Douglas Johnson, ATC, EES, CLS Vice President, Clinical and Scientific Affairs Multi Radiance...
57
Douglas Johnson, ATC, EES, CLS Vice President, Clinical and Scientific Affairs Multi Radiance Medical Low Back Pain and Low Back Pain and MODALITIES MODALITIES
-
Upload
pamela-wood -
Category
Documents
-
view
213 -
download
0
Transcript of Douglas Johnson, ATC, EES, CLS Vice President, Clinical and Scientific Affairs Multi Radiance...

Douglas Johnson, ATC, EES, CLSVice President, Clinical and Scientific Affairs
Multi Radiance Medical
Low Back Pain and Low Back Pain and MODALITIESMODALITIES
Douglas Johnson, ATC, EES, CLSVice President, Clinical and Scientific Affairs
Multi Radiance Medical

Discuss the quality of literature available for the use of modalities in spinal care
Compare various types of commonly used modalities
Introduce new modalities and treatment concepts
LAB: Demonstrate and administer protocols for low level laser therapy
Integration of:◦ Best Research Evidence◦ Clinical Expertise◦ Patient Values
BestResearch Evidence
ClinicalExpertise
PatientValues

Inherent Problems◦ Lack of sound evidence◦ Little or no clinical experience
and/or expertise◦ Patient does not “want” it
Theory vs. Evidence
BestResearch Evidence
ClinicalExpertise
PatientValues

Interventions◦ Massage◦ Thermal Therapy◦ Electrical Stimulation◦ EMG Biofeedback◦ TENS◦ Ultrasound◦ Therapeutic Exercise◦ Combination Therapy
Outcome Measures◦ Functional Status◦ Pain◦ Ability to Work◦ Patient Global Improvement◦ Patient Satisfaction◦ Quality of Life
Time Frames◦ Acute◦ Sub-Acute◦ Chronic◦ Post-Surgical
Acute Low Back Pain (<4 weeks)◦ Ultrasound – 1 Non-randomized Controlled Trial
Continuous US vs. Placebo No evidence to include or exclude alone
◦ TENS – 1 RCT 15 minutes of High Frequency, 15 minutes of AL TENS No evidence to include or exclude alone
◦ E-Stim, Massage, Thermotherapy, Biofeedback Insufficient Data available
Sub-Acute Low Back Pain (4-12 weeks)◦ No data to evaluate effectiveness or efficacy of modalities

Chronic Low Back Pain (>12 weeks)◦ Ultrasound – One RCT
Continuous US vs. placebo No difference in pain improvement after 1 month No other data reported
◦ TENS – Four Controlled Clinical Trials 2 trials used high frequency, 2 trials used low frequency No difference in pain improvement at 1-month post therapy No other data reported
◦ Biofeedback – Five RCT’s No effect on pain relief, functional status, or ROM after 1 month of
therapy

RCT – Manipulative Therapy vs. Interferential Therapy vs. Combination for Acute LBP◦ 240 Subjects◦ Outcome Measures
Roland Morris Disability Questionnaire VAS Pain Rating SF-36 Questionnaire Pain Medication Consumption
◦ Methods Manipulative Therapy vs. Pre-Modulated IFC vs. Combination
Therapy Average of 5 treatments over 5 weeks

Results◦ All subjects in all groups scored significantly “higher” at
discharge, 6 months post-treatment, and 12 months post-treatment as compared with pre-treatment
◦ No significant differences between groups at any data point post-treatment

RCT – IFT to painful area vs. IFT to Spinal Nerve vs. Control◦ 60 subjects with acute LBP◦ Outcome Measures
Pain Rating Index Roland-Morris Disability Questionnaire EuroQol
◦ Methods All subjects received educational material “The Back Book” 3.85kHz carrier frequency, 140Hz “beat frequency” continuous, 30
minutes duration of treatment – altered method of application Testing pre-treatment, at discharge, and at 3-months post-treatment

Results◦ All subjects displayed improvement at outcome measurement
periods post-treatment◦ Subjects receiving spinal nerve IFT displayed statistically
significant reduction in disability compared with painful area IFC and control

Large RCT◦ Various modalities for
Cervical Myofascial Pain and Trigger Point Sensitivity
◦ Multiple combinations of commonly used modalities/techniques TENS 100Hz, 250μs,
“strong but comfortable” 20 minutes
Results ◦ Significant pain relief
TENS + ischemic compression
TENS + hot pack + AROM IFC + hot pack + AROM

TENS vs. NMES vs. TENS + NMES for chronic back pain◦ TENS = 100Hz, 100μs “strong but comfortable”◦ NMES = 5sec on/15sec off, 70 Hz, 200μs
Alternated three 10 min periods of NMES with two 130min periods of no Rx◦ Combined TENS and NMES
Alternated one 10 minutes and two 20 minute periods of NMES with three periods of TENS
◦ All three groups received 5 hours/day for 2 days Subjects had 2 days between each modality
Results◦ Combined NMES/TENS produced best effects
Pain relief/reduction◦ TENS better than NMES alone for pain reduction

Treatment =+ hot packs+ EMS+ ultrasound+ massage+ exercise+ mobilization+ cold packs+ …
Over 3000 published articles on light therapy
Over 170 randomized, double blind studies
200 studies are added each year to PubMed

Acute Low Back Pain with Radiculopathy: A Double-Blind, Randomized, Placebo-Controlled Study.
acute low back pain (LBP) with radiculopathy. randomized, double-blind, placebo-controlled trial of 546 patients. outcomes were VAS; lumbar movement, with a modified Schober test;
Oswestry disability score; and SF-12 Subjects were evaluated before and after treatment. Statistically significant differences were found in all outcomes measured The results of this study show better improvement in acute LBP treated
with LLLT used as additional therapy.

Hurwitz and Carragee, Et AllFor WAD, educational videos, mobilization, and
exercises appear more beneficial than usual care or physical modalities; for other neck pain, the evidence suggests that manual and supervised exercise interventions, low-level laser therapy, and perhaps acupuncture are more effective than no treatment, sham, or alternative interventions. However, none of the active treatments is clearly superior to any other in the short- or long-term.

Efficacy of low-level laser therapy in the management of neck pain: a systematic review and meta-analysis of randomized placebo or active-treatment controlled trials
identified 16 randomized controlled trials including a total of 820 patients. In acute neck pain, results of two trials showed a relative risk (RR) of 1·69 (95%
CI 1·22—2·33) for pain improvement of LLLT versus placebo. Five trials of chronic neck pain reporting categorical data showed an RR for pain improvement of 4·05 (2·74—5·98) of LLLT. Patients in 11 trials reporting changes in visual analogue scale had pain intensity reduced by 19·86 mm (10·04—29·68).
Seven trials provided follow-up data for 1—22 weeks after completion of treatment, with short-term pain relief persisting in the medium term with a reduction of 22·07 mm (17·42—26·72).
Side-effects from LLLT were mild and not different from those of placebo. LLLT reduces pain immediately after treatment in acute neck pain and up to 22
weeks after completion of treatment in patients with chronic neck pain.

Theory Vs. Evidence◦ While there may be inadequate evidence to support the use
or non-use of a given modality, one must remember the theoretical model which caused one to consider the modality in the first place
Clinical Expertise vs. Best Research Evidence◦ If best evidence falls outside of clinical expertise, one must
defer to the weaker or refer to the stronger To Use or Not to Use
◦ When in doubt, trust your clinical judgment over a single study


Laser Therapy Electrical Stimulation Ultrasound
Equipment Type Corded base unit console with cluster probeOrCordless (portable)
Corded base unit console with leadsOrTENS, NMES, IFC (Portable)
Corded base unit console with transducerOrCordless (portable)
Accessories Needed: None Disposable Electrodes Transmission Gel
Applications per day Up to 4 treatments in a given day
1 treatment per day No more than one per day
Tissues Affected: Absorbed by all tissues including skin, subcutaneous, tendons, bone, muscles, nerves and blood
Effects on muscles and nervous system
Absorbed only by white connective tissue

Laser Therapy Electrical Stimulation Ultrasound
Patient Restrictions: Safe to use with children, adults and elderly, safe to use with patient with circulatory and nerve impairments. Do not use over suspicious or cancerous lesions, pregnant women
Potential for burns and blisters. Not for use with patient with circulation or neuropathy conditions, pacemakers, cancer, pregnancy or thrombophlebitis, and fractures
Potential for over-heating and damage caused by burns. Not for use with patients with circulation or neuropathy conditions, pacemakers and cancer, or pregnant women, infection, acute injury, (CW) epiphyseal areas, over the eyes, and fractures
Laser Therapy Electrical Stimulation Ultrasound
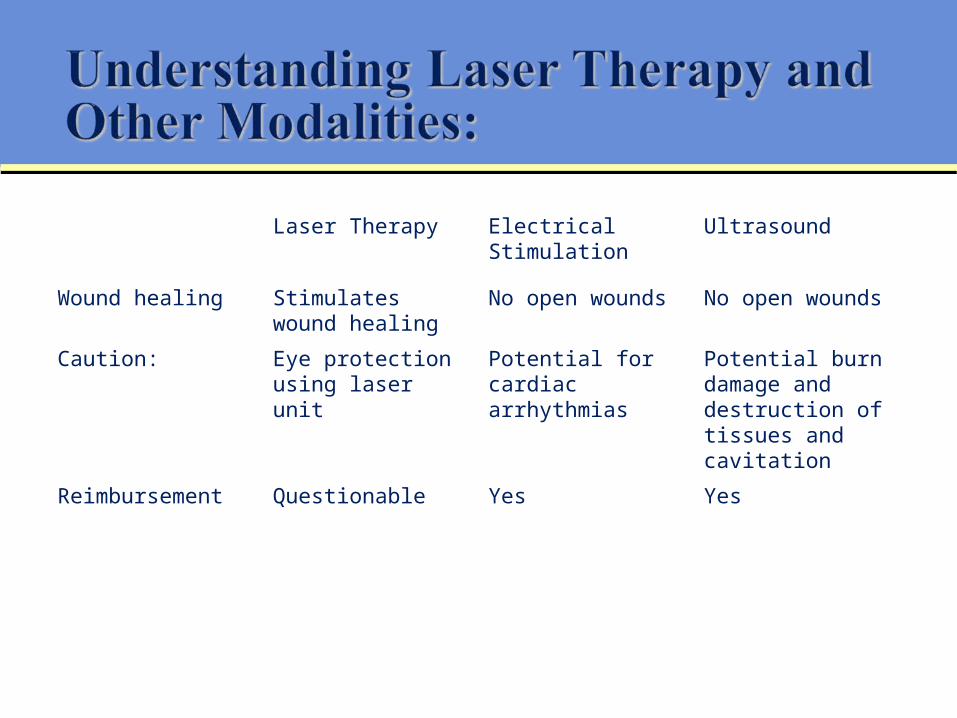
Wound healing Stimulates wound healing
No open wounds No open wounds
Caution: Eye protection using laser unit
Potential for cardiac arrhythmias
Potential burn damage and destruction of tissues and cavitation
Reimbursement Questionable Yes Yes

Assessment of cytoskeleton and endoplasmic reticulum of fibroblast cells subjected to low-level laser therapy and low-intensity pulsed ultrasound.
compare the effect of low-level laser therapy (LLLT) and low-intensity pulsed ultrasound (LIPUS) on the cytoskeleton and endoplasmic reticulum
Each group was irradiated at 24-h intervals, with the following post-treatment incubation times: 24, 48, and 72 h.
The effects were evaluated by the use of fluorescent probes and with fluorescence microscopy analysis.
both LLLT and LIPUS promote changes on the cellular level. LIPUS revealed increased reticulum activity and increased protein synthesis LLLT organized actin filaments better than LIPUS.

The Effectiveness of Conservative Treatments of Carpal Tunnel Syndrome: Splinting, Ultrasound, and Low-Level Laser Therapies.
Abstract Objective: investigate the effectiveness of splinting, ultrasound (US), and low-level laser (LLL) in the management of CTS.
Materials and Methods: 100 hands of 50 women patients with bilateral CTS at 3 months post treatment, three groups, splinting only, splinting + US, and splinting + LLLT. Patients were assessed with the Boston Questionnaire, patient satisfaction inquiry, visual analogue scale for pain, and electroneuromyography.
Results and Conclusion: combinations of US or LLLT with splinting were more effective than splinting alone in treating CTS. However, LLLT + splinting was more advantageous than US + splinting, especially for the outcomes of lessening of symptom severity, pain alleviation, and increased patient satisfaction.
Cryotherapy◦ Use laser therapy after due to vasoconstriction, it increases penetration
Heat therapies (US- HP)◦ Use laser therapy before, increased blood flow causes increased
absorption of light by hemoglobin resulting in decreased penetration Electrical (EMS, TENS)
◦ Use laser therapy before (or during if LaserStim), increased blood flow causes increased absorption of light by hemoglobin
Phono / Iontophoresis◦ Use before steroid or anti-inflammatory agents, this modality lessens
the cellular effects of laser therapy Manipulations
◦ May do before or after, depending on the specific goals of laser therapy

Treat patients that other modalities can not: Pacemakers Implants - metal, joints, plastic Over boney prominences Peripheral vascular disease with decreased sensation When heat is contraindicated (if low level laser and
super-pulsed only)

Absolute Contraindications: Pregnancy Carcinoma Fever (body temperature higher than 38°c) Over hemorrhages

Considerations: Anti-inflammatory medications Steroid Injections Photosensitive Patients
Other Considerations: Wounds – ensure wound are completely cleaned from any topical applications and
debrided prior to treatment Anticoagulants Tattoos Chronic musculoskeletal localized inflammation

What is Low Level Laser Therapy?
Understanding the parameters of laser therapy devices?
Optimal dosimetry for treatment of the spine

In 2003 North American Association of Laser Therapy (NAALT) adopted the terms Phototherapy or Photobiomodulation (PBM)
PHOTOTHERAPY is:A therapeutic physical modality using photons of light from the visible red to the infrared spectrum for tissue healing and pain reduction, including five (5) different technologies:
Low level lasersNon coherent narrow band light diodesNon coherent broad band light diodesPolarized lightPhotodynamic therapy

High Powered Lasers◦ Heat tissue ◦ Greater than 500 mW ◦ Vaporize, coagulate and cut
Low Level Lasers◦ Minimal heating of tissue◦ Less than 500 mW of power◦ Photo-chemical and photo-physical effects
TQ Solo Portable
Energy density Wavelength Schedule of treatments Treatment technique Dose
Pro Sport Package

Misconceptions about Laser Therapy: How to improve clinical and business outcomes through New Hybrid Technology
Technology Advancements in Laser Therapy - Hybrid Solutions for Clinical Applications". Energy density (Power)
Wavelength Schedule of treatments
http://www.multiradiance.com

“…applying a modality incorrectly is akin to not doing it at all…”








“…administering the optimal dose, each and every time, is the most difficult task of all…”

It should be noted that work by Dr. Tina Karu has shown that the biological response to laser stimulation can be significantly different according to the frequency in which different wavelengths are applied, and even non-existent if two or more continuous wavelengths are used simultaneously.

Laser Type Location Points Dose CommentContinuous Cervical spine 2-4 15 Joules Minimum 6
Joules per point
Super Pulsed
Cervical spine 1 500 – 1000 Hz 2 minutes
Minimum 30 seconds per point
Continuous Lumbar spine 2-4 40 Joules Minimum 8 Joules per point
Super Pulsed
Lumbar spine 3 500 – 1000 Hz 2 minutes
Minimum 30 seconds per point

Laser Type Location Points Dose CommentContinuous Cervical
paraspinals2-4 15 Joules Minimum 6
Joules per point
Super Pulsed
Cervical paraspinals
1 2 Joules or500 – 1000 Hz 2 minutes
Minimum 30 seconds per point
Continuous Lumbar paraspinals
2-4 15 Joules Minimum 8 Joules per point
Super Pulsed
Lumbar paraspinals
3 2 Joules500 – 1000 Hz 2 minutes
Minimum 30 seconds per point

Laser Type Location Points Dose CommentContinuous Spinous
process (laterl to affected side)
1-3 Up to 30 Joules
Minimum 15 Joules per point
Super Pulsed
Spinous process (laterl to affected side)
1-3 5 Joules or500 – 1000 Hz 3 minutes
Minimum 2 minutes per point
Continuous Transverse process (associated side)
1-3 Up to 30 Joules
Minimum 8 Joules per point
Super Pulsed
Transverse process (associated side)
1-3 2 Joules5-250 Hz 2 minutes
Minimum 30 seconds per point

Laser Type Location Points Dose CommentContinuous Spinous
process (laterl to affected side)
1-3 Up to 30 Joules
Minimum 15 Joules per point
Super Pulsed
Spinous process (laterl to affected side)
1-3 5 Joules or500 – 1000 Hz 3 minutes
Minimum 2 minutes per point
Continuous Transverse process (associated side)
1-3 Up to 30 Joules
Minimum 8 Joules per point
Super Pulsed
Transverse process (associated side)
1-3 2 Joules5-250 Hz 2 minutes
Minimum 30 seconds per point
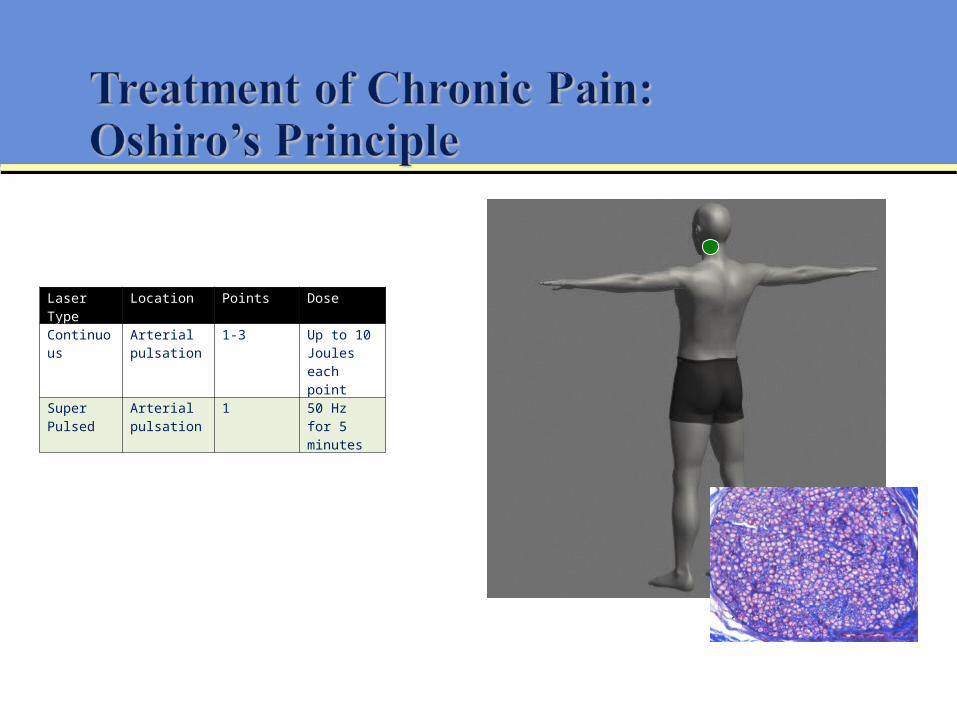
Laser Type Location Points DoseContinuous Arterial
pulsation1-3 Up to 10
Joules each point
Super Pulsed
Arterial pulsation
1 50 Hz for 5 minutes

A measurable goal indicating a positive result in the treatment of an injury/illness from exposure to laser therapy
Be prepared to increase dose to achieve desired response in 1 min increments

An exacerbation of a condition/illness resulting from an overexposure of laser therapy
Decrease treatment dosage by 1 min increments if patient experiences a treatment reaction
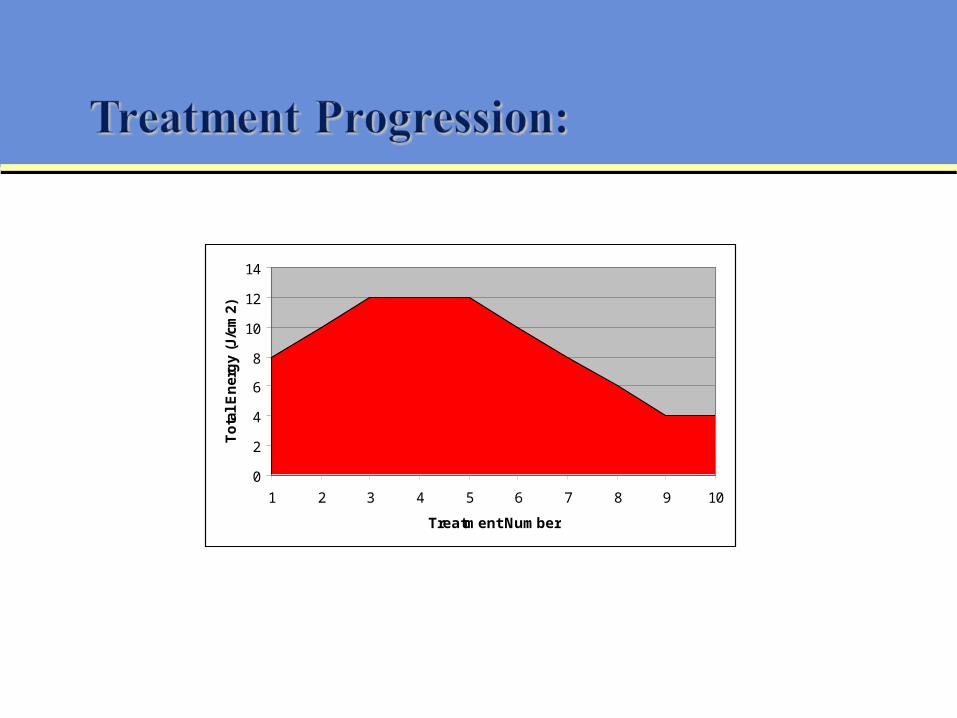
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 10
Treatment Number
To
tal
En
erg
y (J
/cm
2)

LaserStim™ detects “biological information" from the body and, using an "adaptive biofeedback loop", establishes an "interactive dialog" with the body
The body controls LaserStim™ therapy via various, complex changes in skin impedance, or the “interactive dialog".
The LaserStim™ provides feedback by the color change of the LED indicator and audible beeps indicating the optimal treatment target.
Light TherapyLight Therapy
Electrical StimulationElectrical Stimulation