Dr. Khin Maung Aye Vice President Myanmar Medical Association
14
2/7/2012 1 Dr. Khin Maung Aye Vice President Myanmar Medical Association WHO stated that health is : - Basic Human Right Worldwide social goal Is Essential to the satisfaction of basic human needs “Health is Wealth”
Transcript of Dr. Khin Maung Aye Vice President Myanmar Medical Association
2/7/2012
1
Dr. Khin Maung AyeVice President
Myanmar Medical Association
WHO stated that health is : -
Basic Human RightWorldwide social goal Is Essential to the satisfaction of basic human
needs
“Health is Wealth”
2/7/2012
2
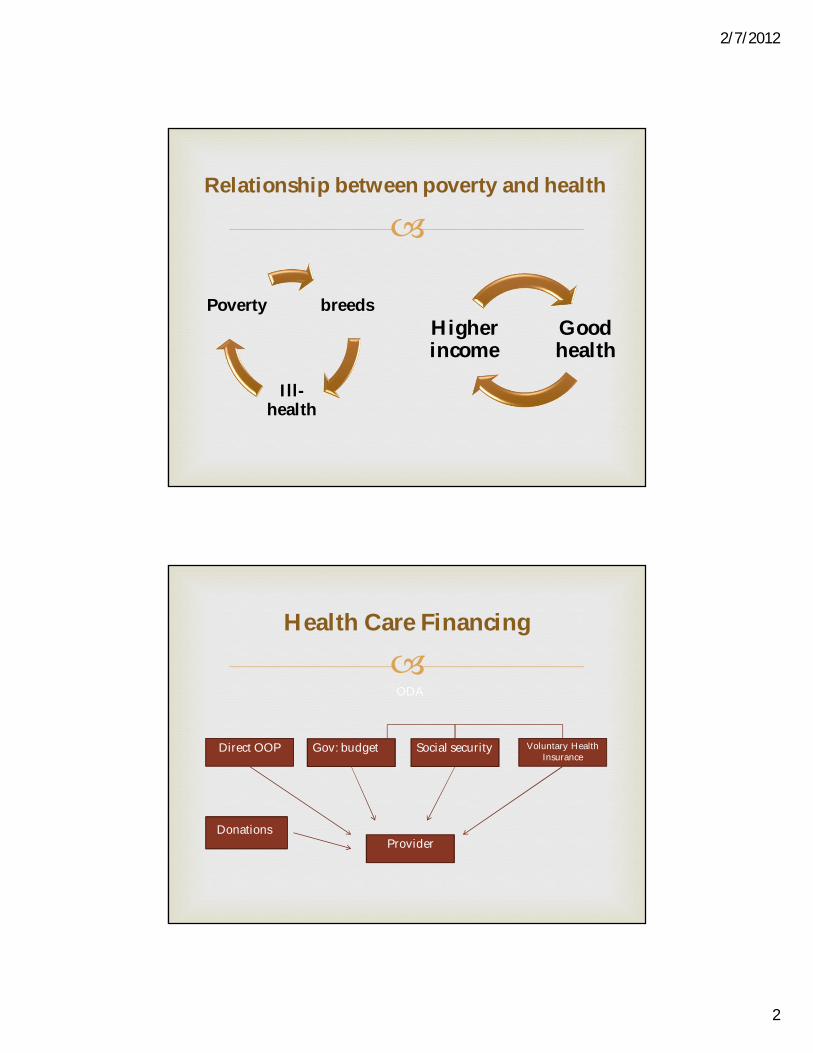
breeds
Ill-health
Poverty
Relationship between poverty and health
Good health
Higher income
Health Care Financing
ODA
Direct OOP Gov: budget Social security Voluntary Health Insurance
ProviderDonations
2/7/2012
3
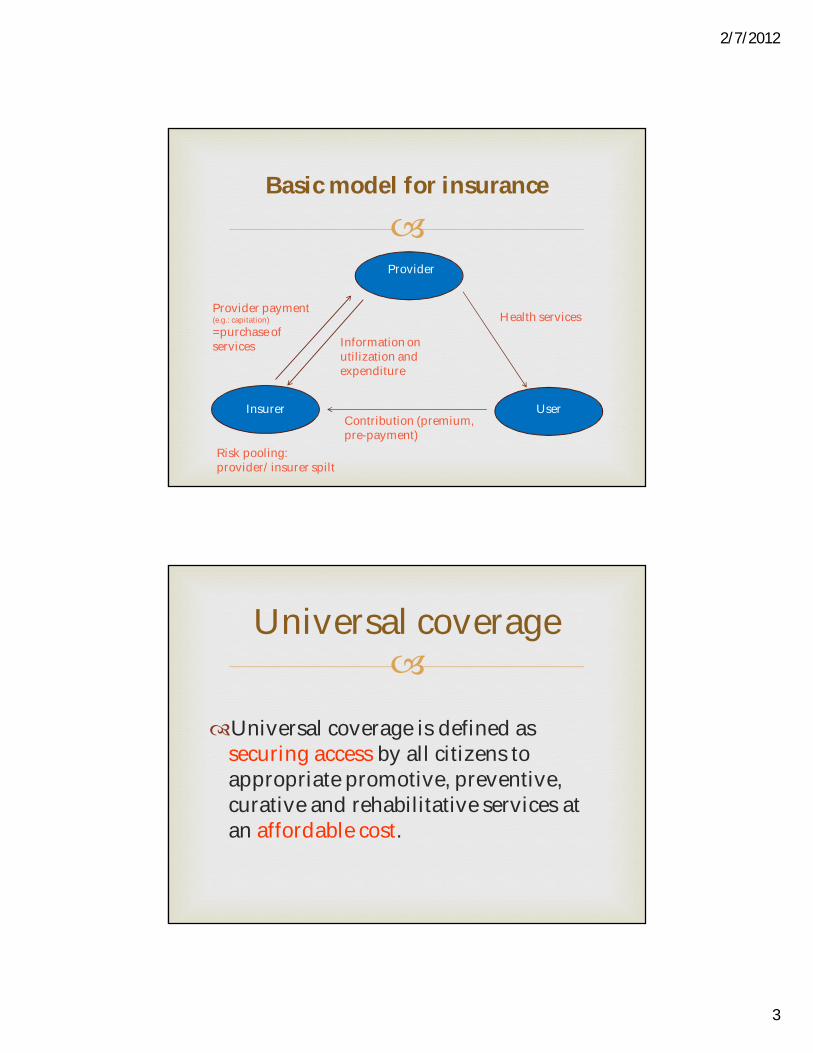
Basic model for insurance
Provider
UserInsurer
Health services
Contribution (premium, pre-payment)
Risk pooling: provider/insurer spilt
Provider payment(e.g.: capitation) =purchase of services Information on
utilization and expenditure
Universal coverage
Universal coverage is defined as securing access by all citizens to appropriate promotive, preventive, curative and rehabilitative services at an affordable cost.
2/7/2012
4
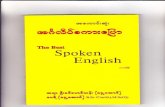
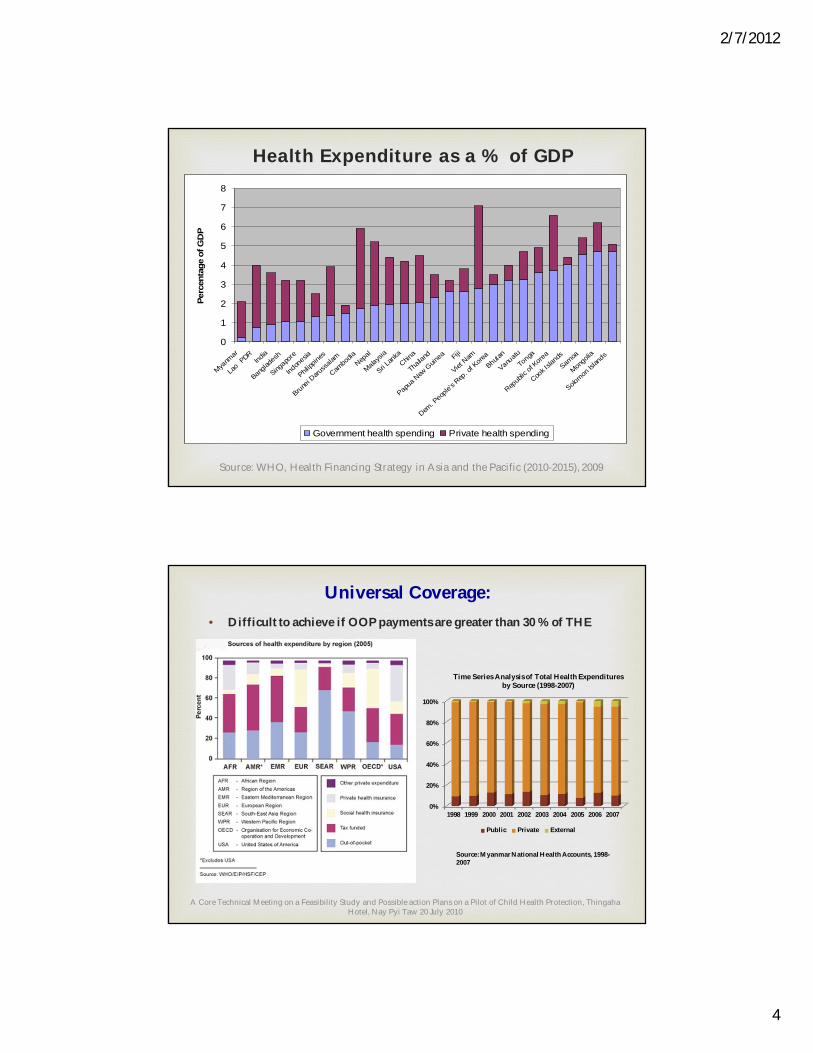
Health Expenditure as a % of GDP
0
1
2
3
4
5
6
7
8
Myanm
ar
Lao
PDRInd
ia
Bangla
desh
Singapo
re
Indon
esia
Philipp
ines
Brunei D
aruss
alam
Cambo
diaNep
al
Malaysia
Sri Lan
kaChin
a
Thaila
nd
Papua
New
Guin
ea Fiji
Viet N
am
Dem. P
eople
's Rep
. of K
oreaBhuta
n
Vanuatu
Tonga
Repub
lic of
Korea
Cook I
sland
s
Samoa
Mongo
lia
Solomon
Islan
ds
Perc
enta
ge o
f GD
P
Government health spending Private health spending
Source: WHO, Health Financing Strategy in Asia and the Pacific (2010-2015), 2009
Universal Coverage:• Difficult to achieve if OOP payments are greater than 30 % of THE
A Core Technical Meeting on a Feasibility Study and Possible action Plans on a Pilot of Child Health Protection, ThingahaHotel, Nay Pyi Taw 20 July 2010
0%
20%
40%
60%
80%
100%
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
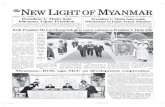
Time Series Analysis of Total Health Expenditures by Source (1998-2007)
Public Private External
Source: Myanmar National Health Accounts, 1998-2007
2/7/2012
5
Catastrophic health expenditure
It defined as spending more than 40% of household consumption expenditure, excluding food, on health, or more than 10% of total household consumption expenditure on health.
10
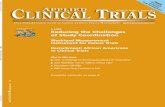
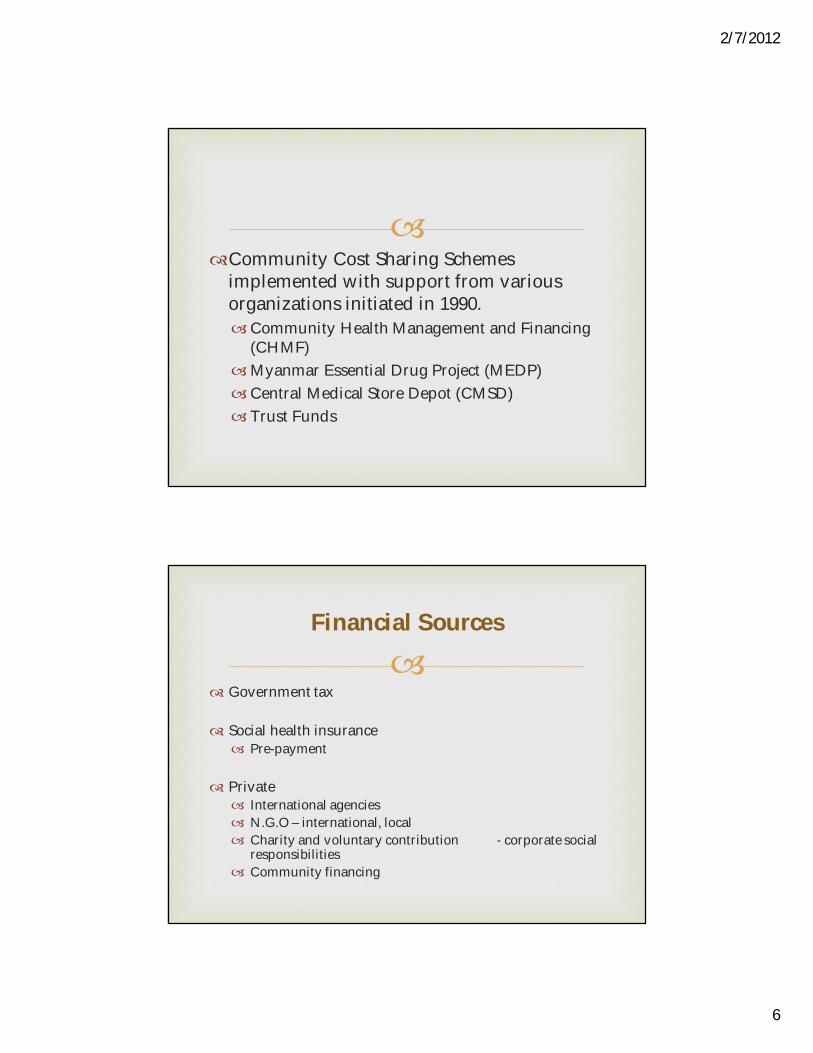
Three path to move toward Universal Coverage
Total Health Expenditure
Breadth: population cover
Depth & QualityService cover
Hei
ght:
Cost
sha
ring
Public Expenditureon Health
Cover vulnerable
Reduce OOPScale-up PHC
2/7/2012
6
Community Cost Sharing Schemes
implemented with support from various organizations initiated in 1990.Community Health Management and Financing
(CHMF)Myanmar Essential Drug Project (MEDP)Central Medical Store Depot (CMSD) Trust Funds
Government tax
Social health insurance Pre-payment
Private International agencies N.G.O – international, local Charity and voluntary contribution - corporate social
responsibilities Community financing
Financial Sources
2/7/2012
7
Government
Hospital Doctor Nurses Staffs
Non-Profit Private Hospital meant for community & poor people
Social Health Insurance Advocacy Education to public
Drugs Local pharmaceutical factories
Reduction of out-of-pocket payment
Most drugs are imported
Prices are high
Unaffordable by most patients
Need pharmaceutical industries locally to make adequate supply for all
Government guidelines for use of essential drugs in day-to-day practice to reduce the cost of medications
Medicine
2/7/2012
8
Population coverage by financial protection schemes
The population groups are re-categorized the formal group, the poor group and the informal and the rest of the population group.
The rest of the population consists of non-poor children and elderly dependents and other economically inactive groups.
Protecting the formal employment sector
• Different provider payment arrangements can have different effects on doctors’ clinical decisions and behaviour on resource use.
• International experience indicates that a fee for service payment stimulates unnecessary diagnosis, prescription, and treatment, resulting in cost escalation; closed-end payment such as capitation and case-based payment have lower costs.
2/7/2012
9
Health Financing Strategy for the Asia Pacific Region (2010-
2015) South-East
Universal coverage usually is attained in countries in
which public financing of health is around 5% of gross domestic product
(GDP). This is an important goal for all countries in the Asia Pacific region to
consider as they move towards universal coverage.
2/7/2012
10
target indicators
(1) out-of-pocket spending should not exceed 30%–40% of total health expenditure;
(2) total health expenditure should be at least 4%–5% of the gross domestic product;
(3) over 90% of the population is covered by prepayment and risk pooling schemes; and
(4) close to 100% coverage of vulnerable populations with social assistance and safety-net programmes.
The eight strategic areas are:
(1) increasing investment and public spending on health
(2) improving aid effectiveness for health (3) improving efficiency by rationalizing health
expenditures (4) increasing the use of prepayment and pooling
2/7/2012
11
The eight strategic areas are:
(5) improving provider payment methods (6) strengthening safety-net mechanisms for the poor
and vulnerable (7) improving evidence and information for
policymaking, and (8) improving monitoring and evaluation of policy
changes.
Efficiency issues in the Asia Pacific region
70% of desirable health interventions can be delivered at the primary level, but an average of only 10% of health resources are used for primary level care in Asia.
2/7/2012
12
Social safety-net mechanisms aim to
increase social protection by reducing barriers that exclude the poor and vulnerable from accessing health services.The barriers may be economic,
political, social and cultural, or a complex interaction of all these factors.
What are the Obstacles to Universal coverage?
Exclusion linked to factors outside the health system – inequalities in income, education and social exclusion associated with e.g. ethnicity, gender and migrant status
Weak health systems: Insufficient health workers, medicines and health technologies. Ineffective service delivery.
2/7/2012
13
What are the Obstacles to Universal coverage?
Health financing systems that do not function. This is critical because the other parts of the health system cannot function if the financing system is weak
Three Fundamental Health Financing Problems The need to raise sufficient funds for health– more
money for health.Heavy reliance on direct out-of-pocket payments to
finance health in many countries, discouraging people from seeking care and resulting in financial hardship when they do.
2/7/2012
14
Three Fundamental Health Financing Problems
Inefficiency and inequity in use of resources,, reducing the amount of "health for the money“ –more health for the money
To initiate a pilot health insurance model.
To explore options of community based health financing mechanisms.
To seek external technical inputs.
NGOs like MMA can take part in advocacy and participation in the pilot project.
Conclusion