Dr Alvin Tan - General Practice Conference & Medical ... North/Sat_Plenary_1215_Tan_UPDATED... ·...
22
Dr Alvin Tan Consultant Medical Oncologist Waikato District Health Board 12:15 - 12:25 Advanced Prostate Cancer Care
-
Upload
truongthuan -
Category
Documents
-
view
218 -
download
3
Transcript of Dr Alvin Tan - General Practice Conference & Medical ... North/Sat_Plenary_1215_Tan_UPDATED... ·...

Dr Alvin TanConsultant Medical Oncologist
Waikato District Health Board
12:15 - 12:25 Advanced Prostate Cancer Care
Advanced Prostate Cancer Care
Alvin Tan, Medical Oncologist, Waikato Hospital
Take Home Message
• Lots of men with prostate cancer
• GPs are important in managing prostate cancer
• PSA screening is controversial
• Increasing number of treatment options available
• GPs can prescribe abiraterone
(But please continue to listen for the next 10 minutes)
Demographics in NZ
• 3000 men are diagnosed with prostate cancer each year
• Approximately 650 men die from this each year
• Maori men are more likely to die from prostate cancer, often presenting with advanced stage at diagnosis.

Male cancer registration rates, by site, 25+ years, Māori and non-Māori, 2010–12
Source: New Zealand Cancer Registry (NZCR), Ministry of Health

Male cancer mortality rates, by site, 25+ years, Māori and non-Māori, 2010–12
Source: New Zealand Cancer Registry (NZCR), Ministry of Health

Importance of GPs in prostate cancer management
• Localised prostate cancer – screening / initial referral / Active surveillance
• Post surgery / radiation follow-up - PSA monitoring
• If recurrent/progressive disease • Prescribing hormone therapy and monitoring response• Managing ADT side effects and patient well-being• Analgesia• Liaise with hospice• Referrals to Radiation Oncology for palliative radiation for bone pain
• (NEW) – when castrate resistant, GPs can now prescribe abiraterone in consultation with Urology/Oncology

PSA – what is it?
• Glycoprotein produced by the prostate gland, responsible for liquefying seminal fluid
• Usually present in small quantities in serum
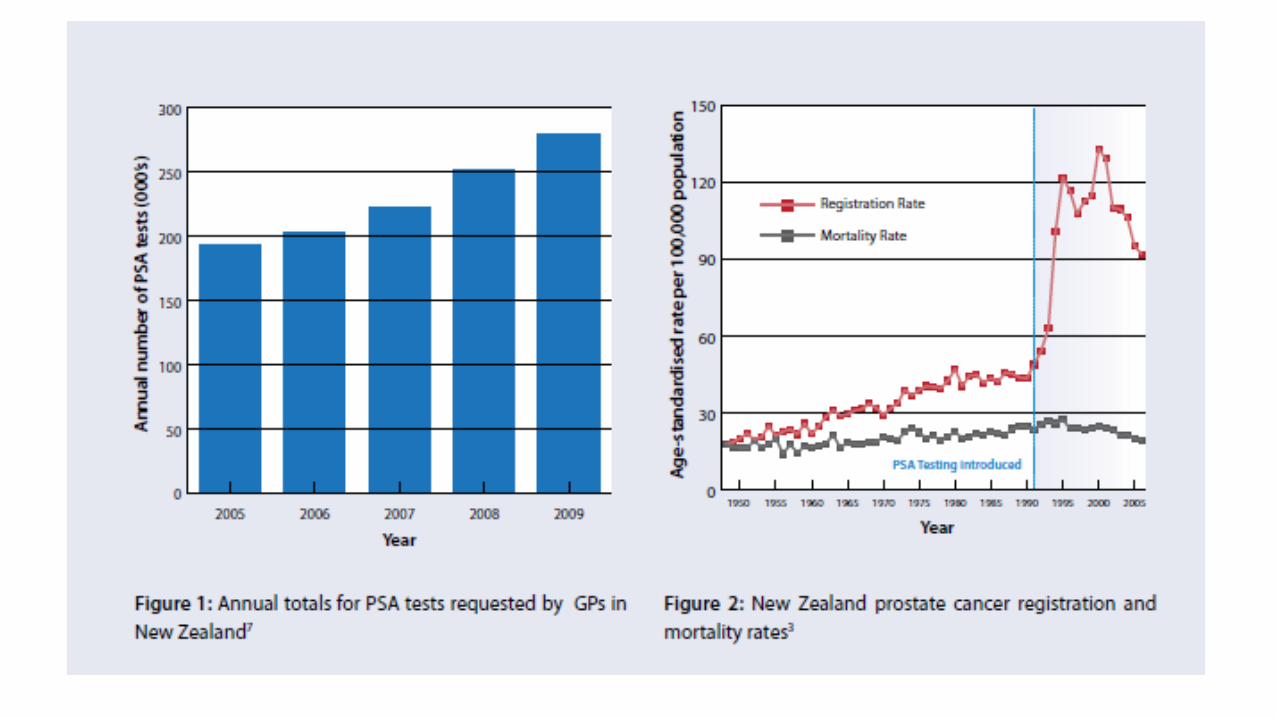
• In 2009, GP’s performed an average of 74 PSA tests per year per clinician (BPAC source)
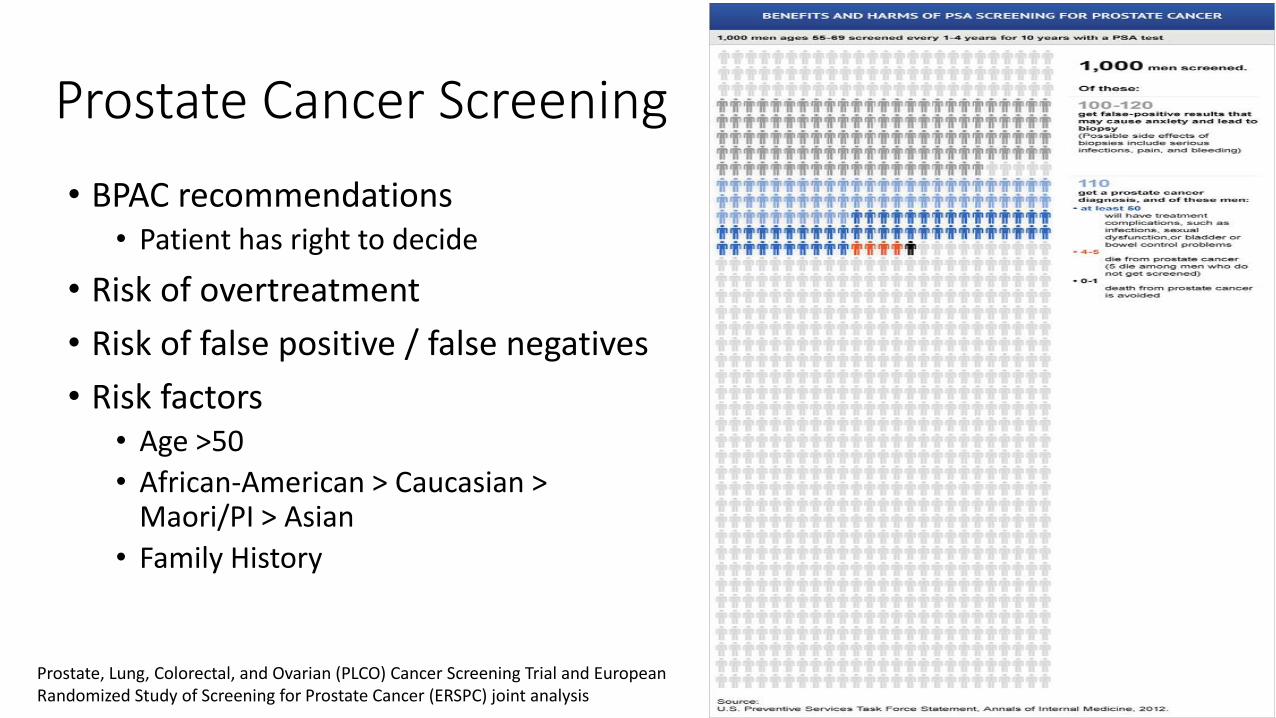
Prostate Cancer Screening
• BPAC recommendations • Patient has right to decide
• Risk of overtreatment
• Risk of false positive / false negatives
• Risk factors• Age >50
• African-American > Caucasian > Maori/PI > Asian
• Family History
Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial and European Randomized Study of Screening for Prostate Cancer (ERSPC) joint analysis
When does Medical Oncology get involved?
• In as many as 10-50% of localised prostate cancer may progress and spread to the pelvic lymph nodes and bone
• Mainstay therapy at this stage usually involves androgen deprivation therapy • This can last for months to years

Androgen Deprivation Therapy
• Inhibitive – GnRH agonist• Goserelin (Zoladex)
• 3.6 mg Q1 monthly, 10.8 mg Q3 monthly depot
• Leuprorelin (Lucrin)• 3.75 mg Q1 monthly, 11.25 mg Q3monthly, 30 mg Q6 monthly depot
• Competitive• Antiandrogens (as lead in prior to androgen inhibition)
• Bicalutamide• Flutamide• Cyproterone

Androgen Deprivation Therapy – Common side effects• Erectile dysfunction
• Loss of libido
• Hot flushes
• Osteoporosis
• Loss of muscle tone
• Weight gain
• Mood swings
Prognosis
• Early advanced disease – potentially years on ADT therapy • Castrate resistance develops over a median span of 18-24 months following
initiation of ADT. • Historically once castrate-resistant, median survival of 1-2 years.
With new therapies, median survival now 2-3 years. • Prognosis is associated with a number of factors:
• Sites of disease (ie visceral, bone alone)• Performance status• ALP• Hb• PSA doubling time• Pain at baseline
Docetaxel chemotherapy – castrate resistant setting• Outpatient IV chemotherapy given every 2 or 3 weeks for each cycle
• Usually 24-30 weeks of treatment
• 50% reduction in PSA levels in about half of patients
• Improve pain symptoms in 1/3 patients
• Improves QOL in 1/4 patients
• Improve overall survival by 2 ½ months
• Common side effects:• Infection risks, peripheral neuropathy, nausea/vomiting, hair loss, diarrhoea, fatigue

Docetaxel chemotherapy – castrate sensitive setting• New trial results in last 2 years (STAMPEDE, E3805)
• Early use of docetaxel in metastatic prostate cancer
• 6 cycles of chemotherapy
• Improves overall survival by 14-17 months, particularly in large volume metastatic disease

Abiraterone – castrate resistant setting
• Novel hormonal therapy affecting the CYP17 pathway
• 1000 mg daily (4 tabs) on an empty stomach
• Prolongs survival (4 months gain), PSA response and delays progression
• Blocks testosterone formation
• But leads to increase in mineralcorticoid hormone production • HTN, fluid retention, electrolyte imbalance
• This is mitigated by taking daily prednisone 5 mg BD.
• GPs can now prescribe this, in discussion with Urologist / Oncologist

Side effects of Abiraterone
• Common (1 in 10)• Fatigue, fluid retention, low potassium, hypertension , diarrhoea, urine
infection
• Occasional (1-10 in 100)• Liver derangement, cardiac arrhythmias, mild myelosuppression, reflux
• Rare (<1 in 100)• Myalgia, muscle weakness, adrenocortical insufficieny
What to do if your patient is on Abiraterone?
• Monthly blood pressure checks
• Monthly UEs
• Monthly review for first 3 months, then can extend out to Q3 months
• Liver functions tests every 2 weeks for the first 3 months, then every month
• Ensure prednisone is taken daily with Abiraterone
• Would check PSA at baseline and at 3 months (PSA can continue to rise for up to 3 months initially). Thereafter, can be Q2-3 monthly.

Other Treatments
• Sipuleucil-T vaccine (US, $$$)
• Radium 223 (AUS, $$$)
• Cabazitaxel chemotherapy (private, $$$)
• Enzalutamide novel androgen receptor antagonist (patient access program)
• Low dose steroids
• Biphosphonate infusions
• Analgesia + Hospice input
• Palliative Radiotherapy for localised symptoms (eg bone pain)
Take Home Message
• Lots of men with prostate cancer
• GPs are important in managing prostate cancer
• PSA screening is controversial
• Increasing number of treatment options available
• GPs can prescribe abiraterone
After reading the the sentence, you are now aware that the the human brain often does not inform you that the the word ‘the’ has been repeated twice every time
THE THE END