DR. IBRAHIM SHAH RESIDENT MEDICAL-B RESIDENT MEDICAL-B.
96
-
Upload
alexandrina-cannon -
Category
Documents
-
view
215 -
download
1
Transcript of DR. IBRAHIM SHAH RESIDENT MEDICAL-B RESIDENT MEDICAL-B.



DR. IBRAHIM SHAHDR. IBRAHIM SHAH RESIDENT MEDICAL-BRESIDENT MEDICAL-B

CASE HISTORYCASE HISTORY
A 28 years old female patient presented A 28 years old female patient presented to emergency department with a history to emergency department with a history of high grad fever and epistaxis from of high grad fever and epistaxis from the last two days.she gave birth to her the last two days.she gave birth to her first child at home. first child at home.
She had received treatment from a local She had received treatment from a local dispenser but not Improved dispenser but not Improved

PAST HISTORYPAST HISTORY Not significant Not significant
Clinical examinationClinical examination Appearance not well Appearance not well Anemia severe Anemia severe Pulse Pulse 110/m R 110/m R B.PB.P 100/70 100/70 Temperature 102 FTemperature 102 F00
RRRR 18/m 18/m

SKINSKIN Bruises & petchieBruises & petchie ENTENT Not RemarkableNot Remarkable CVSCVS Not RemarkableNot Remarkable CHESTCHEST NormalNormal CNSCNS GCS 11/15GCS 11/15
MOTOR MOTOR Normal Normal PUPILSPUPILS Responsive Responsive No Signs of Miningel Irritation No Signs of Miningel Irritation
ABDOMENABDOMEN Utrus palpable up to umbilicusUtrus palpable up to umbilicus No viceromegaly No viceromegaly B/s +veB/s +ve

FBCFBC HbHb 7.5g/dl 7.5g/dl WccWcc 27 x 10 27 x 109/L9/L
NN 72% 72% LL 22% 22% EE 1% 1%
ESRESR 72mm1st hrs 72mm1st hrs Blood filmBlood film
RBC Normochromic & NormocyticRBC Normochromic & Normocytic Fragmented cellsFragmented cells
Reticulocytes 03% Reticulocytes 03% Platlets counts 30 x 10 Platlets counts 30 x 10 99/L/L
LAB STUDIESLAB STUDIES

PT 41s(control 14s) APTT 78s (control 44s) D-dimer 1740mcg/dl FDPS 110mcg/dl S. Creatinine 0.7mg/dl S.urea 90mg/dl S.bilirubin 1.7mg/dl ALT 60iu/l AST 55iu/l Al-phosphatase 80iu/l S. Albumin 30g/l

ECGECG NormalNormal
C XRC XR NormalNormal
U/SU/S Abdomen Abdomen Post natal Utrus with retained Post natal Utrus with retained products of conceptionproducts of conception
CT BrainCT Brain NormalNormal

Serum ElectrolytesSerum Electrolytes S. NaS. Na 137mmol/l137mmol/l S. KS. K 4.6mmol/l4.6mmol/l S. ClS. Cl 98mmol/l98mmol/l
Urine REUrine RE Protein+1Protein+1
Red Cell 3/hf Red Cell 3/hf
pus cell 5/hfpus cell 5/hf Blood C/SBlood C/S Grown E-CholiGrown E-Choli Urine C/SUrine C/S Sterile Sterile

DIAGNOSISDIAGNOSIS
Septicemia due to genital tract Septicemia due to genital tract infection complicated by DICinfection complicated by DIC

DEFINITIONDEFINITION
Disseminated intravascular coagulation Disseminated intravascular coagulation (DIC) is a complex systemic thrombo-(DIC) is a complex systemic thrombo-hemorrhagic disorder involving the hemorrhagic disorder involving the generation of intravascular fibrin and the generation of intravascular fibrin and the consumption of procoagulants and plateletsconsumption of procoagulants and platelets..

ISTH Definition for DIC:
An acquired syndrome characterized by the intravascular activation of coagulation with loss of localization arising from different causes.
It can originate from and cause damage to the microvasculature, which if
sufficiently severe, can produce organ dysfunction.

PATHOPHYSIOLOGYPATHOPHYSIOLOGY
The following pathalogicalThe following pathalogical
events occur in DICevents occur in DIC
Procoagulant activation Procoagulant activation Fibrinolytic activation Fibrinolytic activation Inhibitor consumption Inhibitor consumption Biochemical evidence of end-organ damage Biochemical evidence of end-organ damage
or failureor failure

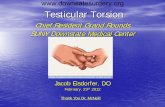
Mechanism
Tissue Injury Sepsis Endothelial Injury
Inhibit Thrombin Bleeding
&
Va &VIIIa Inhibation
Activation of the Intravascular Platlets Aggregation Fibrinolytic System Thrombosis
FDPs MAHA Consumption of platlets
and Coagulation Factors
Tissue Factor
End organ Damage

Initiation of coagulation via endothelial injury or tissue injury
subsequent release of procoagulant material in the form of cytokines and tissue factors.
Interleukin-6 and tumor necrosis factor may be the most influential cytokines involved in coagulation activation .
Regulatory mechanisms of the coagulation cascade, such as tissue factor pathway inhibitor (TFPI), antithrombin III, and activated protein C, are largely defective.

In The Setting Of Sepsis:
neutrophils and their secretory products may promote platelet-mediated fibrin formation.
Two proteolytic enzymes, thrombin and plasmin, are activated and circulate systemically.
•Their balance determines a bleeding or thrombotic tendency.

Thrombin cleaves fibrinogen to form fibrin monomers.
Thrombin ultimately potentiates the coagulation cascade and leads to small- and large-vessel thrombosis, with resultant organ ischemia and organ failure.
Plasmin, a component of the fibrinolytic system, is capable of degrading fibrin into measurable degradation products.

Acute DIC is characterized by
Generalized bleeding, ranges from petechiae to exsanguinating hemorrhage.
Microcirculatory and macrocirculatory thrombosis.
This leads to hypoperfusion, infarction, and end-organ damage.

Chronic DIC is characterized by
Subacute bleeding Diffuse thrombosis.
Localized DIC is characterized by: Bleeding or thrombosis confined to a specific anatomic location e.g.
aortic aneurysmsgiant hemangiomashyperacute renal allograft rejection.

EpidemiologyEpidemiology
DIC may occur in 30-50% of DIC may occur in 30-50% of patients with sepsispatients with sepsis
In the US: 18,000 cases of DIC In the US: 18,000 cases of DIC occurred in 1994.occurred in 1994.
Sex: Incidence is equal in males and females. Age: No age predilection is known. Race: All races

HistoryHistory Symptoms related to the Symptoms related to the underlying diseaseunderlying disease
History of blood loss and hypovolemia e.g History of blood loss and hypovolemia e.g gastrointestinal bleeding.gastrointestinal bleeding.
Symptoms and signs of thrombosis in large
vessels eg DVT
Microvascular thrombosis eg renal failure.

Bleeding from at least 3 unrelated sites is particularly suggestive of DIC.
Epistaxis
Gingival bleeding
Mucosal bleeding
Cough
Dyspnea
Confusion, disorientation
Fever

Clinical ExaminationClinical Examination
CirculationCirculation Signs of spontaneous and Signs of spontaneous and
life-threatening hemorrhage. life-threatening hemorrhage.
Signs of subacute bleeding. Signs of subacute bleeding.
Signs of diffuse or localized Signs of diffuse or localized thrombosis.thrombosis.

1.1. Cardiovascular systemCardiovascular system Hypotension Hypotension Tachycardia Tachycardia Circulatory collapseCirculatory collapse
2. Central Nervous System2. Central Nervous System Nonspecific altered Nonspecific altered
consciousness/stupor consciousness/stupor Focal deficits not usually presentFocal deficits not usually present

3. Respiratory system3. Respiratory system Pleural friction rub Pleural friction rub Signs of adult respiratory distress Signs of adult respiratory distress
syndrome (ARDS)syndrome (ARDS)
4. Gastrointestinal system4. Gastrointestinal system HematemesisHematemesis HematocheziaHematochezia

5. Genitourinary system5. Genitourinary system Signs of azotemia and renal failure Signs of azotemia and renal failure Acidosis Acidosis Hematuria Hematuria Oliguria Oliguria Metrorrhagia Metrorrhagia Uterine hemorrhageUterine hemorrhage

6. Dermatologic system6. Dermatologic system Petechiae, PurpuraPetechiae, Purpura Hemorrhagic bullaeHemorrhagic bullae Acral cyanosisAcral cyanosis Skin necrosis of lower limbs Skin necrosis of lower limbs
(purpura fulminans)(purpura fulminans) Localized infarction and gangrene Localized infarction and gangrene Wound bleeding and deep Wound bleeding and deep
subcutaneous hematomas subcutaneous hematomas ThrombosisThrombosis

ETIOLOGYETIOLOGY
Causes of DIC can be classified as acute Causes of DIC can be classified as acute or chronic, systemic or localized. or chronic, systemic or localized.
DIC may be the result of a single or DIC may be the result of a single or multiple conditions. multiple conditions.

Acute DICAcute DIC
Infectious Infectious Bacterial (gram-negative sepsis, gram-Bacterial (gram-negative sepsis, gram-
positive infections, rickettsial) positive infections, rickettsial) Viral (HIV, cytomegalovirus, varicella, Viral (HIV, cytomegalovirus, varicella,
hepatitis)hepatitis) Fungal (histoplasma) Fungal (histoplasma) Parasitic (malaria)Parasitic (malaria)

Acute DICAcute DIC
Malignancy:Malignancy: Hematologic (acute myelocytic leukemias) Hematologic (acute myelocytic leukemias) Metastatic (mucin-secreting adenocarcinomas)Metastatic (mucin-secreting adenocarcinomas)
Obstetric Obstetric Placental abruption Placental abruption Amniotic fluid embolism Amniotic fluid embolism Acute fatty liver of pregnancy Acute fatty liver of pregnancy EclampsiaEclampsia

Trauma Trauma
Burns Burns
Motor vehicle accidents (MVAs) Motor vehicle accidents (MVAs)
Snake envenomation Snake envenomation
Hemolytic reactionsHemolytic reactions

Massive transfusionMassive transfusion
Liver disease - Acute hepatic failureLiver disease - Acute hepatic failure
Prosthetic devicesProsthetic devices
Shunts (Denver, LeVeen)Shunts (Denver, LeVeen)
Ventricular assist devicesVentricular assist devices

Chronic DICChronic DIC
Hematologic Hematologic Myeloproliferative syndromes Myeloproliferative syndromes Paroxysmal nocturnal hemoglobinuriaParoxysmal nocturnal hemoglobinuria
Vascular Vascular Rheumatoid arthritis Rheumatoid arthritis Raynaud diseaseRaynaud disease

Chronic DICChronic DIC
CardiovascularCardiovascular Myocardial infarctionMyocardial infarction
Inflammatory Inflammatory Ulcerative colitis Ulcerative colitis Crohn disease Crohn disease SarcoidosisSarcoidosis

Localized DICLocalized DIC
Aortic aneurysmsAortic aneurysms
Giant hemangiomas Giant hemangiomas (Kasabach-Merritt syndrome)(Kasabach-Merritt syndrome)
Acute renal allograft rejectionAcute renal allograft rejection
Hemolytic uremic syndromeHemolytic uremic syndrome

DIFFERENTIALSDIFFERENTIALS Hemolytic uremic syndromeHemolytic uremic syndrome Thrombocytopenic purpuraThrombocytopenic purpura
OOther Problems to be Consideredther Problems to be Considered: : Severe liver failure Severe liver failure Vitamin K deficiencyVitamin K deficiency HELLP syndrome (Hemolysis, elevated liver HELLP syndrome (Hemolysis, elevated liver
function, and low platelets)function, and low platelets) Primary fibrinolysisPrimary fibrinolysis Idiopathic purpura fulminansIdiopathic purpura fulminans

INVESTIGATIONSINVESTIGATIONS No single diagnostic test exists for DIC.No single diagnostic test exists for DIC.
DIC is initially suggested by the following DIC is initially suggested by the following
combination: combination: A clinical condition consistent with A clinical condition consistent with
DICthrombocytopenia (<100 X 10DICthrombocytopenia (<100 X 1099/L) /L) prolonged PT and aPTTprolonged PT and aPTT presence of FDP/ D-dimer. presence of FDP/ D-dimer.
Other tests also may help to exclude DIC.Other tests also may help to exclude DIC.

1.1. Lab Studies:Lab Studies:
Prothrombin fragment 1 and 2Prothrombin fragment 1 and 2
Enzyme-linked immunosorbent assay Enzyme-linked immunosorbent assay (ELISA) quantitates levels of prothrombin (ELISA) quantitates levels of prothrombin fragment (PF) 1 and 2 in the circulation. fragment (PF) 1 and 2 in the circulation.
This provides evidence of factor Xa This provides evidence of factor Xa generation and is easily performed. generation and is easily performed.
Levels are abnormal in 90% of patients Levels are abnormal in 90% of patients with DIC.with DIC.

D-DIMER TEST D-DIMER TEST
D-dimer is an antigen formed as a result of D-dimer is an antigen formed as a result of plasmin lysis of cross-linked fibrin clots.plasmin lysis of cross-linked fibrin clots.
The presence of this fragment documents The presence of this fragment documents
the presence of thrombin (cross-linking) the presence of thrombin (cross-linking) and plasmin (fibrinolysis).and plasmin (fibrinolysis).
This monoclonal antibody test has the This monoclonal antibody test has the greatest specificity and is a highly reliable greatest specificity and is a highly reliable test for diagnosis of DIC.test for diagnosis of DIC.

Antithrombin III levelAntithrombin III level
Functional antithrombin III levels decrease Functional antithrombin III levels decrease in DIC. in DIC.
This synthetic substrate assay is a reliable This synthetic substrate assay is a reliable and useful test for diagnosis and and useful test for diagnosis and therapeutic monitoring.therapeutic monitoring.

Fibrin and fibrinogen degradation Fibrin and fibrinogen degradation productsproducts Latex particle agglutination test is used to Latex particle agglutination test is used to
detect fibrinogen and fibrin degradation detect fibrinogen and fibrin degradation products (FDPs). products (FDPs).
Degradation products increase as plasmin Degradation products increase as plasmin biodegrades fibrinogen and fibrin. biodegrades fibrinogen and fibrin.
This test is not diagnostic of DIC, yet This test is not diagnostic of DIC, yet levels are elevated in 85-100% of patients.levels are elevated in 85-100% of patients.

Fibrinopeptide AFibrinopeptide A ELISA or radioimmunoassay is used to ELISA or radioimmunoassay is used to
measure fibrinopeptide A (FPA). measure fibrinopeptide A (FPA). FPA is a breakdown product of fibrinogen, FPA is a breakdown product of fibrinogen,
indicative of thrombin activity. indicative of thrombin activity. Levels are abnormal in 88% in DIC.Levels are abnormal in 88% in DIC.
Platelet countPlatelet count Platelet counts are invariably decreased.Platelet counts are invariably decreased. Functional deficits in platelets are often Functional deficits in platelets are often
present, and further studies are not present, and further studies are not indicated.indicated.

Fibrinogen Fibrinogen
Thrombin-time–based assay is used to Thrombin-time–based assay is used to measure fibrinogen levels. measure fibrinogen levels.
Levels usually are decreased in DIC.Levels usually are decreased in DIC.
Fibrinogen is an acute-phase reactant and Fibrinogen is an acute-phase reactant and
initially may be elevated secondary to the initially may be elevated secondary to the primary disease.primary disease.

Prothrombin timeProthrombin time
Prothrombin time (PT) tests the extrinsic Prothrombin time (PT) tests the extrinsic
and common pathways. and common pathways.
PT may be normal, prolonged, or PT may be normal, prolonged, or shortened in DIC.shortened in DIC.
It is generally an unreliable test for It is generally an unreliable test for diagnosis of DIC, and 50-75% of patients diagnosis of DIC, and 50-75% of patients have prolonged values.have prolonged values.

Activated Partial Thromboplastin Time (aPTT)Activated Partial Thromboplastin Time (aPTT)
aPTT tests the intrinsic and common aPTT tests the intrinsic and common
pathways.pathways.
Values are unpredictable in DIC.Values are unpredictable in DIC.
It is an unreliable test for diagnosis of DIC, It is an unreliable test for diagnosis of DIC,
and 50-60% of patients will have prolonged and 50-60% of patients will have prolonged valuesvalues

Thrombin timeThrombin time
Thrombin time measures the conversion of fibrinogen to Thrombin time measures the conversion of fibrinogen to fibrin. fibrin.
It should be prolonged in DIC.It should be prolonged in DIC.
Protamine testProtamine test It is a paracoagulation test that detects fibrin monomers in It is a paracoagulation test that detects fibrin monomers in
plasma.plasma.
Fibrin web formation indicates a positive result. It should be Fibrin web formation indicates a positive result. It should be positive in DIC.positive in DIC.

OTHER FINDINGS IN DICOTHER FINDINGS IN DIC Anemia Anemia Schizocytosis Schizocytosis Decreased coagulation factorsDecreased coagulation factors
Factor V Factor V Factor VIII Factor VIII Factor X Factor X Factor XIII Factor XIII Protein CProtein C
Hemoglobinuria Hemoglobinuria Hematuria Hematuria Hematochezia Hematochezia

IMAGING STUDIES: IMAGING STUDIES:
Base diagnostic imaging on the underlying Base diagnostic imaging on the underlying pathologic process as well as suspicion for pathologic process as well as suspicion for areas of thrombosis and hemorrhage.areas of thrombosis and hemorrhage.
Perform a bilateral perihilar soft-density Perform a bilateral perihilar soft-density chest radiograph if pulmonary injury is chest radiograph if pulmonary injury is present.present.

OTHER TESTSOTHER TESTS
Base other tests on the underlying Base other tests on the underlying pathologic process as well as suspicion for pathologic process as well as suspicion for areas of thrombosis and hemorrhage.areas of thrombosis and hemorrhage.

PROCEDURESPROCEDURES Base procedures on the underlying Base procedures on the underlying
pathologic process as well as suspicion for pathologic process as well as suspicion for areas of thrombosis and hemorrhage.areas of thrombosis and hemorrhage.
Conduct invasive procedures with care Conduct invasive procedures with care because of bleeding complicationsbecause of bleeding complications
Procedures should follow the administration Procedures should follow the administration of clotting factor and platelet repletion.of clotting factor and platelet repletion.

DIAGNOSTIC ALGORITHM OF OVERT DIAGNOSTIC ALGORITHM OF OVERT DICDIC
1. Risk assessment: Does the patient have a underlying disorder known to be associated with overt DIC?
If yes: proceed
If no: do not use this algorithm
2. Order global coagulation tests (platelet count, prothrombin time (PT), fibrinogen, soluble fibrin monomers or fibrin degradation products)

3. Score global coagulation test results
platelet count (>100 = 0; <100 = 1; <50= 2)
Elevated fibrin-related marker (e.g. soluble fibrin monomers/fibrin degradation products)
(no increase: 0; moderate increase: 2; strong increase: 3)
prolonged prothrombin time
(< 3 sec.= 0; > 3 sec. but < 6 sec.= 1; > 6 sec. = 2)
fibrinogen level
(> 1.0 gram/l = 0; < 1.0 gram/l = 1)

4. Calculate score
5. If > 5: compatible with overt DIC; repeat
scoring daily
If < 5: suggestive (not affirmative) for non-overt
DIC; repeat next 1-2 days;

PREHOSPITAL CAREPREHOSPITAL CARE
Monitor vital signs.Monitor vital signs. Assess and document extent of Assess and document extent of
hemorrhage and thrombosis.hemorrhage and thrombosis. Correct hypovolemia.Correct hypovolemia. Administer basic hemostatic procedures Administer basic hemostatic procedures
when indicated.when indicated.

EMERGENCY DEPARTMENT CAREEMERGENCY DEPARTMENT CARE
The cornerstone of DIC management is The cornerstone of DIC management is treatment of the underlying disorder. treatment of the underlying disorder.

The following supportive measures are The following supportive measures are essential: essential: Continue prehospital measures.Continue prehospital measures. Attend to life-threatening issues such as Attend to life-threatening issues such as
airway compromise or severe hemorrhage.airway compromise or severe hemorrhage. Determine the underlying cause of the Determine the underlying cause of the
patient's DIC and initiate therapy.patient's DIC and initiate therapy. Obtain appropriate imaging studies if Obtain appropriate imaging studies if
necessary.necessary.

Draw specimens for appropriate Draw specimens for appropriate coagulation studies and other diagnostic coagulation studies and other diagnostic laboratory tests. laboratory tests.
Begin anticoagulant therapy if indicatedBegin anticoagulant therapy if indicated

Replace blood productsReplace blood products
RBC transfusion [PRBCs]RBC transfusion [PRBCs] Platelet concentrates Platelet concentrates Fresh frozen plasma (FFP) Fresh frozen plasma (FFP) CryoprecipitateCryoprecipitate Antithrombin III concentrateAntithrombin III concentrate

CONSULTATIONSCONSULTATIONS
Consult a hematologist for assistance with Consult a hematologist for assistance with diagnosis and management.diagnosis and management.
Consult a transfusion specialist to Consult a transfusion specialist to determine the availability of blood productsdetermine the availability of blood products

Consult a critical care specialist if multiple Consult a critical care specialist if multiple organ failure is present.organ failure is present.
Obtain other subspecialty consultations Obtain other subspecialty consultations as indicated by the patient's primary as indicated by the patient's primary diagnosis.diagnosis.

HEPARINHEPARIN
Use and dose of heparin is based on Use and dose of heparin is based on severity of DIC, underlying cause, and severity of DIC, underlying cause, and extent of thrombosis. extent of thrombosis.
Monitoring results of therapy is Monitoring results of therapy is mandatory. mandatory.
Heparin augments antithrombin III Heparin augments antithrombin III activity and prevents conversion of activity and prevents conversion of fibrinogen to fibrin. fibrinogen to fibrin.

HEPARINHEPARIN
Does not actively lyse but inhibits Does not actively lyse but inhibits further thrombogenesis. further thrombogenesis.
Prevents reaccumulation of a clot afterPrevents reaccumulation of a clot after spontaneous fibrinolysis. spontaneous fibrinolysis.

Adult DoseAdult Dose 80-100 U/kg SC q4-6h or 20,000-30,000 U/d IV 80-100 U/kg SC q4-6h or 20,000-30,000 U/d IV
continuous infusion continuous infusion
ContraindicationsContraindications HypersensitivityHypersensitivity Bacterial endocarditisBacterial endocarditis Active bleedingActive bleeding History of heparin-induced thrombocytopenia History of heparin-induced thrombocytopenia

Interactions Interactions Digoxin, nicotine, tetracycline, and Digoxin, nicotine, tetracycline, and
antihistamines may decrease effectsantihistamines may decrease effects NSAIDs, aspirin, dextran, dipyridamole, NSAIDs, aspirin, dextran, dipyridamole,
and hydroxychloroquine may increase and hydroxychloroquine may increase toxicity toxicity
PregnancyPregnancy C - Safety not established. C - Safety not established.

PRECAUTIONSPRECAUTIONS
Monitor for bleeding tendencyMonitor for bleeding tendency In neonates, preservative-free heparin is In neonates, preservative-free heparin is
recommended to avoid possible toxicity recommended to avoid possible toxicity (gasping syndrome) by benzyl alcohol, (gasping syndrome) by benzyl alcohol, which is used as preservative;which is used as preservative;
Caution in severe hypotension and shockCaution in severe hypotension and shock

ANTITHROMBIN III (THROMBATE III)ANTITHROMBIN III (THROMBATE III)
Use for moderately severe to severe DICUse for moderately severe to severe DIC It inactivates thrombin, plasmin, and other It inactivates thrombin, plasmin, and other
serine proteases of coagulation, including serine proteases of coagulation, including factors IXa, Xa, XIa, XIIa, and VIIa.factors IXa, Xa, XIa, XIIa, and VIIa.
These effects inhibit coagulation. These effects inhibit coagulation.

Total units=Total units= (desired level - initial level) (0.6 X total body weight kg) IV (desired level - initial level) (0.6 X total body weight kg) IV
q8h with a desired level >125% q8h with a desired level >125% loading dose of 100 U/kg IV over 3 h; followed by loading dose of 100 U/kg IV over 3 h; followed by
continuous infusion of 100 U/kg/d continuous infusion of 100 U/kg/d ContraindicationsContraindications
Documented hypersensitivityDocumented hypersensitivity
InteractionsInteractions
Increases anticoagulation effects of heparin Increases anticoagulation effects of heparin

Pregnancy:Pregnancy: C – Safety not established. C – Safety not established.
PrecautionsPrecautions Caution in hypotensionCaution in hypotension potentially still can transmit disease potentially still can transmit disease contain unknown infectious agentscontain unknown infectious agents

DROTRECOGIN ALFA-ACTIVATED DROTRECOGIN ALFA-ACTIVATED (XIGRIS)(XIGRIS)
Indicated for reduction of mortality in Indicated for reduction of mortality in severe sepsis associated with acute organ severe sepsis associated with acute organ dysfunction and at high risk of death. dysfunction and at high risk of death.
Recombinant form of human activated Recombinant form of human activated protein C that exerts antithrombotic effect protein C that exerts antithrombotic effect by inhibiting factors Va and VIIIa. by inhibiting factors Va and VIIIa.

Has indirect profibrinolytic activity by inhibiting Has indirect profibrinolytic activity by inhibiting PAI-1 and limiting formation of activated PAI-1 and limiting formation of activated thrombin-activatable-fibrinolysis-inhibitor. thrombin-activatable-fibrinolysis-inhibitor.
May exert anti-inflammatory effect by inhibiting May exert anti-inflammatory effect by inhibiting TNF production by monocytes, blocking TNF production by monocytes, blocking leukocyte adhesion to selectins, and limiting leukocyte adhesion to selectins, and limiting thrombin-induced inflammatory responses within thrombin-induced inflammatory responses within microvascular endothelium. microvascular endothelium.

Adult DoseAdult Dose 24 mcg/kg/h IV by cont infusion over 96 h 24 mcg/kg/h IV by cont infusion over 96 h
ContraindicationsContraindications Documented hypersensitivityDocumented hypersensitivity increased risk of bleedingincreased risk of bleeding

InteractionsInteractions None reportedNone reported Coadministration with drugs that affect Coadministration with drugs that affect
hemostasis may increase risk of bleeding (eg, hemostasis may increase risk of bleeding (eg, warfarin, heparin, thrombolytics, glycoprotein warfarin, heparin, thrombolytics, glycoprotein IIb/IIIa inhibitors) IIb/IIIa inhibitors)
PregnancyPregnancy C - Safety not established. C - Safety not established.

PRECAUTIONSPRECAUTIONS caution with conditions that increase risk of caution with conditions that increase risk of
bleedingbleeding known bleeding diathesis known bleeding diathesis chronic severe hepatic disease chronic severe hepatic disease stop infusion if clinically significant bleeding stop infusion if clinically significant bleeding
occurs occurs caution with thrombocytopenia (<50 X 10caution with thrombocytopenia (<50 X 1099/L) /L) chronic severe hepatic diseasechronic severe hepatic disease

PRBCsPRBCs
Preferred to whole blood since they limit volume, Preferred to whole blood since they limit volume, immune, and storage complications. immune, and storage complications.
Adult DoseAdult Dose 1 unit of PRBCs should raise hemoglobin by 1 g/dL or 1 unit of PRBCs should raise hemoglobin by 1 g/dL or
raise hematocrit by 3% raise hematocrit by 3%

ContraindicationsContraindications Competent adult or legal guardian may refuse blood Competent adult or legal guardian may refuse blood
product; immediate consultation with hospital ethical product; immediate consultation with hospital ethical and legal staff is mandated and legal staff is mandated
InteractionsInteractions None reported None reported
PregnancyPregnancy SafeSafe

PRECAUTIONSPRECAUTIONS
Use CMV-negative units or filtered onesUse CMV-negative units or filtered ones
Transfusion reactions and transmission of Transfusion reactions and transmission of blood-borne pathogens are a concernblood-borne pathogens are a concern
Benefits should outweigh risks associated Benefits should outweigh risks associated with such productswith such products

PLATELET CONCENTRATESPLATELET CONCENTRATES
Adult DoseAdult Dose
Based on platelet count and clinical Based on platelet count and clinical situationsituation

ContraindicationsContraindications
Competent adult may refuse blood product Competent adult may refuse blood product
immediate consultation with hospital ethical immediate consultation with hospital ethical and legal staff mandated and legal staff mandated
InteractionsInteractions None reported None reported

PregnancyPregnancy SafeSafe
PrecautionsPrecautions Platelets should be CMV-negative Platelets should be CMV-negative Benefits should outweigh risks associated Benefits should outweigh risks associated
with such productswith such products

FRESH FROZEN PLASMA (FFP)FRESH FROZEN PLASMA (FFP)
This treatment entails removing blood from This treatment entails removing blood from body, spinning it to separate cells from plasma, body, spinning it to separate cells from plasma, and replacing cells suspended in fresh frozen and replacing cells suspended in fresh frozen plasma, albumin, or saline. plasma, albumin, or saline.
Contains coagulation factors as well as protein C Contains coagulation factors as well as protein C and protein S. and protein S.
Recommended with active bleeding and Recommended with active bleeding and fibrinogen <100 mg/dL. fibrinogen <100 mg/dL.

Adult DoseAdult Dose 15-20 mL/kg IV or based on clinical situation 15-20 mL/kg IV or based on clinical situation
ContraindicationsContraindications hypersensitivity hypersensitivity
InteractionsInteractions None reported None reported
PregnancyPregnancy Safe Safe
PrecautionsPrecautions Viral contamination and infection are remotely Viral contamination and infection are remotely
possible but unlikelypossible but unlikely

CRYOPRECIPITATE CRYOPRECIPITATE
Not commonly recommended except when Not commonly recommended except when fibrinogen is needed. fibrinogen is needed.
Adult DoseAdult Dose Each bag contains 80-100 U of factor VIII; Each bag contains 80-100 U of factor VIII; Base administration on fibrinogen levels, Base administration on fibrinogen levels, Antithrombin III levels, Antithrombin III levels, coagulation parameters coagulation parameters

ContraindicationsContraindications Documented hypersensitivity; Documented hypersensitivity; uncontrolled DIC with abnormal antithrombin uncontrolled DIC with abnormal antithrombin
III levelsIII levels InteractionsInteractions
None reportedNone reported

PregnancyPregnancy SafeSafe
PrecautionsPrecautions Viral contamination and infection are Viral contamination and infection are
remotely possible although unlikely because remotely possible although unlikely because of prescreeningof prescreening

AMINOCAPROIC ACID (AMICAR)AMINOCAPROIC ACID (AMICAR)
Inhibits fibrinolysis via inhibition of plasminogen Inhibits fibrinolysis via inhibition of plasminogen activator substances and, to a lesser degree, activator substances and, to a lesser degree, through antiplasmin activity.through antiplasmin activity.
Main problem is that thrombi that form during Main problem is that thrombi that form during treatment are not lysed, and clinical significance treatment are not lysed, and clinical significance of reducing bleeding is uncertain. of reducing bleeding is uncertain.
Adult DoseAdult Dose Load 5-10 g IV slowly; followed by 2-4 g/h IV; Load 5-10 g IV slowly; followed by 2-4 g/h IV;
not to exceed 30 g/d not to exceed 30 g/d

ContraindicationsContraindications Documented hypersensitivity.Documented hypersensitivity. Evidence of active intravascular clotting process.Evidence of active intravascular clotting process. Important to differentiate between hyperfibrinolysis Important to differentiate between hyperfibrinolysis
and DIC and DIC
InteractionsInteractions Estrogens may cause increase in clotting factors, Estrogens may cause increase in clotting factors,
leading to hypercoagulable stateleading to hypercoagulable state

PregnancyPregnancy
Safety not established. Safety not established.
PrecautionsPrecautions
Do not administer unless definite diagnosis of Do not administer unless definite diagnosis of hyperfibrinolysis has been made hyperfibrinolysis has been made
Caution in cardiac, hepatic, or renal diseaseCaution in cardiac, hepatic, or renal disease

TRANEXAMIC ACIDTRANEXAMIC ACID
Used as alternative to aminocaproic acid. Used as alternative to aminocaproic acid. Inhibits fibrinolysis by displacing Inhibits fibrinolysis by displacing
plasminogen from fibrin. plasminogen from fibrin. Adult DoseAdult Dose
Nonstandardized dosing: 25 mg/kg PO tid/qid; Nonstandardized dosing: 25 mg/kg PO tid/qid; 1-2 g IV q8-12h 1-2 g IV q8-12h

ContraindicationsContraindications Hypersensitivity; ongoing DIC and CNS involvement Hypersensitivity; ongoing DIC and CNS involvement
InteractionsInteractions None reportedNone reported
PregnancyPregnancy Safe Safe
PrecautionsPrecautions: : Adverse effects include gastrointestinal and visual Adverse effects include gastrointestinal and visual
disturbances and hypotension; caution in renal impairmentdisturbances and hypotension; caution in renal impairment

Most patients with acute DIC require critical care Most patients with acute DIC require critical care treatment appropriate for the primary diagnosis, treatment appropriate for the primary diagnosis, occasionally including emergent surgery.occasionally including emergent surgery.
Assessment of severity of DIC (DIC score)Assessment of severity of DIC (DIC score)
Clinical and laboratory parameters are Clinical and laboratory parameters are measured with regularity (every 8 h).measured with regularity (every 8 h).

OUTPATIENT CAREOUTPATIENT CARE
Patients who recover from acute DIC Patients who recover from acute DIC should follow up with their primary should follow up with their primary physician or a hematologist.physician or a hematologist.
Patients with low-grade or chronic DIC Patients with low-grade or chronic DIC may be treated by a hematologist on an may be treated by a hematologist on an outpatient basis after initial assessment outpatient basis after initial assessment and stabilization.and stabilization.

Outpatient medications may include antiplatelet Outpatient medications may include antiplatelet agents for those with low-grade DIC agents for those with low-grade DIC
Antibiotics appropriate to the primary diagnosis.Antibiotics appropriate to the primary diagnosis.
Patients who are stable enough for transfer Patients who are stable enough for transfer should be referred expeditiously to centers with should be referred expeditiously to centers with appropriate critical care and subspecialty appropriate critical care and subspecialty expertise, such as hematology, blood bank, or expertise, such as hematology, blood bank, or surgical centers.surgical centers.

COMPLICATIONSCOMPLICATIONS Acute renal failureAcute renal failure Life-threatening thrombosis and hemorrhage Life-threatening thrombosis and hemorrhage Cardiac tamponadeCardiac tamponade HemothoraxHemothorax Intracerebral hematomaIntracerebral hematoma Gangrene and loss of digitsGangrene and loss of digits DeathDeath

PROGNOSISPROGNOSIS
The prognosis is influenced most by the The prognosis is influenced most by the underlying condition that led to DIC underlying condition that led to DIC
The severity of the DIC.The severity of the DIC. Major Trama with DIC __double the mortalityMajor Trama with DIC __double the mortality Septic abortion with clostridial infection __ Septic abortion with clostridial infection __
50% mortality50% mortality