Doppler Ultrasonography in Obstetrical Practice China Medical University Hospital OBS & GYN...
41
Doppler Ultrasonography in Obstetrical Practice China Medical University China Medical University Hospital Hospital OBS & GYN department OBS & GYN department Chien Chung, Lee Chien Chung, Lee
-
Upload
landon-torney -
Category
Documents
-
view
217 -
download
0
Transcript of Doppler Ultrasonography in Obstetrical Practice China Medical University Hospital OBS & GYN...

Doppler Ultrasonography in Obstetrical Practice
China Medical University HospitalChina Medical University Hospital
OBS & GYN departmentOBS & GYN department
Chien Chung, LeeChien Chung, Lee

Conditions That Place Fetuses at Risk for Adverse OutcomesConditions That Place Fetuses at Risk for Adverse Outcomes MaternalMaternal
Chronic hypertensionChronic hypertensionCollagen-vascular diseasCollagen-vascular diseasesesSickle cell anemiaSickle cell anemiaCurrent substance abuseCurrent substance abuseImpaired renal functionImpaired renal functionAsthmaAsthmaPneumoniaPneumoniaSignificant cardiac diseasSignificant cardiac diseaseeSeizure disordersSeizure disordersDiabetesDiabetesAcute febrile illnessesAcute febrile illnessesSignificant anemia (hemaSignificant anemia (hematocrit <26% tocrit <26%
FetalFetalIntrauterine growth rIntrauterine growth restrictionestrictionCongenital anomalieCongenital anomaliessFetal cardiac arrhythFetal cardiac arrhythmiasmiasIsoimmunizationIsoimmunizationHydrops fetalisHydrops fetalisFetal infections such Fetal infections such as parvovirus, coxsaas parvovirus, coxsackievirus B, syphilis, ckievirus B, syphilis, toxoplasmosis toxoplasmosis
Pregnancy-relatedPregnancy-relatedPoorly controlled gestatioPoorly controlled gestational diabetesnal diabetesMultiple gestationsMultiple gestationsPregnancy-induced hypePregnancy-induced hypertensionrtensionCholestasis of pregnancCholestasis of pregnancyyPremature rupture of the Premature rupture of the membranes (preterm)membranes (preterm)Unexplained elevated mUnexplained elevated maternalaternalserum alpha-fetoproteinserum alpha-fetoproteinPolyhydramniosPolyhydramniosOligohydramniosOligohydramniosPlacental abruptionPlacental abruptionAbnormal placentationAbnormal placentationPostdatesPostdatesUnexplained stillbirth in a Unexplained stillbirth in a prior pregnancy prior pregnancy

General Guidelines for Antepartum TestingGeneral Guidelines for Antepartum Testing Indication Initiation Frequency
Post-term pregnancy 41 weeks Twice a week
Preterm rupture of the membranes At onset Daily
Oligohydramnios 26 weeks or at onset Twice a week
Polyhydramnios 32 weeks Weekly
Class A1 DM (well-controlled, no complications) 36 weeks Weekly
Class A2 and B (well-controlled, no complications) 32 weeks Twice a week
Class A or B with poor control, Class C-R 28 weeks Weekly
Chronic or pregnancy-induced hypertension 28 Weeks Weekly
Steroid-dependent or poorly controlled asthma 28 Weeks Weekly
Collagen-vascular disease including antiphospholipid antibody syndrome
28 Weeks Weekly
Impaired renal function 28 weeks Weekly
Uncontrolled thyroid disease 32 weeks Weekly
Maternal heart disease (NYHA class III or IV) 28 weeks Once a week
Substance abuse 32 weeks Weekly
Prior stillbirth At 2 weeks before prior fetal death Weekly
Multiple gestation 32 weeks Weekly
Fetal growth restriction 26 weeks or at onset Twice a week
Decreased fetal movement At time of complaint Once
Cholestasis 32 weeks Weekly

Biophysical profile for fetal assessment in high Biophysical profile for fetal assessment in high risk pregnancies (Cochrane Methodology Review)risk pregnancies (Cochrane Methodology Review)
Reviewers' conclusions: At present, there is not enough evidence from randomised trials to evaluate the use of biophysical profile as a test of fetal well-being in high risk pregnancies.
Alfirevic Z, Neilson JP. In: Alfirevic Z, Neilson JP. In: The Cochrane Library, The Cochrane Library, Issue 4, 2003. Issue 4, 2003.

Doppler ultrasound for fetal Doppler ultrasound for fetal assessment in high risk pregnancies assessment in high risk pregnancies (Cochrane Methodology Review)(Cochrane Methodology Review)
Reviewers' conclusions: The use of Doppler ultrasound in high risk pregnancies appears to improve a number of obstetric care outcomes and appears promising in helping to reducing perinatal deaths.
Neilson JP, Alfirevic Z.Neilson JP, Alfirevic Z. . In: . In: The Cochrane Library, The Cochrane Library, Issue 4, 2003.Issue 4, 2003.

Descriptive characteristics of randomized trials evaluating the use of Doppler ultrasonography in pregnancy included in overview
ReferenceReference No. of No. of participantparticipant
Perinatal Perinatal deaths deaths
(%)(%)
Type of Doppler ultrasonography usedType of Doppler ultrasonography used AEDV AEDV (%)(%)
Controls Prespecified primary end poiControls Prespecified primary end point with sample size calculationsnt with sample size calculations
Trudinger et al., 1987,
l289 2.1 Umbilical artery, CW 4 MHz ? Gestational age at delivery
McParland and Pearce, 1988
509 5.1 Umbilical and uterine arteries, PW 15.1 Death before discharge from hospital
Tyrell et al., 1990 500 1.2 Umbilical and uterine arteries, CW, 4 MHz, 100 hZ
2.7 No. of days in neonatal intensive care unit, frequency of low Apgar score
Hofmeyr et al., 1991
897 1.3 Umbilical artery, CW, 4 MHz, 50 Hz filter ? Not stated
Newnham et al., 1991
545 3.3 Umbilical artery, CW, 280 Hz filter 2.9 Neonatal hospital stay
Burke et al., 1992 476 1.5 Umbilical artery, CW, 4 MHz, 150 Hz filter ? Not stated
Almstrom et al., 1992
426 0.7 Umbilical artery, PW, 3 MHz, 100 Hz filter 1.9 Not stated
Biljan et al., 1992 674 0.7 Umbilical artery, CW, 4 MHz, 100 Hz filter 1.3 No. of antenatal tests per patient, duration of antenatal stay
Johnstone et al., 1993
2329 1.2 Umbilical artery, CW, 4 MHz, 60-80 Hz filter?
? Not stated
Pattison et al., 1994
212 6.6 Umbilical artery, CW, 4 MHz, 100 Hz filter 9.4 Perinatal mortality
Neales et al 467 5.3 Umbilical artery, CW, 4 MHz 6.4 Not stated
Nienhuis and Hoogland
150S 3.4 Umbilical artery, PW, 50 Hz filter ? Not stated

Proportional effect of Doppler ultrasonography on number of dead babies Proportional effect of Doppler ultrasonography on number of dead babies (stillbirths and neonates) when used in high-risk pregnancies.(stillbirths and neonates) when used in high-risk pregnancies.
Meta-analysis shows that clinical action guided by Doppler ultrasonography reduced the odds ratio of perinatal death by 38%

Effects of Doppler ultrasonography on perinatal outcomes in high-risk pregnancies. Post hoc analysis.
The 16% reduction in the number of elective deliveries, 31% reduction in fetal distress in labor, and 87% reduction in hypoxic encephalopathy in the Doppler group reached statistical significance.

Conditions for Doppler ultrasoundConditions for Doppler ultrasound(1)(1) Pregnancies complicated by IUGRPregnancies complicated by IUGR
(2)(2) Pregnancies in which the fetus is at risk for anemia Pregnancies in which the fetus is at risk for anemia
(3)(3) Multiple gestationsMultiple gestations
(4)(4) Pregnancies treated with prostaglandin inhibitors to mPregnancies treated with prostaglandin inhibitors to monitor the ductus arteriosusonitor the ductus arteriosus
(5)(5) Fetal echocardiograms Fetal echocardiograms


Doppler Flow Velocity in the First TrimesterDoppler Flow Velocity in the First Trimester
Comparison of endometrial thickness, RI, & gestational age between groups
Retained tissueRetained tissue Not retained tissueNot retained tissue PP
Gestational ageGestational age 10.0(3.3)10.0(3.3) 7.6(2.0)7.6(2.0) 0.0010.001
Endometrial thicEndometrial thickness(mm)kness(mm)
19.5(1.8)19.5(1.8) 10.2(7.0)10.2(7.0) 0.0010.001
RIRI 0.38(0.16)0.38(0.16) 0.59(0.12)0.59(0.12) 0.0010.001
Alcazar JL, Ortiz CA. Eur J Obstet Gynecol Reprod Biol. 2002 Apr 10;102(1):83-7.

Doppler Flow Velocity in Uterine ArteryDoppler Flow Velocity in Uterine Artery
Bewley et. al. Br J Obstet Gynaecol 1989;96:1040–6


(A) Normal uterine artery at 12 weeks shows relatively high resistance, absent notching.
(B) Normal midtrimester uterine artery, increased diastolic flow.
(C) Normal third trimester uterine artery, very low resistance.
(D)High resistance with persistent notching may be normal in first trimester, not in this 24-week gestation.
(E) Very high resistance, marked notching, absent diastolic velocities in a woman with pre-eclampsia, and severe intrauterine growth restriction (IUGR) at 28 weeks.

(A) Normal umbilical artery at 18 weeks shows relatively high resistance, but consistent diastolic flow.
(B) Normal umbilical artery at 36 weeks, low resistance, generous diastolic flow.
(C)High resistance, diastolic velocity low.
(D)Absent end-diastolic velocity (AEDV).
(E) Reversed diastolic velocity (REDV) in severe intrauterine growth restriction (IUGR).
Doppler Flow Velocity in Umbilical ArteryDoppler Flow Velocity in Umbilical Artery

Doppler Flow Velocity in Umbilical ArteryDoppler Flow Velocity in Umbilical Artery
Madazli R, Uludag S, Ocak V.
Acta Obstet Gynecol Scand 2001; 80:702
Fetuses with absent end-diastolic velocity of the umbilical artery all died in utero within 3 weeks (median 7 days).

FACTORS AFFECTING UMBILICAL ARTERY DOPPLER FLOW VELOCITY WAVEFORMS
Gestational age EDFV ratio increases with advancing gestational age
Fetal heart rate EDFV decreases with decreasing fetal heart rate
Fetal breathing movements Increases variability in the measurements
Site of measurement EDFV is higher near the placental insertion than near the umbilical cord insertion into the fetal abdomen
Equipment used : continuous Doppler versus pulsed Doppler
Continuous Doppler is more a “blind technique” compared
with pulsed Duplex Doppler, allowing 2D real time ultrasound
User experience Reliability increases with increasing experience
Radius of the umbilical artery Decreasing radius (vasoconstriction) increases EDFV
Impedance to pulsatile flow propagation Increasing vascular impedance increases EDFV
Downstream vascular resistance within the microcirculation
Increasing vascular resistance decreases EDFV
Angle of the fetal Doppler insonation Best if less than 45˚; <15˚ for MCA absolute peak systolic flow
velocity

Diagnostic efficacy of umbilical arterial Doppler in IUGRDiagnostic efficacy of umbilical arterial Doppler in IUGR
Author DI Prevalence Sensitivity Specificity PPV
Fleischer S/DFleischer S/D>>3.0 16.8 78 83 493.0 16.8 78 83 49
Aruidini PI>1SD 30.7 60.8 73 50Aruidini PI>1SD 30.7 60.8 73 50
Berkowitz S/D>3.0 25 55 92 73Berkowitz S/D>3.0 25 55 92 73
Divon S/DDivon S/D>>3.0 35.4 49 94 813.0 35.4 49 94 81
Gaziano S/DGaziano S/D>>4.0 9.4 79 66 794.0 9.4 79 66 79
Ott S/DOtt S/D>>3.0 10.4 59 84 293.0 10.4 59 84 29
Maulik S/DMaulik S/D>>2.9 12.3 75 71 272.9 12.3 75 71 27
Lowery S/DLowery S/D>>4.0 22.6 65 66 24 4.0 22.6 65 66 24
Lee S/DLee S/D>>3.0 15 91.7 68.7 84.63.0 15 91.7 68.7 84.6

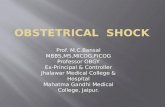
Middle cerebral artery Doppler waveforms
Normal flow of the Middle Cerebral Artery in 1º trimester
Normal flow of the Middle Cerebral Artery in 2º and 3º trimester

Middle cerebral artery Doppler waveforms
(A) Normal middle cerebral artery (MCA) at term - normal peak systolic velocity (58 cm/s), high resistance, low end-diastolic velocity.
(B) ‘Brain sparing’ MCA - lower peak, much higher diastolic velocity suggests cerebrovasodilation.
(C) Anemic fetus with retained high resistance, elevated peak systolic velocity (77 cm/s).

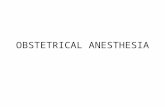
Doppler Flow Velocity in Ductus venosusDoppler Flow Velocity in Ductus venosus

The upper panel represents the venous waveform, correlated with the EKG in the lower panel. A = atrial systole, S = ventricular systole, D = early ventricular diastole. The colored portions of the waveform represent the Tamx for atrial systole (gold), ventricular systole (red), and early ventricular diastole (blue). The yellow arrows represent the measurement of the peak velocity for ventricular systole and early ventricular diastole. The black arrow represents the peak velocity for atrial systole.

(A) Ductus venosus (DV) Doppler waveforms at 12 weeks gestation.
(B) At 12 weeks gestation, an abnormal a-wave (a), correctly predicted anomalous pulmonary and systemic venous return, proven by fetal echocardiography at 24 weeks.
(C) DV at 26 weeks, with 4-phase waveform. (1) atrial contraction (2) ventricular systole, (3) return (ascent) of the annulus (called the y-descent of the DV waveform), & (4) diastole.
(D) Normal waveform from the middle hepatic vein which, is only a few millimeters from the DV.

Doppler Flow Velocity in IUGRDoppler Flow Velocity in IUGR

Progressive changes in Doppler parameters in IUGR fetuses delivered for an Progressive changes in Doppler parameters in IUGR fetuses delivered for an abnormal Biophysical Profile Score. abnormal Biophysical Profile Score.

Hemodynamic changes occurring in fetal arterial vessels during hyHemodynamic changes occurring in fetal arterial vessels during hypoxemia and acidemia induced by uteroplacental insufficiencypoxemia and acidemia induced by uteroplacental insufficiency
Vessel Vessel Impedance to flow Impedance to flow Descending aortaDescending aorta IncreasedIncreased
Renal arteryRenal artery IncreasedIncreased
Femoral arteryFemoral artery IncreasedIncreased
Peripheral pulmonary arteryPeripheral pulmonary artery IncreasedIncreased
Mesenteric arteriesMesenteric arteries IncreasedIncreased
Cerebral arteriesCerebral arteries DecreasedDecreased
Adrenal arteriesAdrenal arteries DecreasedDecreased
Splenic arteriesSplenic arteries DecreasedDecreased
Coronary arteriesCoronary arteries DecreasedDecreased


Fetal Systemic Vascular Responses in IUGRFetal Systemic Vascular Responses in IUGRA/REDV, absent or reversed end-diastolA/REDV, absent or reversed end-diastol
ic velocitiesic velocities HARMAN: Clin Obstet Gynecol, 46(4).December 2003.931-946

Aortic isthmus blood velocity waveform a) normal blood flow pattern in an uncomplicated pregnancy
In the sagittal view of the fetus, the aortic arch and the location of the aortic isthmus (white triangle) are shown.
b) antegrade net blood flow (antegrade/retrograde ratio of 2.0)
c) retrograde net blood flow with a corresponding value of 0.54 in pregnancies complicated by placental insufficiency.

Coronary artery blood velocity waveform of a growth-restricted 32 week fetus (heart sparing effect).

Alfred Abuhamad et al. Contemporary Ob/Gyn May 1, 2003;48:56-73

Evaluation of fetal intrapartum hypoxia by middle ceEvaluation of fetal intrapartum hypoxia by middle cerebral & umbilical artery Doppler velocimetry with srebral & umbilical artery Doppler velocimetry with simultaneous cardiotocography & pulse oximetry imultaneous cardiotocography & pulse oximetry
During active labor the fetus maintains oxygen During active labor the fetus maintains oxygen supply to the brain by redistributing blood flow. In supply to the brain by redistributing blood flow. In cases of hypoxia this is feasible for only 2 min. cases of hypoxia this is feasible for only 2 min.
Siristatidis C, Salamalekis E, Kassanos D, Loghis C, Creatsas G Arch Gynecol Obstet. 2003 Nov 5

Spectral Doppler waveform of an A-A anastomosis with characteristic bidirectional, pulsatile flow.

Systematic Doppler Evaluation HARMAN: Clin Obstet Gynecol, Volume 46(4).December 2003.931

Which Doppler Tests Should Which Doppler Tests Should be Performed?be Performed?
1. Uterine arteries depict maternal vascular effects of the invading placenta
2.2. Umbilical artery Doppler reflects downstream pUmbilical artery Doppler reflects downstream placental vascular resistance lacental vascular resistance
3.3. Middle cerebral artery changes begin when the Middle cerebral artery changes begin when the redistribution of cardiac output reflects rising plredistribution of cardiac output reflects rising placental resistance acental resistance
4.4. precordial veins illustrate fetal cardiac function precordial veins illustrate fetal cardiac function


DIFFERENTIAL DIAGNOSIS OF OLIGOHYDRAMNIOSDIFFERENTIAL DIAGNOSIS OF OLIGOHYDRAMNIOS PPROM --- normal renal vessels, normal umbilical flow & normal --- normal renal vessels, normal umbilical flow & normal filling of the bladder. filling of the bladder.
Bilateral renal agenesis or dysplasia --- umbilical artery Doppler is normal, but no renal vessels & --- umbilical artery Doppler is normal, but no renal vessels & no bladder fillingno bladder filling
Severe hypoxia with IUGR --- fetal measurements are small for gestation, fetal heart --- fetal measurements are small for gestation, fetal heart looks dilated & the bowel is echogenic. Doppler looks dilated & the bowel is echogenic. Doppler demonstrates the presence of two renal arteries and absent demonstrates the presence of two renal arteries and absent or reversed end-diastolic frequencies in the umbilical arteriesor reversed end-diastolic frequencies in the umbilical arteries

Deficient placentation defined by notched uterine arteriesDeficient placentation defined by notched uterine arteries
Increased umbilical artery resistance with progression to AEDV/REDVIncreased umbilical artery resistance with progression to AEDV/REDV
Declining CPR, brain-sparing MCA Declining CPR, brain-sparing MCA
As the arteriovenous ratio decline, ductus venosus abnormality beginsAs the arteriovenous ratio decline, ductus venosus abnormality begins
Abnormal biophysical variables emerge Abnormal biophysical variables emerge
Oligohydramnios and abnormal (non-reactive) fetal heart rate tracingOligohydramnios and abnormal (non-reactive) fetal heart rate tracing
Loss of fetal breathing movements, body movements and fetal tone Loss of fetal breathing movements, body movements and fetal tone

THE USE OF FETAL DOPPLER IN OBSTETRICS Society of Obstetricians and Gynaecologists of Canada. No. 130, July 2003
1. Umbilical artery Doppler should be available for assessment of the fetal-placental circulation in pregnant women with suspected severe placental insufficiency. (I-A)
2. Depending on other clinical factors, reduced, absent, or reversed umbilical artery end-diastolic flow is an indication for enhanced fetal surveillance or delivery. If delivery is delayed to enhance fetal lung maturity with maternal administration of glucocorticoid, intensive fetal surveillance until delivery is suggested for those fetuses with reversed end-diastolic flow. (II-1B)
3. Umbilical artery Doppler should not be used as a screening tool in healthy pregnancies, as it has not been shown to be of value in this group. (I-A)
4. Umbilical venous double pulsations, in the presence of abnormal umbilical artery Doppler waveforms, necessitate a detailed assessment of fetal health status. (II-3B)
5. Measurement of the fetal middle cerebral artery Doppler peak systolic flow velocity is a predictor of moderate or severe fetal anemia and can be used to avoid unnecessary invasive procedures in pregnancies complicated with red blood cell isoimmunization. (II-1A)
6. Since inaccurate information concerning fetal Doppler studies could lead to inappropriate clinical decisions, it is imperative that measurements be undertaken and interpreted by expert operators who are knowledgeable about the significance of Doppler changes and who practise appropriate techniques. (II-1A)

ConclusionConclusion
No single diagnostic modality can provide informatNo single diagnostic modality can provide information complete enough to adequately address the cion complete enough to adequately address the complex nature of IUGR and its interacting fetal coomplex nature of IUGR and its interacting fetal compensations and compromises mpensations and compromises
Management decisions based on Doppler data arManagement decisions based on Doppler data are gestational age dependent e gestational age dependent

Thank You For Your Attention!