Does Primary Care need a Pain Clinic? Selina Dunn CCG Clinical lead.
34
Does Primary Care need a Pain Clinic? Selina Dunn CCG Clinical lead
-
Upload
maurice-owens -
Category
Documents
-
view
216 -
download
1
Transcript of Does Primary Care need a Pain Clinic? Selina Dunn CCG Clinical lead.
Does Primary Care need a Pain Clinic?
Selina Dunn
CCG Clinical lead
Chronic Pain
”Pain that persists beyond the point at which
healing would be expected to be complete (3
mths) or that which occurs in disease processes in
which healing does not take place”. International
Association for the Study of Pain 1994
Does Primary Care need a Pain Clinic?
Mrs. Smith is here again, Monday morning you are
on call. Complaining of pain in her back …she has
been investigated and you know she has chronic
back pain. She has physio etc with no
improvement.
What do you do???
Chronic Pain
• Common dilemma, accounts for at least 22% of GP consultations
• 2nd most common complaint for benefits claimants
• A major clinical, social and economic problem however under
recognised and under treated
• For many it is a prominent feature of their lives and has a profound
impact on their QOL
• JSNA Kirklees PCT, pain had the greatest impact on health and
function
• How much education have doctors received?
Pain pathways
1.Pain primary assessment and management
2.Spinal Pain
3. Musculoskeletal pain (non spinal, non-inflammatory)
4. Neuropathic Pain
5.Pelvic Pain/Visceral (Male and female)
• Changes in structure and function of the nervous system
(brain, spinal cord and periphery), peripheral receptors
fire independently of stimulus
• Central Nervous Sensitivity – “plasticity”
• Many believe it is a disease in its own right as opposed to
those who believe it is a simple sign of disease process
Chronic Pain
What is Pain?
A complex multidimensional experience with
sensory,
cognitive,
emotional,
behavioural +
motivational components
All of which need addressing not just physical dimensions, a
simple pain history is therefore not enough…..
Biopsychosocial model
• Gold standard to understand and explain pain (Gatchel
2007,Weiner 2008)
• Bio - the role of nociception neuropathy interacting with
psychosocial factors. These are not mutually exclusive
and are invariably interwoven in an individual case
• Helps to explain the divergence in symptoms and signs
Biopsychosocial model
• Biological – to arrive at a diagnosis,
red flag exclusion, pain history,
nature, intensity
• Psychosocial – may or may nor be pain
related, emotional aspects, beliefs and
functional and dysfunctional aspects
Earlier identification of patients at risks of chronicity
• Earlier identification and treatment proven to
reduce risk of chronic pain
• 60 - 80% pts with LBP consulting in primary care
still report problems one year later. (Croft1998)
85% of those consulting have NSLBP. (Deyo
2001)
Pain primary assessment and management
Bio
•Pain history: sensory nature, qualities of pain, many types of
pain have features of neuropathic and nociceptive pain
mechanisms
•Verbal Rating Scale: 0= no pain,10=worst pain ever
•Exclusion of red flags
•PMH e.g DM
•Medication
Condition specific pathways
1. Spinal Pain
2. Musculoskeletal pain (non spinal, non-
inflammatory)
3. Neuropathic Pain
4. Pelvic Pain/Visceral (Male and female)
LBP – Initial Consult
1. ICE, reassurance, advice to keep active and
continue working if possible
2. Analgesia, may need neuropathic pain
medications as per NICE
3. Signposting to self care/management (leaflets,
book, video, 3rd sector peer support)
Self care and management
• Underpins all activities within ALL pain pathways, at
each care point.
• Pain management is most effective when it engages the
patient in self-management / care
• Provision of reliable information about their condition and self-care
options and how to access these appropriately
• Promotion of an individual’s understanding of his or her own health
and its maintenance
• Development of self-management or ‘coping’ skills.
Self care and management
www.selfcareconnect.co.uk includes EPP
www.paintoolkit.org/
www.sheffieldbackpain.com
www.nhsinform.co.uk/health-zones/scottish-backs.aspx
www.backcare.org.uk/
www.arthritisresearchuk.org/
'Non-specific Lower Back Pain in Adults' (PDF) from Patient UK at http://www.patient.co.uk
Back and neck pain' (PDF) from the British Brain & Spine Foundation http://brainandspine.org.uk
'Back pain' (URL) from Bupa at http://www.bupa.co.uk
Self care and management 'Back pain: patient perspective articles' (URL) from the British Brain & Spine Foundation at
http://brainandspine.org.uk
'Injections for chronic back pain' (URL) from Bupa at http://www.bupa.co.uk
'Low back pain: understanding NICE guidance' (PDF) from the National Institute for Health
and Clinical Excellence at http:// www.nice.org.uk
Book: Roland, M.O et al. (2002) The back book. London: The Stationary Office.
DVD: Get Back Active www.youtube.com/watch?v=7ao9Y19TZJQ
Review 2 weeks
No improvement /deterioration:
1. Severe radicular pain/neurological defecit: refer spinal centre
2. Biopsychosocial assessment
a. 4D’s risk assessment tool to support review
•Depression
•Disability
•Drug use problematic
•Diagnostic uncertainty, red flags
b. Keele STarT Back Tool
The Keele STarT Back ToolHill 2001
•Diagnosis and management of BP is often difficult in primary care, but
prognostic indicators offer assistance in management of the patient
•Often treatment modifiable prognostic indicators are identified too late
therefore problems are entrenched, STarT - early targeted intervention
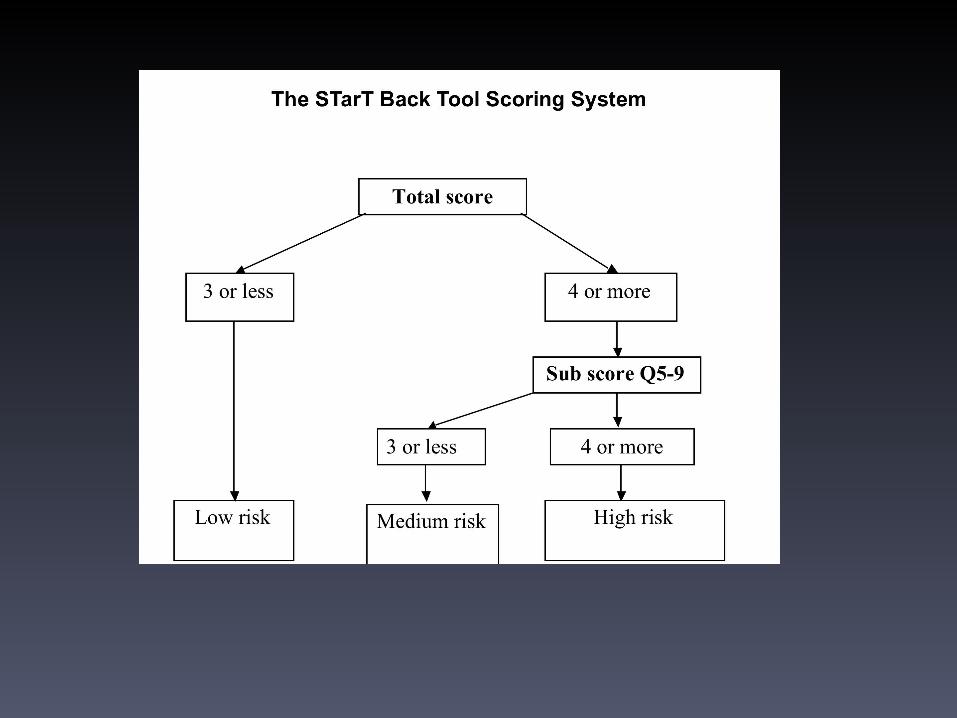
•9 item tool to identify subgroups (high, medium or low risk) by screening
for prognostic indicators that can be targeted with evidence based
treatment options
STarT Back tool improves back pain management
• Preventing low risk patients from being over-treated
• Reducing medium risk patient secondary care referrals
• Improving high risk patient access to targeted treatment
aimed at preventing long-term disability
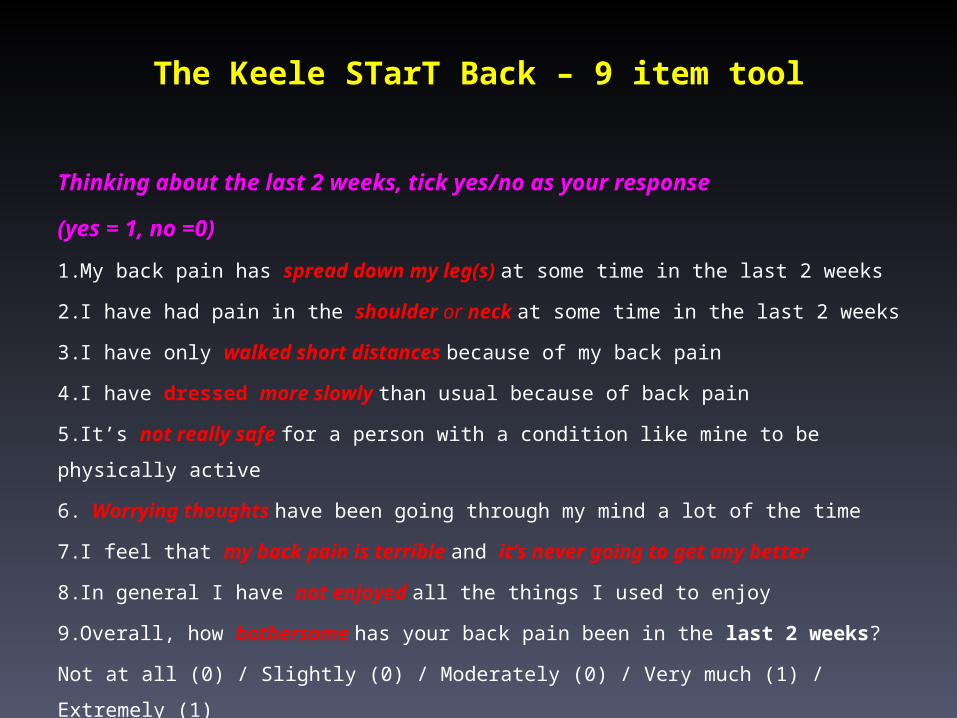
The Keele STarT Back – 9 item tool
Thinking about the last 2 weeks, tick yes/no as your response
(yes = 1, no =0)
1.My back pain has spread down my leg(s) at some time in the last 2 weeks
2.I have had pain in the shoulder or neck at some time in the last 2 weeks
3.I have only walked short distances because of my back pain
4.I have dressed more slowly than usual because of back pain
5.It’s not really safe for a person with a condition like mine to be physically active
6. Worrying thoughts have been going through my mind a lot of the time
7.I feel that my back pain is terrible and it’s never going to get any better
8.In general I have not enjoyed all the things I used to enjoy
9.Overall, how bothersome has your back pain been in the last 2 weeks?
Not at all (0) / Slightly (0) / Moderately (0) / Very much (1) / Extremely (1)
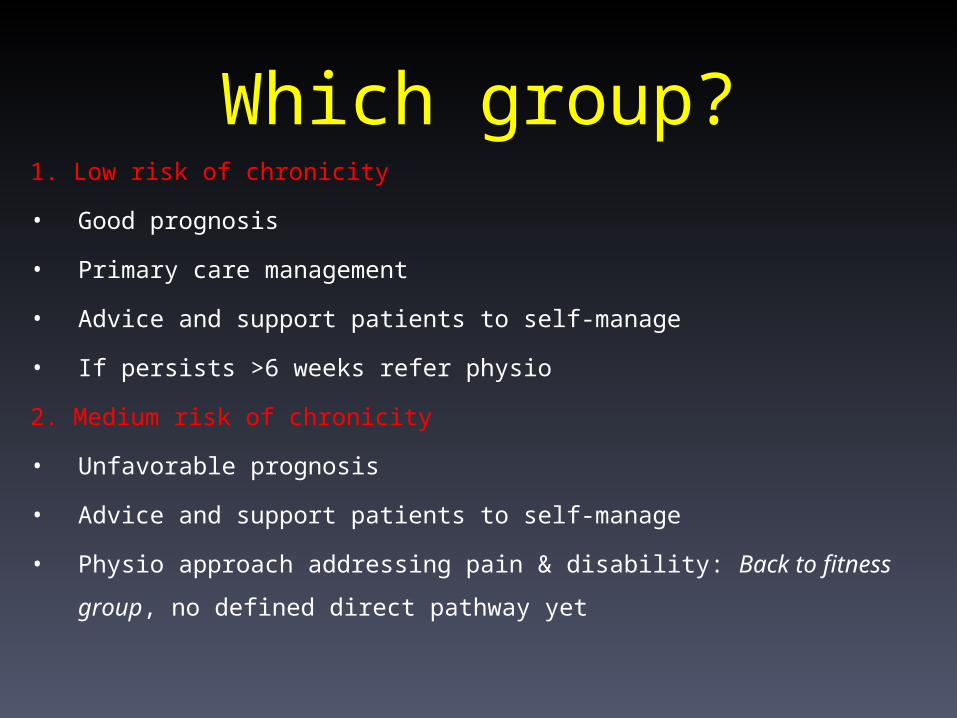
Which group?1. Low risk of chronicity
• Good prognosis
• Primary care management
• Advice and support patients to self-manage
• If persists >6 weeks refer physio
2. Medium risk of chronicity
• Unfavorable prognosis
• Advice and support patients to self-manage
• Physio approach addressing pain & disability: Back to fitness group, no defined
direct pathway yet
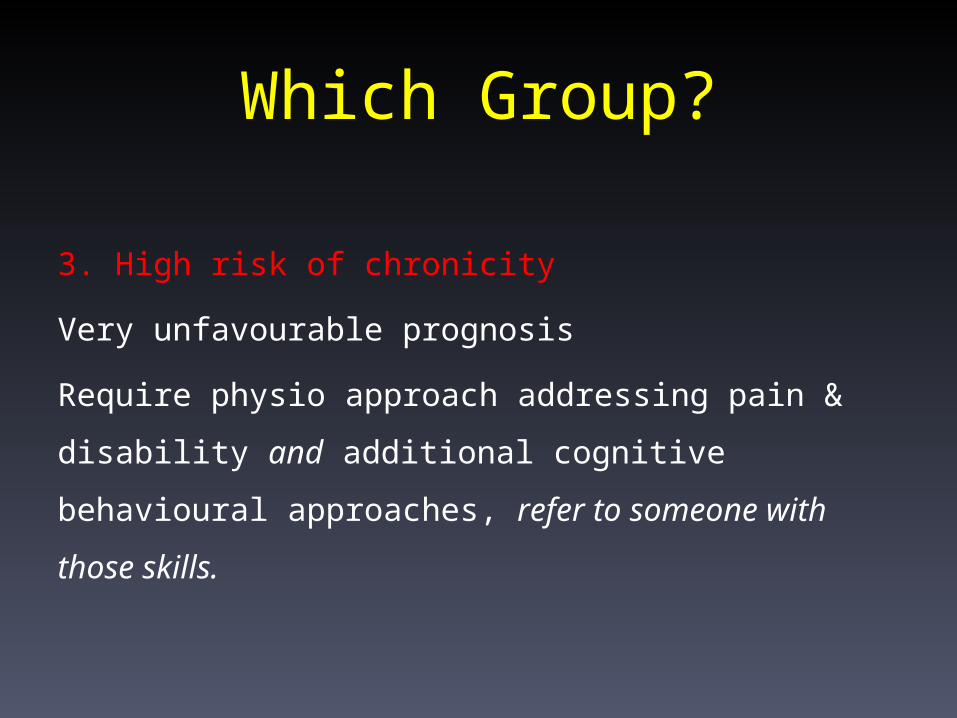
Which Group?
3. High risk of chronicity
Very unfavourable prognosis
Require physio approach addressing pain & disability and
additional cognitive behavioural approaches, refer to
someone with those skills.
Pain Management Programme (PMP)?
10 week programme at a hospital
Long waiting list
Average length of time from onset of CP to PMP is 5 yrs!
Chronicity likely to be entrenched by the time arrive!!
One-size-fits all policy
£10,000 per patient
Tier 2 service
• GPSI, ESP and health trainers with motivational skills to support patients in
self management and coping
• Focused on preventing and reducing long term disability and distress in
those with complex problems
• Patients need to have accepted that there is no further medical investigation
or treatment available and be willing to follow a self management approach
Tier 2 service
• A home based cognitive behavioral approach supporting the
self-management of chronic pain
1. Pain Management Plan book www.npowered.co.uk
• £12 per book (£7 in bulk)
• 9-10 yr old reading level
2. On-line www.pathwaythroughpain.com
• £150
Review no later than 12 weeks
• RED FLAGS?
• Alternative diagnosis?
• Screen risk of persisting pain-related disability and refer
Consider earlier review if :
• if patient not returned to work job is at risk
• there is a suspicion of opioid misuse/chemical coping
Take Home Pain Messages
• A multidimensional experience therefore in order to understand a persons
pain, all dimensions need to be considered: BPS model
• A key focus must be to enable patients to effectively manage their own
pain
• Prognostic Indicators (PI) exist that increase the risk of chronicity/long term
disability
• Screening for PI with subsequent allocation of patients into subgroups
enables targeted treatment of increasing complexity with the aim of
improving self management and reducing chronicity
References
• Accident compensation Corporation and the New Zealand Guidelines Group, Wellington, New Zealand. 1999
• Buchbinder R, Jolley D, Wyatt M. Population based intervention to change back pain beliefs and disability: three part
evaluation. BMJ. 2001 Jun 23;322(7301):1516-20.
• Croft PR, Macfarlane GJ, Papageorgiou AC, Thomas E, Silman AJ. The outcome of low back pain in general practice: a
prospective study. BMJ 1998;316:1356 –9.
• Deyo RA, Weinstein JN. Low back pain. N Engl J Med 2001; 344:363–70.
• Gatchel RJ, Peng Y, Peters ML, Fuchs PN, Turk DC. The Biopsychosocial Approach to Chronic Pain: Scientific Advances
and Future Directions. Psychological Bulletin. 2007;133:581-624.
• Hill JC, Dunn KM, Lewis M, Mullis R, Main CJ, Foster NE, et al. A primary care back pain screening tool: identifying patient
subgroups for initial treatment. Arthritis Rheum 2008;59(5):632–41www.keele.ac.uk
• Hill J. Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a
randomised controlled trial. The Lancet. 2011;9378(9802):1560-71.
• Weiner BK. Spine update: the biopsychosocial model and spine care. Spine. 2008;33(2):219-23.
Opioid Guidance
Full guidance for prescribers and patients available at
http://www.britishpainsociety.org/book_opioid_main.pdf
and
http://www.britishpainsociety.org/book_opioid_patient.pdf
Unsuitable for combined physio/cbt
• Patient unwilling/not ready yet for self- management approach
• Primary drug or alcohol problems
• Psychological or psychiatric problems which require urgent intervention
or which preclude the use of cognitive and behavioural methods
• Severe disability such that the basic requirements of attending treatment
exceed the patient’s current capacity. This depends in part on the
physical characteristics of the treatment setting and access to it.
Risk of chronicity yellow flags
• Beliefs that pain and activity are harmful
• “Sickness behaviours” – extended rest
• Low, negative mood, social withdrawal
• Problems at work (high or low demands), control, support, satisfaction
• Threat to benefits, issues with claim and compensation
• Beliefs / attitudes of friends or relatives (solicitousness, punitive responses
in an unhappy relationship)
• Medication and/or treatment not working
Common problematic beliefs about chronic pain.
“I may become paralysed if I am physically active”.
“My pain is either real (physical) or all in my head”.
“My suffering is someone else’s fault”.
“Nobody understands what I’m going through”.
“I need an operation”.
“Doctors should be able to cure me”.
“I should not be working”.
“I should rest in bed”.
“I should be on stronger medication”.
“I need to wait for a medical breakthrough”.
“I do not have a correct diagnosis”.
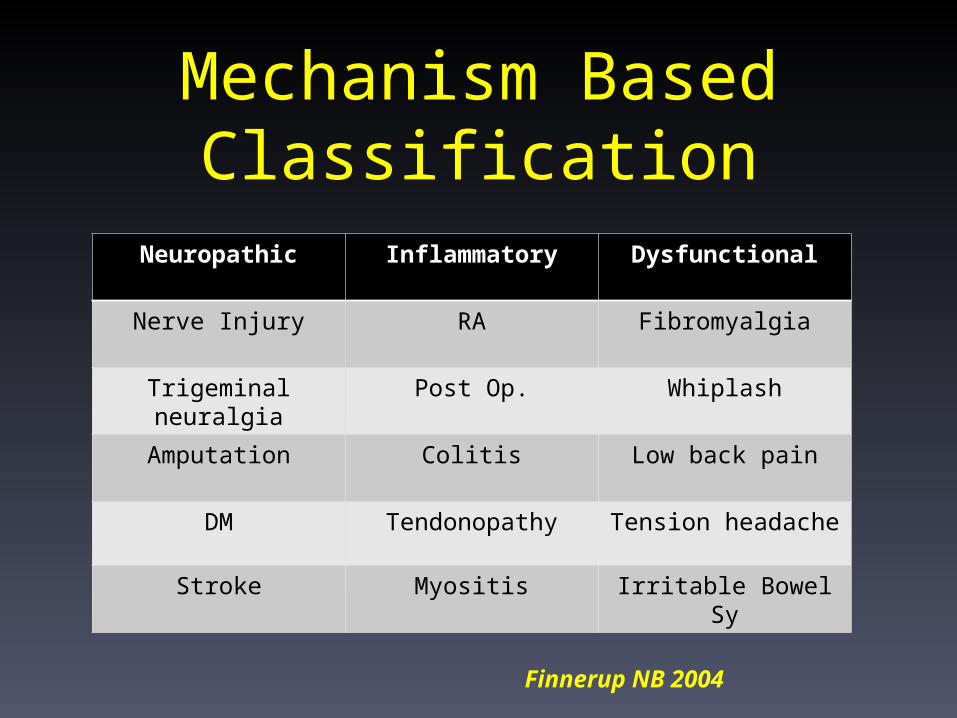
Neuropathic Inflammatory Dysfunctional
Nerve Injury RA Fibromyalgia
Trigeminal neuralgia Post Op. Whiplash
Amputation Colitis Low back pain
DM Tendonopathy Tension headache
Stroke Myositis Irritable Bowel Sy
Mechanism Based Classification
Finnerup NB 2004