
• Thick film – 15 times more sensitive than thin film
• Detect parasitemia at a level as low as 50 parasites/microlitre
• Thin film – provides specificity by confirming the plasmodium species
• Monitoring of treatment
• Two or three negative
smears r/o malaria

Detection of malarial antigen(RDT)
HRP-2 detection (molecule present throughout the
erythrocytic cycle)
• First rapid malaria detection test to be developed
• sensitivity – 96%, specificity - >95%
pLDH detection
• Not species specific
• Can detect parasitaemia as low as 0.1% (100 parasites
per microlitre)
• sensitivity – 94%, specificity – 99%


Minimal risk of resistance


National Guidelines on Malaria

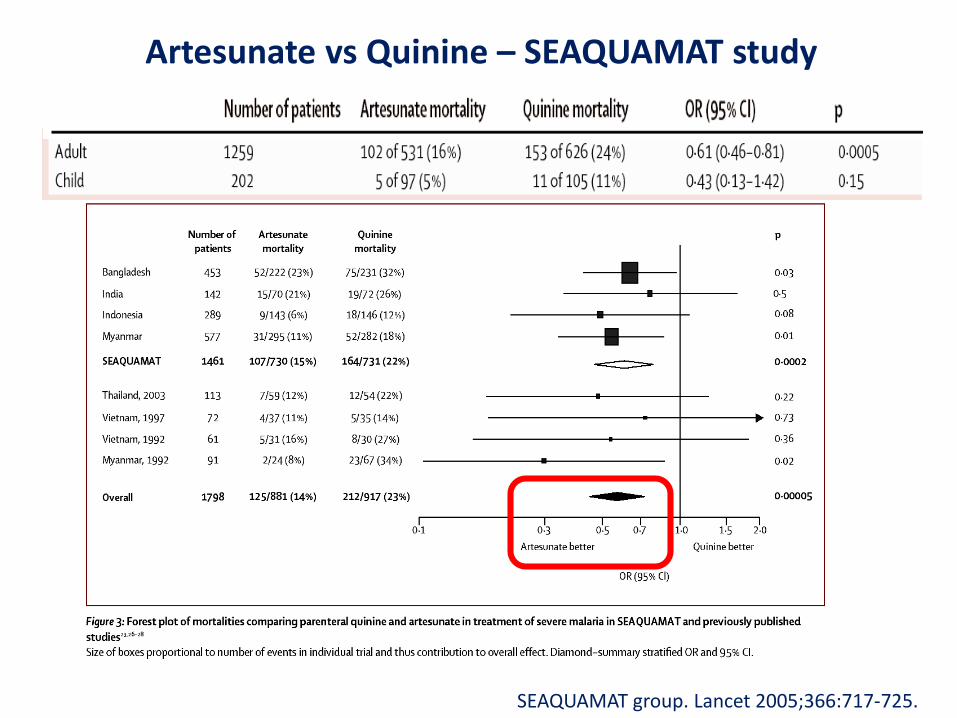
Artesunate vs Quinine – SEAQUAMAT study
SEAQUAMAT group. Lancet 2005;366:717-725.
WHO guidelines for severe falciparum malaria
• Artesunate 2.4 mg/kg IV or IM given on admission (time = 0), then at 12 h and 24 h, then once a day for total 7 days
• Add doxycycline or clindamycin
• Avoid mefloquine if altered sensorium

Severe falciparum malaria
• Parenteral for atleast 24h
• Complete with either
artemether + lumefantrine
artesunate + SP
artesunate + clinda / doxy

Vivax malaria
• Chloroquine 25mg/kg over 3 days
• + Primaquine 0.25mg/kg od x 14d
• ACT with primaquine for chloroquine resistance
• Avoid ACT with SP



P. knowlesi – the fifth malaria species
• Macaques natural host for P. knowlesi, lives in forest areas in South East Asia
• In a study from Malaysia 28% (n=960) malaria patients were confirmed by PCR to be P. knowlesi, mainly misdiagnosed as P. malaria*
• Potentially severe malaria like P. falciparum
• Malaria diagnosed as P. malariaefrom Asia should be suspected to be P. knowlesi and managed as severe malaria
Thin blood slide from one of four patients who
died with the diagnosis ”P. malariae” in Sarawak
in Malaysia; later confirmed by PCR to be P. knowlesi.*Cox-Singh J et. al. Plasmodium knowlesi Malaria in Humans is Widely Distributed and Potentially Life Threatening.CID2008:46

Artesunate resistance

Poor-quality antimalarial drugs in Southeast Asia andsub-Saharan Africa
Lancet Infect Dis 2012,12: 488–96
1437 samples, five classes tested
7 countries in southeast Asia
➢ 497 (35%) failed chemical analysis
➢ 423 (46%) of 919 failed packaging analysis
➢ 450 (36%) of 1260 were falsified


Typhoid worldwide
Widal & Enteric feverSource: WHO Guidelines on typhoid - 2003
• Endemic area (?Cut-off)
• Negative in up to 30% of culture-proven cases
• False Positive – Previous inf, anamnestic, auto-immune diseases, malaria, typhus, bacteremia, cirrhosis, vaccination
• False Negative – Too early, antibiotic use, kit used
• The Widal test can be dangerously misleading and shouldno longer be used in clinical practice (WHO – Good Clinical Diagnostic Practice Guidelines)

When to suspect enteric fever?
• Fever > 72 hrs
• Normal WBC, Eosinopenia
• Normal ESR
• Young individuals, outside food intake


S.Typhi senstivities

Time to defervescence with ceftriaxone+azithromycin3.2 days vs 6.6 days for ceftriaxone

Dengue Incidence
Nature 2013 Apr 25; 496(7446): 504–507507.


Dengue serology

Antigen (NS-1) detection test :
• Glycoprotein produced by all flaviviruses
• Appears as early as Day 1 after the onset of the fever and declines to undetectable levels by 5–6 days
• Can be detected in both patients with primary and secondary dengue infections
• Good sensitivity and specificity, but not yet approved by WHO
• IgM circulates for up tothree months or longer, itspresence might not bediagnostic of a currentillness
• To diagnose a currentdengue infection, thedemonstration of aseroconversion (four foldor greater changes inantibody titres) in pairedsera is required
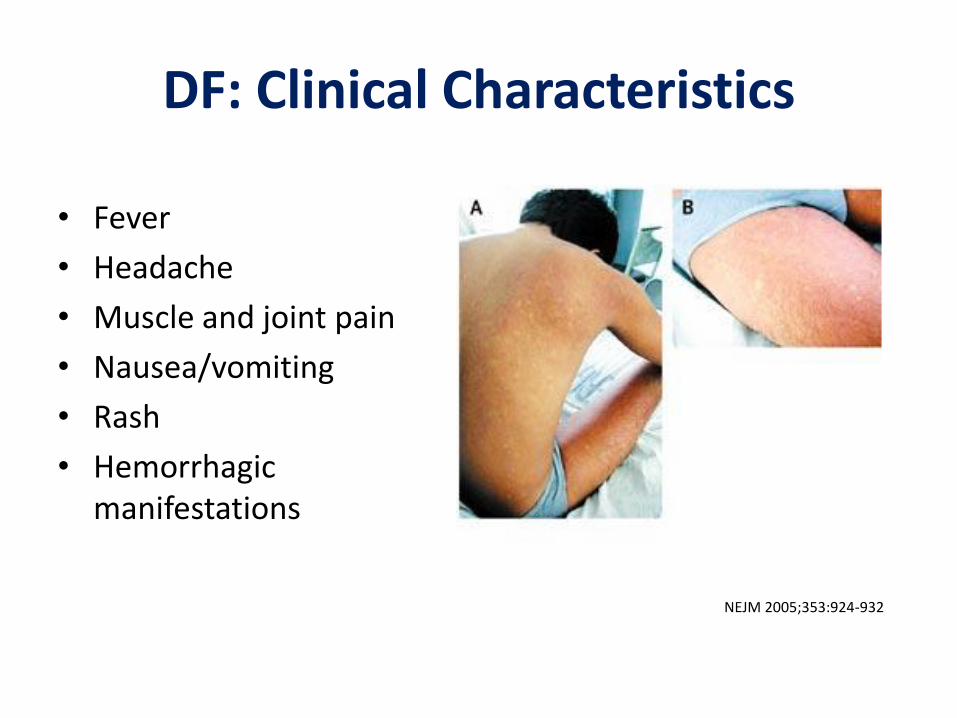
DF: Clinical Characteristics
• Fever
• Headache
• Muscle and joint pain
• Nausea/vomiting
• Rash
• Hemorrhagic manifestations
NEJM 2005;353:924-932



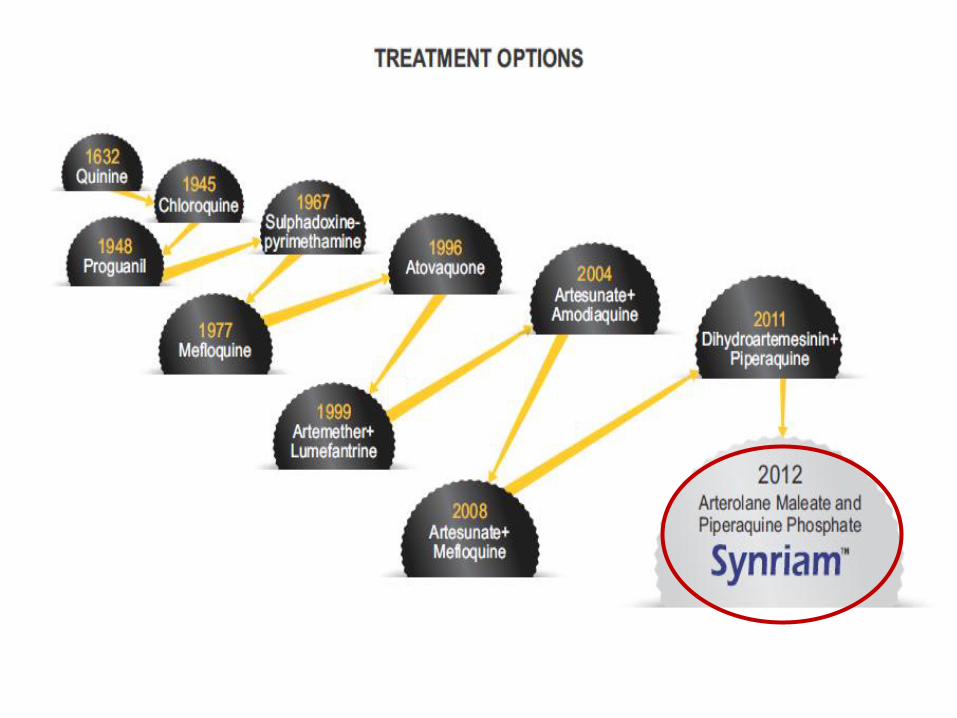
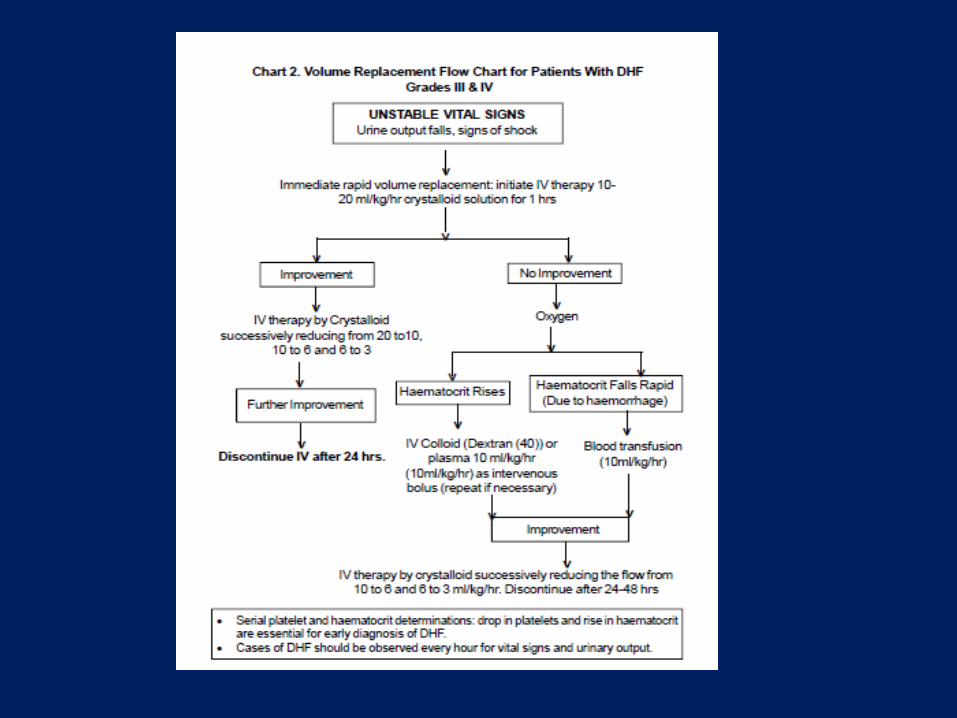
Treatment
• No specific antiviral drug available
• Avoid aspirin, NSAID
• Prompt fluid replacement– 0.9% NS as effective as colloids for initial resuscitation
• Blood transfusion only with overt bleeding
• Avoid IM injections
NEJM 2005;353:877-889

• Dengue - Who needs admission ?
- Presence of Shock
- Dangerously low platelets
- Progressive disease & warning signs
- High risk patients esp children and comorbidities
- Indication of platelets transfusion ?
- if < 10,000
- if any overt bleeding

Are prophylactic platelet transfusionsnecessary?
• Doesnt shorten period of thrombocytopenia
• Bleeding risk not correlated with platelet count
• Limited data on effectiveness of platelet transfusions to prevent bleeding complications
• May lead to fluid overload & prolonged hospitalization
Chuansumrit et al. Transfusion requirements in patients with DHF. SE Asian J Trop Med Public Health, 2000, 3:10-14.
Lye et al. Lack of efficacy of prophylactic platelets for severe thrombocytopenia in adult with dengue. CID, 2009, 48:1262-1265.
Chairulfatah et al. Thrombocytopenia and platelet transfusions in DHF and DSS. Dengue Bulletin, 2003, 27:138-143.
What is an effective way to prevent bleeding?
• Prevent prolonged shock – recognize and treat it EARLY
• Avoid trauma (provokes bleeding) – CVP insertion by experienced persons

• Insufficient evidence to use corticosteroids
• Corticosteroids can potentially do harm
• Clinicians should not use them

Discharge criteria - Dengue
• Absence of fever for at least 24 hours without the use of anti-fever therapy
• Return of appetite
• Visible clinical improvement
• Good urine output
• Minimum of 2/3 days after recovery from shock
• No respiratory distress from pleural effusion or ascites
• Platelet count > 50,000/ cumm

Dengue vaccine!
• CYD-TDV (Dengvaxia®) registered in several countries for use in people 9-45 years of age
• Live attenuated (recombinant) tetravalent vaccine
• Other 2 most advanced candidates are also tetravalent live attenuated (recombinant) vaccines & are currently under evaluation in Phase 3 trials
Lancet 2014, NEJM 2014

Leptospira under the Microscope
Long, Thin, Highly Coiled
Dark Field Microscopy FL


Clinical Illnesses
Types Anicteric (common 95% recover)
Icteric ( Weil’s Syndrome) (rare, fatal)
Hepato-renal syndrome
Hemorrhagic syndrome with ARF
Atypical pneumonia syndrome
Aseptic meningo-encephalitis
Myocarditis, Chronic uveitis

Diagnosis
✓Dark field microscopy
sensitivity 40 %, specificity 60%
✓ Culture
EMJH medium
Availability?
✓MAT
✓ IgM antibodies✓ ELISA
✓Detectable after 5th day

Microscopic agglutination test (MAT) - Lepto
• Sensitivity within the first 15 days only 17%
• Persists longer (5 to 10 yrs)
• Technically challenging
• Requires demonstration of seroconversion or a ≥4-fold MAT titer increase between paired acute & convalescent phase specimens
• WHO recently defined MAT titer of ≥1:400 in a single serum specimen as significant
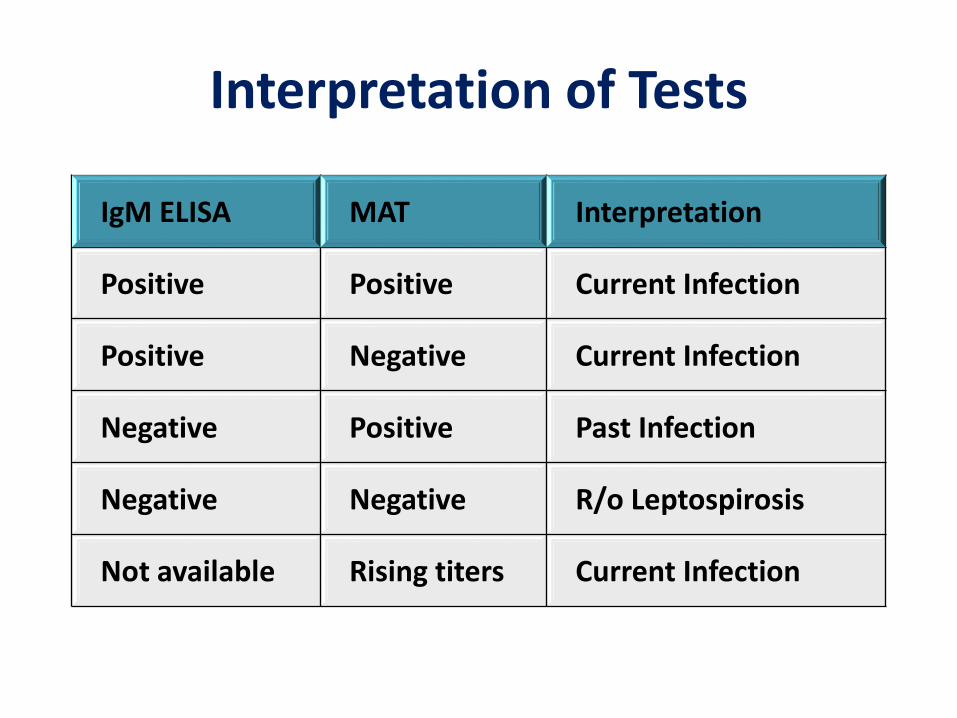
Interpretation of Tests
IgM ELISA MAT Interpretation
Positive Positive Current Infection
Positive Negative Current Infection
Negative Positive Past Infection
Negative Negative R/o Leptospirosis
Not available Rising titers Current Infection

Panaput T, et al. CID 2003;36:1507-13.

Leptospirosis – Treatment
Mild
✓ Doxy 100mg BD
✓ Ampicillin 500-750 mg q6h; Amox 500 mg q 6h
✓ Azithromycin 500mg OD
Moderate to severe
✓ Penicillin G 1.5 million units IV q6h
✓ Ceftriaxone 1 gm IV q 24h (as good as CP)
✓ Ampicillin 0.5-1gm IV q 6h
Watt G et al. Lancet 1988; 1(8583):433–5; ; Supputamongkol Y et al. Clin Infect Dis. 2004;39:1417–1424; Panaphut T et al. Clin Infect Dis 2003; 36:1507–13
Scrub typhus
✓ Causative agent – O. tsutsugamushi
✓ Transmitted by larval mites

Scrub typhus endemic areas
Diagnosis
➢ IgM ELISA
✓ IFA, Immunoperoxidase test
✓ PCR
✓ Weil-Felix
Treatment
➢doxycycline
✓azithromycin, chloramphenicol, rifampicin

Typhus - pointers
• Scrub typhus is a re emerging infection
• Look carefully for an eschar
• Typical clinical situations:– Leukocytosis with thrombocytopenia
– Cholestatic hepatitis with fever
– Acute or subacute meningitis
– Atypical pneumonia
– Sepsis syndrome with multi-organ involvement
• Specific serology available
• Start doxycycline as soon as diagnosis considered

Spotted fevers – Tick borne (Ixodid and others)
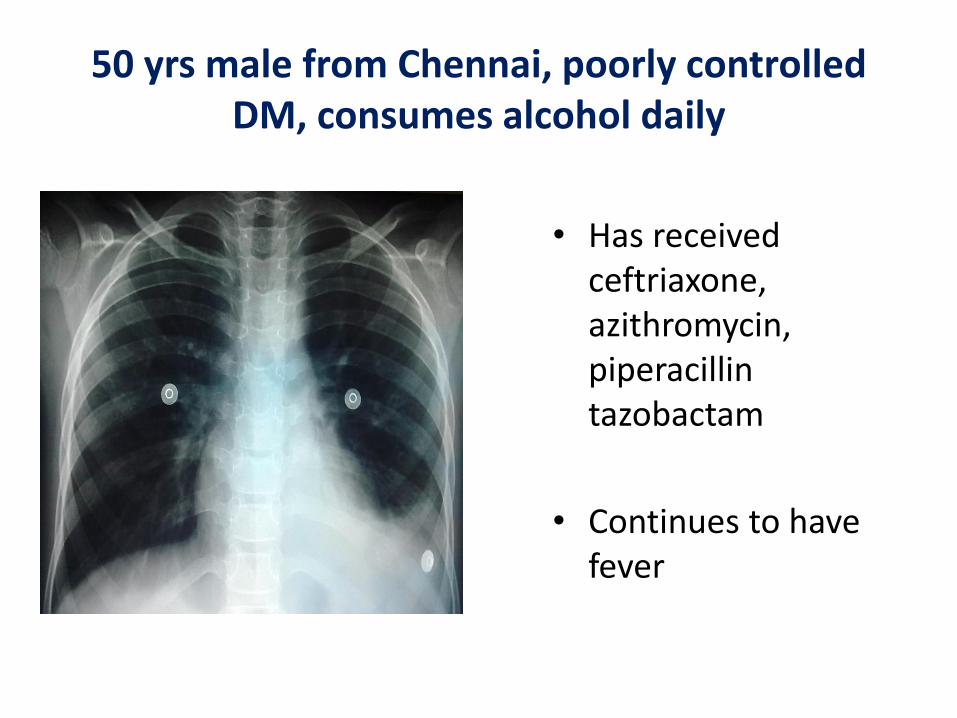
50 yrs male from Chennai, poorly controlled DM, consumes alcohol daily
• Has received ceftriaxone, azithromycin, piperacillintazobactam
• Continues to have fever

Blood cultures (2 sets) grewNon fermenting gram negative bacilli
Sensitive
CotrimoxazoleCefotaximeCef-sulbactamCeftazidimeImipenemMeropenem
Resistant
CefuroximeGentamycinCipro
Amikacin

Distribution of Melioidosis

Melioidosis
• Spread by inhalation, percutaneousinoculation
• Risk factors:
➢ Diabetes
➢ Alcohol consumption
➢ Chronic renal failure
➢ Chronic lung disease
• Acute (88%) & chronic presentation (12%)
• Septicemic/localized
• Pneumonia, skin abscesses, genitourinary, arthritis or osteomyelitis

Melioidosis - Treatment
Intensive therapy (2 weeks)
✓ Ceftazidime
✓Meropenem
✓ Imipenem
With or without cotrimoxazole
Eradication therapy (3-6 months)
✓ Cotrimoxazole plus
✓Doxy

Zika..

Zika & India

Zika - Symptoms
▪ Flavivirus; Vector – Aedes; Incubation period: 2 -12 days
▪ Symptomatic in 20 – 25%
▪ Low-grade fever (37.8 to 38.5°C)
▪ Maculopapular rash
▪ Arthralgia (notably the small joints of hands and feet)
▪ Conjunctivitis (nonpurulent)
▪ Other clinical manifestations include myalgia, headache, retro orbital pain & asthenia



Zika & Pregnancy
• No evidence to suggest that pregnant women are more susceptible or experience more severe disease
• Greatest risk of microcephaly & malformations appears to be associated during the first trimester
• Rate of vertical transmission & the rate with which infected fetuses manifest complications are unknown
• No developmental complications have been observed in otherwise healthy infants with postnatal Zika virus infection

Diagnosis
• Reverse-transcription polymerase chain reaction (RT-PCR) – In the first 7 days of the illness
• Zika virus IgM and neutralizing antibody titers that are ≥4-fold higher than dengue virus neutralizing antibody titers in serum
• Testing is considered inconclusive if Zika virus neutralizing antibody titers are <4-fold higher than dengue virus neutralizing antibody titers


Global air travel map