
International accounting Modulo 1 Dott.ssa Antonella Portalupi.
Upload
karly-charlesworthCategory
view
226download
0
Dott.ssa Pamela GuglielminiDott.ssa Pamela Guglielmini
Prof. Francesco BoccardoProf. Francesco Boccardo
USA – SEER 2008 182,000 new cases of
breast cancer 83,000 women would
develop metastatic disease 46,000 women would die
of metastatic breast cancer
The dimension of the problem

Advanced Breast Cancer: Heterogeneous Population Requires Tailored Treatments
Symptomatic/ poor PS Palliation
Elderly/indolent disease/poor PS Improve TTP &
QoL
Amenable to locoregional control Increase
response rate
Young/good PS visceral mts Prolong survival
Characteristics Treatment Objectives
Is metastatic breast cancer a
curable disease?
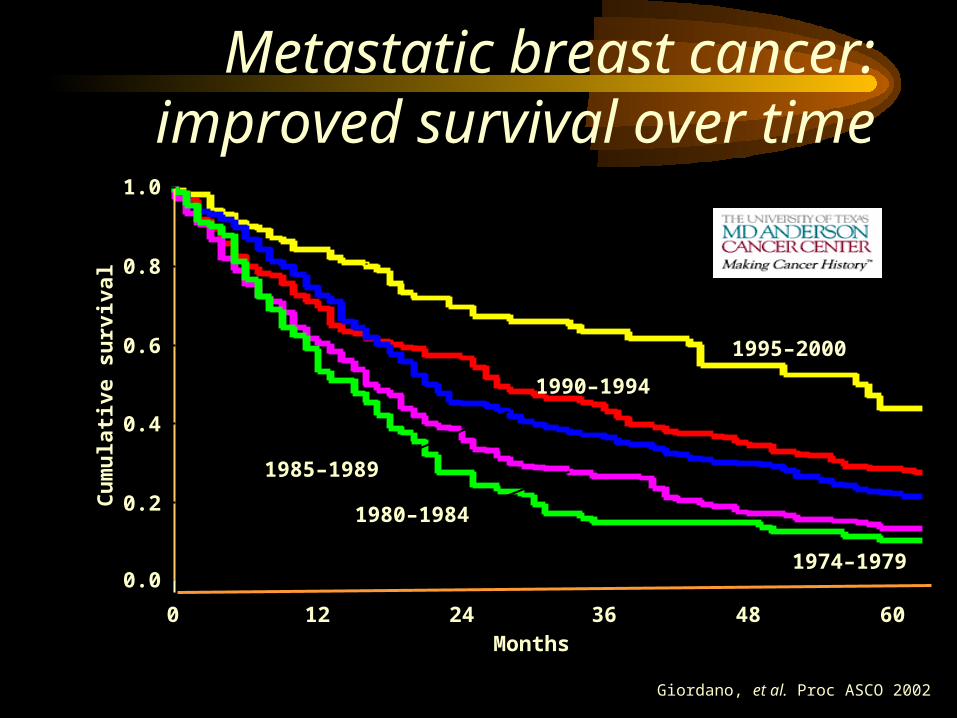
Metastatic breast cancer:improved survival over time
Giordano, et al. Proc ASCO 2002
Months60483624120
Cu
mu
lati
ve s
urv
ival
1.0
0.8
0.6
0.4
0.2
0.0
1995–2000
1990–1994
1985–1989
1980–1984
1974–1979
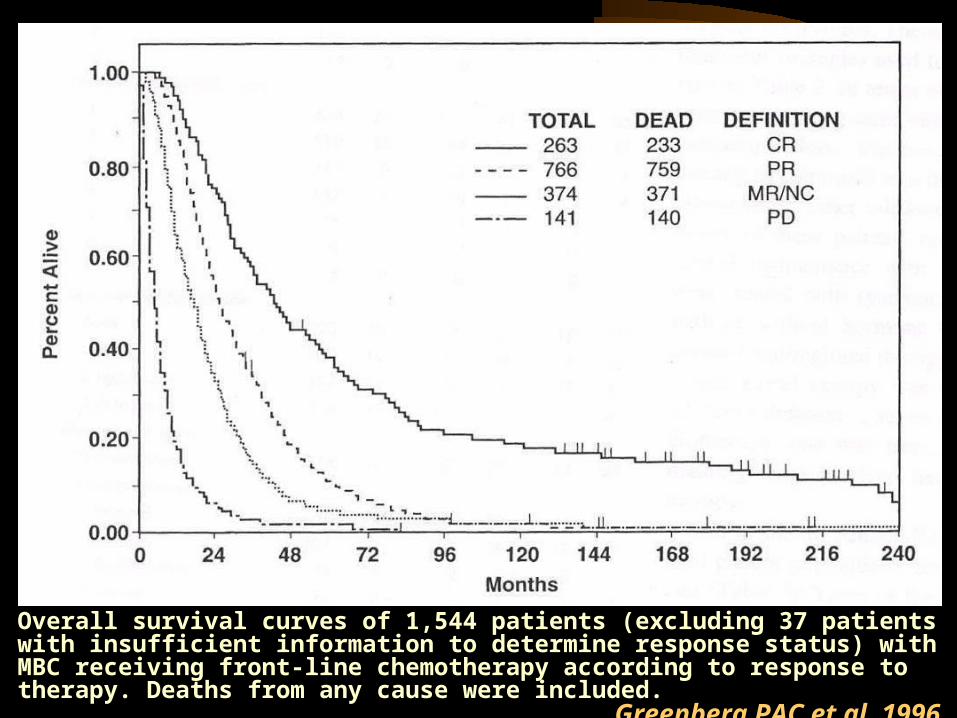
Overall survival curves of 1,544 patients (excluding 37 patients with insufficient information to determine response status) with MBC receiving front-line chemotherapy according to response to therapy. Deaths from any cause were included.
Greenberg PAC et al, 1996

Symptoms palliation Quality of life improvement Survival prolongation
Objective tumor response is correlated with each of the previous one
Which end points can be achieved in all other
patients?
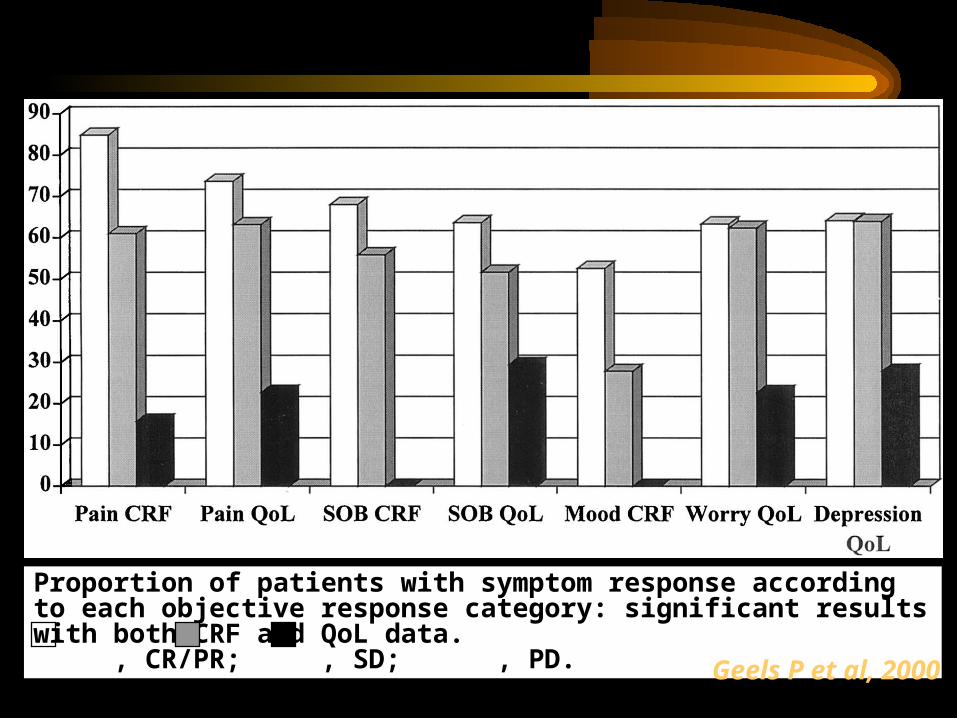
Proportion of patients with symptom response according to each objective response category: significant results with both CRF and QoL data. , CR/PR; , SD; , PD. Geels P et al, 2000
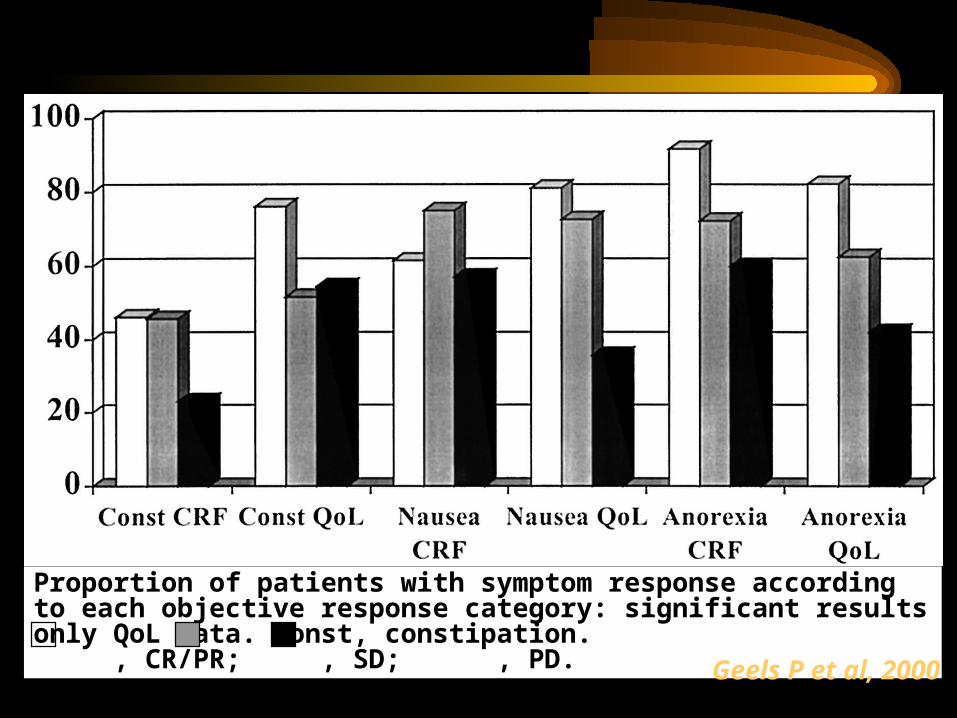
Proportion of patients with symptom response according to each objective response category: significant results only QoL data. Const, constipation. , CR/PR; , SD; , PD. Geels P et al, 2000
Hormone therapy Chemotherapy Biologicals Surgery/radiotherapy Analgesics Bisphosphonates Supportive care
(eritropoietin)
Which treatment options?

Patients characteristics: age/menopausal status Tumor characteristics:
DFI durationtumor burdendominant site of diseaseER/PgR statusprevious response to
endocrine therapy
Which patients are best candidate to
hormonetherapy?
Suppressive treatments Premenopause: ovariectomy, LH-
RHa Postmenopause: aromatase
inhibitors Competitive treatments Pre/postmenopause:
antiestrogens (TAM, TOR)
steroidal antiestrogen (Faslodex)
progestagensantiprogestins
Hormonetherapy: which drugs?
which sequences?

Invasive Breast Cancer by Age Invasive Breast Cancer by Age (Year 1998)(Year 1998)
Li CL et al. J Clin Oncol 2003,
1:28
5,8
18,3
23,421,0 21,0
10,3
0,0
5,0
10,0
15,0
20,0
25,0
20-39 40-49 50-59 60-69 70-79 80+
Premenopausal ≈ 25% - 30%
0
10
20
30
40
50
60
70
20-39 40-49 50-59 60-69 70-79 80+
ER-/PR-ER+/PR+ Other
Premenopausal, and HR+ ≈ 60%

Sir G.T. BEATSON Dr E. JENSEN

Mechanism of action of LHRHaMechanism of action of LHRHaFigure AFigure A- Hypersecretion of LH - Hypersecretion of LH
following acute following acute administration of LHRHaadministration of LHRHa
Figure BFigure B- Hyposecretion of LH - Hyposecretion of LH
following chronic following chronic administration of LHRHaadministration of LHRHa
LHRH
a
LHRH
a
LHRHaLHRHa
LHRHa
LHRHa
LH
RH
aL
HR
HaL
HR
Ha
LH
RH
a
LHRHa
LHRHa
LHRHaLHRHa
LHR
Ha
LHR
Ha
LH
RH
aL
HR
Ha
PituitaryPituitaryCellCell LHLH
LHR
Ha
LHR
Ha
LH
RH
a
LH
RH
a
LHRHaLHRHa
LHRHaLHRHa
LHRHa
LHRHa
LH
RH
aL
HR
Ha
LHRHaLHRHa
LHRH
a
LHRH
a
LHR
Ha
LHR
Ha
PituitaryPituitaryCellCell LHLH

Treatment response
Measurable diseaseGoserelin (n
29)Ovariectomy (n
30)Response No. % No. %CR 4 14 3 10PR 5 17 5 17Stable disease 8 28 8 26Increased disease 7 24 9 30Inadequate assessment
5 17 5 17
Taylor CW et al, 1998
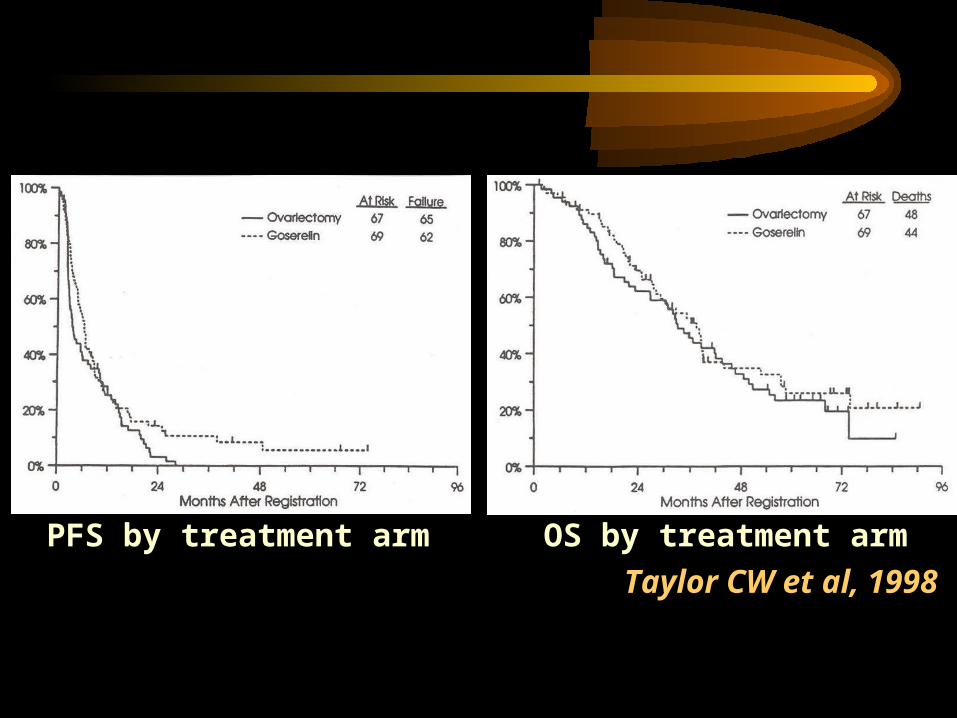
PFS by treatment arm OS by treatment armTaylor CW et al, 1998

Summary of results by treatment group
Endpoint LHRH-agonist alone
(n=256)
LHRH-agonist + tamoxifen (n=250)
Hazard Ratio/Odd
s Ratio (95% CI)
Log-rank p value
Primary median survival (yrs)
2.5 2.9 0.78(0.63-0.96)
0.02
Secondary median progression- free survival (mos)
5.4 8.7 0.70(0.58-0.85)
<0.001
Objective response (%)
29.7 38.8 0.67(0.46-0.96)
0.03
CHAT and EORTC meta-analysis, 1999
Combined use of Goserelin and Anastrozole as second-line endocrine treatment in pre menopausal women with advanced breast cancer. (Cheung et al, 2004)
16 women with M1 (13) or locally advanced primary breast cancer (3).
All previously treated with Z+T.
Clinical results: 75% OR/SD
Endocrine effects: mean E2 (pmol/L) Z+T (pre )= 224 Z+T (6 mos)= 24 Z+A (3 mos)= 6 Z+A (6 mos)= 5
Suppressive treatments Premenopause: ovariectomy, LH-
RHa Postmenopause: aromatase
inhibitors Competitive treatments Pre/postmenopause:
antiestrogens (TAM, TOR)
steroidal antiestrogen (Faslodex)
progestagensantiprogestins
Hormonetherapy: which drugs?
which sequences?

Structures of non-steroidal anti-oestrogens clinically available or in clinical trials.
Howell A et al, 1996

Results of studies using newer non-steroidal anti-oestrogens as first-line endocrine therapy for
advanced breast cancer
Drug Dose (mg/day)
No. of patients
Response CR/PR (%)
Toremifene [Valavaara, 1990] (Phase II trials summarised)
2060
240
149338
215268
Toremifene [Stenbygaard et al,
1993] (Phase III trial)
24040
3131
2944
Toremifene [Hayes et al, 1995]
60200
221212
2122
Tamoxifen (Phase III trial)
20 215 19
Droloxifene [Rauschning et al,
1994] (Randomised phase
II trial
2040
100
848896
304744
TAT-59 [Tominaga, 1995] (Randomised Phase II trail)
102040
151113
155531
Howell A et al, 1996
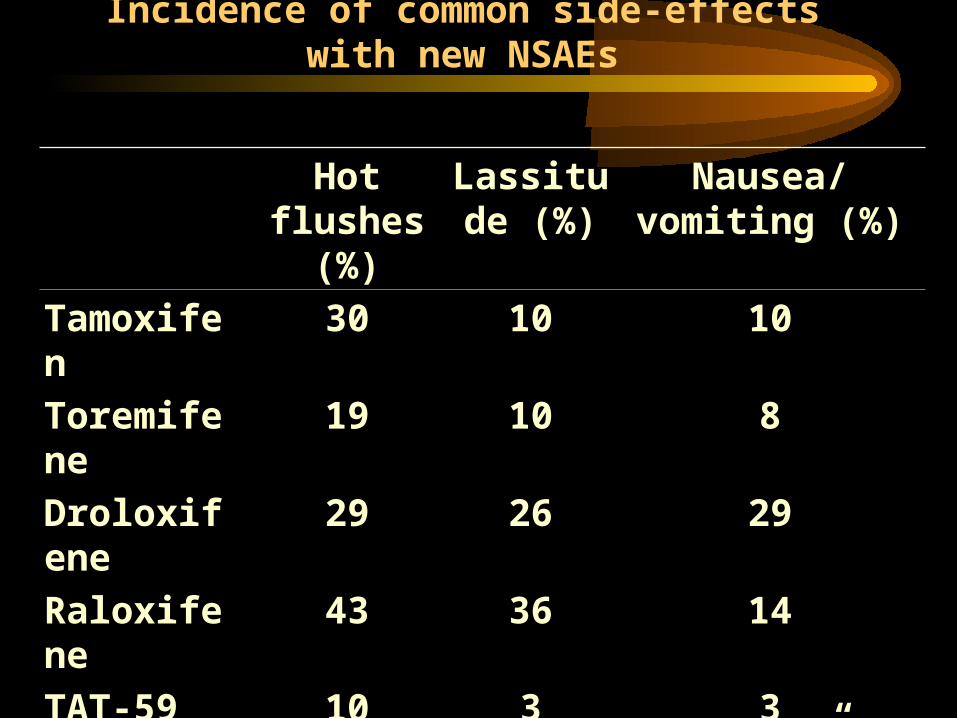
Incidence of common side-effects with new NSAEs
Hot flushes
(%)
Lassitude (%)
Nausea/vomiting (%)
Tamoxifen
30 10 10
Toremifene
19 10 8
Droloxifene
29 26 29
Raloxifene
43 36 14
TAT-59 10 3 3Idoxifene “similar to tamoxifen”
Howell A et al, 1996

Suppressive treatments Premenopause: ovariectomy, LH-
RHa Postmenopause: aromatase
inhibitors Competitive treatments Pre/postmenopause:
antiestrogens (TAM, TOR)
steroidal antiestrogen (Faslodex)
progestagensantiprogestins
Hormonetherapy: which drugs?
which sequences?
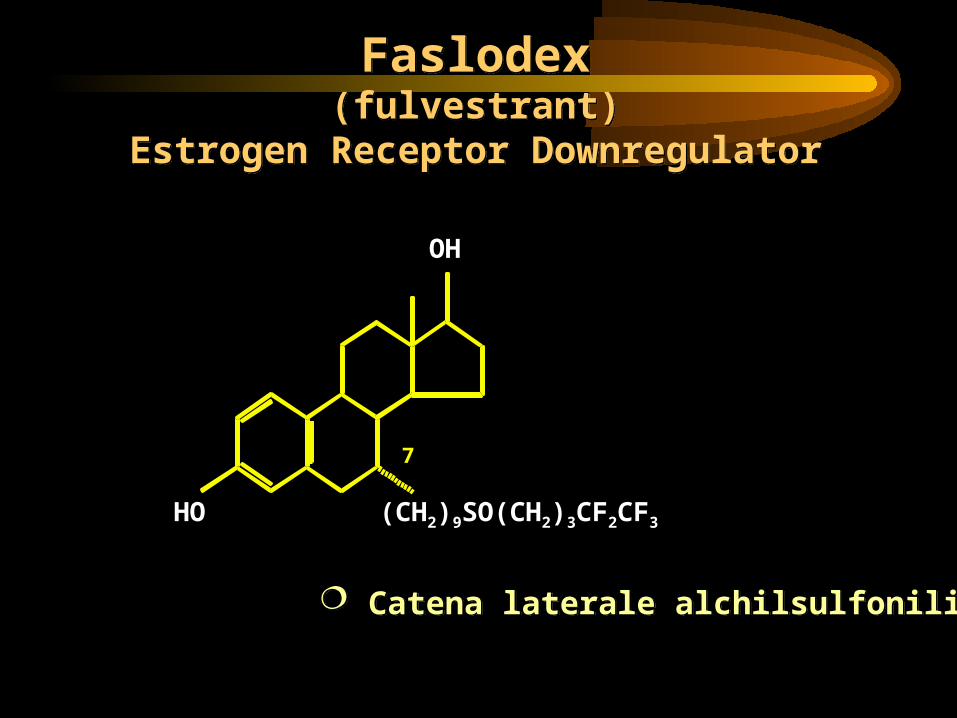
Faslodex(fulvestrant)
Estrogen Receptor Downregulator
Faslodex(fulvestrant)
Estrogen Receptor Downregulator
Catena laterale alchilsulfonilica Catena laterale alchilsulfonilica
OH
HO (CH2)9SO(CH2)3CF2CF3
7

ER: Interazione con estradiolo
estradiolo estradiolo+ER
Attivazione AF1 e AF2 Omodimerizzazione

ER: Interazione con Tamoxifene
Tamoxifene Dimerizzazione con solo AF1 attivato
Parziale trascrizione e legame con un solo coattivatore
Legame con RNA Pol.II e parziale trascrizione con riduzione prolif.cellulare
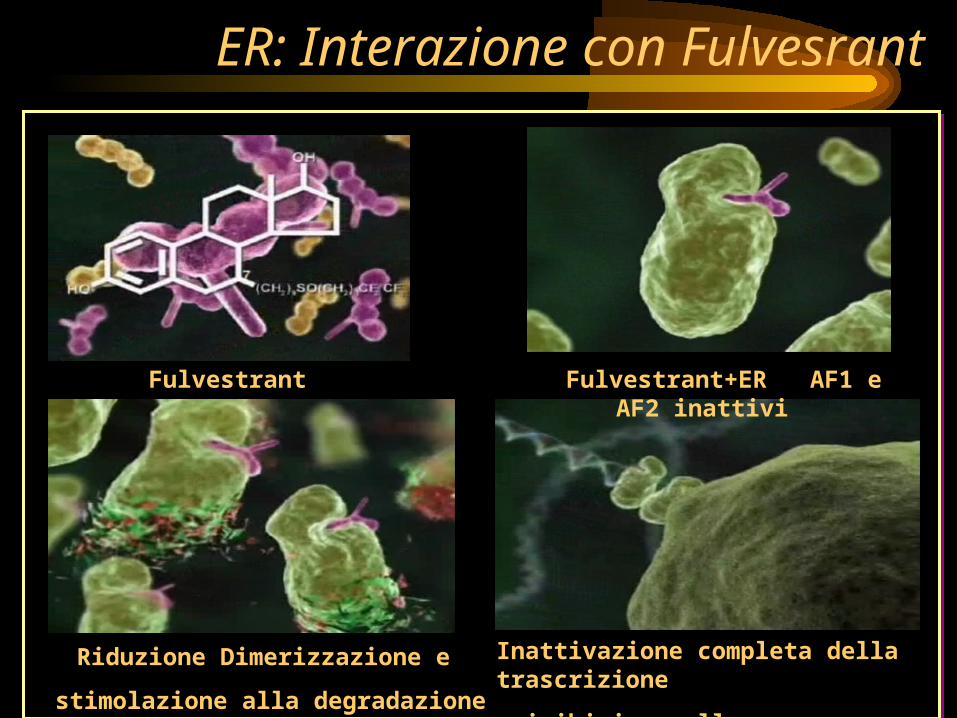
ER: Interazione con Fulvesrant
Fulvestrant Fulvestrant+ER AF1 e AF2 inattivi
Riduzione Dimerizzazione e
stimolazione alla degradazione ER
Inattivazione completa della trascrizione
e inibizione alla proliferazione cellulare

Howell A et al. Lancet 1995; 345: 29–30.
ICI 182,780 (‘Faslodex’): Phase II Results
Clinical Efficacy - Response RateResponse n %
Complete response 0 0Partial response 7 37Stable disease 6 32Progression 6 31
19 100
}69
69% of patients achieved OR or SD 24 weeks

2nd line Phase III Trial Designs Postmenopausal women with advanced breast cancer.
Prior HT for early or advanced breast cancer
Anastrozole 1mg daily orallyTrial 20: n=229Trial 21: n=194
Fulvestrant 250mg i.m. once monthlyTrial 20: 1 x 5ml (n=222)
Trial 21: 2 x 2.5ml (n=206)
Analysis after 340 eventsAnalysis after 340 events(progression or death prior to progression)(progression or death prior to progression)
Analysis of TTD performed after >75% of patients deadAnalysis of TTD performed after >75% of patients dead
Trial 20 Trial 21
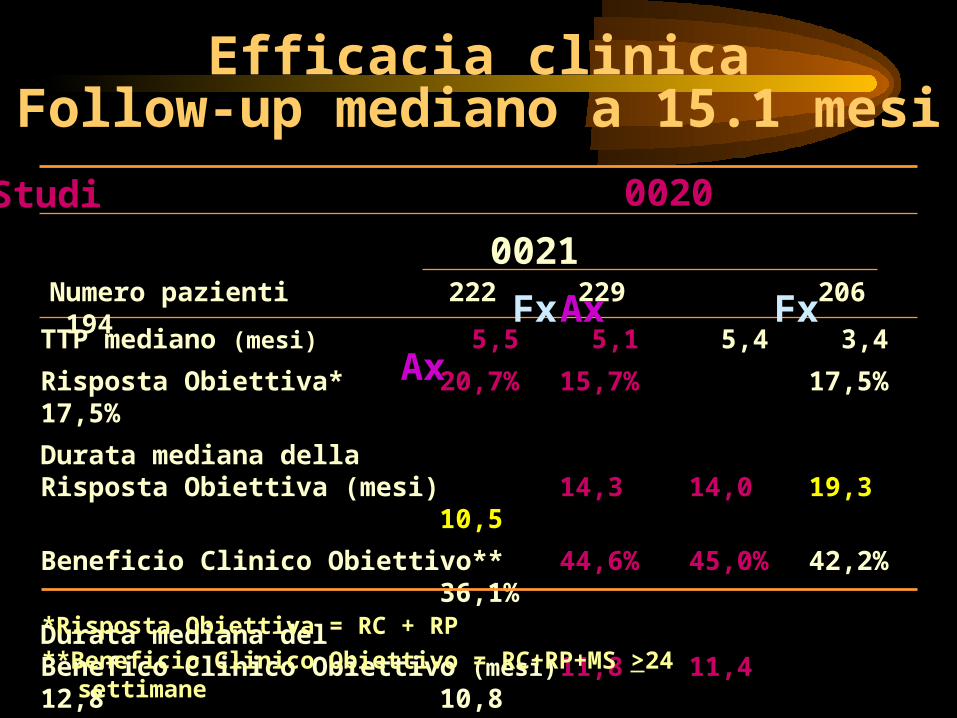
TTP mediano (mesi) 5,5 5,1 5,4 3,4
Risposta Obiettiva* 20,7% 15,7% 17,5% 17,5%
Durata mediana della Risposta Obiettiva (mesi) 14,3 14,0 19,3 10,5
Beneficio Clinico Obiettivo** 44,6% 45,0% 42,2% 36,1%
Durata mediana delBenefico Clinico Obiettivo (mesi) 11,8 11,4 12,8 10,8*Risposta Obiettiva = RC + RP**Beneficio Clinico Obiettivo = RC+RP+MS >24
settimane
Studi
Numero pazienti 222 229 206 194
0020
0021
Fx Ax Fx Ax
Efficacia clinicaFollow-up mediano a 15.1 mesi

Suppressive treatments Premenopause: ovariectomy, LH-
RHa Postmenopause: aromatase
inhibitors Competitive treatments Pre/postmenopause:
antiestrogens (TAM, TOR)
steroidal antiestrogen (Faslodex)
progestagensantiprogestins
Hormonetherapy: which drugs?
which sequences?


Second-line therapy with aromatase inhibitors
Goss PE & Strasser K, 2001

Front-line Therapy With Aromatase Inhibitors ANA vs TAM1
(1 mg)ANA vs TAM2
(1 mg)LTZ vs TAM3
(1 mg)No. of patients 171/182 340/328 453/454Response rate (CR + PR) %
21/17 33/32 30/20 (0.006)
Clinical benefit (CR + PR + SD>24 wks) %
59/45 56/55 49/38 (0.001)
Median TTP, mos 11.1/5.6 (0.005)
8.2/8.3 (8.9/7.8)
10.1/6.2 (0.0001)
Median TTF, mos 7.6/5.4 7.3/6.3 (6.2/6.0)
10/6.1 (0.001)
Median OS, mos -/- -/- -/-Edema (weight gain) 2.9/1.1 1.8/1.8
Hot flashes 36.5/24.2 20.5/20.7 18/15Thromboembolic disease 4.1/8.2 4.8/7.3 -/-Nausea 30.6/34.1 12.5/13.4 15/16Vomiting 14.7/12.1 3.9/4.3 -/-Asthenia 31.8/35.5 8.6/4.9 11/10Pain 25.3/26.4 6.3/6.1 20/18
1Nabholtz JM, 2000; 2Bonneterre J, 2000; 3Mouridsen H, 2001

Suppressive treatments Premenopause: ovariectomy, LH-
RHa Postmenopause: aromatase
inhibitors Competitive treatments Pre/postmenopause:
antiestrogens (TAM, TOR)
steroidal antiestrogen (Faslodex)
progestagensantiprogestins
Hormonetherapy: which drugs?
which sequences?
• Many premenopausal and postmenopausal women Many premenopausal and postmenopausal women with hormoneresponsive breast cancer benefit with hormoneresponsive breast cancer benefit from sequential use of endocrine therapies from sequential use of endocrine therapies at the at the time of disease progressiontime of disease progression. .
• Therefore, women whose breast cancers respond Therefore, women whose breast cancers respond to an endocrine manouvre with either shrinkage of to an endocrine manouvre with either shrinkage of the tumor or long-term disease stabilization the tumor or long-term disease stabilization (clinical benefit) should receive additional (clinical benefit) should receive additional endocrine therapy endocrine therapy at the timeat the time of disease of disease progressionprogression. .

Ormonoterapia – Pre-Ormonoterapia – Pre-menopausamenopausa
AIOM 2009

Ormonoterapia – Post-menopausaOrmonoterapia – Post-menopausa
AIOM 2009
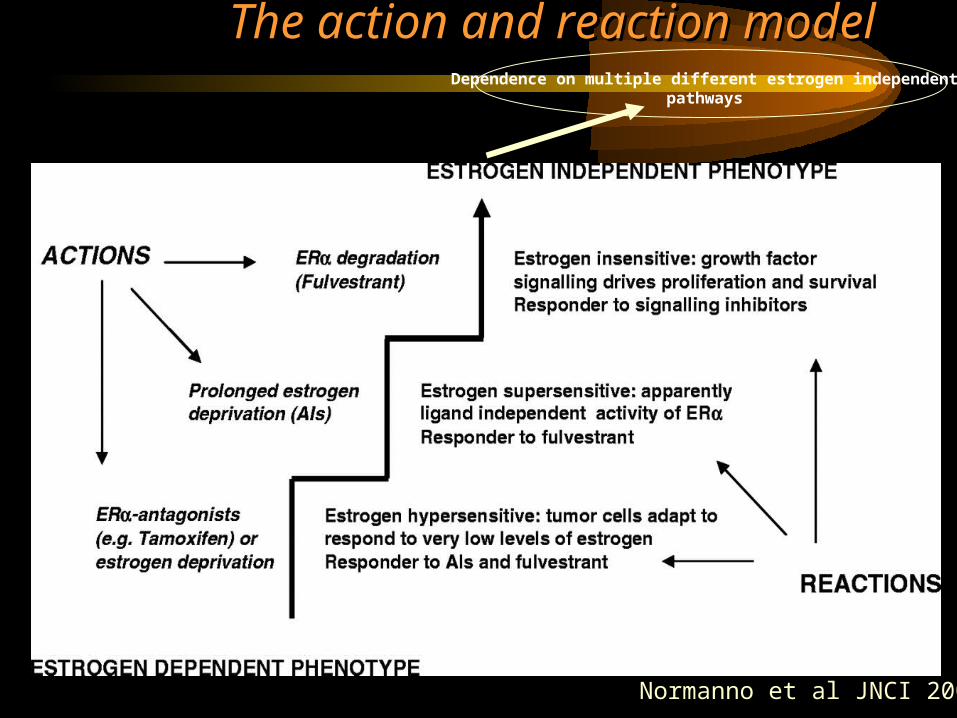
The action and reaction modelThe action and reaction model
Normanno et al JNCI 2005
Dependence on multiple different estrogen independent pathways
CAUSES OF ENDOCRINE-RESISTANCECAUSES OF ENDOCRINE-RESISTANCEAROMATASE INHIBITORSAROMATASE INHIBITORS
CAUSES OF ENDOCRINE-RESISTANCECAUSES OF ENDOCRINE-RESISTANCEAROMATASE INHIBITORSAROMATASE INHIBITORS
• Hypersensitivity
• Increased cross-talk between the growth factor signalling pathways and ER
– ER remains an integral part of signalling
• Hypersensitivity
• Increased cross-talk between the growth factor signalling pathways and ER
– ER remains an integral part of signalling

Tumor cell adaptation:effects of long-term estrogen deprivation

Ellis MJ, SABCS 2008
A Randomized phase 2 trial of Low Dose (6 mg Daily) versus High Dose (30 mg Daily) Estradiol for Patients with Estrogen Receptor Positive AI- Resistant ABC


CAUSES OF ENDOCRINE-RESISTANCECAUSES OF ENDOCRINE-RESISTANCEAROMATASE INHIBITORSAROMATASE INHIBITORS
CAUSES OF ENDOCRINE-RESISTANCECAUSES OF ENDOCRINE-RESISTANCEAROMATASE INHIBITORSAROMATASE INHIBITORS
• Hypersensitivity
• Increased cross-talk between the growth factor signalling pathways and ER
– ER remains an integral part of signalling
• Hypersensitivity
• Increased cross-talk between the growth factor signalling pathways and ER
– ER remains an integral part of signalling

Possible approaches to overcoming Possible approaches to overcoming endocrine resistance:endocrine resistance:
• Maximal blockade of ER signaling
• Co-targeting ERand HER family signalling
• Co-targeting IGF-1 system
• Targeting downstream signalling
• Maximal blockade of ER signaling
• Co-targeting ERand HER family signalling
• Co-targeting IGF-1 system
• Targeting downstream signalling

FASLODEX
EXEMESTANE
OR(CR+PR)
20/270 [7.4%]
18/270 [6.7%]
CBR(CR+PR+SD>
24WS)
87/270 [32.2%]
85/270 [31.5%]

Fulvestrant plus letrozole is more active thaneither agent alone in tumour xenografts
Jelovac et al. Cancer Res 2005; 65: 5439–5444
Changeof meantumourvolume(%)
Time (weeks)0
0
100
200
300
400
500
600
700
800
6 12 18 24 30 36
Control
Letrozole (10 µg/day)
Fulvestrant (1 mg/day)+ letrozole (10 µg/day)
Fulvestrant (1 mg/day)
Fulvestrant Fulvestrant combination trials with AIscombination trials with AIs
• SWOG S0226 – ‘Faslodex’ + ‘Arimidex’ versus ‘Arimidex’
• FACT – ‘Faslodex’ and ‘Arimidex’ in Clinical Trial
• SOFEA – Study Of ‘Faslodex’, Exemestane and ‘Arimidex’

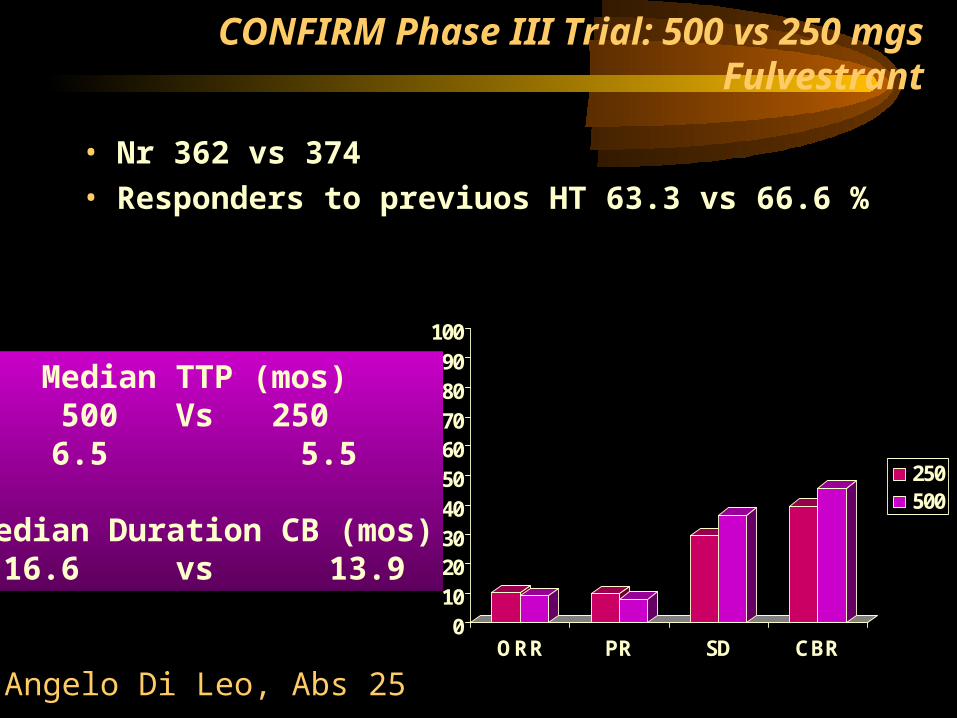
CONFIRM Phase III Trial: 500 vs 250 mgs Fulvestrant
• Nr 362 vs 374
• Responders to previuos HT 63.3 vs 66.6 %
0102030405060708090
100
%
ORR PR SD CBR
250500
Median TTP (mos) 500 Vs 250 6.5 5.5
Median Duration CB (mos)
16.6 vs 13.9
Angelo Di Leo, Abs 25
Cross-talk and endocrine resistance
• Increased EGFR and HER2 signalling is associated with the development of resistance to endocrine agents
• Targeting both the ER with endocrine agents andthe EGFR with anti EGFR agents delays the onset of resistance in pre-clinical models

Possible approaches to overcoming Possible approaches to overcoming endocrine resistance:endocrine resistance:
• Maximal blockade of ER signaling
• Co-targeting ERand HER family signalling
• Co-targeting IGF-1 system
• Targeting downstream signalling
• Maximal blockade of ER signaling
• Co-targeting ERand HER family signalling
• Co-targeting IGF-1 system
• Targeting downstream signalling

Trial Regimen PopulationNo. of
patients
Median PFS, mo
Endocrine therapy alone
Endocrine therapy + anti-ErbB
TAnDEM 1
Phase IIIAnastrozole +/-
trastuzumabHER2+ 208 2.4 * 4.8 *
Osborne et al2
Randomized, placebo-controlled phase II
Tamoxifen +/- gefitinib
ITT
HER2+ subset
206†
37
8.8
5.8
10.9
6.7
Cristofanilli et al3
Randomized, placebo-controlled phase II
Anastrozole +/- gefitinib
ITT 93 8.2 14.5
Clinical Evidence for Co-TargetingGrowth Factor Receptors in ER+
MBC
1Mackey J, et al. Breast Cancer Res Treat. 2006;100. Abstract 3; 2Osborne K, et al. Breast Cancer Res Treat. 2007;106. Abstract 2067; 3Cristofanilli M, et al. J Clin Oncol. 2008;26(No 15S). Abstract 1012.

In newly diagnosed MBC or had completed adj Tam > 1 yrs:PFS (ITT): T+G= 10.9 mos T+P = 8.8 mos HR: 0.84, 95% CI 0.59-1.18
Randomized Phase II study of gefitinib or placebo in combination with tamoxifen in pts with hormone receptor positive metastatic breast cancerOsborne CK,SABCC 2007

PFS: A+G = 14.5 mos A+P = 8.2 mos HR: 0.55, 95% CI 0.32-0.94
Conclusions:”…..A+G well tolerated and associated with a marked advantage in PFS versus A+P in postmenopausal women with newly diagnosed HR+ MBC….”
A phase II multicenter, randomized trial to compare anastrozole plusGefitinib with anastrozole plus placebo in postmenopausal women with hormone receptor-positive metastatic breast cancer (MBC).
Cristofanilli M et al ASCO 2008
12%5%
Zac-FasT Trial (Zactima Faslodex Trial): a randomised, double-blind, parallel-group, multicentre, phase II study to evaluate the safety and pharmacological activity of the combination of a new TKI Vandetanib (100 or 300 mg/daily or placebo) with Fulvestrant (loading dose), in postmenopausal advanced breast cancer patients.
Primary endpoint:EFSMain Secondary endpoints: - Success rate at 6 months- Objective tumor response rate - Time to Progression- Progression-free survival- Overall survival- Safety and tolerability of the combination

All
HER-2+
HER-2+ Median OS 33 m
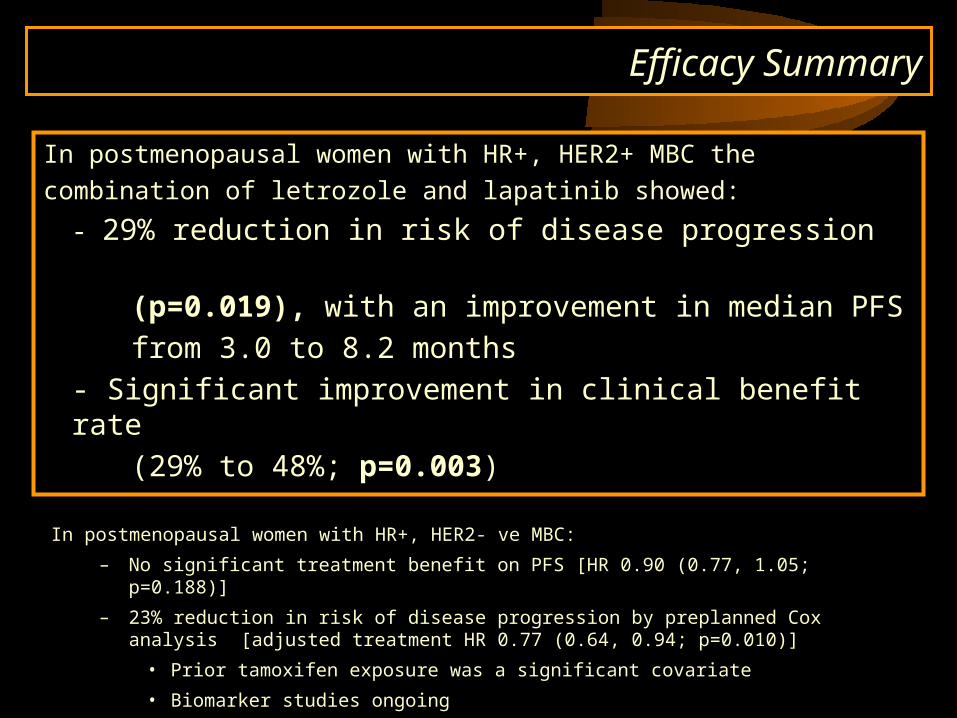
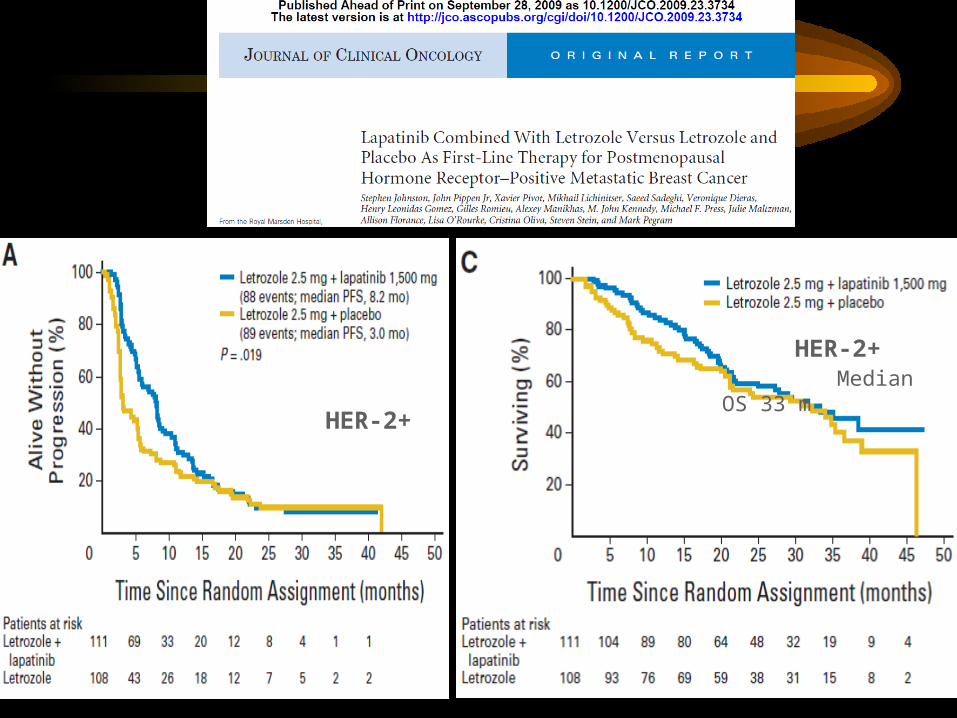
Efficacy Summary
In postmenopausal women with HR+, HER2+ MBC the
combination of letrozole and lapatinib showed:
- 29% reduction in risk of disease progression
(p=0.019), with an improvement in median PFS
from 3.0 to 8.2 months
- Significant improvement in clinical benefit rate
(29% to 48%; p=0.003)
In postmenopausal women with HR+, HER2- ve MBC:
– No significant treatment benefit on PFS [HR 0.90 (0.77, 1.05; p=0.188)]
– 23% reduction in risk of disease progression by preplanned Cox analysis [adjusted treatment HR 0.77 (0.64, 0.94; p=0.010)]
• Prior tamoxifen exposure was a significant covariate
• Biomarker studies ongoing

Possible approaches to overcoming Possible approaches to overcoming endocrine resistance:endocrine resistance:
• Maximal blockade of ER signaling
• Co-targeting ERand HER family signalling
• Co-targeting IGF-1 system
• Targeting downstream signalling
• Maximal blockade of ER signaling
• Co-targeting ERand HER family signalling
• Co-targeting IGF-1 system
• Targeting downstream signalling

TCD 10631 Study: Multicenter, randomized, open label study evaluating an anti Insulin-like Growth Factor-1 Receptor (IGF-1R/CD221) monoclonal antibody, AVE1642, administered every 4 weeks in combination with Faslodex® in postmenopausal patients with advanced hormono-dependent breast cancer (in I or II line)
Primary endpoint : Clinical Benefit (CB)
Main Secondary endpoints :- Progression Free Survival Rate (PFSR) at 6 months- Progression Free Survival (PFS)- Safety
Possible approaches to overcoming Possible approaches to overcoming endocrine resistance:endocrine resistance:
• Maximal blockade of ER signaling
• Co-targeting ERand HER family signalling
• Co-targeting IGF-1 system
• Targeting downstream signalling
• Maximal blockade of ER signaling
• Co-targeting ERand HER family signalling
• Co-targeting IGF-1 system
• Targeting downstream signalling

1. Treatment of postmenopausal women with LABC or MBC with Let alone or in combination with Tensirolimus: a randomized, 3-arm, phase 2 study: “…Combination well tolerated, longer PFS….”
2. Phase 3 study of tensirolimus plus Let vs Let alone in postmenopausal women with LABC or MBC:”… No improvement in PFS was seen in the overall population..”
Baselga J, et al. Breast Cancer Res Treat, 2005
Chow LWC, et al. Breast Cancer Res Treat, 2006
Tailor treatment according to disease characteristics and patients expectations!A negligible achievement to the physician might be terribly important to the patient (… and viceversa).


















