Dr Jenny Visser - GP CME North/Sun_Baytrust_0715... · #6 Cook Islands (3.3%) #7 Samoa (2.0%) #8...
96
Don’t let the travel bugs get you This meeting is sponsored by GSK Dr Jenny Visser Senior Lecturer in Travel Medicine University of Otago School of Medicine Wellington Chaired by Dr Bryn Thompson General Practitioner, Crawford Medical Centre, Auckland
Transcript of Dr Jenny Visser - GP CME North/Sun_Baytrust_0715... · #6 Cook Islands (3.3%) #7 Samoa (2.0%) #8...

Don’t let the travel bugs get you
This meeting is sponsored by GSK
Dr Jenny Visser
Senior Lecturer in Travel Medicine
University of Otago School of Medicine
Wellington
Chaired by Dr Bryn Thompson
General Practitioner, Crawford Medical Centre, Auckland

To understand the:
The importance of travel medicine
The steps that form the foundations for an effective pre-travel consultation
Common travel health topics, including:
Vaccine-preventable diseases
Malaria prevention
Objectives for today’s meeting

Resource to support your pre-travel
consultations
Pre-travel consultation checklist
Written by Jenny Visser & provided in your
delegate folders from GSK
Email [email protected]
for an electronic version if you want
to print additional copies

Request from GSK – “help us improve our meetings”
Evaluation form is also in your delegate folders
Please complete and leave on your chair at the
end of the session or hand to a GSK staff member

Enter the quiz to win...
5
Hint: listen very carefully to Jenny’s presentation....
Please pass your entry forms to GSK staff at door
as you leave the meeting room

TRAVEL MEDICINE
GP CME CONFERENCE ROTORUA
2014
Dr
DR JENNY VISSER
GSK BREAKFAST SYMPOSIA
Don't let the travel
bug get you”

Disclaimer
The speaker received funding from GlaxoSmithKline (GSK)
to prepare and present this symposia. She has no other
commercial interests to disclose.

Outline
Overview of Travel
Medicine
Key Resources
The Pre-Travel
Consultation
Information gathering
Travel Health Topics
Vaccine preventable diseases
Malaria
Q&As

Why Travel Medicine? Because
People travel
Destinations often
tropical
developing countries
Travellers get sick
Modern travel is usually rapid
the chance for acclimatisation
is limited
We can offer some protection
from travel related risks
It’s fun!


How many NZers travel/year?
Total NZ Residents short-term departures*
2013: 2.20 million
2012: 2.17 million
2011: 2.09 million
2010: 2.03 million
2009: 1.92 million
2000: 1.28 million
*Ministry of Transport. See http://www.transport.govt.nz/ourwork/tmif/transport-volume/tv011/

See: http://www.transport.govt.nz/assets/TI-Images/TV011-series1-image1.PNG

NZ Resident short-term departures: Top 10
“main” destination 2013/%*
#1 Australia (46.0%)
#2 USA (6.5%)
#3 Fiji (5.2%)
#4 UK (4.4%)
#5 China (3.3%)
#6 Cook Islands (3.3%)
#7 Samoa (2.0%)
#8 Thailand (1.9%)
#9 India (1.9%)
#10 Indonesia (1.1%)
* Statistics New Zealand. See http://www.stats.govt.nz/browse_for_stats/industry_sectors/imports_and_exports/global-nz-dec-13.aspx




Travellers get sick*
Between 20-70% of
international travellers
suffer some illness
About 5% need to seek
medical care
About 1% hospitalised
*Steffen R, Amitirigala I, Mutsch
M. Health Risks Among Travelers
— Need for Regular Updates.
Journal of Travel Medicine.
2008;15(3):145-6.

Travel Medicine: Assessing Risk
Hazard+Exposure+Susceptibility
Individualised Risk Assessment
Risk Management/Health Promotion

Outline
Overview of Travel
Medicine
Key Resources
The Pre-Travel
Consultation
Information gathering
Travel Health Topics
Vaccine preventable diseases
Malaria
Q&As

Travel Medicine resources Travel medicine
practitioners
Electronic: World Health Organization Centre for Disease Control and
Prevention (USA) Fit for Travel UpTo Date BPAC NZ Holidayhealth.co.nz NZ Ministry Foreign Affairs
Publications
Travel Medicine Research Reviews
MIMS Travel Medicine Guide

World Health Organization Travel Health Homepage http://www.who.int/topics/travel/en/
International Travel & Health http://www.who.int/ith/en/
Country list http://www.who.int/ith/ITH_country_list.pdf?ua=1
“Annex 1” http://www.who.int/ith/ITH_Annex_I.pdf?ua=1
Disease Topics http://www.who.int/topics/en/

WHO: International travel and health
and Country List


Centre for Disease Control and
Prevention
Travel Health Homepage
http://wwwnc.cdc.gov/travel/
CDC Health Information for International Travel “Yellow Book”http://wwwnc.cdc.gov/travel/page/yellowboo
k-home-2014
Destinationshttp://wwwnc.cdc.gov/travel/destinations/list
/?s_cid=cdc_homepage_topmenu_003


Areas with malaria: Present in the
following districts: Central and
North West (including Chobe National
Park). None in the cities of
Francistown and Gaborone.
Estimated relative risk of malaria
for
US travelers:Very low.
Drug resistance4: Chloroquine.
Malaria species: P. falciparum 90%,
P. vivax 5%, P. ovale 5%.
Recommended chemoprophylaxis:
Atovaquone-proguanil, doxycycline,
or mefloquine.
CDC Yellow Book Chapter 3: Travel Vaccines and Malaria Information by Country: See
http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-
related-to-travel/travel-vaccines-and-malaria-information-by-country/botswana#seldyfm533

UK Resources
“Fit for Travel”
http://www.fitfortravel.scot.nhs.uk/
The National Travel Health and Network
Centre
http://www.nathnac.org/

“Fit for Travel: See http://www.fitfortravel.nhs.uk/home.aspx

UpToDate
UpToDate general information and patient
education
http://www.uptodate.com/contents/tra
vel-
advice?source=search_result&search=trav
el&selectedTitle=1~150


BPAC NZ
Providing Medical Advice to Travellers
http://www.bpac.org.nz/BPJ/2011/dec
ember/travellers.aspx

Research Reviews
http://www.researchreview.co.nz/nz/Clin
ical-Area/Internal-Medicine/Infectious-
Diseases/Travel-Medicine.aspx

MIMS Travel Medicine Guide

NZ Travel Advisories
NZ MFAT “Safe Travel”
https://www.safetravel.govt.nz/

Outline
Overview of Travel
Medicine
Key Resources
The Pre-Travel
Consultation
Information gathering
Travel Health Topics
Vaccine preventable diseases
Malaria
Q&As

The Pre-travel Consultation..setting the
scene
24 year old about to embark
on a 12 month backpacking
trip through Asia, Europe and
Africa.
What more do you need to
know?
What topics do you need to
cover in the pre-travel
consultation?

Pre-Travel Consultation: What information
do you need?
About them
Demographics Contact details
Travel experience Past Medical History
Past DVT/VTE Ongoing & specific medical
conditions Regular & intermittent medications Allergies (general and specific) Recent
illness/operations/hospitalisations/investigations
Women:Pregnancy(current or planned)/Contraception
Vaccination history
About the trip
When do they leave
Where? (Exact itinerary)
How long?
Type of trip? Guided Independent Business/Employment Holiday Volunteer
Mode of transport?
Type of accommodation?
Planned activities?
Any specific concerns?

Pre-Travel Consultation: Range of topics
to covered
Fitness to Fly Issues Vaccine preventable
diseases/vaccines Preventing food and water-
borne illnesses Travellers diarrhoea
Prevention of Vector-borne Diseases
Malaria
Dengue
Chikungunya
Zika Sexual & Reproductive Health
STIs
Other Infectious Diseases
Schistosomiasis Activity specific advice
Altitude/Trekking
Scuba diving Management of ongoing
medical conditions Psychological preparedness Safety & Security/Responsible
travel Medical Kit Post Travel visit

How are you going to fit this into your
busy practice?
Refer some/all
Yellow Fever Nearest approved vaccinator
Rabies/JE
Identify pre-travel consultations
Book dedicated consultation
30 minutes
Submit itinerary before
Multiple visits
Team approach
Inter-professional
Written material/online traveller resources
Use the pre-travel checklist
Develop resources eg pre-travel health questionnaire
Up skill
PG qualifications
ISTM Certificate of Knowledge

Outline
Overview of Travel
Medicine
Key Resources
The Pre-Travel
Consultation
Information gathering
Travel Health Topics
Vaccine preventable diseases
Malaria
Q&As

Vaccinations for Travel: The Three “Rs”
Routine
National vaccination schedule
Childhood
Adult boosters
Influenza
Required
Yellow Fever
Meningococcal
Polio
Recommended for travel

Routine: WHO Extended Programme
Immunisation* Diphtheria/Tetanus/Pertussis
Poliomyelitis
Measles/Mumps/Rubella
Varicella
Haemophilus influenzae type b
Pneumococcal disease
Hepatitis B
Human papillomavirus**
Rotavirus**
Influenza**
Tuberculosis (BCG)**
**may be targeted
THE PRE TRAVEL CONSULTATION IS AN OPPORTUNITY TO ENSURE THAT THE
TRAVELLER IS UP TO DATE FOR ALL ROUTINE VACCINATIONS
*http://www.who.int/ith/ITH_chapter_6.pdf?ua=1

The pre-travel consultation and Routine
vaccines
“The pre travel consultation is
an opportunity to ensure that
the traveller is up to date for
all routine vaccinations” .
Update these especially if:
Any doubt regarding status
Single adult booster good for
life
Polio
Recent outbreaks/resurgence
Pertussis
Measles/Mumps

Measles in travellers: 2013/2014 Many countries reporting
importation of measles including Including New Zealand (ex
Philippines and Vietnam) http://www.health.govt.nz/our-
work/diseases-and-conditions/2014-measles-outbreaks
Australia http://www.health.nsw.gov.au/infecti
ous/pages/measles.aspx
USA http://www.cdc.gov/measles/cases-
outbreaks.html
Europe
ttp://ecdc.europa.eu/en/publications/Publications/measles-rubella-monitoring-february-2014.pdf
If any doubt:
Give MMR pre-travel

Catch-up vaccines; Are FREE for all NZ
resident adults and children*
Children
Up to 18th birthday
Includes
Tdap
Hepatitis B
*See:
http://www.immune.org.nz/ne
ws/extension-catch-eligibility
Adults (18yrs +)
NZ Resident or Refugee
Eligible for
3 Td
3 IPV
2 MMR (DOB > 1/1/1969)
3 HPV (females 18-20 yrs)
All funded vaccines but
cannot claim vaccine
administration charge


NZ Immunisation Schedule: July 1st
2014 changes *
New Vaccines listed: Rotavirus (for all eligible
patients) Varicella (for patients at high
risk from infection) Hepatitis A (for eligible
patients) Higher strength hepatitis B
for the vaccination of dialysis patients and patients who have had a liver or kidney transplant
Monovalent conjugated meningococcal C.
Other changes: Gardasil funded up to 18 years Pneumococcal: 13 valent
Prevenar® replaces 10 valentSynflorix®
Revaccination of children post immunosuppression funded
Meningococcal: Menactra® (conjugate) replaces Menomune®(polysaccharide)
See: * http://www.pharmac.health.nz/news/notification-2013-12-17-national-immunisation-schedule-changes/

As Travel Medicine practitioners we
need to be familiar with
NZ National Immunisation
Schedule
Overseas schedules
Europe: http://vaccine-
schedule.ecdc.europa.eu/Pages/S
cheduler.aspx
USA:
http://www.cdc.gov/vaccines/sc
hedules/easy-to-read/child.html
Criteria for funded vaccines
for at risk populations
Pre/Post Splenectomy &
functional asplenia
Hib
Pnuemococcal
Meningococcal
IMAC/MOH
recommendations for use of
non-funded vaccines
2013 Vaccination “Research
Review”

Travel Vaccines -Recommended
Hepatitis A
Typhoid fever
Cholera
Japanese encephalitis
Meningococcal disease
Rabies
Tick-borne encephalitis
Yellow fever (personal
protection)

Travel Vaccines -Required
International Health Regulations 2005
Yellow fever (public health)
Meningcoccal disease
Saudi Arabia to attend Haj
Polio
Saudi Arabia to attend Haj
May 2014: All residents/long term travellers leaving Cameroon, Pakistan & Syria

Temporary Polio Requirements (effective as of 5th May 2014 and will be reviewed in 3m)*
Exporting Countries
“Cameroon
Pakistan
Syria
Recommendations: Countries which are currently
exporting wild poliovirus should ensure that all residents and long-term visitors (of over 4 weeks) receive a dose of oral polio vaccine (OPV) or inactivated poliovirus vaccine (IPV) between 4 weeks and 12 months before international travel; and should ensure that such travellers are provided with proof of vaccination” (ie on International Certificate of Vaccination or Prophylaxis)
Other Polio Affected Countries “Afghanistan
Equatorial Guinea
Ethiopia
Iraq
Israel
Nigeria
Somalia
Recommendations:
Other polio-affected countries are encouraged to vaccinate residents and long-term visitors before international travel”.
*http://www.polioeradication.org/Infectedcountries/PolioEmergency.aspx#sthash.lCe6RgnG.dpuf

Rationalising Travel Vaccines
STEP 1: What vaccine preventable diseases are a hazard, what is exposure & susceptibility?
STEP 2: Risk Assessment: Which ones are a high enough risk to justify vaccination?
STEP 3: Negotiate with the traveller
STEP 4: Which vaccines and when?
Helpful Hint: Split into those
Highly recommended
Recommended
Are they planning other travel in the future?

Some are both Routine and
Recommended for Travel
Tetanus/Diptheria/Pertussis
Polio
Influenza
Hepatitis B

The Pre-Travel Consultation and Vaccines:
Quick and Easy approach….
Always Routine
Required Nearly always*
Tetanus, Diphtheria & Pertussis
Hepatitis A
Influenza Often*
Typhoid
Hepatitis B Sometimes*
Yellow fever
Meningitis
Rabies
Cholera
Japanese encephalitis
Pneumococcal
(* Assuming travel to developing country)

Best value for money?
What is the most commonly caught vaccine preventable disease of International Travellers?
Influenza*
*Steffen R. Influenza in Travelers: Epidemiology, Risk, Prevention, and Control Issues. Curr Inf Dis Rep. 2010;12(3):181-5.

Common pre-travel “vaccine errors”
Ordering serology eg pre-MMR and hepatitis B
Poor advice regarding rabies
Revaccinating hepatitis B
Giving a single Twinrix® pre-travel
Ideal traveller for Twinrix®
Older
Time for full series Licensed for rapid schedule
(Day 0, 7, 21 and 12 months)*
*http://www.medsafe.govt.nz/profs/datasheet/t/Twinrixinj.pdf

Prescribe, Schedule & Administer

Administration of Vaccines
The maximum number of vaccines that can be given at one visit is:
One
Two
Four
Six
No limit

Administration of Vaccines
The maximum number of injections that can be given into one
muscle is:
One
Two
Four
No limit

Live vaccines
General administration
principles?
Either on same day or 4
weeks apart

MMR & Hepatitis B in 2014
Hepatitis B Covered?
Age up to 26yr Yes: 3 x Hep B vaccinations, so immune
Age 26 – 30 Probably: Pre-school catch-up programme
Age 31 – 40 Possibly: School based catch up programme extended in 1990
Age 40+ No: unlikely vaccinated
MMR
Age up to 25yr Yes: 2 x MMR
Age 25 - 36 No: 1 x MMR only
Age 36 - 45 No: 1 x monovalent measles only
Age 45+ Yes: Natural immunity from childhood disease

Vaccination Scenario 50-year old Dan going on a high end 3-week African adventure
Starting with 2 days in Stellenbosch, Capetown, before flying to
Skeleton Coast (Namibia) & visiting Etosha
Overlanding to Chobe & the Okovango Delta in Botswana
Crossing into Zambia, staying in Livingstone and seeing Victoria
Falls
Flying to Zanzibar via Dar Es Salaam for 4 days on the beach
Return flight: Zanzibar, Jo-Burg, Perth, NZ
He leaves in I month

Vaccines for Dan?
Routine:
Did he get his childhood vaccines? MMR
ADT at 45 years
Influenza
Has he had chicken-pox/Varicella (the disease)?
Required:
Yellow Fever Risk of exposure very low
But having been in Zambia and Tanzania ,South Africa can demand proof of vaccination
Recommended:
AdTap (if > 10years)
Influenza
Hepatitis A
Discuss
Rabies
Typhoid
Hepatitis B
ETEC (Dukoral®)
Polio
Meningococcal

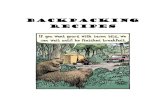
WHO: Yellow Fever Vaccination
Recommendations
See: http://gamapserver.who.int/mapLibrary/Files/Maps/ITH_YF_vaccination_africa.png?ua=1

Vaccines for Dan?
He agrees to:
AdTap
Influenza
Hepatitis A
Hepatitis B
Rabies
Yellow fever

Vaccines for Dan?
Which vaccines? AdTap
Boostrix®/Adacel®
Influenza Fluarix® /Influvac®/Fluvax®
Hepatitis A Havrix®/Vaqta®/Avaxim®
Twinrix®
Hepatitis B Engerix®/HBVax®
Twinrix®
Rabies Verorab®
Yellow Fever Stamaril®
And if had opted for Typhoid:
Typherix® /TyphimVi®
Hepatyrix® /Vivaxim®

Vaccine Schedule: Name/Dose/Route: one
example
Vaccine Visit one - Day 0 Visit two – Day 7 Visit three – Day21
Boostrix®
0.5ml IM
*
Twinrix®1.0ml IM
* * *
Stamaril® 0.5ml SC *
Fluarix® 0.5ml IM *
Verorab® 0.5ml IM * * *
* 4th Twinrix® due 12 months


Vaccination…….
There is no magic list
Many vaccine preventable diseases and few absolute guidelines
Need to make a careful risk assessment and advise which vaccinations would be beneficial for each specific traveller
Need to strike the right balance. Just because there is a vaccine does not mean every traveller should get it.
Travel vaccines are NOT cheap, the cost to the traveller (or employer/aid agency) rapidly adds up

Outline
Overview of Travel
Medicine
Key Resources
The Pre-Travel
Consultation
Information gathering
Travel Health Topics
Vaccine preventable diseases
Malaria
Q&As

Malaria in Travellers
Annually approximately 25-30 million international
travellers from non endemic areas travel to endemic areas*
Internationally an estimated 30 000 cases of travel-associated
malaria occur**
Evidence that incidence is reducing in returning travellers,
but proportion of falciparum malaria increasing***
*Loutan, L. (2003) Malaria: still a risk to travellers. Int J Antimicrob Agents 21, 158-63
** Kain, K., & Keystone, J. (1998) Malaria in travellers: epidemiology, disease and prevention. Inf Dis
Clin N Am 12, 267-84
*** Schlagenhauf P, Hommel M. (2011) Travellers' malaria-'one shoe does not fit all'. Malaria J.
10(1):129

Malaria notifications New Zealand

NZ Imported Malaria: 13 years data* 666 cases
80% (533) non-military: 20% (133) military
In non-military
Average 41 cases/year
Acquired in PNG (24.4%)
India (18.6%)
Solomon Islands (8.8%)
Indonesia (6.1%)
Vanuatu (5.9%)
Uganda (2.9%)
Thailand (2.7%)
Tanzania (2.7%)
Malawi (2.7%)
*Lau et al. VBZ Dis. 2014;14(2):134-40.

Lau et al. VBZ Dis.
2014;14(2):134-40.P. vivax: 72.7%
P. falciparum: 27.2%

Imported malaria Auckland 2008-
2009*
34 cases in 32 individuals
24 male & 8 female
Mean age 21 (6m-75 yrs)
Background
11/32 NZ residents
21/32 new arrivals
11 refugees
10 migrants
*Camburn et al. NZMJ
2012;125(1365):1-6.
Of 11/32 NZ residents
8/11 VFRs
3/11 missionaries
6 falciparum malaria
4 vivax malaria
1 both
“Malaria in Akld is seen
in new arrivals and VFR
travellers, not in
tourist travellers”

Lau et al. VBZ Dis.
2014;14(2):134-40.

Risk of Malaria Incidence of malaria in travellers without chemoprophylaxis
(per month)*
PNG >3%
Solomon Islands >3%
West Africa 2.4%
East Africa 1.2%
India 0.35%
South-east Asia 0.1%
South America 0.05%
*Loutan L. Malaria: still a threat to travellers. International Journal of Antimicrobial Agents. 2003;21(2):158-63.

PREVENTING MALARIA in Travellers
A Awareness-know the risk
B Bites by mosquitoes-prevent
C Compliance with Chemoprophylaxis
D Diagnose malaria swiftly and treat
appropriately

Malaria Chemoprophylaxis Malaria chemoprophylactics
currently available in New Zealand
Chloroquine
Mefloquine
Doxycycline*
Malarone
Primaquine**
* Not licensed as an antimalarial in NZ
Unlicensed medication. Available only under Section 29 of Medicines Act.

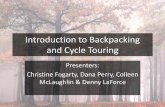
Malaria transmission and drug sensitivity across the world.
Lalloo D G , Hill D R BMJ 2008;336:1362-1366
©2008 by British Medical Journal Publishing Group

Anti-malarial Regimens* All Regions (no mefloquine
resistance) Mefloquine Doxycycline Atovaquone plus Proguanil
(Malarone®)
Regions with chloroquine sensitivity Chloroquine
Mefloquine resistant areas Doxycycline Malarone
* WHO: http://www.who.int/ith/ITH_country_list.pdf?ua=1


MALARIA LIFECYCLE

Chloroquine resistant malaria World wide all P falciparum
malaria is chloroquine resistant*
In areas of chloroquine resistance (but no mefloquine resistance) use*:
Mefloquine or Doxycycline or Malarone®
* WHO: http://www.who.int/ith/ITH_country_list.pdf?ua=1
This order implies nohierarchy of choice.
Which is chosen will depend on pre-existing conditions
concomitant medications
personal preference
what the traveller can afford.

Chloroquine In New Zealand currently
only available as Hydroxychloroquine
(Historically and overseas chloroquine sulphate/phosphate)
Dose: 400mg (310mg base) once weekly commenced 2 weeks prior to entering malarial area, weekly while there and weekly for 8 weeks after*
* http://www.medsafe.govt.nz/profs/datasheet/p/Plaqueniltab.pdf
Only indicated in areas where no chloroquine resistance recorded* BUT
Only in areas with P vivax alone
Few destinations, parts of Central America
Few travellers go to these areas
In chloroquine sensitive P vivax regions, can use doxycycline, mefloquine or Malarone®
Hydroxychloroquine costs about the same as mefloquine
RARELY used
** WHO: http://www.who.int/ith/ITH_country_list.pdf?ua=1

Mefloquine Lariam® in New Zealand
Various generics available overseas
DOSE*: one tablet (250mg) once weekly commencing 2-4 weeks prior to entering malarial zone, once weekly while there and once weekly for 4 weeks after
Rapid loading dose is licensed (but use with caution) one tablet daily for 3 days and
weekly there-after
* http://www.medsafe.govt.nz/profs/datasheet/l/lariamtab.pdf
Adverse events Neuropsychiatric (NP)
Prevalence highly variable depending on study population and definitions
One review.* Disabling NP AEs reported in 0.008-0.1% of users
Recent “Blackbox” warning in USA**
Carefully select who you prescribe it to
* Toovey S. Mefloquine neurotoxicity: A literature review. Trav Med Inf Dis. 2009;7(1):2-6.
** http://www.fda.gov/drugs/drugsafety/ucm362227.htm

Doxycycline Widely used as malaria
chemoprophylaxis
Not licensed as such in NZ, but widely prescribed
DOSE: 100mg once daily commencing 2 days prior to entering malarial zone, daily while there and daily for 4 weeks after*
* WHO: http://www.who.int/ith/ITH_country_list.pdf?ua=1
Adverse events*
oesophagitis, oesophageal perforation, indigestion/dyspepsia
sun sensitivity/rash
Candidiasis
* http://www.medsafe.govt.nz/profs/datasheet/d/Doxinetab.pdfand http://www.medsafe.govt.nz/profs/datasheet/d/Doxytab.pdf

Malarone® Combination tablet of
Atovaquone 250mg and Proguanil 100mg
Dose: One tablet once daily commencing one day before entering malarial area, daily while there and daily for 7 days after leaving*
* http://www.medsafe.govt.nz/profs/datasheet/m/Malaronetab.pdf
Adverse events
Low discontinuation rates**
Commonest adverse events nausea and headache*
** Høgh B et al. Atovaquone-proguanil versus chloroquine-proguanil for malaria prophylaxis in non-immune travellers: a randomised, double-blind study. Lancet. 2000;356(9245):1888-94.

Primaquine
Not licensed in NZ Section 29
Used for eradication therapy (of the hypnozoite) in known vivax malaria or in those at increased risk of vivax malaria *
Must check for G6PD deficiency
A handful of small but well conducted studies show it is also an effective chemoprophylactic agent and it is worth considering for those where all else contraindicated **, ***
* http://www.who.int/ith/ITH_chapter_7.pdf?ua=1
** Fernando D et al. Primaquine in vivax malaria: an update and review on management issues. Malaria Journal. 2011;10(1):351
*** http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-related-to-travel/malaria

To prescribe or Not? Hospitalisation rate for adverse
events due to chloroquine or mefloquine has been measured as 1 per 10 000 users*
The incidence of malaria in travellers to many destinations (egmuch of Asia and the Americas) is less than the risk of adverse events due to chemoprophylaxis
Therefore, prescribing must be tailored taking into account: destination, season, type of travel, length of travel and personality
*Steffen R et al.(1993). Mefloquine compared with other chemoprophylactic regimens in tourists visiting East Africa.
Lancet, 341, 1299-1303

Medication Advantages Disadvantages
Mefloquine (Lariam®) Weekly dosing
Long half life
Good data for long term use
“No” accumulative adverse events
Pregnancy?: NZ Medsafe Category
B3 and advises against use in first
trimester
Safe in children ( ≥5kg)
Real and perceived adverse events
Excess neuropsychiatric side
effects
“Mid range” price
“Black Box” warning USA FDA
and European Drug safety
authorities considering the same
Doxycycline Cheap
Widely prescribed
Daily dosing
Generally well tolerated (but risk
of gastrointestinal side effects)
Compliance with 4 weeks post
travel dosing
Can’t use in children < 11yrs
(?8yrs) and pregnant women
(except maybe 1st trimester)
Atovaquone/Proguanil
(Malarone®)
Short course/easy compliance
Long half life
Well tolerated
Safe in children (≥11kg)
Cost
Limited data on use in pregnancy

Outline
Overview of Travel
Medicine
Key Resources
The Pre-Travel
Consultation
Information gathering
Travel Health Topics
Vaccine preventable diseases
Malaria
Q&As

Want to learn more?
Postgraduate qualifications in Travel
Medicine University of Otago,
Wellington.
See
http://www.otago.ac.nz/wellington
Join NZ Society of Travel Medicine
www.nztravelmedicine.co.nz
Conference August 30th/31st Rotorua

Questions?
15/06/2014
95

Reminder — evaluation forms please & remember to pass your quiz
entry to GSK as you leave the room