Presented by: MEHAK ZAIB SUDDLE FAIZA IRFAN AYESHA SHAHEEN NARGIS JAHANGIR.

Mind the Gap: A review of child & adolescent deliberate self-harm admissions to University
College London Hospital (UCLH)
Dr Golnar Aref-Adib, Esha Abrol, Arisa Harada, Dr Zaib Davids

Contents
• Background
• Aims
• Method
• Results
• Conclusions
• Recommendations

Self-harm and suicide in the UK
• 1 in 10 young people self-harm at some point
• 2nd most common cause of death in young people worldwide
• Hospital admissions = small proportion of those who self-harm

Common Assessment Framework (CAF)
“A framework to help practitioners working with
children, young people and families to assess children
and young people’s additional needs for earlier, and
more effective services, and develop a common
understanding of those needs and how to work
together to meet them.”
– Children’s Workforce Development Council

Common Assessment Framework (CAF)
Children with no identified
additional needs
Children with additional needs
Children with complex needs
Common Assessment Framework (CAF)
Social Service input

The use of the CAF in practice
• NICE recommendation:
�Professionals should consider using the CAF following
a presentation to Child and Adolescent Mental Health
Services (CAMHS)
�To help professionals, the family and the school to
support and protect the child
• UCLH recommends the use of an electronic
version (eCAF)

Contents
• Background
• Aims
• Method
• Results
• Conclusions
• Recommendations

Aims
• Determine current practice of eCAF reporting
• Develop a standardised tool to ensure the eCAF is
completed at each CAMHS presentation

Contents
• Background
• Aims
• Method
• Results
• Conclusions
• Recommendations

Methods
• Retrospective case note review
• Inclusion criteria:
�Self-harm CAMHS admissions to UCLH
− deliberate self-harm, suicidal ideation, suicidal attempt
�August 2012 to February 2013
• Data analysis

Methods
• Included:
Sex Length of admission
Age Previous contact with CAMHS services
Borough First admission or previously admitted
Ethnicity Nature of the presentation
Month of admission Nature of follow-up
Admission and discharge within or out of hours

Contents
• Background
• Aims
• Method
• Results
• Conclusions
• Recommendations

Results
• There were 40 admissions extracted from hospital
databases
• 29 admissions met our inclusion criteria
• 83% of admissions were female
• The average length of stay was 2 days
• 55% of patients were from Camden & Islington
• Ratio of patients known to CAMHS vs. not known was
approximately 1:1
• For the majority of patients (69%) this was their 1st
admission
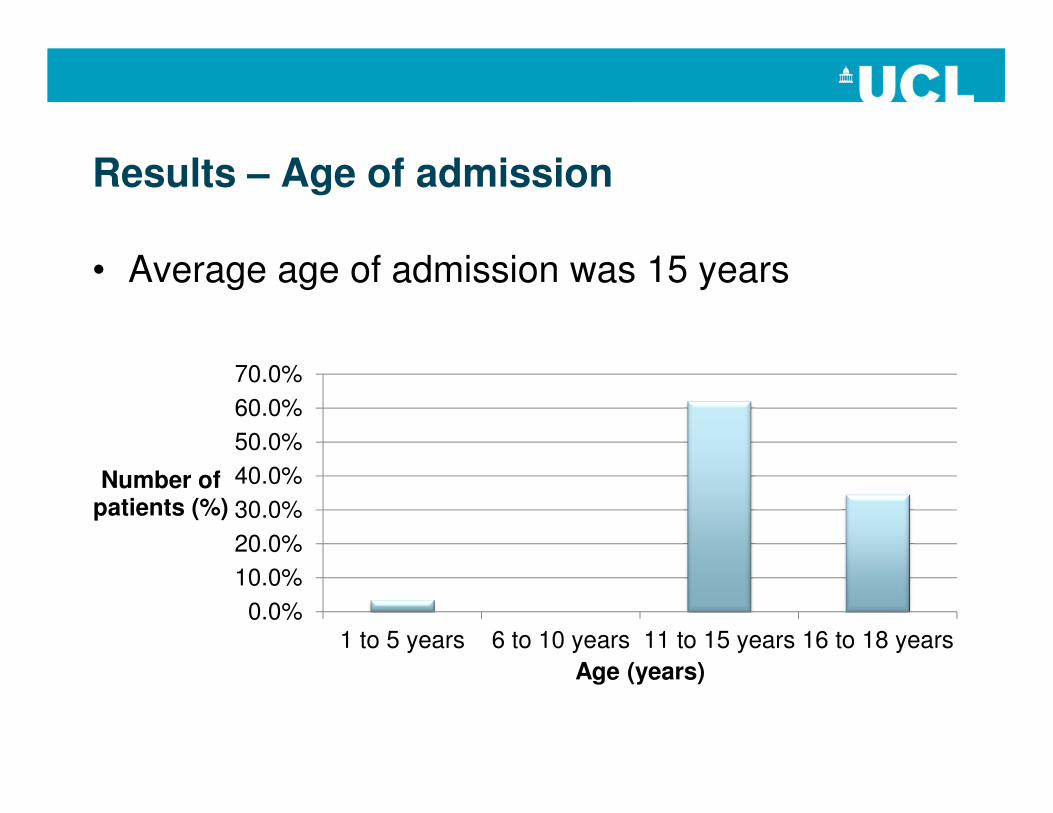
Results – Age of admission
• Average age of admission was 15 years
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
1 to 5 years 6 to 10 years 11 to 15 years 16 to 18 years
Number of patients (%)
Age (years)

Results – Overall
Suicide attempt, 58.62%
DSH, 24.14%
Suicide ideation, 13.79%
Accidental overdose,
3.45%
Context of admission
eCAF completed,
62.07%
No eCAF completed,
20.69%
Previous eCAF only,
17.24%
eCAF forms

Results – Age: eCAF vs. Non-eCAF
11 to 15 years,
44.83%
16 to 18 years,
17.24%
eCAF completed
1 to 5 years, 3.45%
11 to 15 years,
17.24%
16 to 18 years,
17.24%
eCAF not completed
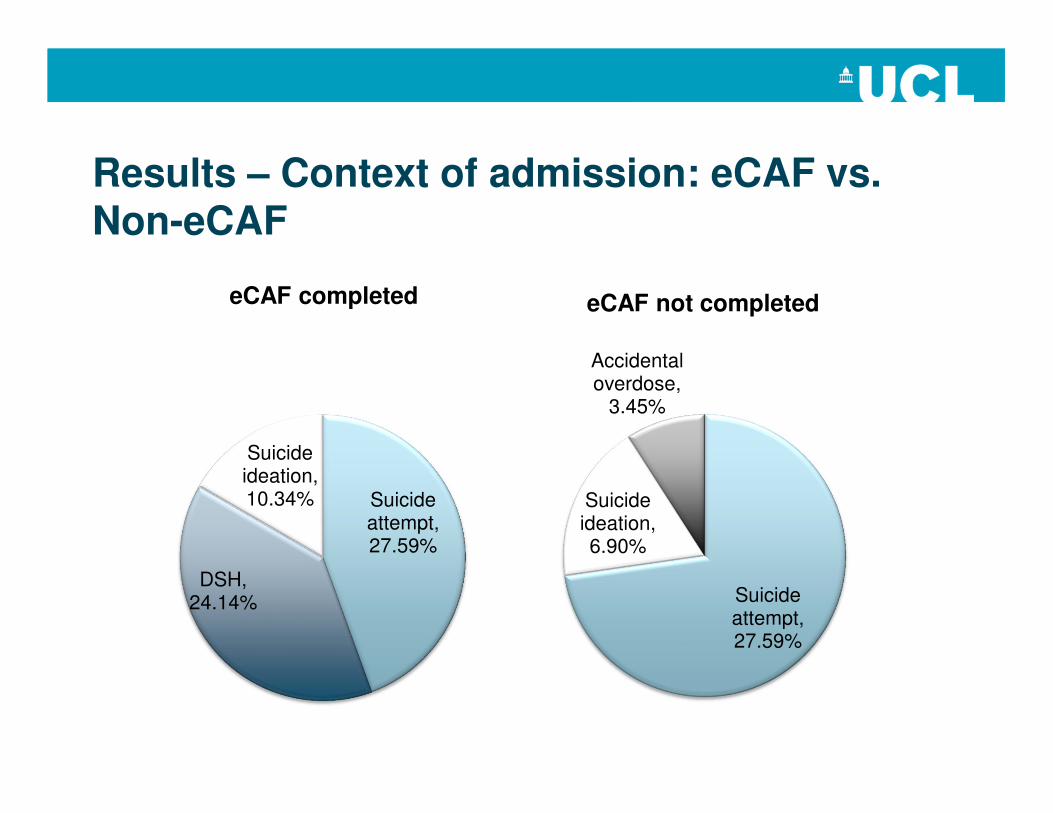
Results – Context of admission: eCAF vs. Non-eCAF
Suicide attempt, 27.59%
DSH, 24.14%
Suicide ideation, 10.34%
eCAF completed
Suicide attempt, 27.59%
Suicide ideation, 6.90%
Accidental overdose,
3.45%
eCAF not completed

Results – History of admissions? eCAF vs. Non-eCAF
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
eCAF completed eCAF not completed
First admission
History of admissions

Results – Ethnicity: eCAF vs. Non-eCAF
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
eCAF not completed
eCAF completed

Results – Follow up: eCAF vs. Non-eCAF
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
Follow upCAMHS
UCH
Follow upCAMHS
local
Dischargeto GP
In patientadmission
Unknown
eCAF completed
eCAF not completed

Results – Supplementary findings
• Gender: all male patients had an eCAF completed, whereas almost half (45.8%) of females did not
• Known to CAMHS: This did not affect whether they had an eCAFcompleted
• Residence of patient: Overseas patients (n = 2) did not have an eCAF completed
• Month of admission: Fewer were completed Sept– Nov (50% completed), most were completed Dec – Jan (66% completed)
• Out of hours admission / discharge: if both within working hours, there was a 50% chance of an eCAF being completed
• Duration of admission: Patients admitted for ≥4 days did not have eCAFs completed. 70% of those discharged on the same day had eCAFs completed.

Contents
• Background
• Aims
• Method
• Results
• Conclusions
• Recommendations

Conclusions
• eCAF forms are not being completed across all patient
groups
• They are significantly being missed in those from an ethnic
minority
• This may represent lack of clinician confidence across
varying cultural backgrounds
• A standardised tool with prompts for eCAF is being
developed to ensure that this vital referral is not
overlooked

Contents
• Background
• Aims
• Method
• Results
• Conclusions
• Recommendations

Recommendations
1. Leaflet distribution
2. Poster distribution
3. Departmental presentation at induction
4. Electronic pop-up on hospital systems
5. Electronic prompt on paediatric discharge summary
6. eCAF sticker for medical notes
7. Creation of an eModule on the use of eCAF
8. Re-audit
References
• http://www.rcpsych.ac.uk/expertadvice/problems/depression/self-harm.aspx
• Madge N, Hewitt A, Hawton K, de Wilde EJ, Corcoran P, Fekete S, van
Heeringen K, De Leo D, Ystgaard M. Deliberate self-harm within an
international community sample of young people: comparative findings from
the Child & Adolescent Self-harm in Europe (CASE) Study. Journal of Child
Psychology and Psychiatry 49:6 (2008), p 667-677.
• Hawton K, Saunders KEA, O’Connor RC. Self-harm and suicide in
adolescents. Lancet 379 (2012), p 2373-2382.
• guidance.nice.org.uk/cg133

THANK YOU!
• Dr Zaib Davids (Consultant Child & Adolescent Pychiatrist,
UCLH)
• Dr Golnar Aref-Adib (CT3 Psychiatrist)
• A&E Team UCLH