Download
7
European Journal of Radiology 61 (2007) 195–201 BIRADS TM mammography: Exercises Corinne Balleyguier a,∗ , Franc ¸ois Bidault a , Marie Christine Mathieu b , Salma Ayadi a , Dominique Couanet a , Robert Sigal a a Radiology Department, Institut de Canc´ erologie Gustave-Roussy, 39 rue Camille Desmoulins, 94805 Villejuif Cedex, France b Biopathology Department, Institut de Canc´ erologie Gustave-Roussy, 94805 Villejuif, France Received 18 August 2006; received in revised form 21 August 2006; accepted 24 August 2006 Abstract Some radiological cases are presented in this article to train the reader to the BIRADS TM classification in mammography. Each case is described according to the fourth American version of the BIRADS TM lexicon. Some classifications difficulties will also be presented, in order to show the complexity and the observer variability, commonly encountered in BIRADS TM 3 and 4 categories. © 2006 Published by Elsevier Ireland Ltd. Keywords: BIRADS TM classification; BIRADS TM 3 category; Mammography; Training; Microcalcifications; Breast 1. Illustrating cases of BIRADS TM mammography classification An oval shape mass is visible on this view. Contours are well circumscribed (arrows), a mixed content with fat and glandular tissue is visible within the mass. The diagnosis is an hamartoma. This is a typical example of the BIRADS TM 2 classification in mammography. No further examination is necessary (Fig. 1). Macrocalcifications are dense, linear and needle-shape, fol- lowing the ducts and oriented toward the nipple, which is very suggestive of a plasma cell mastitis (arrows). This a typically benign disease of the breast which can be classified in the BIRADS TM 2 category (Fig. 2). Multiple round calcified masses are visible in the right breast. The peripheral calcifications are typical of calcified fibroade- noma. No further examination is necessary. BIRADS TM 2 category (Fig. 3). This view shows at least three microcalcifications clusters. All microcalcifications are round, homogeneous, isodense and monomorphous. These microcalcifications do not look like milk or calcium calcifications, because of their round shape on the ML view. If they are recently detected, it is recommended to perform a short follow-up at 6, 12, 24 and 48 months to insure of their sta- bility. They are classified in the BIRADS TM 3 category (Fig. 4). ∗ Corresponding author. Tel.: +33 1 42 11 60 74; fax: +33 1 42 11 52 79. E-mail address: [email protected] (C. Balleyguier). An oval, homogeneous mass is visible in the right breast. Contours are well circumscribed and lobulated (arrow). Ultra- sonography showed an homogeneous solid mass. Because of the solid content, the classification is BIRADS TM 3. The first follow-up should be performed 4 months later, conversely to microcalcifications (Fig. 5). An extended area of thin and amorphous microcalcifications is visible in the upper and outer quadrant of the left breast (arrows). These microcalcifications were stable since 5 years. The BIRADS TM category is BIRADS TM 4 and as the calcifica- tions are not evolutive, the attended result is benign: BIRADS TM 4a. Vacuum macrobiopsy revealed benign lobular microcalcifi- cations (Fig. 6). This oval mass is partially well circumscribed. The inferior border of the mass is indistinct (ill-defined) (arrow). Ultrasound showed a solid, homogeneous mass. Because of the contours, the mass is categorized in BIRADS TM 4b. A biopsy is recommended and the radiologist has to compare the histologic results to the mammographic features. Ultrasound guided biopsy revealed a cellular adenofibroma (Fig. 7). An architectural distorsion is visible in the upper and outer quadrant of the right breast (arrows). Ultrasound was normal. This image is suspicious of malignancy and can be classified as BIRADS TM 4c. Stereotactic biopsy revealed a 7 mm DIC (Fig. 8). A cluster of microcalcifications is visible in the upper quad- rant of the left breast. Microcalcifications are homogenous and some look like milk calcifications (arrows). Categorization is 0720-048X/$ – see front matter © 2006 Published by Elsevier Ireland Ltd. doi:10.1016/j.ejrad.2006.08.034
-
Upload
betty-romero-barrios -
Category
Documents
-
view
213 -
download
0
description
X
Transcript of Download

A
ac©
K
1c
ctTm
lsbB
Tnc
Amov
sb
0d
European Journal of Radiology 61 (2007) 195–201
BIRADSTM mammography: Exercises
Corinne Balleyguier a,∗, Francois Bidault a, Marie Christine Mathieu b, Salma Ayadi a,Dominique Couanet a, Robert Sigal a
a Radiology Department, Institut de Cancerologie Gustave-Roussy, 39 rue Camille Desmoulins, 94805 Villejuif Cedex, Franceb Biopathology Department, Institut de Cancerologie Gustave-Roussy, 94805 Villejuif, France
Received 18 August 2006; received in revised form 21 August 2006; accepted 24 August 2006
bstract
Some radiological cases are presented in this article to train the reader to the BIRADSTM classification in mammography. Each case is describedccording to the fourth American version of the BIRADSTM lexicon. Some classifications difficulties will also be presented, in order to show theomplexity and the observer variability, commonly encountered in BIRADSTM 3 and 4 categories.
2006 Published by Elsevier Ireland Ltd.
; Train
Cstfm
i(Tt4c
bsmamc
eywords: BIRADSTM classification; BIRADSTM 3 category; Mammography
. Illustrating cases of BIRADSTM mammographylassification
An oval shape mass is visible on this view. Contours are wellircumscribed (arrows), a mixed content with fat and glandularissue is visible within the mass. The diagnosis is an hamartoma.his is a typical example of the BIRADSTM 2 classification inammography. No further examination is necessary (Fig. 1).Macrocalcifications are dense, linear and needle-shape, fol-
owing the ducts and oriented toward the nipple, which is veryuggestive of a plasma cell mastitis (arrows). This a typicallyenign disease of the breast which can be classified in theIRADSTM 2 category (Fig. 2).
Multiple round calcified masses are visible in the right breast.he peripheral calcifications are typical of calcified fibroade-oma. No further examination is necessary. BIRADSTM 2ategory (Fig. 3).
This view shows at least three microcalcifications clusters.ll microcalcifications are round, homogeneous, isodense andonomorphous. These microcalcifications do not look like milk
r calcium calcifications, because of their round shape on the MLiew.
If they are recently detected, it is recommended to perform ahort follow-up at 6, 12, 24 and 48 months to insure of their sta-ility. They are classified in the BIRADSTM 3 category (Fig. 4).
∗ Corresponding author. Tel.: +33 1 42 11 60 74; fax: +33 1 42 11 52 79.E-mail address: [email protected] (C. Balleyguier).
qTa(
rs
720-048X/$ – see front matter © 2006 Published by Elsevier Ireland Ltd.oi:10.1016/j.ejrad.2006.08.034
ing; Microcalcifications; Breast
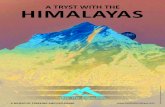
An oval, homogeneous mass is visible in the right breast.ontours are well circumscribed and lobulated (arrow). Ultra-
onography showed an homogeneous solid mass. Because ofhe solid content, the classification is BIRADSTM 3. The firstollow-up should be performed 4 months later, conversely toicrocalcifications (Fig. 5).An extended area of thin and amorphous microcalcifications
s visible in the upper and outer quadrant of the left breastarrows). These microcalcifications were stable since 5 years.he BIRADSTM category is BIRADSTM 4 and as the calcifica-
ions are not evolutive, the attended result is benign: BIRADSTM
a. Vacuum macrobiopsy revealed benign lobular microcalcifi-ations (Fig. 6).
This oval mass is partially well circumscribed. The inferiororder of the mass is indistinct (ill-defined) (arrow). Ultrasoundhowed a solid, homogeneous mass. Because of the contours, theass is categorized in BIRADSTM 4b. A biopsy is recommended
nd the radiologist has to compare the histologic results to theammographic features. Ultrasound guided biopsy revealed a
ellular adenofibroma (Fig. 7).An architectural distorsion is visible in the upper and outer
uadrant of the right breast (arrows). Ultrasound was normal.his image is suspicious of malignancy and can be classifieds BIRADSTM 4c. Stereotactic biopsy revealed a 7 mm DIC
Fig. 8).A cluster of microcalcifications is visible in the upper quad-ant of the left breast. Microcalcifications are homogenous andome look like milk calcifications (arrows). Categorization is

196 C. Balleyguier et al. / European Journal of Radiology 61 (2007) 195–201
Fig. 1. 53-Year-old woman. No palpable mass. Cranio-caudal (CC) view of theleft breast. Hamartoma.
Fig. 2. 55-Year-old woman. Medio-lateral (ML) view of the right breast. Plasmacell mastitis.
Fig. 3. 60-Year-old women. ML view of the right breast. Multiple calcifiedfibroadenoma.
Fig. 4. 45-Year-old woman. Magnification ML view of the right breast. Lobularbenign microcalcifications.
C. Balleyguier et al. / European Journal of Radiology 61 (2007) 195–201 197
Fn
Fig. 7. 53-Year-old woman. Spot compression view of the left breast. Adenofi-broma.
ig. 5. 48-Year-old woman. Spot compression view of the right breast. Ade-
ofibroma.Fig. 6. 72-Year-old woman. CC (a) and ML (b) vie
ws of the left breast. Lobular calcifications.
198 C. Balleyguier et al. / European Journal of Radiology 61 (2007) 195–201
Fh
Fig. 8. 69-Year-old woman. CC (a) and MLO (b) views o
ig. 9. 53-Year-old woman. Magnification view of the left breast. Typical ductalyperplasia.
Fc
f the right breast. Ductal invasive carcinoma (DIC).
ig. 10. 55-Year-old woman. Magnification view of the right breast. Ductalarcinoma in situ (DCIS).

C. Balleyguier et al. / European Journal of Radiology 61 (2007) 195–201 199
b) views of the left breast. Ductal invasive carcinoma.
Bbma
tdB
it
(r
2
cbg
tssmp(
Fig. 11. 47-Year-old woman. CC (a) and MLO (
IRADSTM 4b due to the linear distribution. Biopsy revealedenign microcalcifications, with typical ductal hyperplasia. A 6onths follow-up mammogram is recommended in this case to
void false negative cases of biopsy (Fig. 9).Multiple dense, irregular and heterogeneous microcalcifica-
ions in a microcalcifications cluster. Due to the localized roundistribution, the final classification is not BIRADSTM 5 butIRADSTM 4c. Biopsy revealed a DCIS (Fig. 10).
A 15 mm spiculated mass (arrows) is visible in the inner andnferior part of the left breast. The mammographic features areypically malignant: BIRADSTM 5 (Fig. 11).
Typically malignant fine linear branching microcalcificationsarrows) are suggestive of malignancy: BIRADSTM 5. Biopsyevealed a DCIS (Fig. 12).
. Difficult cases
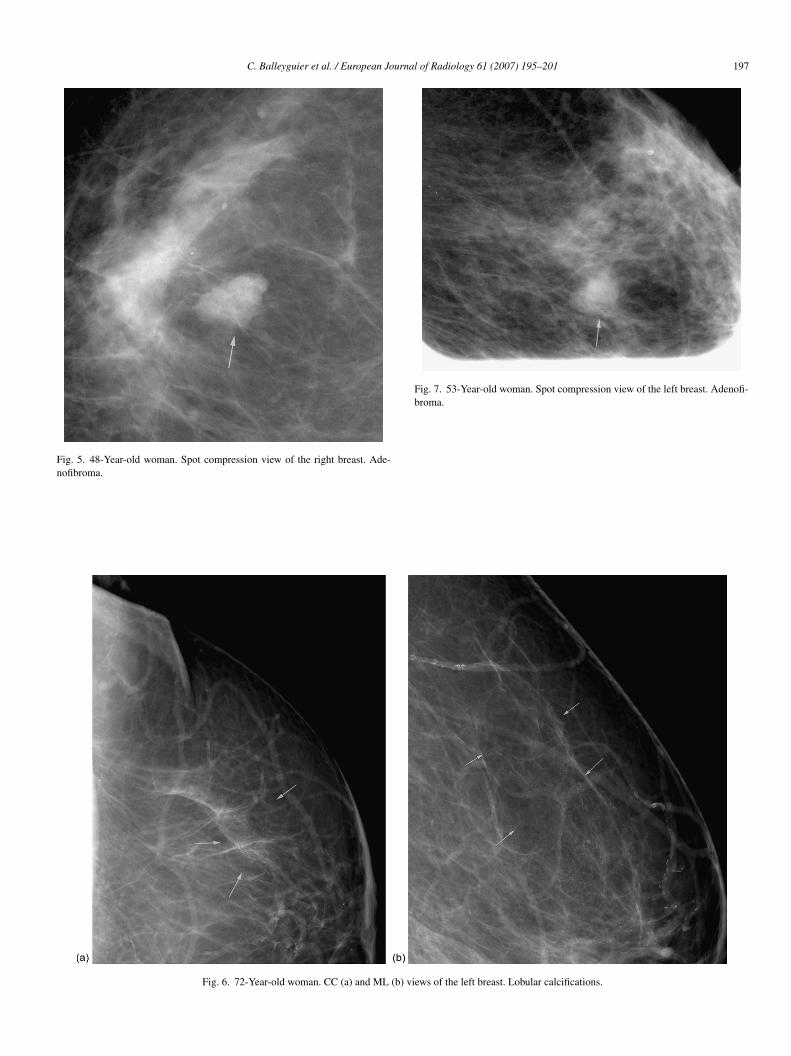
Multiple amorphous microcalcifications are suspicious in thisase due to pleomorphism (arrows): BIRADSTM 4b. Macro-iopsy revealed only benign microcalcifications and atrophiclandular tissue. No surgery was performed (Fig. 13).
An ill-defined mass is visible in the outer quadrant ofhe right breast (arrow, Fig. 14a): BIRADSTM 4b. Ultra-
onography confirmed the suspicious features of this lesion:olid content, microlobulated mass but a posterior enhance-ent is visible. Biopsy (Fig. 14c) revealed a benign lesion,seudo-tumoral adenosis, with multiple round epithelial cellsarrows) which can be frequently misdiagnosed as a breast F
ig. 12. 52-Year-old woman. Magnification view of the right breast. DCIS.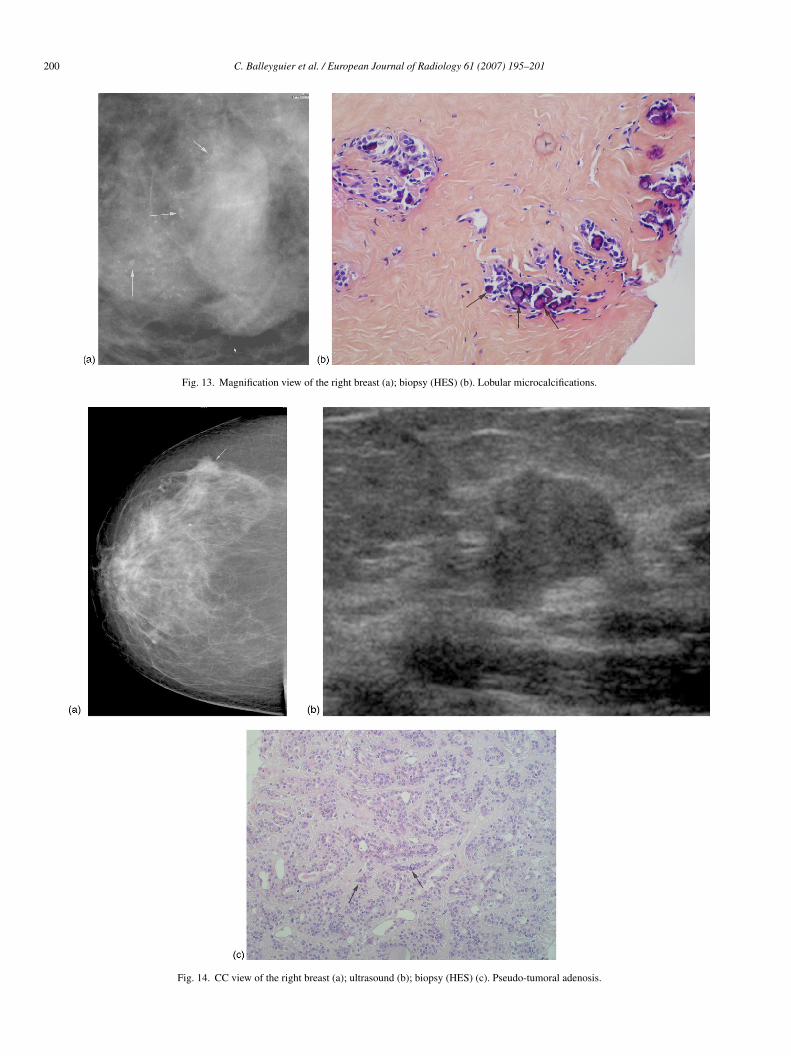
200 C. Balleyguier et al. / European Journal of Radiology 61 (2007) 195–201
Fig. 13. Magnification view of the right breast (a); biopsy (HES) (b). Lobular microcalcifications.
Fig. 14. CC view of the right breast (a); ultrasound (b); biopsy (HES) (c). Pseudo-tumoral adenosis.

C. Balleyguier et al. / European Journal of Radiology 61 (2007) 195–201 201
on vie
ca
e
p
cdensity: BIRADSTM 4c.
Fig. 15. ML view of the left breast (a); magnificati
arcinoma on mammogram. In this case, biopsy could not bevoided.
Typically benign, milk microcalcifications are visible in thentire breast (arrowheads, Fig. 15a): BIRADSTM 2.
A different cluster of microcalcifications is visible in theosterior inferior quadrant of the left breast (arrows). These cal-
co
w (b). DCIS and diffuse milk microcalcifications.
ifications are suspicious due to the irregular shape and high
When there are two types of microcalcifications, the finalategory is the most suspicious. In this case, a biopsy was rec-mmended and revealed a DCIS.