Dr Heelen M. Oudemans-van Straaten Department of … · He induced an acute phase reaction and...
27
CRRT IN SEPSIS, DOES THE ANTICOGULANT MATTER? Heleen M. Oudemans-van Straaten, Amsterdam, Netherlands Chair: Norbert Lameire, Ghent, Belgium Mehmet Sukru Sever, Istanbul, Turkey Dr Heelen M. Oudemans-van Straaten Department of Intensive Care Medicine O nze Lieve V rouwe Gasthuis A msterdam, The Netherlands Slide 1 Good morning, thank you for this nice invitation to have this talk here. I’m a critical care specialist, I’m not a nephrologist but I have however my interests. Chairman: We will not hold that against you! Ok! Slide 2
Transcript of Dr Heelen M. Oudemans-van Straaten Department of … · He induced an acute phase reaction and...

CRRT IN SEPSIS, DOES THE ANTICOGULANT MATTER?
Heleen M. Oudemans-van Straaten, Amsterdam, Netherlands
Chair: Norbert Lameire, Ghent, Belgium
Mehmet Sukru Sever, Istanbul, Turkey
Dr Heelen M. Oudemans-van StraatenDepartment of Intens ive C are Medic ine
O nze Lieve V rouwe Gas thuis
A msterdam, The Netherlands
Slide 1
Good morning, thank you for this nice invitation to have this talk here. I’m a critical care specialist, I’m not anephrologist but I have however my interests.
Chairman: We will not hold that against you!
Ok!
Slide 2

Well, sepsis is a state of hypercoagulability and bleeding tendency at the same time.
Slide 3
Heparin is the first choice anticoagulant for CRRT in most units. However, in patients with sepsis heparin may beproblematic.
Slide 4
Heparin causes anticoagulation by binding to antithrombin and antithrombin is the most potent endogenousanticoagulant in the body preventing the formation of thrombin.
Slide 5
Heparin prevents thrombin formation and by this it may have anti-inflammatory properties because thrombin doesnot only activate coagulation but also inflammation.
Slide 6

However, there are many other problems or there are many problems with heparin in sepsis. First is heparinresistance. There may be heparin resistance because antithrombin is low not only because of increased consumptionbut also because of increased inactivation.
Slide 7
How do we explain this? In sepsis there is an increased formation of elastase from activated polymorphonuclearleucocytes but in addition there is a reduced activity of its natural inactivator α1-antitrypsin and this is so becauseoxygen radicals inactivate α1-antitryopsin.
Slide 8
Furthermore, apart from binding to circulating antithrombin, heparin binds to endothelial anti-thrombin, acute phaseproteins and to necrotic and apoptotic cells. In contrast to its binding to the circulating antithrombin the other bindings lead to inactivation of the heparin but alsoof the processes of binding.
Slide 9
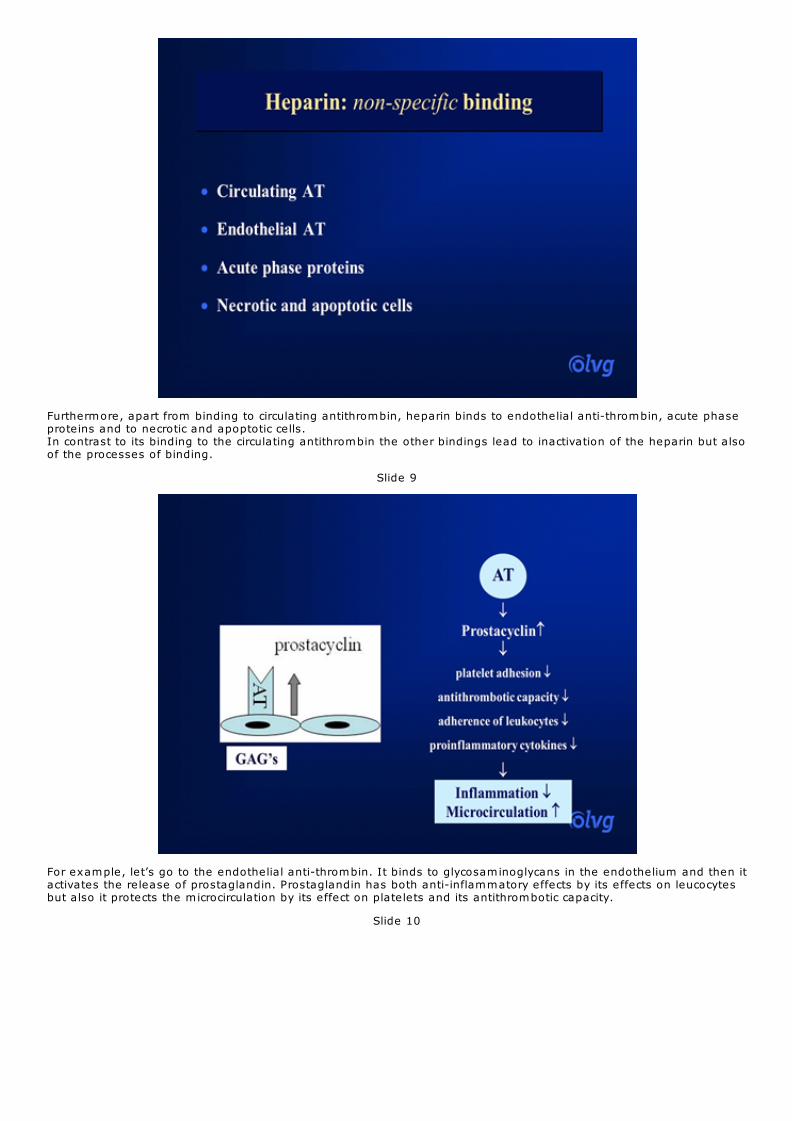
For example, let’s go to the endothelial anti-thrombin. It binds to glycosaminoglycans in the endothelium and then itactivates the release of prostaglandin. Prostaglandin has both anti-inflammatory effects by its effects on leucocytesbut also it protects the microcirculation by its effect on platelets and its antithrombotic capacity.
Slide 10
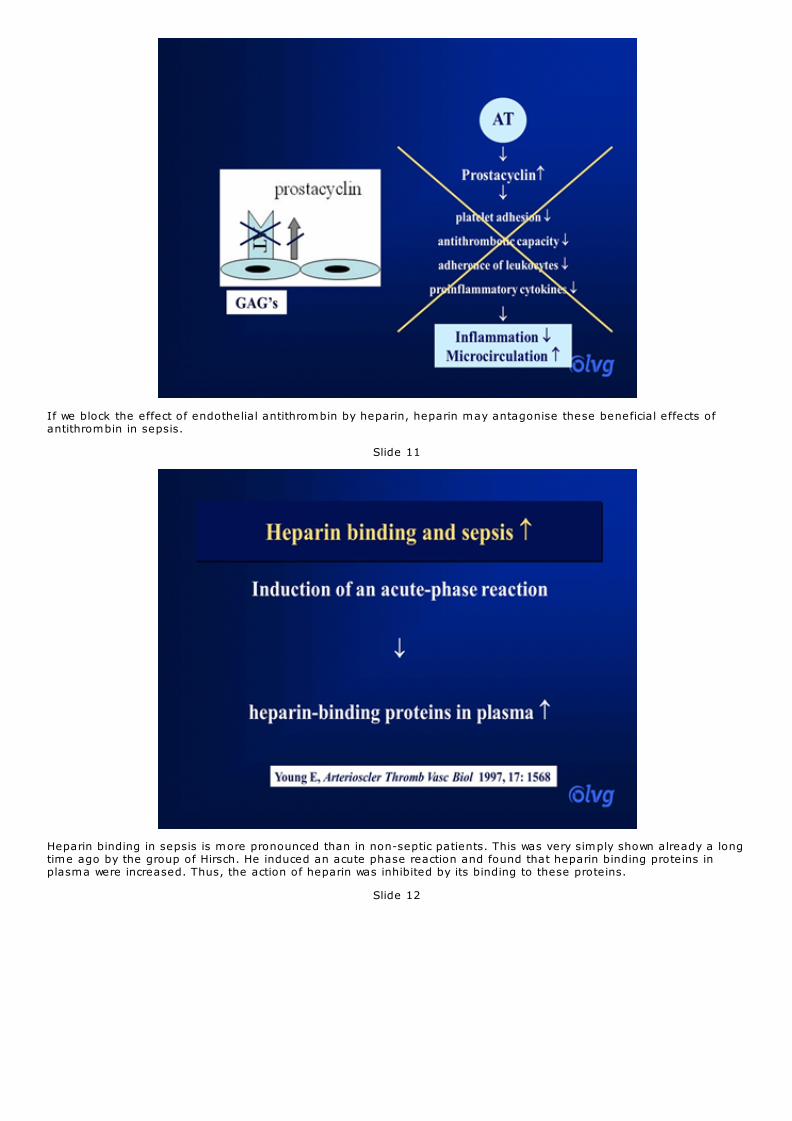
If we block the effect of endothelial antithrombin by heparin, heparin may antagonise these beneficial effects ofantithrombin in sepsis.
Slide 11
Heparin binding in sepsis is more pronounced than in non-septic patients. This was very simply shown already a longtime ago by the group of Hirsch. He induced an acute phase reaction and found that heparin binding proteins inplasma were increased. Thus, the action of heparin was inhibited by its binding to these proteins.
Slide 12

Well, this is very important information I think that heparin also binds to necrotic and apoptotic cells.
Slide 13
These necrotic and apoptotic cells release certain domains from the nucleus to the membrane and these domainssignal phagocytosis.
Slide 14

Heparin binds to these domains
Slide 15
and by binding of heparin phagocytosis is inhibited.
Slide 16

Thus, the binding of heparin to necrotic and apoptotic cells may delay the phagocytosis of these cells and this isimportant in patients with sepsis and multiple organ failure.
Slide 17
Next heparins may contribute to bioincompatibility. During hemodialysis that’s what you all know leucocytes aretrapped in the membrane and activated and they release their granular products from their granules and this processmay be enhanced by heparin.
Slide 18

This was first shown or this was shown by the group of Leitienne and he compared low molecular heparin andunfractionated heparin in a high and in a low dose and found that a release of elastase was increased in a dose-dependent way. So the high dose heparin had a higher release than the low dose heparin.
Slide 19
Sepsis and heparin,
Slide 20

let’s go on because this process is more important in sepsis because in sepsis PMNLs degranulate endothelialsurfaces and they release myeloperoxidase. This is locally bound to the glycosaminoglycans and causes vascularinjury; it’s one of the mechanisms.
Slide 21
If we infuse exogenous heparins, they bind to the heparin binding molecules and release myeloperoxidase which isreleased into the circulation and may augment inflammation.
Slide 22
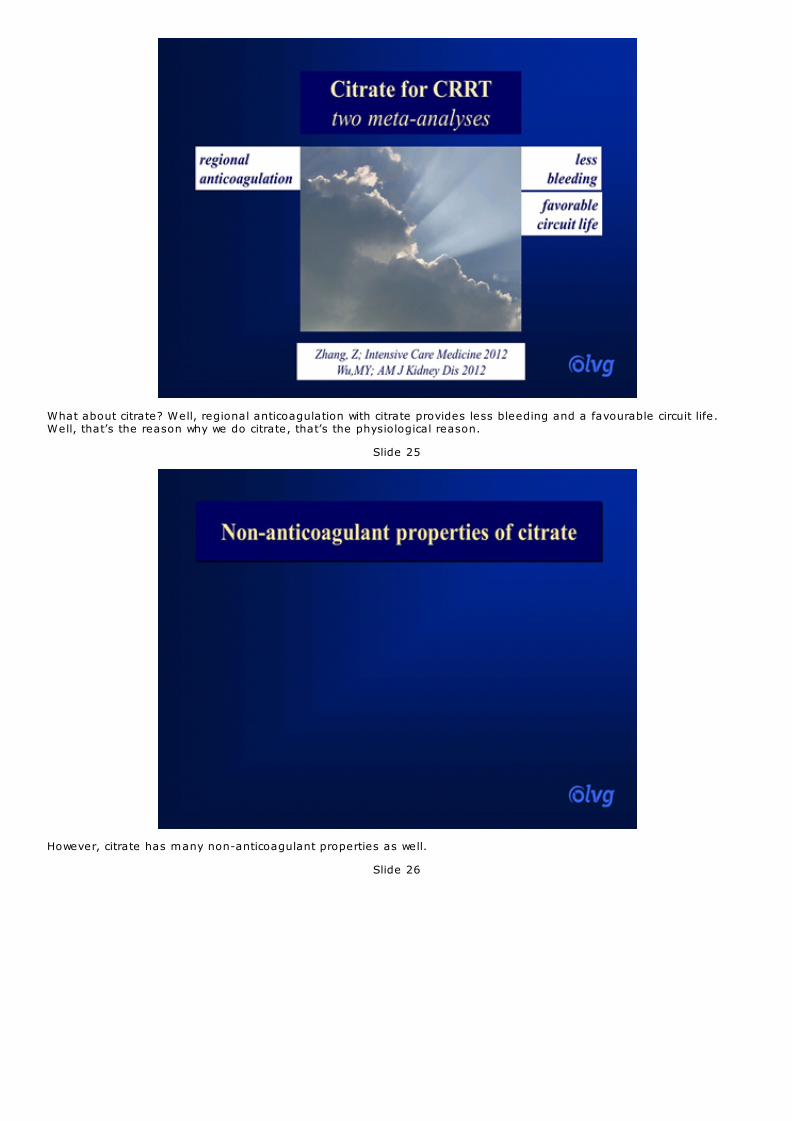
This is a factor shown by a Dutch group and they measured platelet factor 4 in chronic dialysis patients just beforeconnecting this circuit and before giving the heparin, after heparin administration at the entrance and outlet of thecircuit. They found a massive release of platelet factor 4, one of the heparin binding molecules already after theinfusion of heparin before connection of the circuit.
Slide 23
So this platelet factor 4 must have come from the patient and not from the circuit.
Slide 24
What about citrate? Well, regional anticoagulation with citrate provides less bleeding and a favourable circuit life.Well, that’s the reason why we do citrate, that’s the physiological reason.
Slide 25
However, citrate has many non-anticoagulant properties as well.
Slide 26

Citrate may in contrast to heparin improve biocompatibility.
Slide 27
This was already shown a long time ago when comparing heparin to citrate anticoagulation using a biocompatiblemembrane. The group shows that release of elastase and lactoferrin was mitigated when using citrate. Complementactivation was not influenced.
Slide 28

The results with these released products were repeated by many other investigators
Slide 29
and I want to mention this to my opinion very interesting hypothesis generating study, an E. coli peritonitis model inpigs. The authors used a selective cytopheretic device which was put into the hemofiltration circuit and the idea isthat this device binds activated leucocytes and they compared heparin to citrate anticoagulation.
Slide 30

The thing they found is that when using citrate there was less systemic neutrophil activation and less release ofmyeloperoxidase, cytokines were not different but they found also less hemodynamic instability, less lungsequestration of leukocytes, less renal dysfunction and a better survival. These are pigs but this is important I think.
Slide 31
This is a study from the same group of the Netherlands and these were measurements within the circuit and theyshowed that citrate does not only abolish release or degranulation from leukocytes but also from platelets comparedto heparin and unfractionated heparin.
Slide 32
They also saw after the two sessions that there was a low concentration of oxidized LDL, lower oxidative stressindicating or suggesting that this may be clinically relevant.
Slide 33
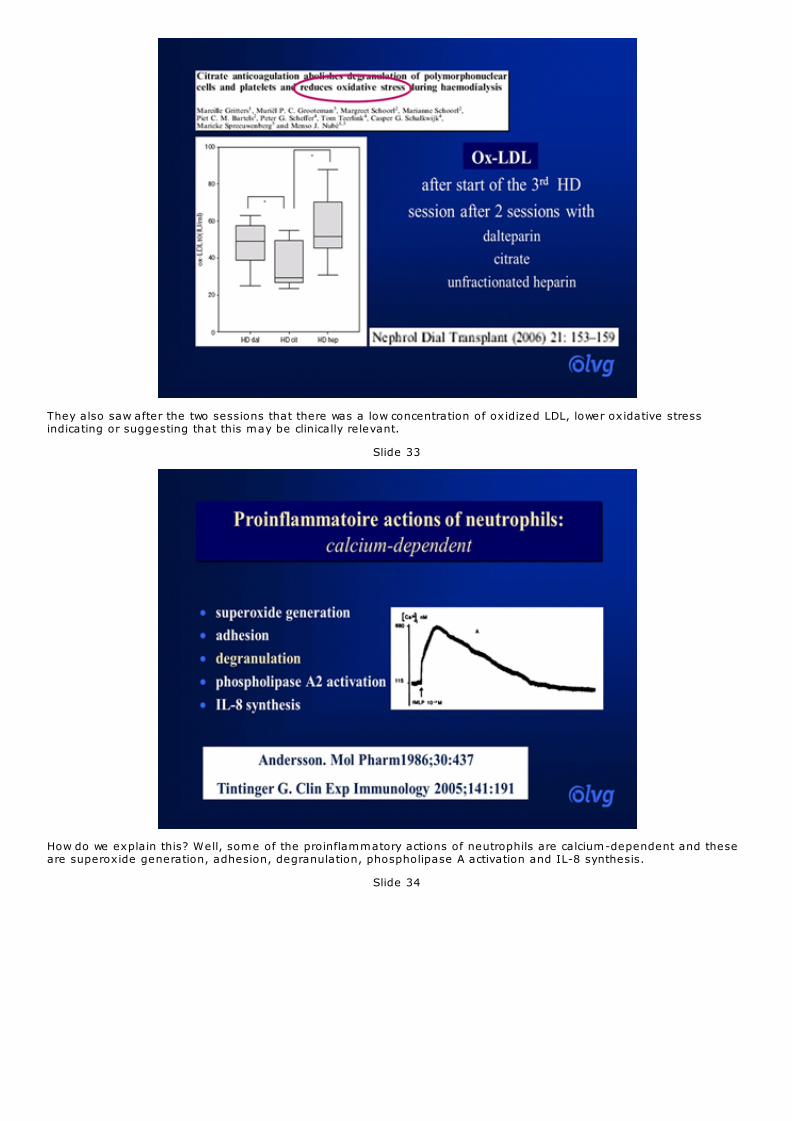
How do we explain this? Well, some of the proinflammatory actions of neutrophils are calcium-dependent and theseare superoxide generation, adhesion, degranulation, phospholipase A activation and IL-8 synthesis.
Slide 34

Citrate creates a hypocalcaemia at the membrane
Slide 35
and this hypocalcaemia may influence intracellular calcium signalling.
Slide 36
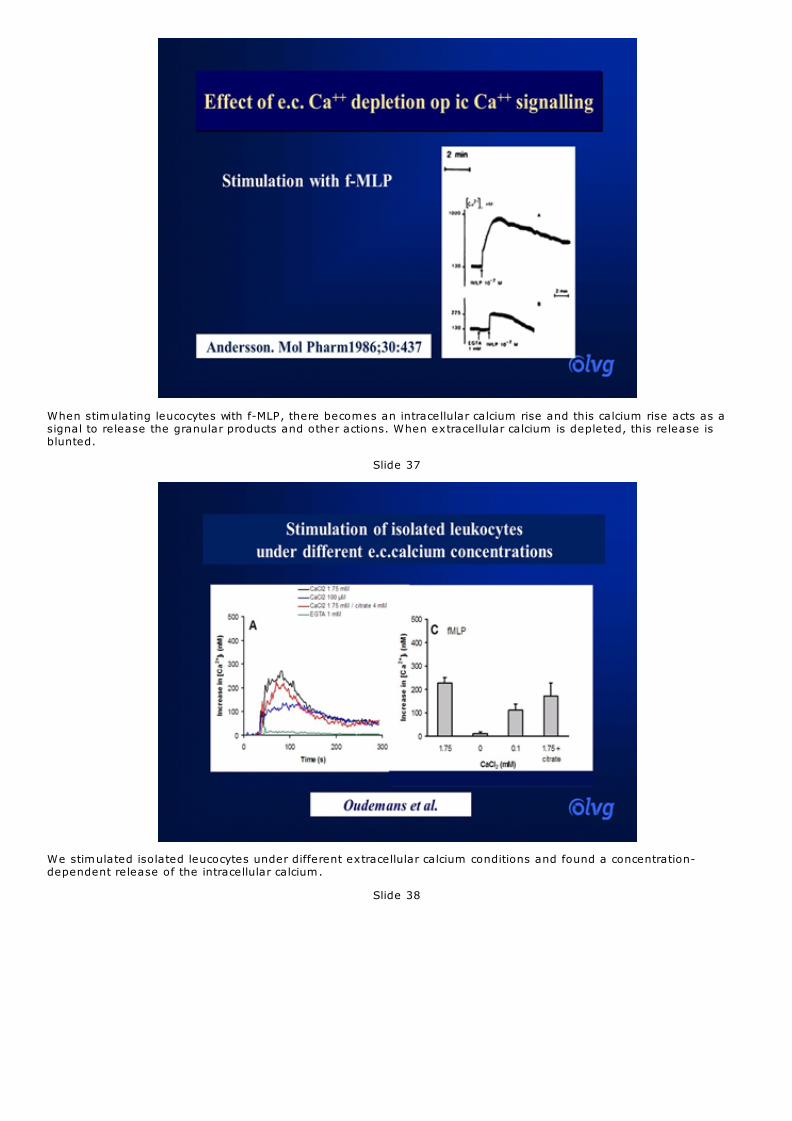
When stimulating leucocytes with f-MLP, there becomes an intracellular calcium rise and this calcium rise acts as asignal to release the granular products and other actions. When extracellular calcium is depleted, this release isblunted.
Slide 37
We stimulated isolated leucocytes under different extracellular calcium conditions and found a concentration-dependent release of the intracellular calcium.
Slide 38

Well, this was already found in the year 2000 by the group of our Chair session and they used unmodified cellulosemembranes at this time and during hemodialysis and they measured activation of leucocytes by the CD11b andCD11c receptor.
Slide 39
They found that there was a significant correlation between the decrease in ionized calcium and the expression of themembrane receptor. So they also found that the degree of hypocalcaemia was important.
Slide 40

Other aspects of citrate are that citrate is fuel and no insulin is needed.
Slide 41
Citrate fuels the citric acid cycle which has a very central position in metabolism. In energy metabolism it connectsglycolysis, cytoplasmatic glycolysis to the oxidative phosphorylation which is the main energy producing machine inour body.
Slide 42

Flux of this cycle depends on oxygen consumption, higher needs when oxygen consumption is high, need forintermediates and maybe limited by substrate availability.
Slide 43
Citrate may be an anaplerotic substance providing a shortness of intermediates when needs are high for energy orother intermediates.
Slide 44
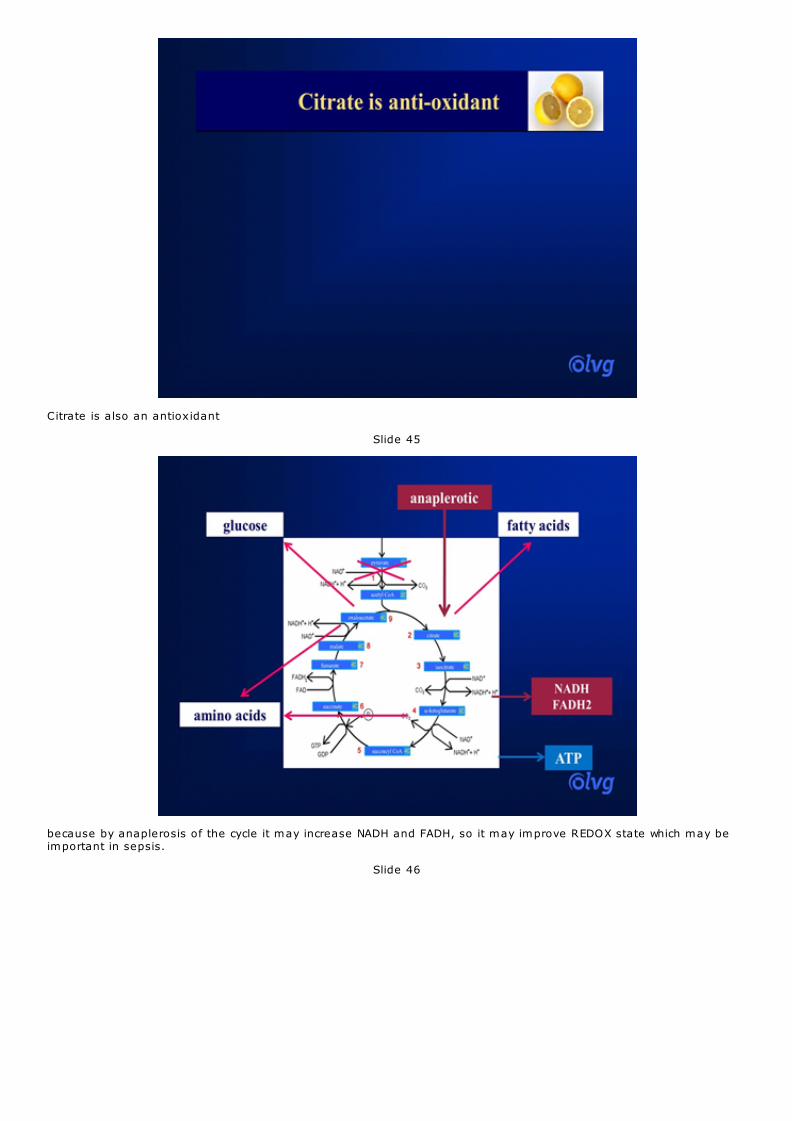
Citrate is also an antioxidant
Slide 45
because by anaplerosis of the cycle it may increase NADH and FADH, so it may improve REDOX state which may beimportant in sepsis.
Slide 46
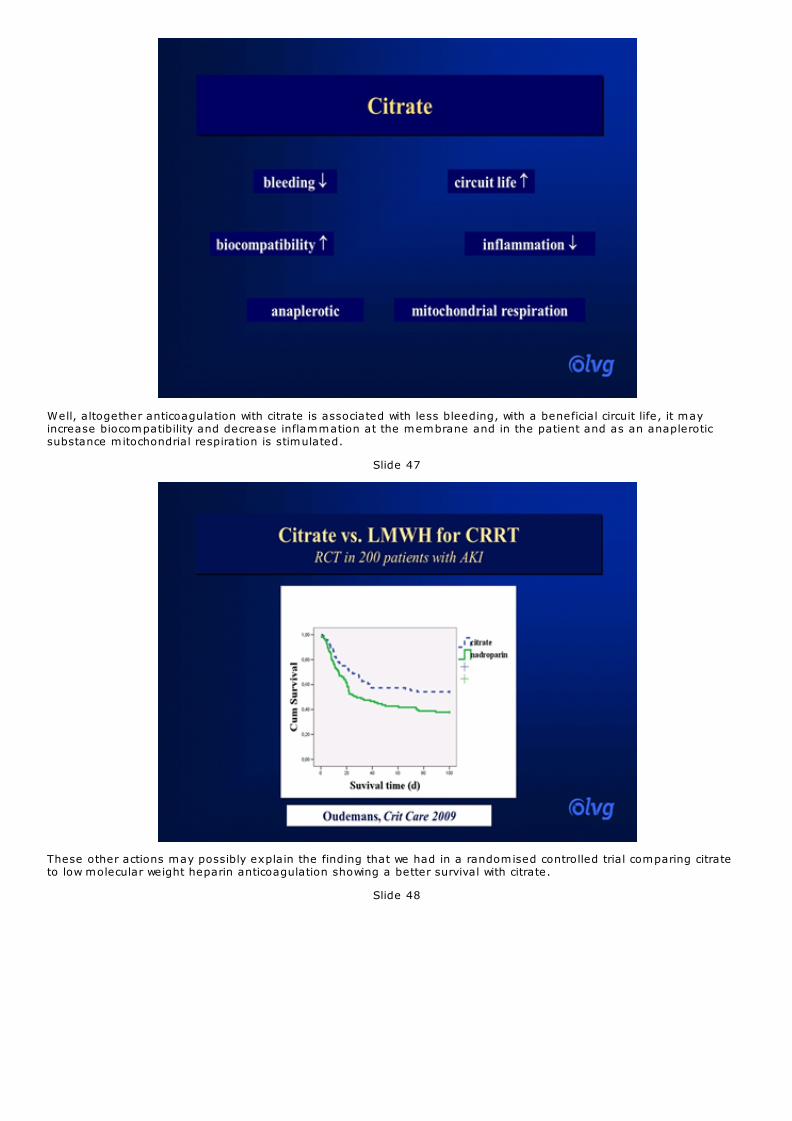
Well, altogether anticoagulation with citrate is associated with less bleeding, with a beneficial circuit life, it mayincrease biocompatibility and decrease inflammation at the membrane and in the patient and as an anapleroticsubstance mitochondrial respiration is stimulated.
Slide 47
These other actions may possibly explain the finding that we had in a randomised controlled trial comparing citrateto low molecular weight heparin anticoagulation showing a better survival with citrate.
Slide 48

Citrate didn’t worsen any of the subgroups but this survival was especially seen in the patients with sepsis
Slide 49
and in those with higher than mean organ failure score.
Slide 50

This may be possibly because we didn’t use the high dose of heparin and could prevent the binding of heparin toendothelial antithrombin, the release of inflammatory mediators and the delay of the clearance apoptotic andnecrotic cells
Slide 51
or it could also be a benefit of the citrate reducing inflammation and improving mitochondrial bioenergetics.
Slide 52

So the answer to the question whether the anticoagulant matters, I think it does and citrate may become the firstchoice in patients with sepsis provided that its safe use can be guaranteed. Thank you.