Dr ghazy 2012 my implant lecture for 4th year students
25
19/04/2012 1 Fourth year Class 2011/2012 IMPLANT–SUPPORTED FIXED PROSTHESIS BY Dr MoHAMeD H. GHAZY Febuary 12, 2012 • Implant prosthodontics : • The phase of prosthodontics concerning replacement of missing teeth and/or associated structures by restorations that are attached to dental implants A prosthetic device of alloplastic material implanted into the oral tissue beneath the mucosal or/and periosteal tissue for fixed or removable prosthesis What is a dental implant ? Indication & contraindication Indications • Single tooth loss • Inability to wear a removable P.D. • Free end distal extension • Need for long span FPD with questionable prognosis • Unfavorable number and location of potential natural tooth abutment Contraindications • Lack of operator experience • Smoking • Pregnancy • Immunosuppression (chemotherapy, HIV, etc) • Antimetabolic treatment • Poorly controlled cardiovascular problems • Tumoricidal radiation to implant site • Psychiatric disorders • Patients with bone diseases, such as Histiocytosis X , Paget's Disease and Fibrous Dysplasia • uncontrolled hematologic disorders such as Generalized Anemias , Hemophilia • Patients with endocrine disorders, such as uncontrolled Diabetes Mellitus , Pituitary and Adrenal insufficiency and Hypothyroidism Treatment planning for implant patient Indication &contraindication Clinical evaluation Adequate bone and anatomic structure Visual inspection & palpation Flabby excess tissues Bony ridges Sharp underlining osseous formations and undercuts Radiographic evaluation Panoramic view with small radio opaque reference Cephalometric film to evaluate bone width CT scan to locate inferior alveolar canal & maxillary sinuses Diagnostic casts Study the remaining dentition Evaluate residual bone Analyze maxillo-mandibular relationship Diagnostic waxing and surgical templates Bone sounding With probe judging the soft tissue thickness and bone soundness
-
Upload
mohamed-ghazy -
Category
Education
-
view
2.654 -
download
3
Transcript of Dr ghazy 2012 my implant lecture for 4th year students

19/04/2012
1
Fourth year Class 2011/2012 IMPLANT–SUPPORTED FIXED PROSTHESIS
BY Dr MoHAMeD H. GHAZY Febuary 12, 2012
• Implant prosthodontics :
• The phase of prosthodontics concerning replacement of missing teeth and/or associated structures by restorations that are attached to dental implants
A prosthetic device of alloplastic material implanted into the oral tissue beneath the mucosal or/and periosteal tissue for fixed or removable prosthesis
What is a dental implant ?
Indication & contraindication
Indications • Single tooth loss
• Inability to wear a removable P.D.
• Free end distal extension • Need for long span FPD with
questionable prognosis • Unfavorable number and location
of potential natural tooth abutment
Contraindications • Lack of operator experience
• Smoking
• Pregnancy
• Immunosuppression (chemotherapy, HIV, etc)
• Antimetabolic treatment
• Poorly controlled cardiovascular problems
• Tumoricidal radiation to implant site
• Psychiatric disorders
• Patients with bone diseases, such as Histiocytosis X, Paget's Disease and Fibrous Dysplasia
• uncontrolled hematologic disorders such as Generalized Anemias, Hemophilia
• Patients with endocrine disorders, such as uncontrolled Diabetes Mellitus, Pituitary and Adrenal insufficiency and Hypothyroidism
Treatment planning for implant patient Indication &contraindication
Clinical evaluation Adequate bone and anatomic structure
Visual inspection & palpation Flabby excess tissues
Bony ridges
Sharp underlining osseous formations and undercuts
Radiographic evaluation Panoramic view with small radio opaque reference
Cephalometric film to evaluate bone width
CT scan to locate inferior alveolar canal & maxillary sinuses
Diagnostic casts Study the remaining dentition
Evaluate residual bone Analyze maxillo-mandibular relationship
Diagnostic waxing and surgical templates
Bone sounding With probe judging the soft tissue thickness and bone soundness

19/04/2012
2
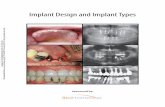
Subperiosteal Transosteal
Endosteal plate
form
Endosteal
root form
To the left you can
see a typical modern
Root form Implant
and to the right of
the implant is a
picture of a natural
tooth.
One can see how the
implant is designed
to replace the root of
a tooth by the
somewhat apparent
similarity.
Screw Retained
Transocclusal
Screw Retained
Transversal
Cemented
Fixed Partial Denture
Implant supported prosthesis may be
OSSEOINTEGRATION A direct structural and functional
connection between ordered living
bone and the surface of a load
carrying implant
Swedish professor of orthopedics
named Per-Ingvar Branemark in 1965 he used the first titanium dental implant into a human volunteer

19/04/2012
3
Implant most commonly used from
–commercially pure (CP) titanium – titanium-aluminum-vanadium alloy (Ti-
6Al-4V) - stronger & used w/ smaller diameter implants
Why Titanium
• lightweight • biocompatible • corrosion resistant (dynamic inert oxide layer)
• strong & low-priced
Principles of Implant location Anatomic limitation
General guide lines
• Ideal bone should be 10 mm vertical and 6 mm horizontal
• Two mm above the superior aspect of inferior alveolar canal
• Five mm anterior to mental foramen
• one mm from the periodontal ligament of adjacent tooth
• Three mm between 2 implant to ensure bone vitality.
Anterior maxilla
• 1- Minimum of 1 mm between the
implant apex and nasal vestibule
• 2- Implant slightly off midline on either
sides of incisive foramen.
Principles of Implant location Anatomic limitation
Posterior maxilla
Bone less dense, larger narrow spaces, and thin cortex
• 1- One implant for every tooth
• 2- One mm of bone between the floor of
sinus and implant
Principles of Implant location Anatomic limitation

19/04/2012
4
Anterior mandible
• 1- One implant placed through the
entire cancellous bone
• 2- Five mm anterior to the foramen
Principles of Implant location Anatomic limitation
Posterior mandible
• 1- Two mm above the superior aspect
of inferior canal
• 2- More time required for integration
• 3- Attachment of mylohyoid muscle
Principles of Implant location Anatomic limitation
Principles of Implant location Restorative consideration
Implant placement 1- Stay 1mm from the adjacent natural tooth but not so far
to for contouring restoration
Less ideal location
2- Long axis of implant should be positioned in the central
fosse of the restoration
Principles of Implant location Restorative consideration
Implant placement
Natural
tooth
Ideal
implant placement

19/04/2012
5
Implant and restoration size 1-Size should be considered during treatment planning
2- 4mm diameter for maxillary central
3- 3mm for mandibular incisors
4- 5-6mm for molars
Surgical guide Template extremely useful for anterior
implant Objectives 1- Delineate the embrasures 2- Locate the implant within the restoration contour 3- Align the implant within the long axis of the restoration 4- Identify the level of CIJ or tooth emergence from the soft tissue
Wax model of a tooth to be replaced in the surgical guide

19/04/2012
6
Surgical guide template
Stent used as guide for implant placement
Surgical guide for correct implant
placement Implant surgery
Surgical access
Implant placement
Postoperative evaluation
Implant uncover
Guide drill / 2mm twist drill / Pilot drill / 3mm twist drill / Countersink

19/04/2012
7
Implant restorations Significant factors for success 1- Precise placement 2- A traumatic surgery 3- Unloaded healing 4- Passive restoration
Fourth year Class 2011/2012 IMPLANT–SUPPORTED FIXED PROSTHESIS
BY Dr MoHAMeD H. GHAZY February 19, 2011
Implant fixture
Abutment
Retaining screw
Abutment screw
Components of an
implant restoration Composite resin
Screw- retained implant
restorations consist of
three components.
(a) Implant fixture
(b) Abutment
(c) Restoration
- The abutment screw secures
the abutment to the fixture
- The prosthetic retention screw
secures the prosthesis to the
abutment.
Gutta percha

19/04/2012
8
• Lekholm and Zarb bone type classification Type I bone homogenous, compact bone Type II bone a thick layer of compact bone surrounding a core of dense trabecular bone Type III bone a thin layer of cortical bone surrounding a core of dense trabecular bone of good strength Type IV bone thin layer of cortical bone surrounding core of low density .
Implant insertion into
the prepared socket
Unscrewing the abutment from the implant
fixture, screw covering and suturing

19/04/2012
9
Removal of the cover screw in
the 2nd stage and abutment attached to the fixture as a
coping ready for impression
The abutment removed from the implant
fixture
Abutment and its implant analog and
repositioned in the impression
Abutment prepared to its final form in the
working cast

19/04/2012
10
Prepared abutment and final restoration
in the patient mouth Impression post Closed tray
Impression
Imp post & analog
Imp post & analog relocated on the
impression
Polyether soft tissue injected around
analog before
pouring
Implant restorations
Poured cast
Impression coping locates the analog in
the same position in
the cast as the implant in the mouth
Contouring of the soft tissue material
Zirconia abutment seated on cast Zirconia abutment
seated in the mouth
Zirconia abutment for cement retained
restoration selected

19/04/2012
11
Dental Implant Should promote bone in-
growth. Structure and
geometry differences are the selling point for most
companies.
Prosthetic Crown Look and feel of real
tooth. Easily replaced.
Abutment Secures the crown to the
Dental Implant. Can be
straight or angled depending on implant location
Titanium
screw
Clinical Implant system components
Hydroxyl appetite coated screw
Hydroxyl Apatite coated cylinder
Titanium plasma sprayed cylinder
Implant body
Titanium screw
Is the component placed within the bone during 1st stage surgery
Two images showing two different types of tapered,
cylindrical implants. One looks like a Christmas tree with fins projecting out to the sides; the other shows a special surface
treatment consisting of spherical titanium beads.
Cover screw It is the component placed over the dental implant during the
osseointegration phase to seal the occlusal surface of the
implant and prevent tissue from proliferating into the internal
portion of the implant body It should be of low profile to facilitate the suturing of soft
tissue tension _free.

19/04/2012
12
Healing abutment
A- screw into implant
B- Screw into abutment
(healing cap)
Dome shaped 2-10 mm screw placed on the implant after the 2 and stage surgery & before insertion of the prosthesis
Healing Abutments
Transgingival Titanium piece which
will form the soft tissue
Selected considering the
Emergence Profile needed for the restoration and the tissue height
Healing Abutments
Necessary Information:
Healing Abutment Height
Platform Diameter (normally same as implant diameter )
Healing Abutment Diameter (EP Profile
Height
Restorative Platform
EP® (Emergence Profile)

19/04/2012
13
Abutment Component of the implant system that screw directly into the implant to support and or retains a prosthesis or implant superstructure
Abutment
Abutment
screw
(green)
Abutment
- can be either parallel
(standard) or conical
(estheticone) in shape.
- are secured with an
abutment screw that is
tightened to 20 Ncm.
(Screw retained restoration)
Abutment
(Cemented restoration)
- Cera One abutment
- secured with a square
head screw tightened to 32
Ncm.
(red)
Straight
15º Pre-Angled
Engages Implant Hex
Engages 12 Point Double Hex
Click Zone

19/04/2012
14
2 impression techniques
Open tray impression Closed tray impression
Education
Open tray impression Concept
Intraoral situation Implant & impression post Analog & impression post
55 Education
Impression procedure
Remove closure screw or healing abutment
Insert impression post and hand tighten screw with the screwdriver
56 Education
Take impression with an open tray
Use an elastomeric impression material
Impression procedure

19/04/2012
15
57 Education
When impression material is set, unscrew and remove the impression
Impression procedure
A one piece coping
Screw into the abutment
used if the abutment does not need to be changed on the
lab cast
Two piece coping
Screw into the implant
used if the abutment does not need to be
changed on the lab cast
Two piece coping
Screw into the abutment
used to orient the anti-rotational feature or to
make impression of very divergent implant
Types of impression posts
Two piece Impression coping
Impression coping attached to the implant analog
• The impression posts attached to the implants fixtures.
Impression with laboratory analog to make the master cast.
The master cast is that one used to fabricate the final prosthesis.

19/04/2012
16
Laboratory analogs Components made to represent the top of the implant fixture or the abutment in the laboratory cast
Fixture analog
{Duplicate implant top}
Abutment analog
{Duplicate abtument top}

19/04/2012
17
Attach Analog
Push Analog/Impression Coping Assembly into Impression Twist and Lock Grooves into Impression

19/04/2012
18
Waxing sleeves
Plastic waxing sleeve tightened
to a laboratory analog
Gold cylinder tightened to a
laboratory analog
Combination
Prosthesis retaining
screw Screw used to secure the
prosthesis to the implant
or the transmucosal
abutment
Prosthetic
retaining screw
Prosthetic retaining screw
Have a slot or hex head Access is usually covered by a combination of gutta percha and composite. used to retain the prosthesis to the abutment. Tightened to 10 Ncm.
Implant fixture
Abutment
Retaining screw
Abutment screw
Components of an implant
restoration Composite resin
Screw retained implant restorations
consist of three components.
(a) Implant fixture
(b) Abutment
(c) Restoration
- The abutment retaining screw
secures the abutment to the fixture
- The prosthetic retaining screw
secures the prosthesis to the abutment.
Gutta percha

19/04/2012
19
Screw retained implant crown Slot Screw
Driver
- Used to remove or replace slotted prosthetic retention screws.
- Tighten to 10 Ncm
Hex Screw Driver
- Used to remove or replace hex prosthetic retention screws.
- Tighten to 10 Ncm.
Abutment Screw Driver
- Used to remove or replace abutment screws for standard or
conical (estheticone / mirus cone) abutments.
- Tighten to 20 Ncm.

19/04/2012
20
Square Screw Driver
- Used to remove or replace Cera One abutment screw.
- Tighten to 32 Ncm
Impression tray without impression material: After the impression tray is prepared, it should be checked to see that it fits and fully covers the area of the impression and that the hole in the tray is aligned with the guide pin.
Impression tray with impression material in the jaw: The coping must be completely covered by impression material and the tray be fully seated. It is very important that the guide pin protrudes through the impression tray in order to open it with the hex driver.
Inverted impression tray with emphasized hex: The hexagon of the impression coping can be seen. It is very important to check that the position of the impression coping has been accurately recorded and that the hex is clear of any impression material.
Inverted impression showing gingiva being syringed around analog The analogue can now be attached to the impression coping by screwing in the guide pin. It should be confirmed that the coping is attached to the analogue with no misalignment of gaps. At this stage, injecting impression material around the neck of the analog can simulate the gingiva.
Stone model prepared with simulated gingiva and implant analog In the final stage in impression taking, a stone model of the gingiva and teeth should be cast, and the simulated gingiva should remain on the model. After the stone is hardened, the impression coping can be released from the model by removing the guide pin. The impression tray can now be separated from the model

19/04/2012
21
Silicone index and wax model of tooth When the wax model of the tooth is appropriately positioned a silicon key can be prepared that will serve as a good replica of the missing tooth.
Option 1: Placing the gold plastic cylinder abutment on the stone model Following the construction of the silicone index a gold plastic cylinder abutment with hexagon can be selected.
Option 1: Wax Carving The plastic part of the gold plastic cylinder abutment can now be grind to the appropriate height on the stone model, taking into account the height of the adjacent teeth. After the gold abutment and the plastic cylinder have been prepared, it is possible to carve the wax to the desired shape. Following the carving of the wax on the gold abutment and the plastic cylinder they will be cast.
Option 1: Silicon index with wax up The silicon index will be used to check that the dimensions of the wax-up are appropriate to its surroundings.
Option 1: Metal casting When fabricating P.F.M crown, using the direct wax-up technique on the cap to get a metal frame onto which the porcelain firing takes place. Checking the metal on the stone model and the seating of the external hex of the gold abutmnent in the internal hex of the implant analog.
Option 1: Porcelain in mouth After placing the crown, the screw of the gold abutment should be tightened to 20 Ncm utilizing the TORKIT wrench. This will minimize the chances of the screw opening. After the screw has been tightened, the screw hole should be closed.

19/04/2012
22
Option 2: Placing the plastic cylinder on the stone model Following the construction of the silicon index a plastic cylinder with hexagon can be selected
Option 2: Wax Carving The plastic cylinder can now be grind to the appropriate height on the stone model, taking in the account the height of the adjacent teeth. After the plastic cylinder have been prepared, it is possible to carve the wax to the desired shape. Following the carving of the wax on the plastic cylinder they will be cast.
Option 2: Silicon index with wax up The silicon index will be used to check that the dimensions of the wax-up are appropriate to its surroundings. MT-HHR13
Option 2: Metal casting When fabricating P.F.M crown, using the direct wax-up technique on the plastic cylinder a metal frame onto which the porcelain firing takes place. Checking the metal on the stone model and the seating of the external hex of the casting (what was previously the external hex. of the plastic cylinder MD-CPH13), in the internal hex of the implant analog.
Option 2: Check the casting in the mouth After completion of the casting, a check must be made in the paient’s mouth using the screw MD-SO220 to connect it.
Option 2: Porcelain on plaster model Following the selection of the appropriate color, the porcelain is fired on the metal casting.
Option 2: Porcelain in mouth After placing the crown, the screw of the plastic cylinder should be tightened to 20 Ncm utilizing the TORKIT wrench. This will minimize the chances of the screw opening. After the screw has been tightened the screw hole should be closed.

19/04/2012
23
IMPLANT RESTORATIVE OPTIONS Distal-extension Implant Restoration. There are two distal-extension restorative options.
1. Tooth-implant supported restoration Place an implant distal to the most
posterior natural abutment and fabricate a fixed prosthesis connecting the implant with the natural tooth. However, there are problems associated with implants connected to natural teeth .
2. Implant supported restoration Place two or more implants posterior to the most distal natural tooth and fabricate a completely implant-supported restoration ).
If the crown-to-implant ratio is favorable, two implants to support a three-unit fixed prosthesis. If implants are short and crowns are long, one implant to replace each missing tooth. If doubt remains, more implants are used when heavier forces are expected (e.g., posterior part of the mouth in patients with evidence of parafunctional activity). Fewer implants are used when lighter forces are expected (e.g., those opposing a complete denture or those supporting a prosthesis in the anterior part of the mouth).
IMPLANT RESTORATIVE OPTIONS Distal-extension Implant Restoration.
Long Edentulous Span Restoration. 1. The clinician may choose to have multiple
implants placed between the remaining natural teeth and to fabricate a fully implant-supported restoration.
2. One or two implants can be placed in the long edentulous span and the final restoration connected to natural teeth.
When it is necessary to connect implants and the natural teeth, protecting the teeth with telescopic copings is recommended .
In this manner, prosthesis retrievability can be maintained.
Some long edentulous spans require the reconstruction of soft and hard tissue and teeth. using resin teeth processed to a metal substructure rather than a conventional metal-ceramic restoration is recommended.
Soft tissue esthetics can be more easily and accurately mimicked with heat-processed resin and large defects .
This type of restoration has been called a hybrid because it combines the principles of conventional fixed and removable prosthodontics.
IMPLANT RESTORATIVE OPTIONS Distal-extension Implant Restoration. Long Edentulous Span Restoration.
Single-tooth Implant Restoration. Indicated in the following situations:
1. An otherwise intact dentition 2. spaces difficult to treat with conventional fixed prosthodontics 3. Distally missing teeth. 4. A prosthesis that needs to closely mimic the missing natural tooth
The requirements for single-tooth implant crowns are:
1. Esthetics 2. Ant rotation to avoid prosthetic component loosening 3. Simplicity-to minimize the amount of components used 4. Accessibility-to maintain optimum oral health 5. Variability-to allow the clinician to control the height, diameter, and angulations of the implant restoration

19/04/2012
24
IMPLANT RESTORATIVE OPTIONS Distal-extension Implant Restoration.
Long Edentulous Span Restoration. Single-tooth Implant Restoration.
Fixed Restoration in the Completely Edentulous Arch. 1.The hybrid prosthesis is a cast alloy framework with processed denture resin and teeth. It requires a minimum of five implants in the mandible and six in the maxilla. Suitable for patients who have had moderate bone loss, the prosthesis restores both bone and soft tissue contours. 2. The metal-ceramic rehabilitation also requires five implants in the mandible and six in the maxilla. Only if minimal bone loss has occurred and is best suited for patients who have recently lost their natural teeth (within 5 years). 3. For patients with severe bone loss, there is probably only one option: a removable restoration . Minimal resorption
—Metal ceramic restorations
Moderate resorption —resin to metal restorations
sever resorption —Over denture
CEMENT-RETAINED VERSUS SCREW-RETAINED IMPLANT CROWNS Zinc phosphate, glass ionomer, and composite resin cements have all been suggested for this purpose. Advantages of cement-retained restorations. 1. Simplicity 2. Less expensive. 3. Allow minor angle correction. 4. More esthetically pleasant
Disadvantages of cement-retained restorations. 1. Require more chair time 2. Have the same propensity to loosen as the
screw retained. Advantages of screw-retained restorations. 1. Retrievability
Disadvantage of a screw-retained implant
restoration 1. The screw may loosen during function. 2. Cost
CEMENT-RETAINED VERSUS SCREW-RETAINED IMPLANT CROWNS If the screw is sufficiently tightened into the implant crown to seat it, a clamping load or preload is developed between the implant and the crown. If this clamping force is greater than the forces trying to separate the joint between implant and crown, the screw will not loosen.
Screw Retained
Transocclusal

19/04/2012
25
Screw-Retained Crowns
Screw Retained
Transversal
Cemented Crowns