Clinical diagnostic biochemistry - 12 Dr. Maha Al-Sedik 2015 CLS 334.
Upload
aubrey-wadeCategory
view
224download
2
Diseases of the Eyes, Ears, Nose, and Throat - 4
Dr. Maha Al-Sedik
THE NOSE
Objectives:
Anatomy, physiology of the nose.
Patient Assessment.
Pathophysiology of the nose.
Susceptible to injury because of prominence
Allergens, particles, and chemicals can cause
inflammation, infection, and injury.
Inside of the nose is extremely vascular.
Excellent route for some medicines.

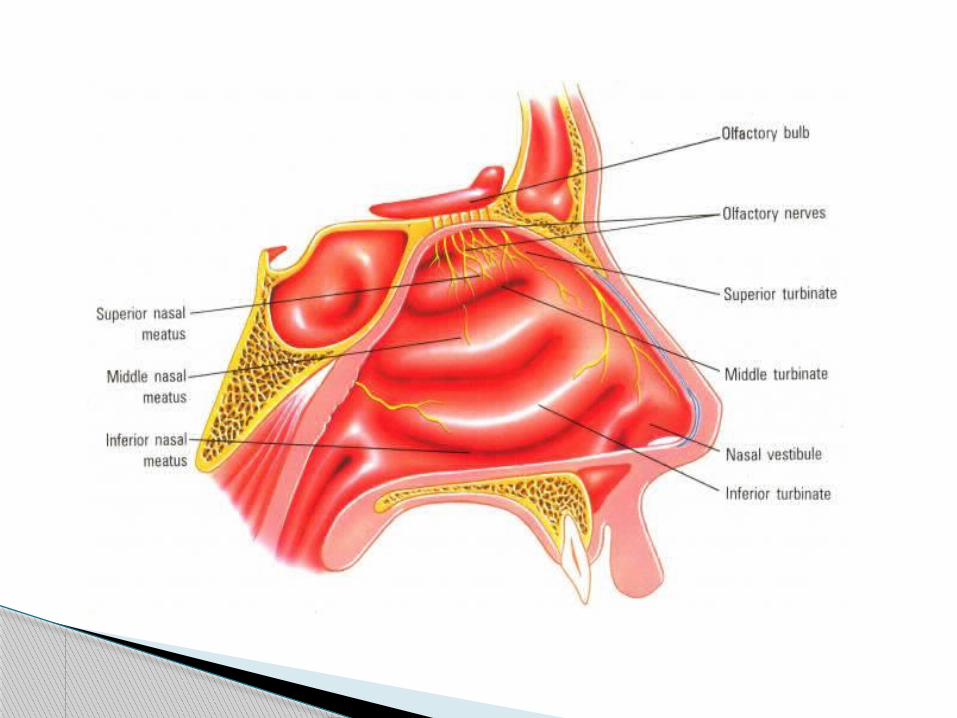
Smelling disorders include:
Anosmia: total loss of sense of smell.
Dysosmia: distorted sense of smell.
Hyperosmia: increased sensitivity to smell.

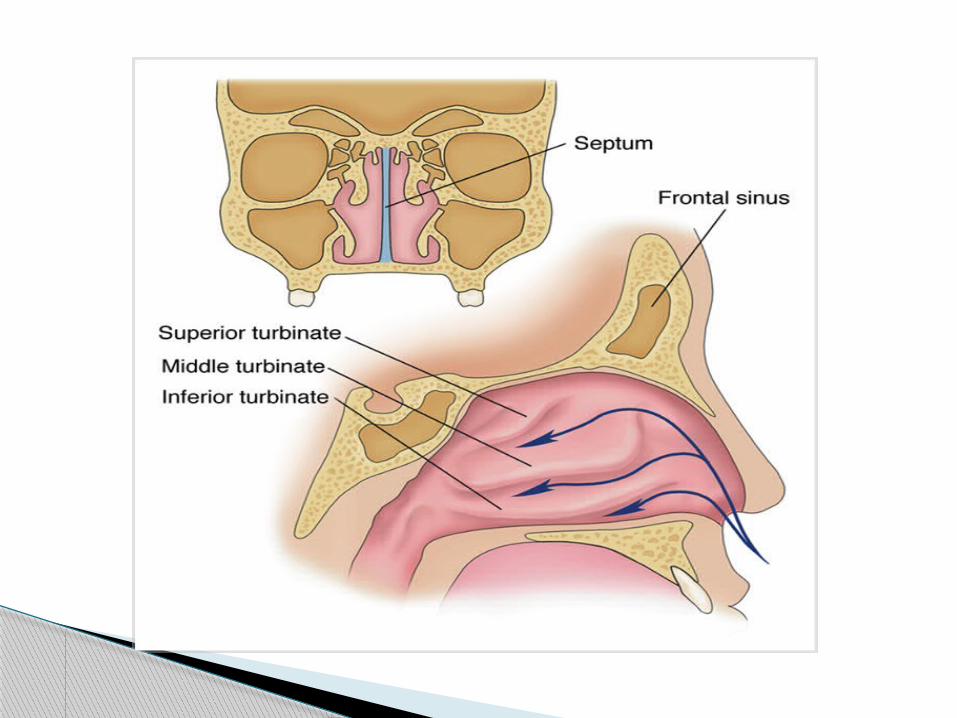
Anatomy and Physiology of the Nose
One of two primary entry points for oxygen
Nasal septum: separation between the nostrils
Turbinate: 3 layers of bone within each nasal
chamber
Patient Assessment
Look for environmental clues.
Ensure scene safety.
Assess airway and breathing.
Determine level of distress.
Do not insert a nasopharyngeal airway or attempt
naso - tracheal intubation with:
o Suspected nasal fractures.
o CSF or blood leakage from the nose.
Inquire about history of nose conditions.
Pathophysiology of the nose
Epistaxis
Nose bleed
Anterior
Posterior
Anterior
Bleed fairly slowly.
Self-limiting and resolve quickly.
Posterior
More severe.
Often cause blood to drain into the throat,
causing nausea and vomiting.
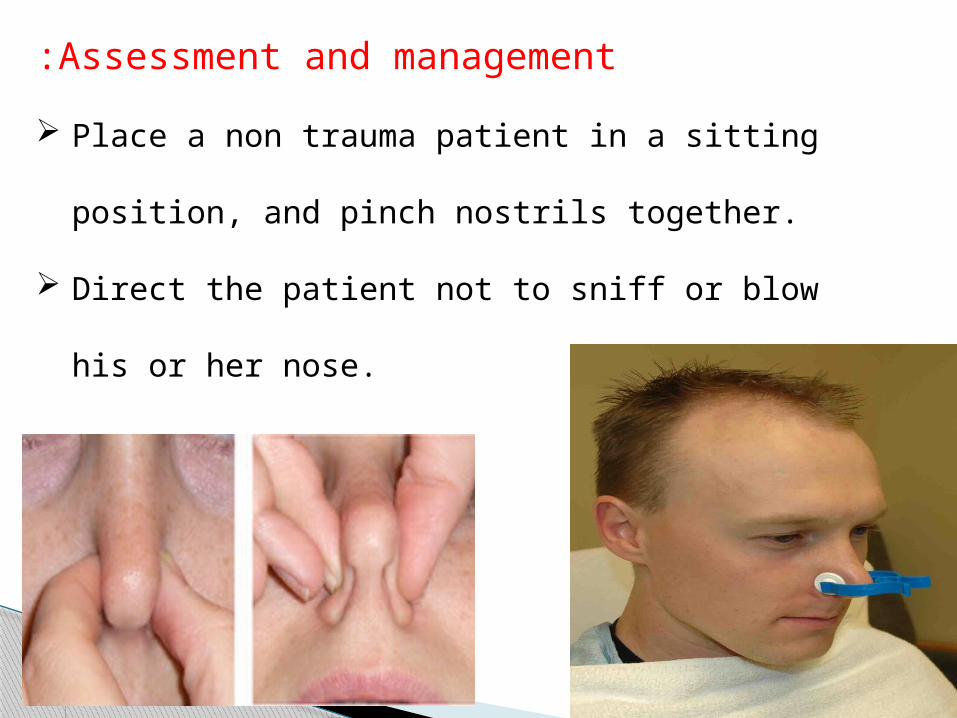
Assessment and management:
Place a non trauma patient in a sitting position,
and pinch nostrils together.
Direct the patient not to sniff or blow his or her
nose.
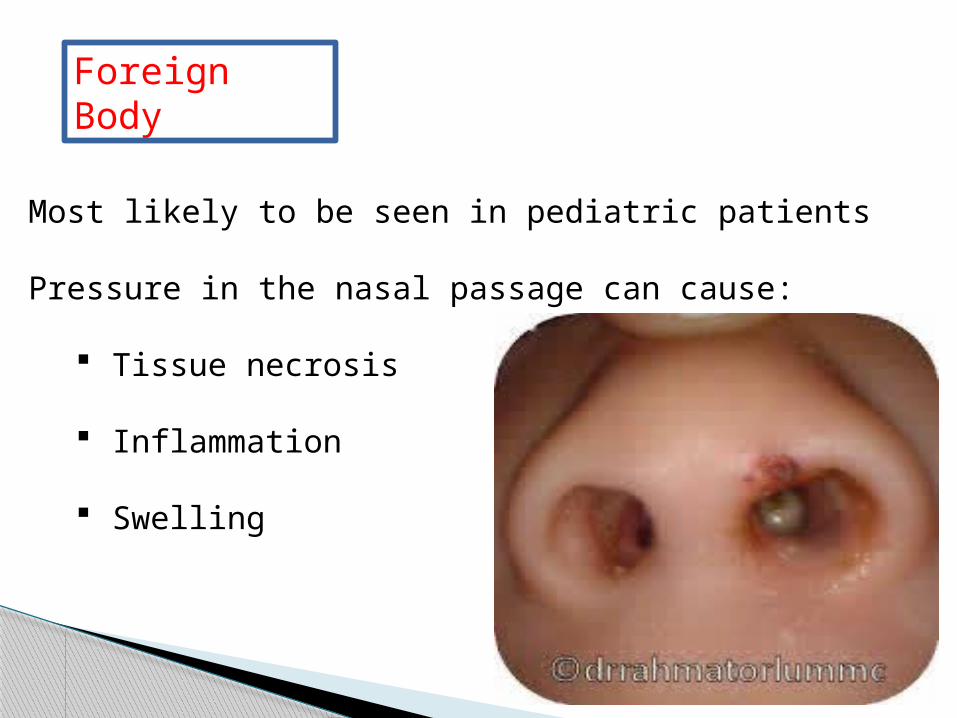
Foreign Body
Most likely to be seen in pediatric patients
Pressure in the nasal passage can cause:
Tissue necrosis
Inflammation
Swelling
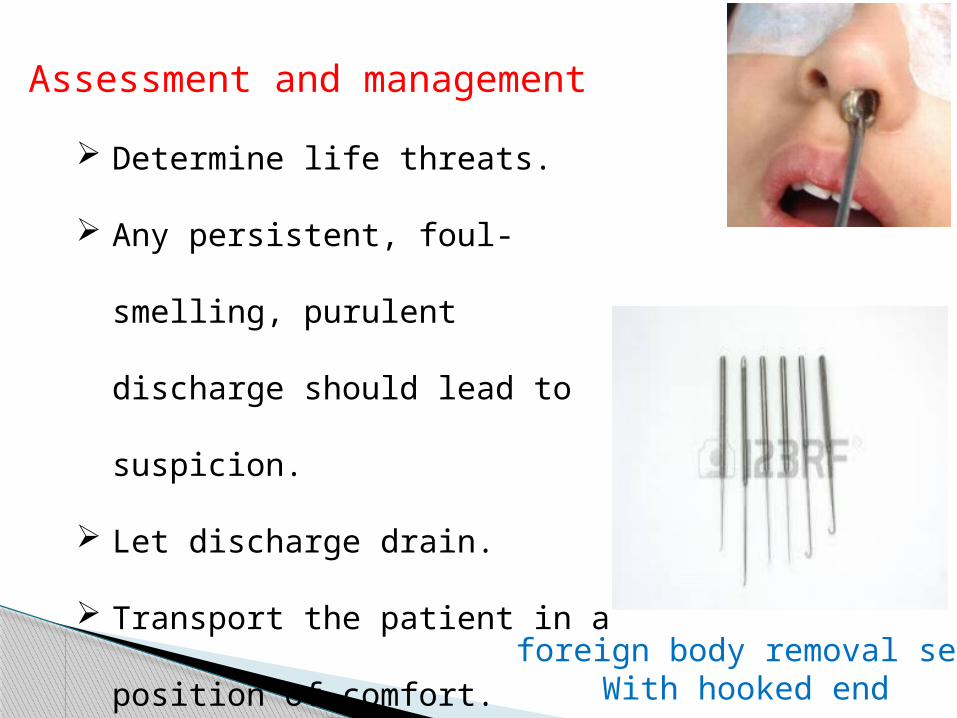
Assessment and management
Determine life threats.
Any persistent, foul-smelling,
purulent discharge should lead
to suspicion.
Let discharge drain.
Transport the patient in a
position of comfort. foreign body removal set
With hooked end
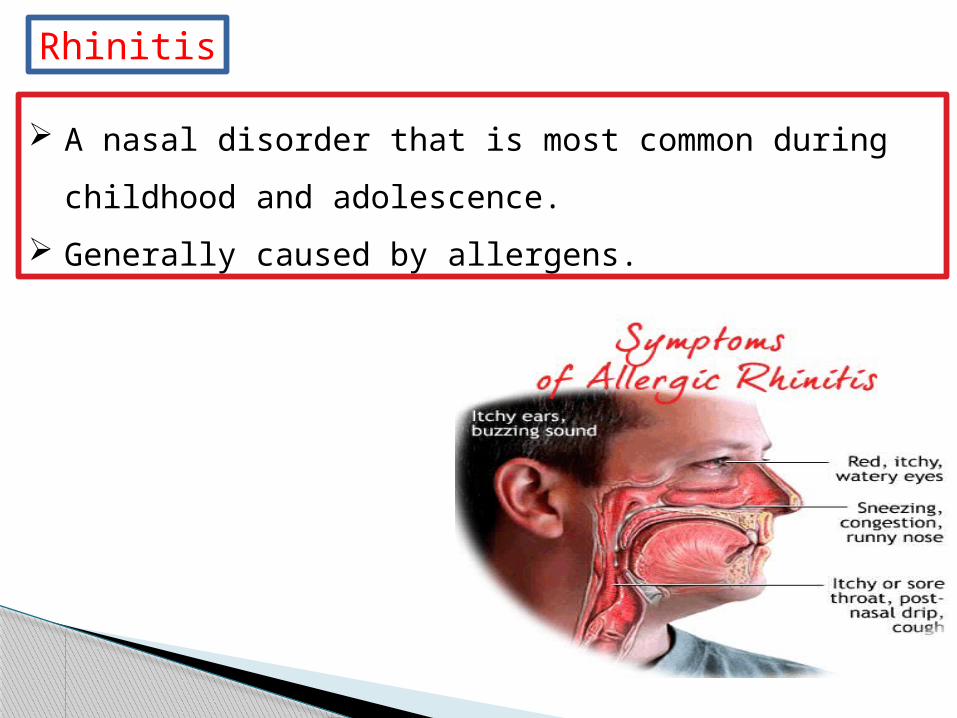
Rhinitis
A nasal disorder that is most common during
childhood and adolescence.
Generally caused by allergens.
Assessment and treatment:
Signs and symptoms may include:
• Nasal congestion.
• Itchy runny nose and eyes.
Keep the patient in the Fowler position.

THE THROAT
Objectives:
Anatomy, physiology of the pharynx and larynx.
Patient Assessment.
Pathophysiology of the pharynx and larynx.
1- The Pharynx (throat):
Funnel-shaped tube of skeletal muscle that connects
to the:
• Nasal cavity and mouth superiorly.
• Larynx and esophagus inferiorly.
Extends from the base of the skull to the level of the
sixth cervical vertebra.
Anatomy and Physiology of the throat
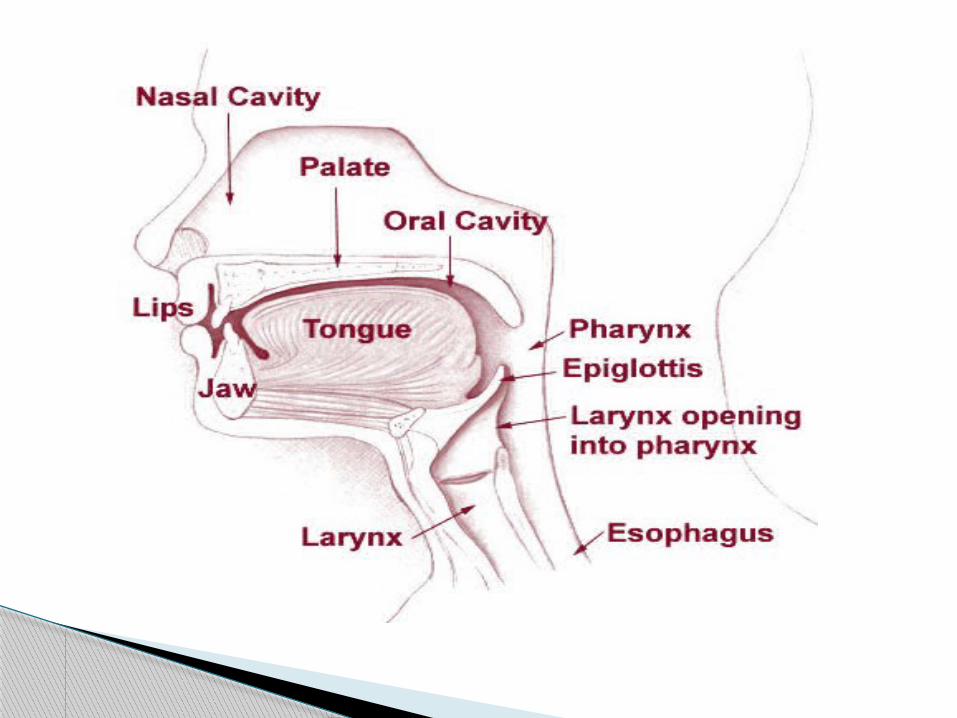
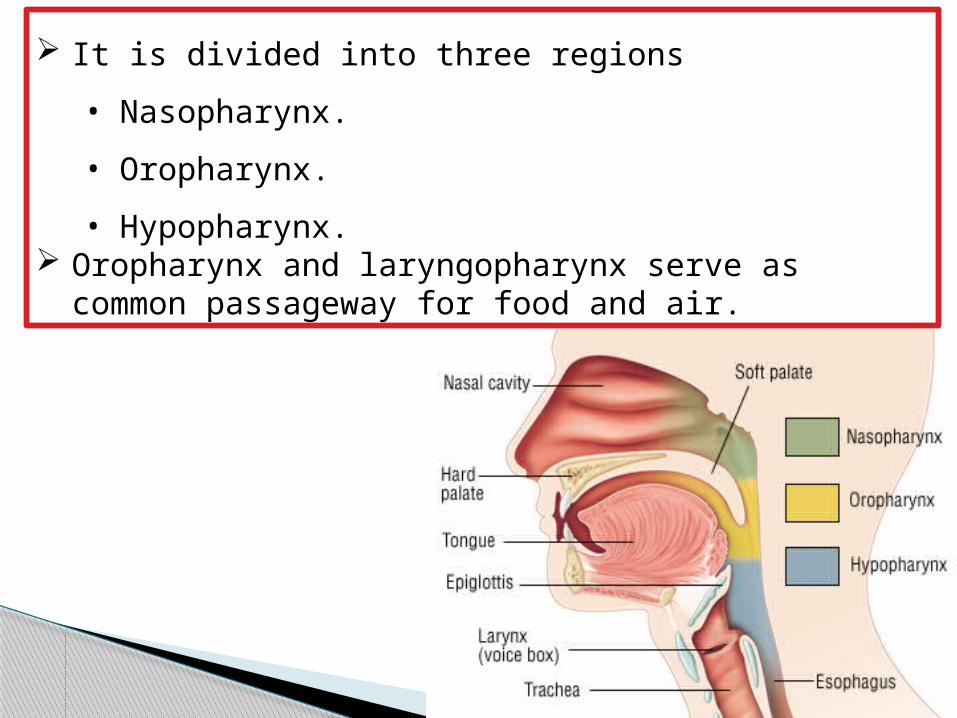
It is divided into three regions
• Nasopharynx.
• Oropharynx.
• Hypopharynx. Oropharynx and laryngopharynx serve as common
passageway for food and air.
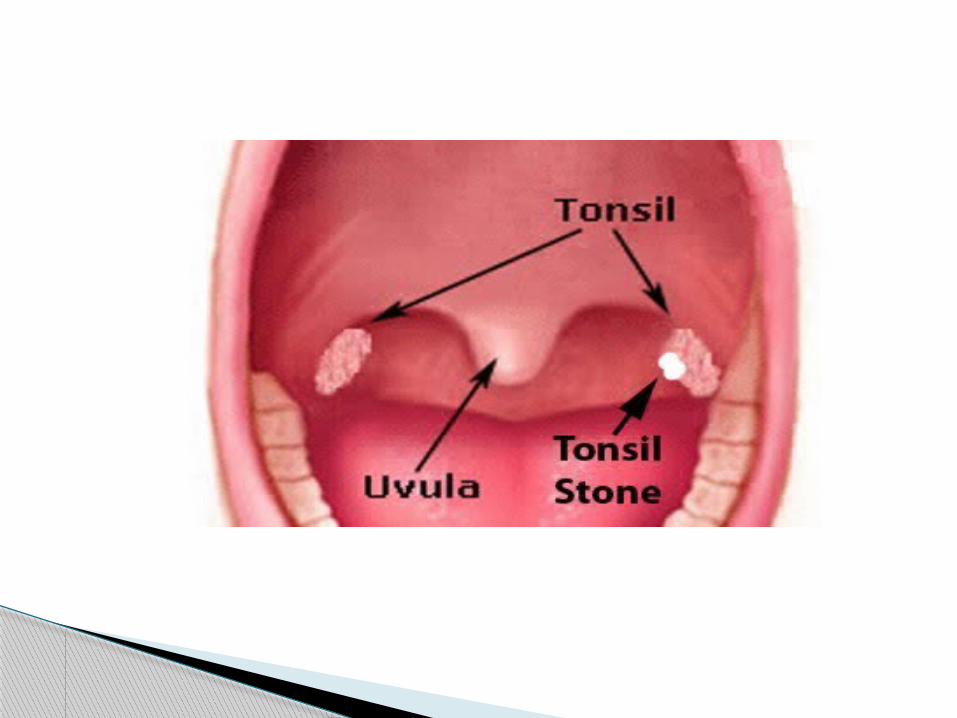
Hypopharynx :
Where the oropharynx and nasopharynx meet
Gag reflex is profound.
• Triggering may cause vagal bradycardia,
vomiting, and increased intracranial pressure.
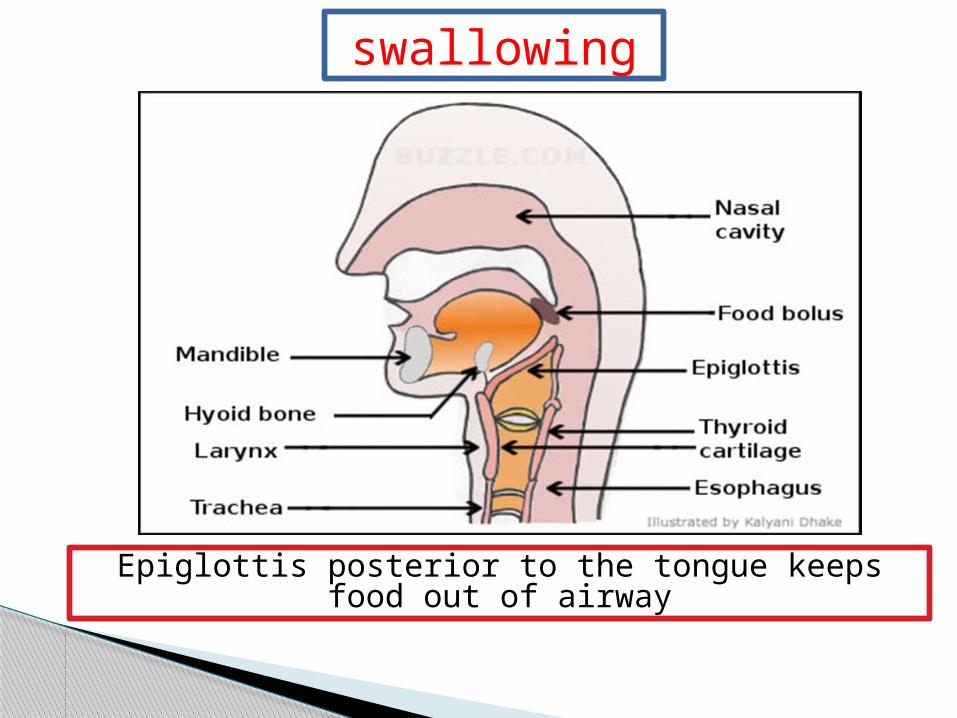
swallowing
Epiglottis posterior to the tongue keeps food out of airway
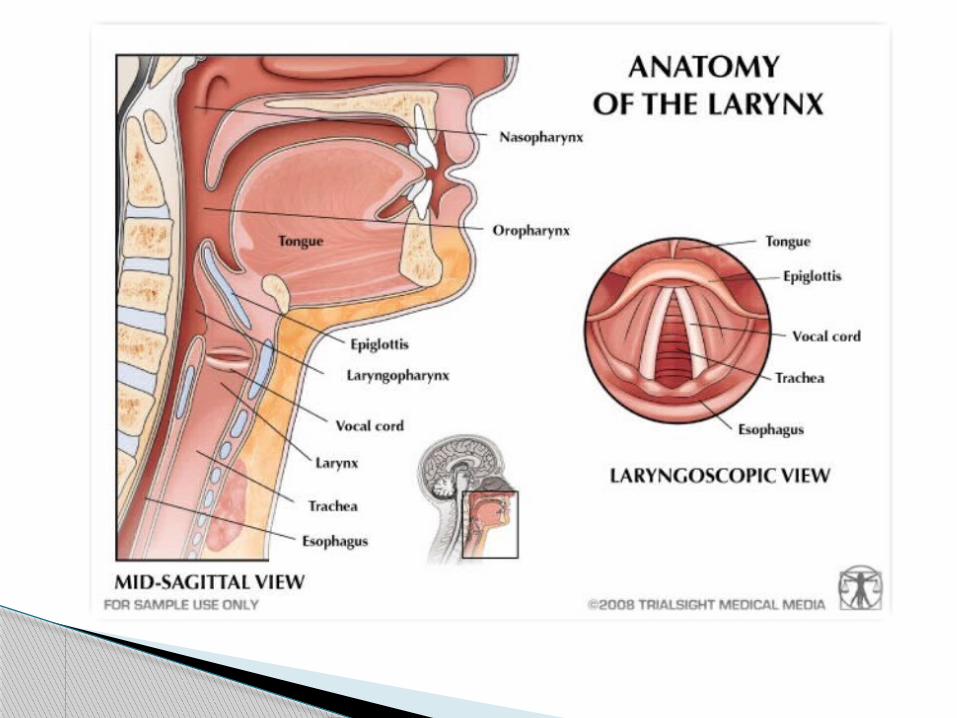
2- Larynx (Voice Box):
It opens into the laryngopharynx superiorly and
continuous with the trachea.
The three functions of the larynx are:
• To provide a patent airway
• To act as a switching mechanism:
Closed during swallowing
Open during breathing
• To function in voice production.
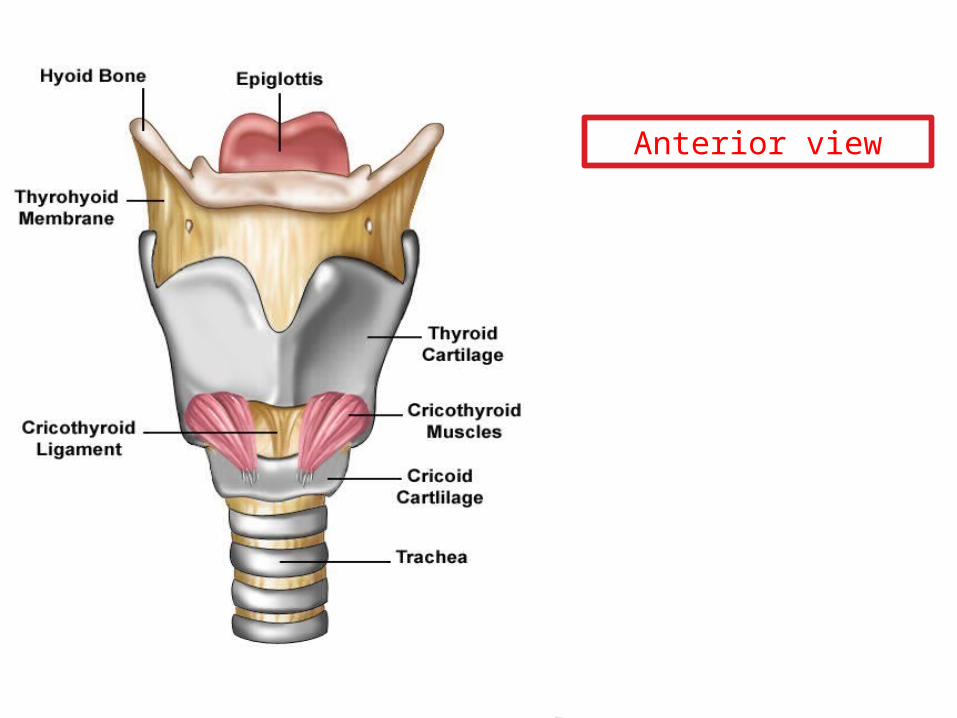
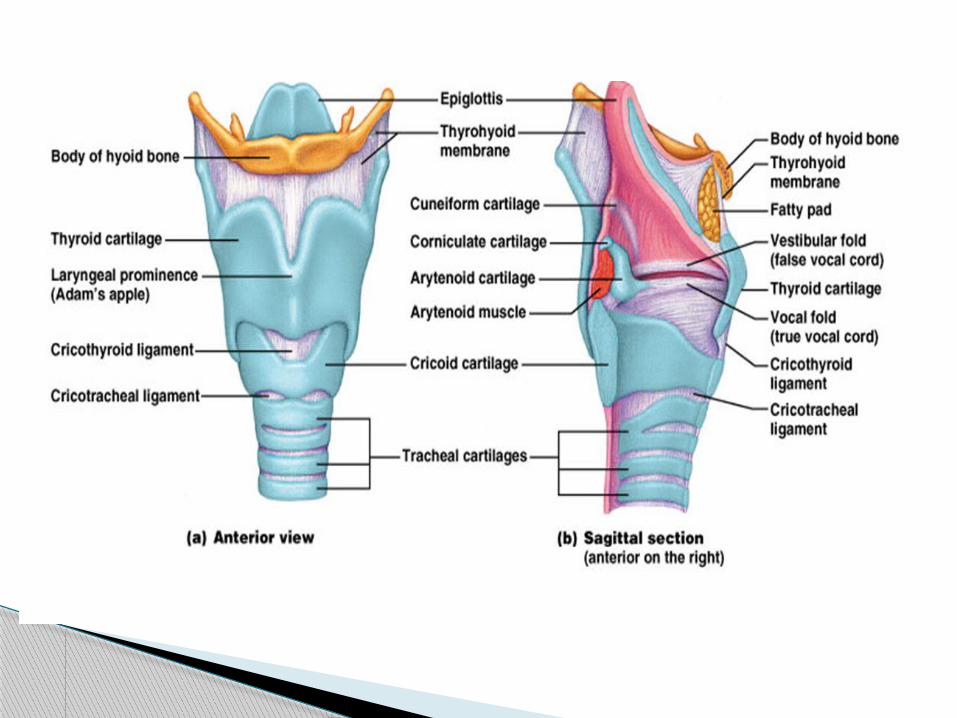
Anterior view
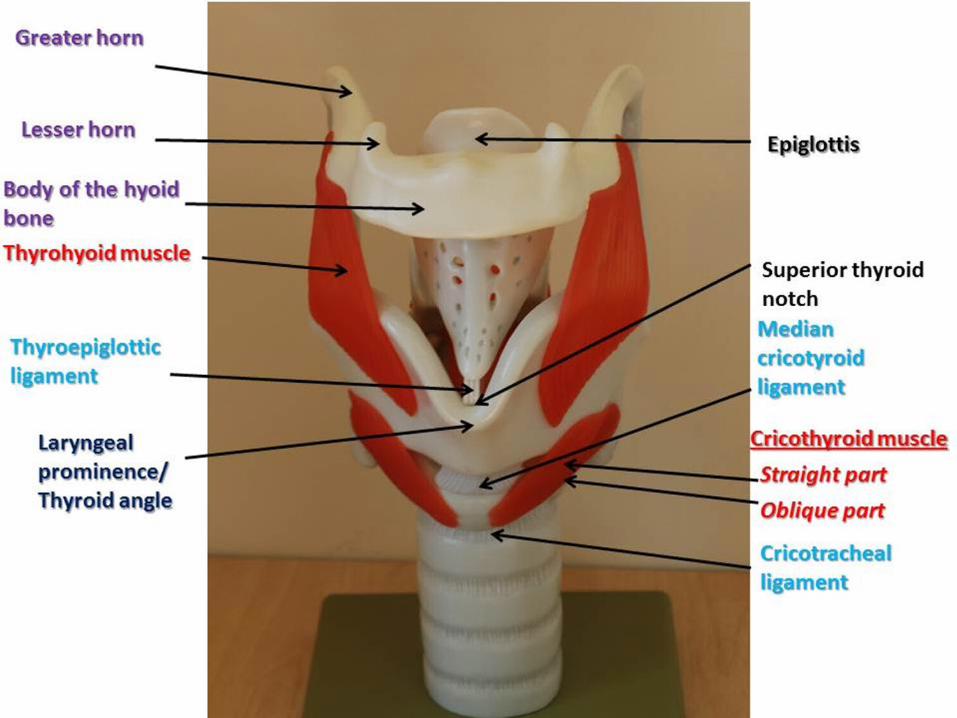
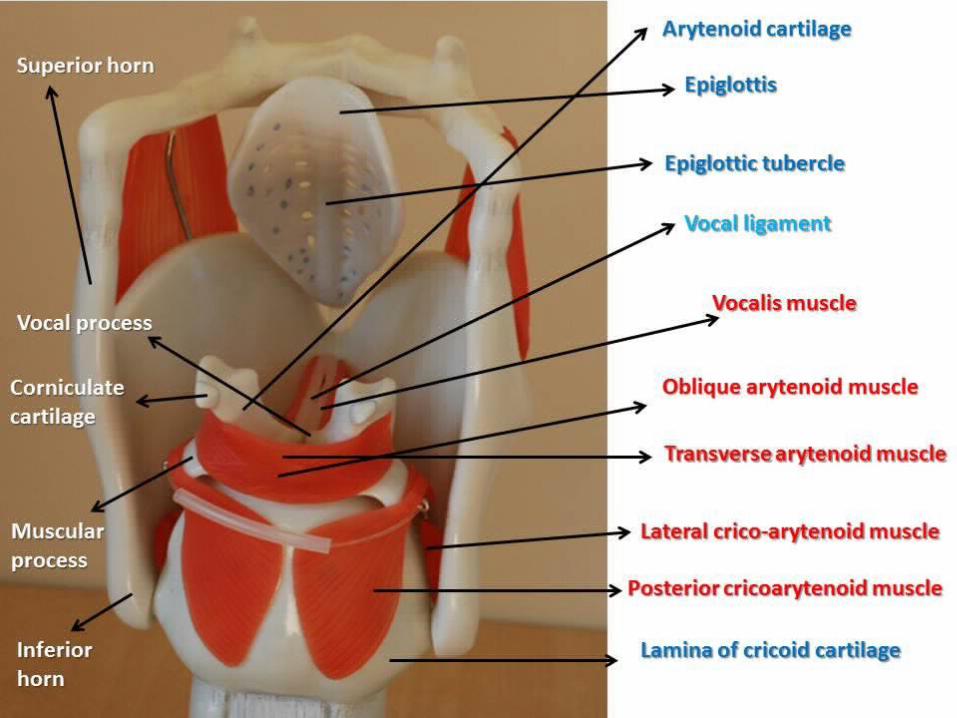
Framework of the larynx:
It is composed of 9 cartilages connected by
membranes and ligaments
Thyroid cartilage: with laryngeal prominence
( Adam’s apple ) anteriorly.
Cricoid cartilage: inferior to thyroid cartilage: the
only complete ring of cartilage: signet shaped and
wide posteriorly.
Behind thyroid cartilage and above cricoid: 3
pairs of small cartilages.
1. Arytenoid: anchor the vocal cords.
2. Corniculate.
3. Cuneiform.
9th cartilage: epiglottis.
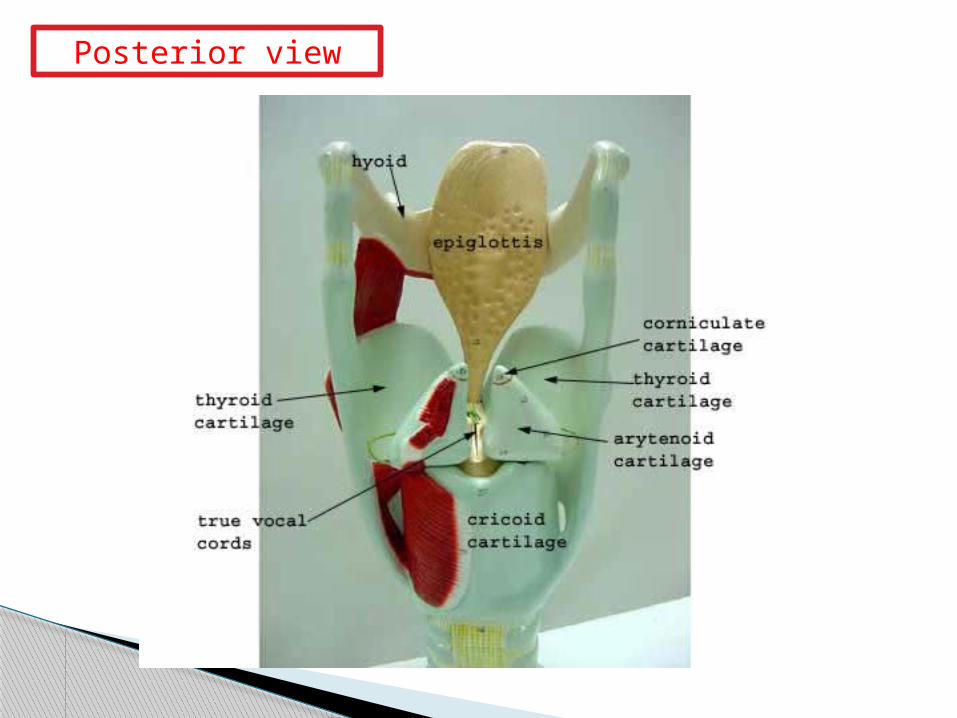
Posterior view
Vocal Ligaments:
Attach the arytenoid cartilages to the thyroid
cartilage.
Composed of elastic fibers that form mucosal folds
called true vocal cords.
The medial opening between them is the glottis.
They vibrate to produce sound as expired air rushes
up from the lungs.
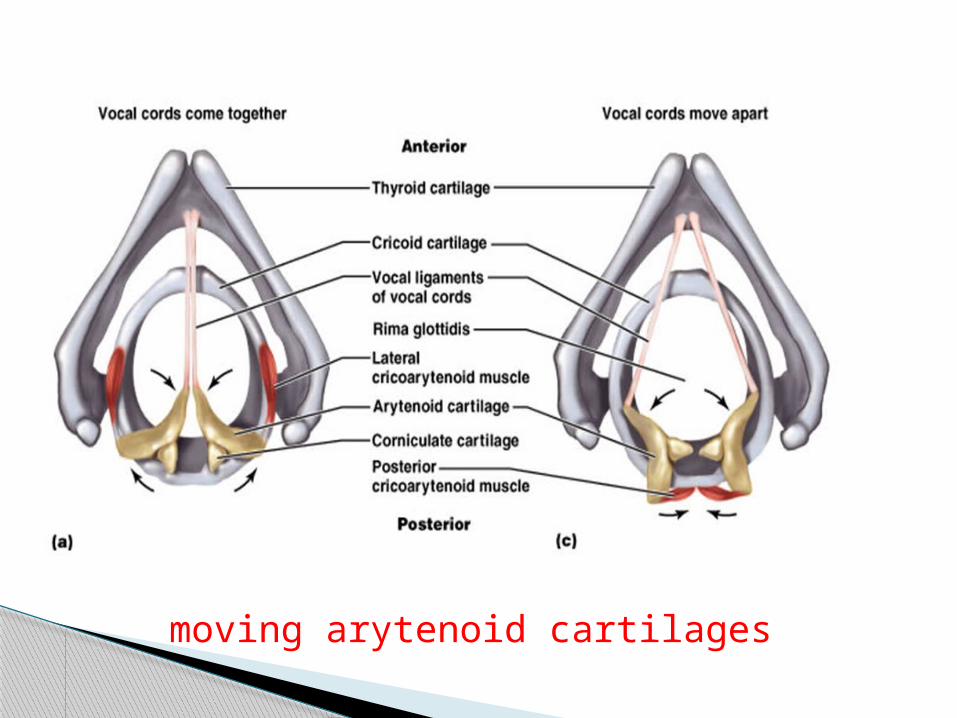
moving arytenoid cartilages
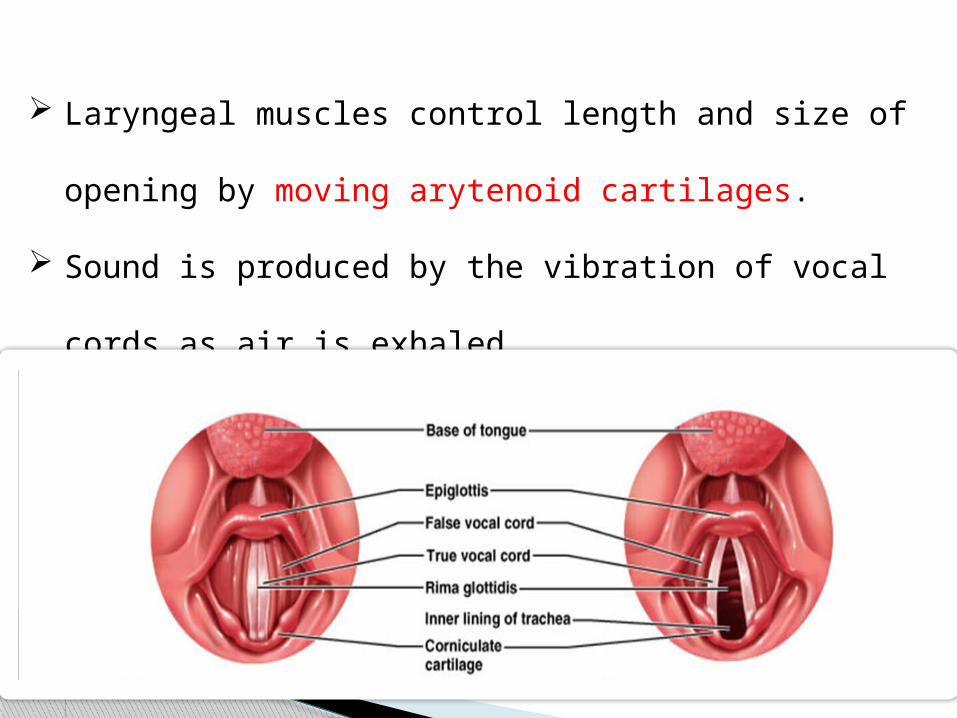
Laryngeal muscles control length and size of
opening by moving arytenoid cartilages.
Sound is produced by the vibration of vocal cords as
air is exhaled.
Neck contains
important structures:
• Thyroid and cricoid cartilage
• Trachea• Thoracic duct• Esophagus• Thyroid and parathyroid
glands• Lower cranial nerves
Pathophysiology of the throat
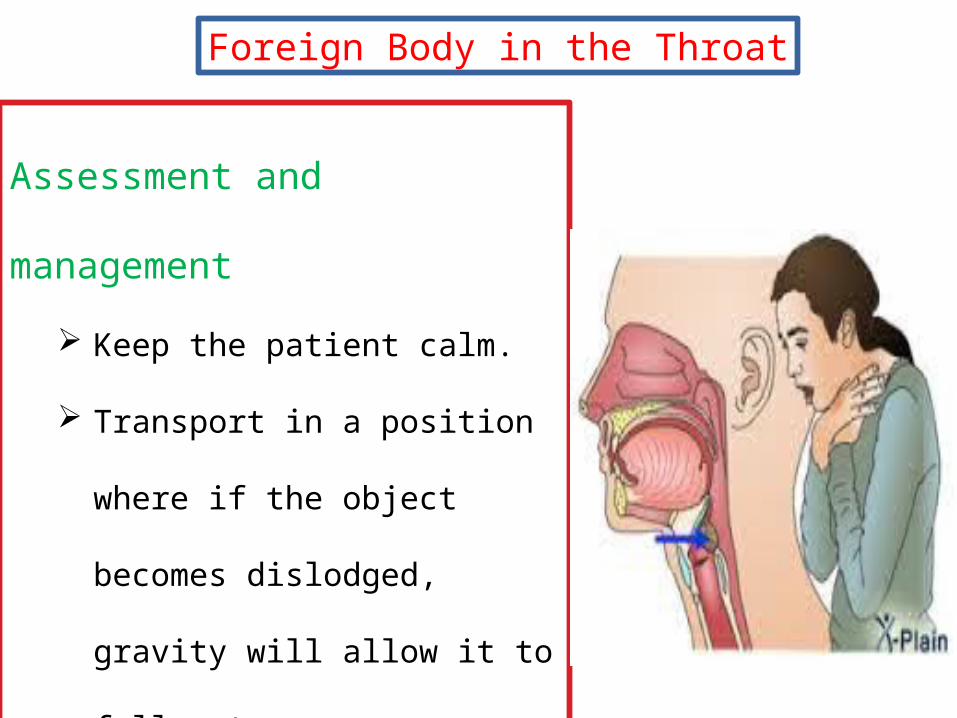
Foreign Body in the Throat
Assessment and
management
Keep the patient calm.
Transport in a position where
if the object becomes
dislodged, gravity will allow
it to fall out.
Managing an airway obstruction is a priority.
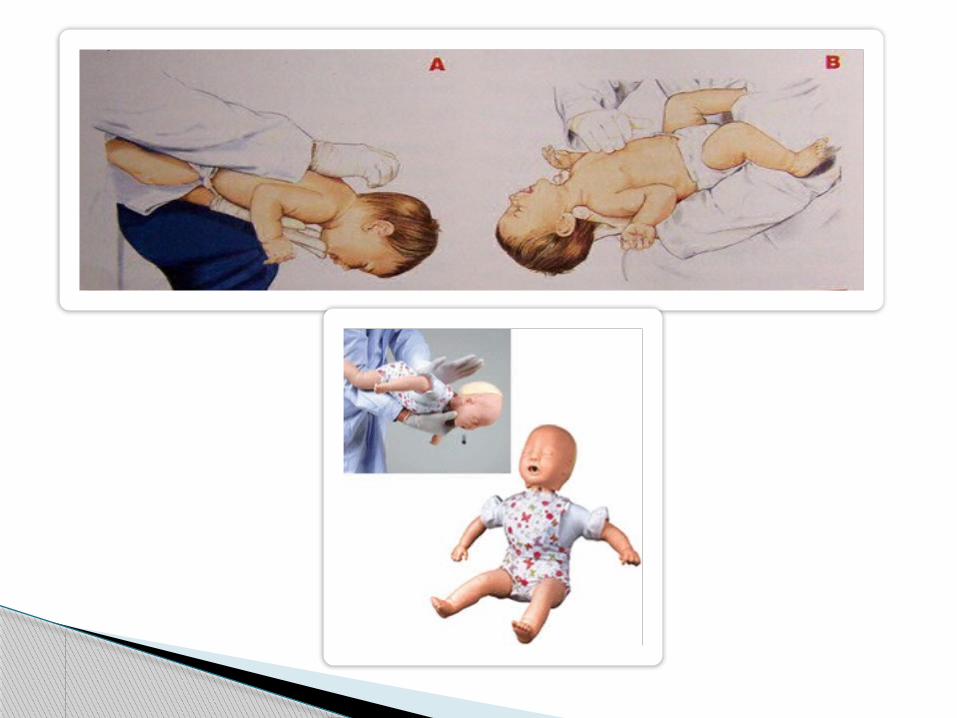
Use age appropriate basic life support foreign body
airway obstruction maneuvers to clear the airway.
Administer supplemental oxygen, and transport the
patient to the closest hospital.
Management:
First Aid treatment
There are three steps that you should follow for adults
and children over 1:
1. Encourage the victim to cough:
Always ask the person if he/she can cough and if so
encourage it
2. Back slaps:
Deliver 5 hard backslaps with the heel of the hand
between the shoulder blades.
After each slap check if the object has been dislodged.
3. Abdominal thrusts or better known as Heimlich
Maneuver
The Heimlich Maneuver is most likely one of best known
First Aid techniques.
You are trying to push the foreign object back out of the
trachea / wind pipe by exerting pressure on the bottom
of the diaphragm. This compresses the lungs and exerts
pressure on any object lodged in the trachea, hopefully
expelling it.
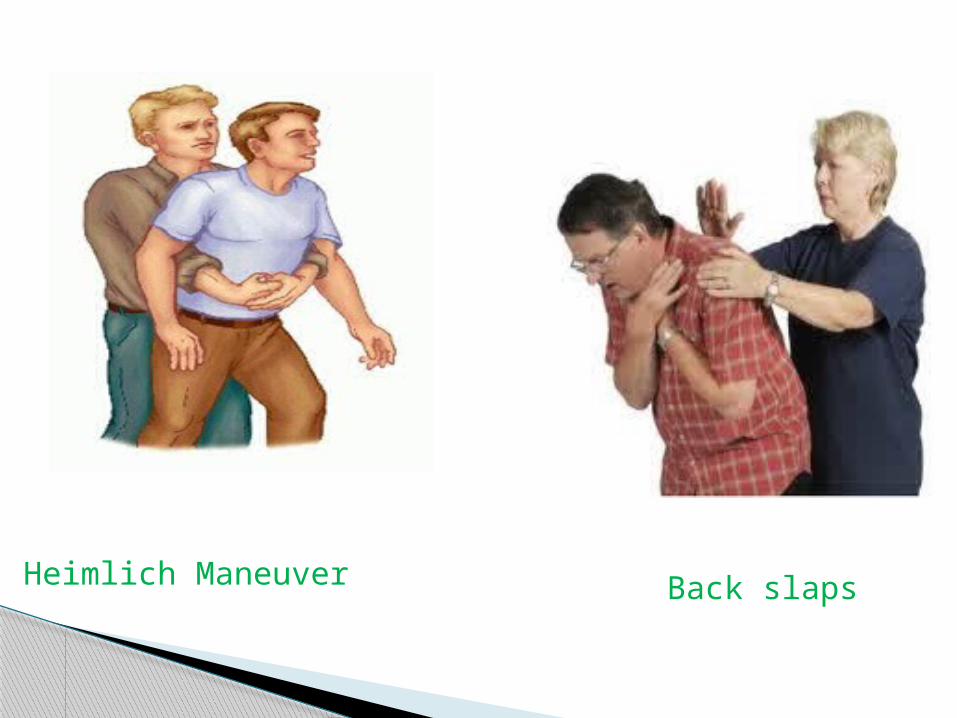
Back slapsHeimlich Maneuver
Epiglottitis
Inflammation of the epiglottis
Blocks the trachea and obstructs the airway
Often a result of the H. influenzae type b virus
Never to do suction.

Symptoms and signs may include:
Air way closed
Increased pulse
Restlessness
Retraction of inter costal muscles
Anxiety
Inspiratory stridor
Drooling: dropping of saliva.
AIR RAID
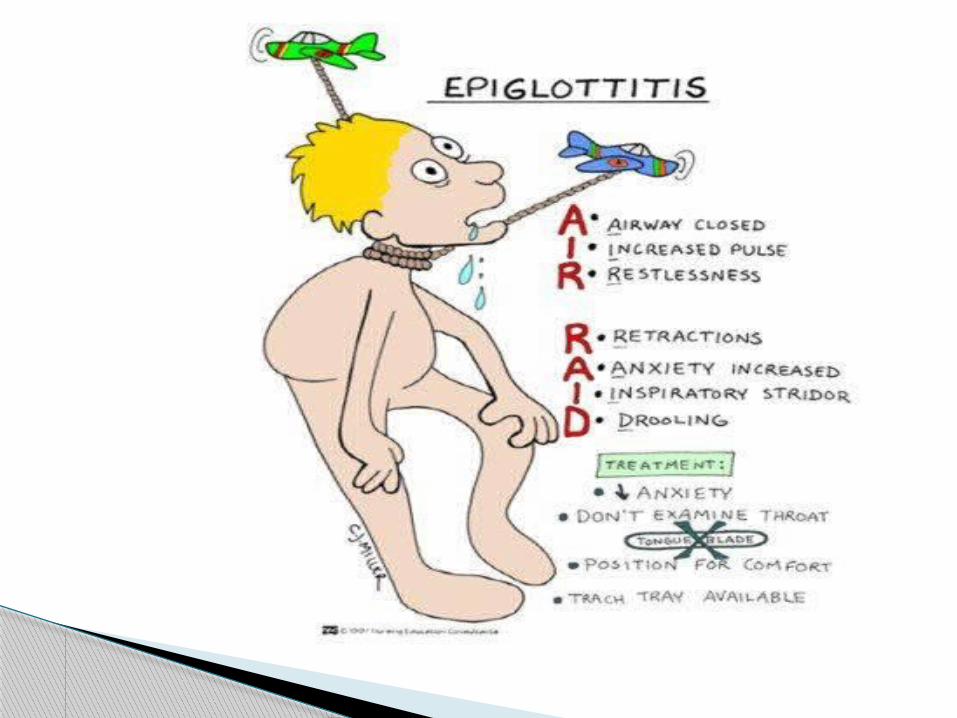
Assessment and management:
Transport to an appropriate hospital.
Minimize scene time.
Do not start suction.
Do not attempt to look in the mouth.
Laryngitis
Swelling and inflammation of the larynx
Causes may include:
Bacterial ( Pneumonia ).
Irritants and chemicals
Allergies
Assessment and management
Symptoms include:
Fever.
Hoarseness of voice.
Swollen lymph nodes or glands.
Have the patient follow up with a physician.
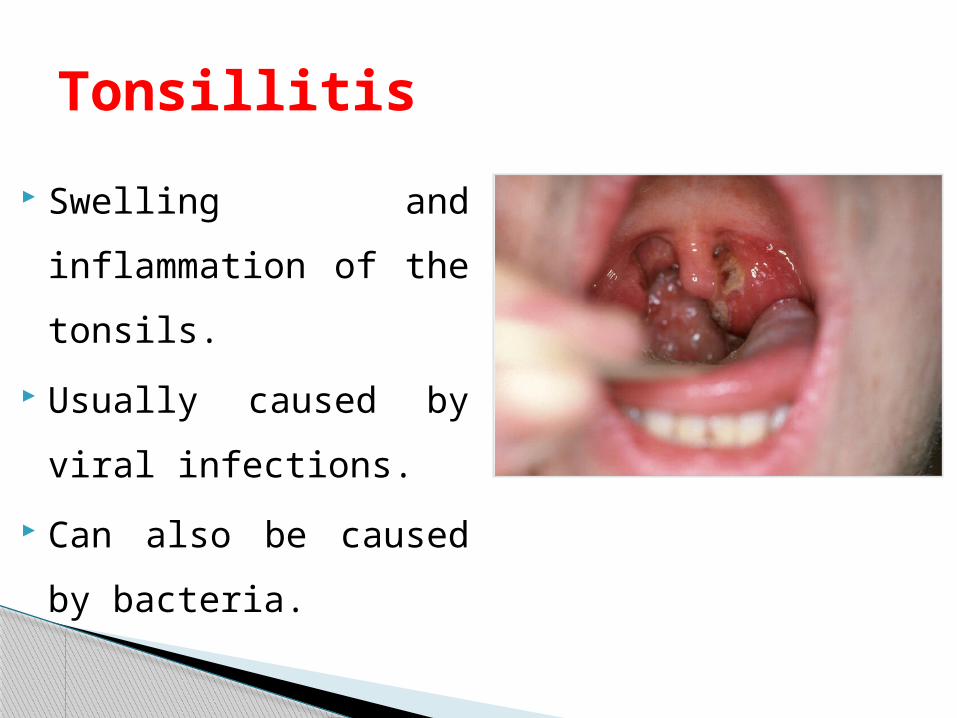
Swelling and
inflammation of the
tonsils.
Usually caused by viral
infections.
Can also be caused by
bacteria.
Tonsillitis
Assessment and management
◦ Symptoms:
Sore throat
Difficulty swallowing
◦ Signs:
White or yellow coating or patches
Swollen tonsils
Fever
Sore throat
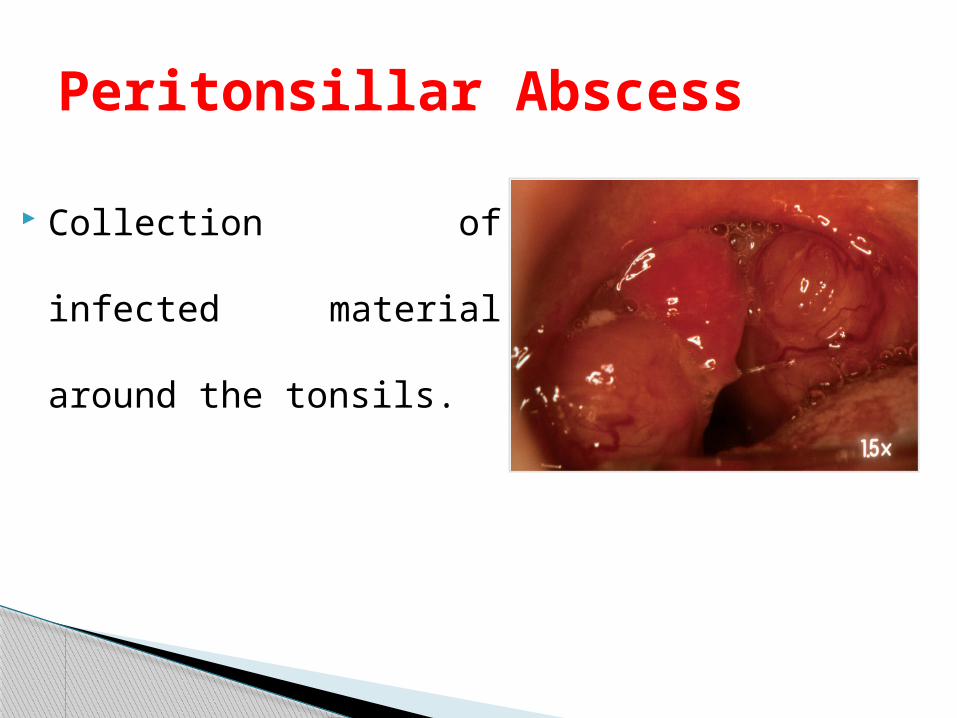
Collection of infected
material around the
tonsils.
Peritonsillar Abscess
Symptoms may include:
Facial swelling.
Inability to swallow.
Sore throat.
Difficulty swallowing.
Treatment:
Treatment involves antibiotics and draining the
abscess.
Transport patient to the hospital.