
Document Control - northdevonhealth.nhs.uk · Neonatal, Neonatal Nursing, Neonates, Paediatric Tags...
17
Hypoglycaemia Management and Prevention in Neonates Guideline Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 1 of 17 Document Control Title Hypoglycaemia Management and Prevention in Neonates Guideline Author Author’s job title Senior Neonatal Staff Nurse and Educator Directorate Medical Department SCU Version Date Issued Status Comment / Changes / Approval 0.1 August 2015 Draft Initial version by SN Deborah Malpass and Dr Ragavendra Subba-Rao for comments. 0.2 November 2015 Draft Extensive editing following comments. Changes to format and order. Further changes to condense and simplify contents. 1.0 November 2015 Final draft Final draft for comments. 1.1 February 2016 Revision Changes after comments from Dr Selter and Sara Wright. 2.0 November 2016 Final Amendments made following comments from midwifery staff. 2.1 September 2017 Revision Feeding chart added to appendices Main Contact Special Care Unit North Devon District Hospital Raleigh Park Barnstaple, EX31 4JB Tel: Direct Dial – 01271 322610 Tel: Internal – 2610 Lead Director Medical Director Superseded Documents None Issue Date November 2016 Review Date November 2019 Review Cycle Three years Consulted with the following stakeholders: Paediatrics consultant group Neonatal nurses Head of midwifery / midwives Approval and Review Process Group/Committee Local Archive Reference G:\ Paediatric Resources/Neonates/Neonatal Guidelines/previous versions of guidelines Local Path G:\ Paediatric Resources/Neonates/Neonatal Guidelines Filename Hypoglycaemia Management and Prevention in Neonates Guideline v2.1
Transcript of Document Control - northdevonhealth.nhs.uk · Neonatal, Neonatal Nursing, Neonates, Paediatric Tags...
Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 1 of 17
Document Control
Title
Hypoglycaemia Management and Prevention in Neonates Guideline
Author
Author’s job title Senior Neonatal Staff Nurse and Educator
Directorate Medical
Department SCU
Version Date Issued Status Comment / Changes / Approval
0.1 August 2015
Draft Initial version by SN Deborah Malpass and Dr Ragavendra Subba-Rao for comments.
0.2 November 2015
Draft Extensive editing following comments. Changes to format and order. Further changes to condense and simplify contents.
1.0 November 2015
Final draft Final draft for comments.
1.1 February 2016
Revision Changes after comments from Dr Selter and Sara Wright.
2.0
November 2016
Final Amendments made following comments from midwifery staff.
2.1 September 2017
Revision Feeding chart added to appendices
Main Contact Special Care Unit North Devon District Hospital Raleigh Park Barnstaple, EX31 4JB
Tel: Direct Dial – 01271 322610 Tel: Internal – 2610
Lead Director Medical Director
Superseded Documents None
Issue Date November 2016
Review Date November 2019
Review Cycle Three years
Consulted with the following stakeholders:
Paediatrics consultant group
Neonatal nurses Head of midwifery / midwives
Approval and Review Process
Group/Committee
Local Archive Reference G:\ Paediatric Resources/Neonates/Neonatal Guidelines/previous versions of guidelines Local Path G:\ Paediatric Resources/Neonates/Neonatal Guidelines Filename Hypoglycaemia Management and Prevention in Neonates Guideline v2.1

Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 2 of 17
Policy categories for Trust’s internal website (BOB) Neonatal, Neonatal Nursing, Neonates, Paediatric
Tags for Trust’s internal website (Bob) Blood Glucose, Blood Sugar, Newborn, Infant, Jittery
Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 3 of 17
CONTENTS
Document Control........................................................................................................................ 1
1. Purpose ................................................................................................................................ 3
2. Definitions............................................................................................................................ 4
3. Responsibilities .................................................................................................................... 4
4. Introduction and Definition................................................................................................... 4
5. Pathophysiology ................................................................................................................... 5
6. Measurement of glucose ...................................................................................................... 5
7. Risk Factors for hypoglycaemia ............................................................................................. 6
8. Possible symptoms of hypoglycaemia in the newborn ........................................................... 6
9. Management of newborn infants to prevent hypoglycaemia ................................................. 7
10. Management of hypoglycaemia ............................................................................................ 7
11. SCBU management of infants ................................................................................................ 9
12. Process for Implementation and Monitoring Compliance and Effectiveness ........................... 10
Appendix 1 - Flowchart for the management of infants at risk of hypoglycaemia ........................ 11
Appendix 2 ................................................................................................................................ 12
Appendix 3 ................................................................................................................................ 13
Appendix 4 ................................................................................................................................ 13
Appendix 5 Feeding Chart .......................................................................................................... 14
13. References ......................................................................................................................... 16
14. Associated Documentation ................................................................................................. 17
1. Purpose
The purpose of this document is to give guidance on the management and prevention of hypoglycaemia in neonates on the post-natal ward, special care baby unit and paediatric ward if applicable.
This guideline applies to midwives and maternity care assistants on Delivery Suite and Bassett Ward, registered nurses and Health Care Assistants on the Special Care Unit and Caroline Thorpe paediatric ward and all paediatric doctors.
Implementation of this policy will ensure that:
The risks to neonates associated with hypoglycaemia are minimised.
Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 4 of 17
2. Definitions
3. Responsibilities
Role of all clinical staff including nurses, midwives and doctors who care for neonates:
To act in accordance with this guideline
To minimise the risks to neonates associated with hypoglycaemia
4. Introduction and Definition
This document highlights the importance of blood glucose levels in neonates within the first few days of life and explores best practice in relation to the management of hypoglycaemia in order to prevent harm to the neonate. The exact definition of neonatal hypoglycaemia is unclear, and the definition of clinically significant hypoglycaemia remains “one of the most confused and contentious issues in contemporary neonatology” (Cornblath et al, 2000). However, commonly defined and accepted normal blood sugar limits for neonates are 2.6mmol/L to 7mmol/L (Koh et al, 1988, Lucas et al, 1988, Bowell, 2010). Therefore, in neonates blood glucose of less than 2.6mmol/L is defined as hypoglycaemia (WHO, 1997).
EBM Expressed breast milk mmol/l millimole per litre ˃ Greater than ˂ Less than ≥ Greater than or equal to
Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 5 of 17
5. Pathophysiology
Glucose is transferred to the foetus by facilitated diffusion from the maternal circulation. In the first two hours after birth the blood glucose levels fall rapidly. In a healthy term infant the brain is protected by elevated levels of lactate and ketones, with an enhanced ability to use these metabolites. As a healthy term infant it is normal for the blood glucose level to fall and then rise again in the next few hours, either spontaneously or after feeding. Healthy asymptomatic term babies’ blood glucose levels may be normally low in the first few days of life, but this does not seem to have any adverse consequences. Glucose supply is essential, more so when there are conditions associated with high energy demands, such as the exhaustion of glycogen stores caused by birth asphyxia, or the increased metabolic rate caused by sepsis or hypothermia. Preterm infants are at high risk of neonatal hypoglycaemia due to decreased stores of glycogen and fat, poor feed tolerance and impaired hormonal responses. They are also at risk of hypothermia, which can then cause hypoglycaemia. Infants who have been Intra-Uterine Growth Restricted (IUGR) are also at increased risk due to the same reasons. Infants of diabetic mothers are at an increased risk of hypoglycaemia following birth due to the hyperinsulinaemic environment in-utero (Boxwell, 2010).
6. Measurement of glucose
Blood glucose measurement should be carried out using the Roche Performa ‘AccuCheck’ Blood Glucose Meter as screening tool
If AccuCheck reading is below 1.5 mmol/L send sample for laboratory testing for confirmation, but treat immediately
Always ensure ‘AccuCheck’ equipment is maintained and calibrated as per manufacturer’s instructions and that clinical staff are trained in use and signed-off as competent
Biochemistry laboratory using a paediatric grey bottle
Blood gas machine using a capillary tube or blood gas syringe

Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 6 of 17
7. Risk Factors for hypoglycaemia
1. Infants of diabetic mothers (including gestational diabetes)
2. Preterm infants (<37 weeks)
3. Infants Small for Gestational Age (SGA) Or Intra-Uterine Growth Restricted
(IUGR), (ie. <2.5kg and/or <2nd centile)
(see web link here for WHO 0-4 years Boys and Girls Growth Charts)
4. Infants of macrosomic appearance (large for gestational age)
5. Maternal medication (ie. beta blocker therapy, insulin)
6. Hypothermia
7. Haemolytic Disease of the Newborn (bilirubin approaching exchange
transfusion line)
8. Moderate to severe birth asphyxia (requiring admission)
9. Sepsis
10. Seizures
11. Poor feeding (As defined in Appendix F of Newborn Infant Feeding policy)
8. Possible symptoms of hypoglycaemia in the newborn
Tremors and jitteriness
Seizures
Apnoea
Lethargy
Hypotonia
Poor feeding
Weak or high pitched cry
“Jitteriness” alone is not a definitive sign of hypoglycaemia. Many babies will appear
jittery on handling, jitteriness is defined by UNICEF (2013) as “Excessive repetitive
movements of one or more limbs, which are unprovoked and usually relatively fast. It is
important to be sure that this movement is not simply a response to stimuli.”
Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 7 of 17
9. Management of newborn infants to prevent hypoglycaemia
Encourage skin to skin contact – a warm environment and early feed are the best
ways to prevent hypoglycaemia for all babies.
Early feed - Feed within an hour of birth if possible, and at least 3 hourly thereafter.
If baby not interested in first feed, make sure they have some expressed colostrum
and are fully assessed for signs or ill health and hypoglycaemia. If baby is well check
a blood glucose at least 2 hours after birth. If baby is unwell or symptomatic of
hypoglycaemia this can be done sooner. Follow guidance in Appendix F of Newborn
Infant Feeding policy.
Teach mother how to recognise feeding cues and how to hand express if
breastfeeding.
Monitor baby’s well being - All ‘at-risk’ infants must have an accurate up-to-date
feed chart and prior to feeds check the wellbeing of the baby, considering the infants
level of consciousness, tone, temperature, respiration, colour/perfusion (Unicef,
2013). This can be documented using the NEWS observation chart.
If a baby is less than the 10th centile on a GROW chart, then the weight should be
plotted on a WHO 0-4 years Boys or Girls Growth Chart to establish if they are below
the 2nd centile, and therefore at risk.
10. Management of hypoglycaemia
Blood glucose levels should be checked on all infants who have any risk factors.
Blood glucose should also be checked in infants who exhibit symptoms of
hypoglycaemia and a paediatrician should be informed.
Records of blood glucose measurements, treatment, response to treatment and the management decisions made as a result should be documented accurately in the baby’s purple post-natal notes or care plan and feed chart.
Hypoglycaemia should be treated with an immediate enteral feed, even if the baby is
asymptomatic. This should be the most appropriate method to gestation and clinical
status.
Expressed breast milk will be used for breast fed babies wherever possible.
Supplements with infant formula will be required only when the blood glucose is
below 2.5 mmols and breastfeeding has not been successful and the amount of
Expressed Breast Milk is insufficient to increase blood glucose.
Infants of women with diabetes should not be discharged home to community care until they at least 24 hours of age and have been seen by a medical professional who is satisfied they are feeding well and maintaining their blood glucose level ≥2.6 mmol/l (NICE, 2008).

Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 8 of 17
Infants of women with diabetes who are hypoglycaemic with symptoms should also have blood testing for polycythaemia, hyperbilirubinaemia, hypocalcemia and hypomagnesia. (NICE, 2008).
If the blood glucose of at ‘at-risk’ infant being tested is ≥ 2.6 mmol/l, the blood glucose should be checked before subsequent feeds. Stop monitoring when 3 successive pre-feed blood glucose levels are ≥ 2.6 mmol/l.
Feeding should be ‘baby-led’ as per Newborn Infant Feeding Policy, but with a maximum interval of 3 hours between feeds. Prior to feeds check the wellbeing of the baby, considering the infants level of consciousness, tone, temperature, respiration, colour/perfusion (Unicef, 2013).
All stages apply to the first blood sugar result, if the next result (the
second) remains <2.6 mmol/l, this should be discussed with a paediatrician
Blood glucose 1.5 mmol/l to 2.5 mmol/l
Give breastfeed with top-up of expressed breast milk or appropriate formula top-up, or if formula feeding give a full 3 hourly amount of first infant formula at 8-12ml/kg.
If baby reluctant to feed (even with top-up) follow the guidance in Appendix F of the ‘Newborn Infant Feeding policy’ and ask for paediatric review
Inform Paediatric SHO or Registrar to make them aware and discuss plan
Check blood glucose 1 hour post-feed If the second result remains <2.6 mmol/l, this should be discussed again with a paediatrician
Blood glucose <1.5mmol/l
Send blood glucose sample for laboratory testing
Give breastfeed and a full feed top-up of 8-12ml/kg, or a 3 hourly amount of appropriate
formula top-up at 8-12ml/kg each feed.
Inform Paediatrician and arrange to attend and clinically review infant
Consider admission to SCBU if feeds poorly tolerated, and consider 2.5ml/kg Dextrose bolus
over 5 minutes and/or intravenous 10% Dextrose infusion as per SCBU maintenance fluid
regime
If intravenous access is difficult consider use of Dextrose Gel 40% 0.5ml/kg massaged onto
the buccal membranes or Glucagon 0.1 mg/kg IM (maximum of 1mg).
Check blood glucose 1 hour-post feed / change
If the second result remains <2.6 mmol/l, this should be discussed with a paediatrician
˂1.0mmol/l or unreadable
Admit to SCBU and consider feeding interval or volume changes
If feeds poorly already tolerated consider intravenous bolus of 10% Dextrose at 2.5ml/kg
and/or commencing infusion as per SCBU maintenance fluid regime
Re-check blood glucose after 30 minutes
Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 9 of 17
11. SCBU management of infants
(for infants who are symptomatic, or high-risk infants where enteral feeds are contra-indicated, or infants who’s blood glucose remains low after intervention):
- Consider admission to SCBU
- Consider changing feed interval to more frequent ie. 1 or 2 hourly feeds
- Consider increasing fluid intake to next day mls/kg on SCBU maintenance
fluid regime
- Consider an intravenous Dextrose bolus at 2.5mls/kg
- Consider increasing intravenous 10% Dextrose infusion up to a maximum of
90ml/kg/day if newborn and monitor serum sodium levels to prevent
hyponatraemia
- If blood glucose still low, ensure Paediatric consultant has been informed,
and once up to 90mls/kg/day of intravenous 10% Dextrose, increase the
concentration rather than volume appropriately, up to 12.5% then 15% if
necessary. (If > 12.5% Dextrose is used, this must be given via a central line
to avoid complications - See appendix 3 for how to prepare).
- Infants over a few days old will need fluid maintenance volumes managed on
an individual basis
- If intravenous access is difficult ask for senior help and consider use of
Dextrose gel 40% 0.5ml/kg using an enteral syringe to draw up and then
massage onto the buccal membranes OR glucagon (Gluca-gen HypoKit in
fridge on SCBU) 0.1 mg/kg IM (maximum of 1.0mg)
- Investigations: When hypoglycaemia is persistent (glucose <2.2 mmol/L for
more than 72 hours) in the absence of clearly identifiable risk factors, further
investigation should be undertaken (as in appendix 2).
- Investigations for CRP, FBC and blood cultures and treatment with antibiotics
should be considered if sepsis is suspected.
-If repeated blood glucose is ≥ 2.6 mmol/l or rapidly rising and infant is on intravenous Dextrose,
re-start enteral feeds and titrate with Dextrose as tolerated and as per Paediatrician’s advice
Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 10 of 17
- Consider testing Calcium levels if infant is jittery
12. Process for Implementation and Monitoring Compliance and Effectiveness
Implementation of this guideline not required, as this practice is already in place in
all applicable areas.
Staff are informed of revised documentation. There is an expectation that staff are
responsible to keep updated on any improvements to practice and deliver care
accordingly.
Non-adherence to the guideline is reported by use of the Datix system. Incidents are
monitored and reviewed by the neonatal governance team and action plans made if
required. Individual cases are discussed at handover, on ward rounds and weekly on
grand rounds and are used for learning in safeguarding supervision.
Further discussion and reviews occur at Directorate meetings, Neonatal/Paediatric
Governance meetings Maternity Patient Safety Meetings and locally at Ward
meetings. Learning and action plans are cascaded at these meetings and
improvements implemented. Key findings and learning points will be disseminated
to relevant staff.

Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 11 of 17
Appendix 1 - Flowchart for the management of infants at risk of
hypoglycaemia
No
Yes
Care at birth to include:
• Dry baby, keep warm, initiate skin-to-skin contact
• First feed as soon as possible, always within the first hour; observation of wellbeing
Fed effectively?
Ongoing management to include:
* Review
Baby-led feeds (but at least 3 hourly)
Encourage mother to observe feeding
cues
Keep baby warm
Pre-feed blood glucose monitoring,
(initially prior to 2nd
feed), then stop when
level is normal x3
Blood glucose measurement above 2.6 mmol/l
Blood glucose measurement between 1.5 and 2.6 mmol/l
Proactive management:
Ongoing observation
Give breast or formula feed
If breastfeeding, hand express and give EBM (if not available continue expressing hourly)
Ongoing skin contact/ temperature maintenance
Newborns at risk of hypoglycaemia:
Infants of diabetic mothers Pre-term infants (<37 weeks) Low birth weight (<2.5 kgs or <2
nd centile)
Infants of macrosomic appearance Maternal medications Hypothermia Haemolytic Disease of Newborn Mod. or Sev. Birth Asphyxia Sepsis Seizures Poor feeding (See Appendix F Newborn Infant Feeding guideline)
Within 3-4 hours of age:
Review
Pre-feed glucose
measurement
*Review
Prior to feeds check:
Level of
consciousness
Tone
Temperature
Respirations
Colour
Inform paediatrician
Breastfeed followed by EBM or formula
full top-up by cup or nasogastric tube/
Formula feed full 3 hourly amount by
bottle or nasogastric tube
Repeat blood glucose in 1 hour
Blood glucose above 2.6 mmol/l
Blood glucose below 2.6 mmol/l
Symptomatic hypoglycaemia:
Apnoea Cyanosis Jitteriness Convulsions Or blood glucose below 1.5 mmol/l at any stage:
Refer baby to paediatrician
Blood glucose measurement below 1.5mmol/L
Refer to paediatrician, consider SCBU
Management’
Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 12 of 17
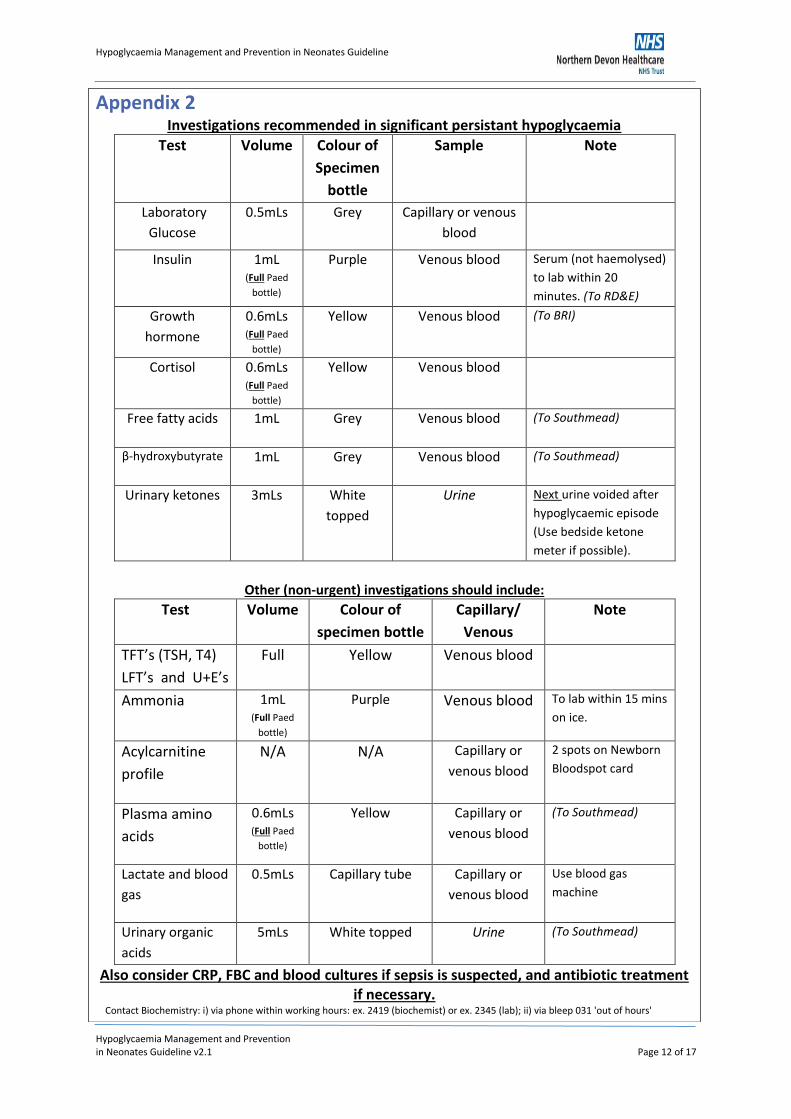
Appendix 2 Investigations recommended in significant persistant hypoglycaemia
Test Volume Colour of
Specimen
bottle
Sample Note
Laboratory
Glucose
0.5mLs Grey Capillary or venous
blood
Insulin 1mL (Full Paed
bottle)
Purple
Venous blood Serum (not haemolysed)
to lab within 20
minutes. (To RD&E)
Growth
hormone
0.6mLs (Full Paed
bottle)
Yellow Venous blood (To BRI)
Cortisol 0.6mLs (Full Paed
bottle)
Yellow Venous blood
Free fatty acids 1mL Grey Venous blood (To Southmead)
β-hydroxybutyrate 1mL Grey Venous blood (To Southmead)
Urinary ketones 3mLs White
topped
Urine Next urine voided after
hypoglycaemic episode
(Use bedside ketone
meter if possible).
Other (non-urgent) investigations should include:
Test Volume Colour of
specimen bottle
Capillary/
Venous
Note
TFT’s (TSH, T4)
LFT’s and U+E’s
Full Yellow Venous blood
Ammonia 1mL (Full Paed
bottle)
Purple
Venous blood To lab within 15 mins
on ice.
Acylcarnitine
profile
N/A N/A Capillary or
venous blood
2 spots on Newborn
Bloodspot card
Plasma amino
acids
0.6mLs (Full Paed
bottle)
Yellow Capillary or
venous blood
(To Southmead)
Lactate and blood
gas
0.5mLs Capillary tube Capillary or
venous blood
Use blood gas
machine
Urinary organic
acids
5mLs White topped Urine (To Southmead)
Also consider CRP, FBC and blood cultures if sepsis is suspected, and antibiotic treatment if necessary.
Contact Biochemistry: i) via phone within working hours: ex. 2419 (biochemist) or ex. 2345 (lab); ii) via bleep 031 'out of hours'
Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 13 of 17
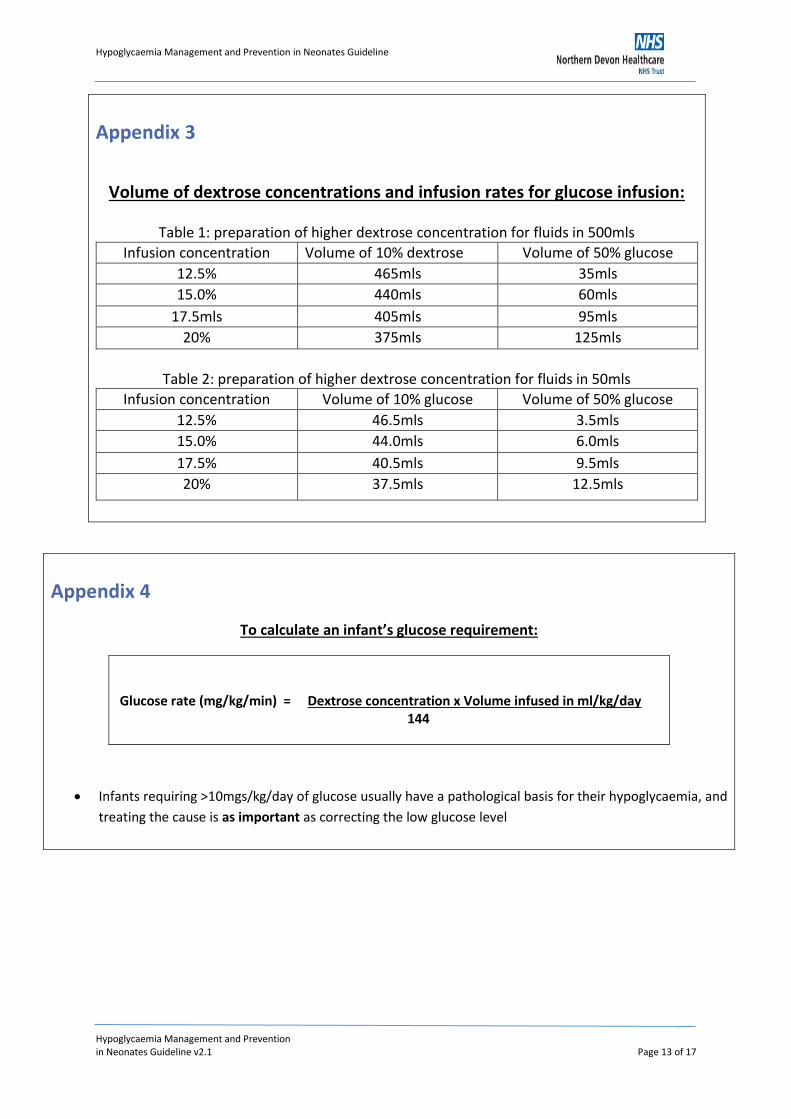
Appendix 3
Volume of dextrose concentrations and infusion rates for glucose infusion:
Table 1: preparation of higher dextrose concentration for fluids in 500mls
Infusion concentration Volume of 10% dextrose Volume of 50% glucose
12.5% 465mls 35mls
15.0% 440mls 60mls
17.5mls 405mls 95mls
20% 375mls 125mls
Table 2: preparation of higher dextrose concentration for fluids in 50mls
Infusion concentration Volume of 10% glucose Volume of 50% glucose
12.5% 46.5mls 3.5mls
15.0% 44.0mls 6.0mls
17.5% 40.5mls 9.5mls
20% 37.5mls 12.5mls
Appendix 4
To calculate an infant’s glucose requirement:
Glucose rate (mg/kg/min) = Dextrose concentration x Volume infused in ml/kg/day 144
Infants requiring ˃10mgs/kg/day of glucose usually have a pathological basis for their hypoglycaemia, and
treating the cause is as important as correcting the low glucose level
Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 14 of 17
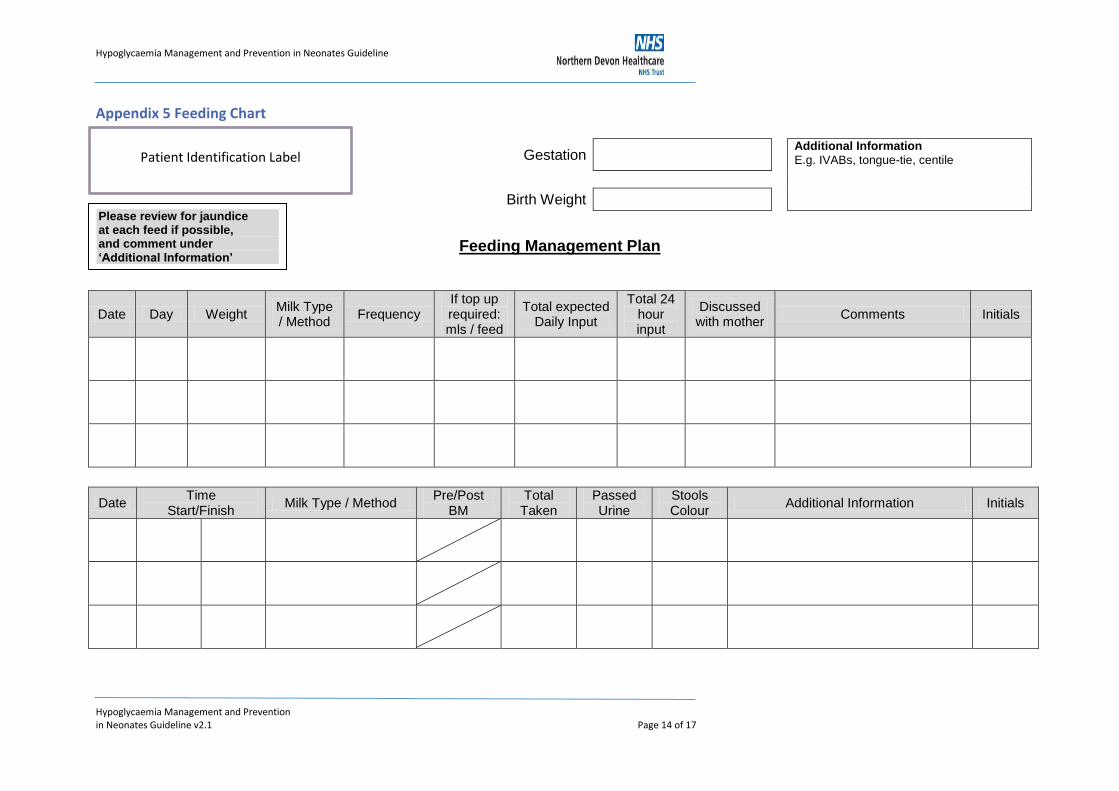
Appendix 5 Feeding Chart
Gestation Additional Information
E.g. IVABs, tongue-tie, centile
Birth Weight
Feeding Management Plan
Date Day Weight Milk Type / Method
Frequency If top up required: mls / feed
Total expected Daily Input
Total 24 hour input
Discussed with mother
Comments Initials
Date Time
Start/Finish Milk Type / Method
Pre/Post BM
Total Taken
Passed Urine
Stools Colour
Additional Information Initials
Please review for jaundice at each feed if possible, and comment under ‘Additional Information’
Patient Identification Label
Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 15 of 17
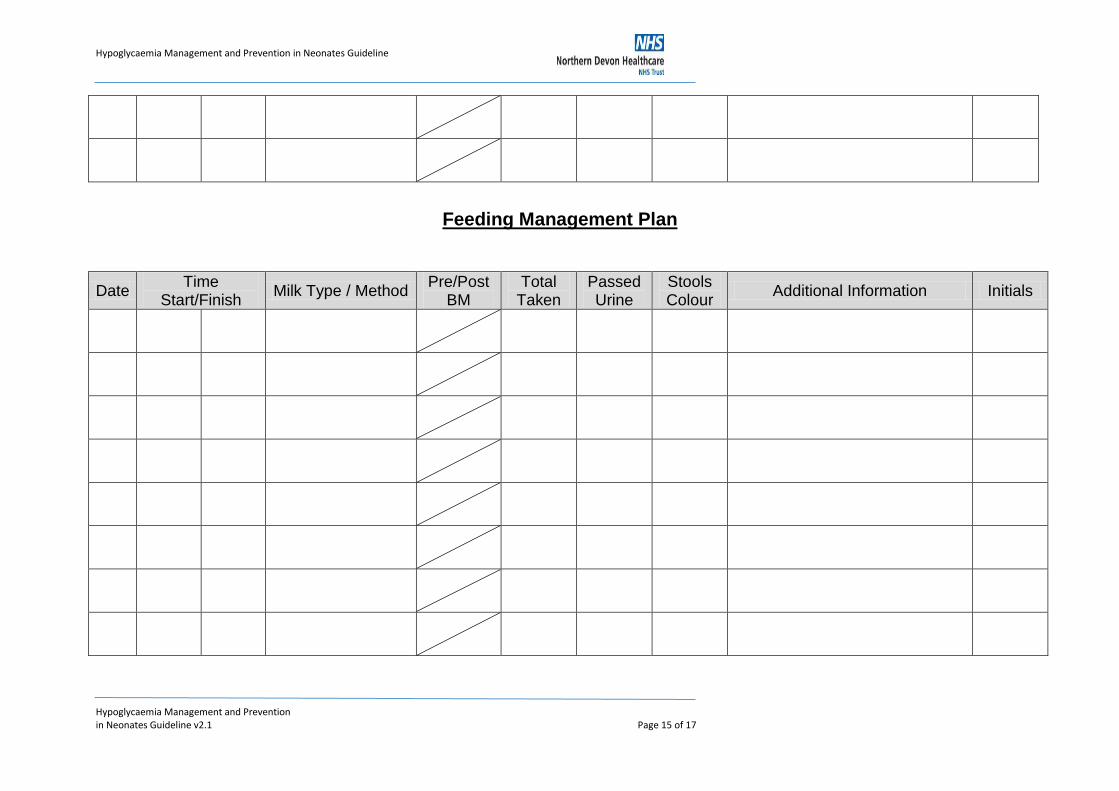
Feeding Management Plan
Date Time
Start/Finish Milk Type / Method
Pre/Post BM
Total Taken
Passed Urine
Stools Colour
Additional Information Initials
Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 16 of 17
13. References
Adamkin, D. H. (2009) Late preterm infants: severe hyperbilirubinemia and postnatal glucose homeostasis. Journal of Perinatology (29) 12-17. Boxwell, G. (2010) Neonatal Intensive Care Nursing, 2nd Edition. Routledge, New York. Cornblath, M. Hawdon, J. and Williams, A. (2000) Controversies regarding definition of neonatal hypoglycaemia: suggested operational thresholds. Paediatrics (105) 1141-1145. Cornblath, M, Schwartz, R. (1993) Hypoglycaemia in the neonate. Journal of Paediatric Endocrinology. (6) 113-129. Cornblath, M. and Ichord, R. (2000) Hypoglycaemia in the neonate. Seminars in Perinatology (24) 136. CEMACH (2007) Diabetes in pregnancy: caring for the baby after birth. Findings of a national enquiry. Hawdon, J. M., Ward-Platt, M. P., Aynsley-Green, A. (1992) Patterns of metabolic adaptation for preterm and term infants in the first neonatal week. Archives of Disease in Childhood (67) 357-365. Hay, Jr. W., Faju, T., Higgins, R. D., Kalhan, S. C., Devaskar, S. U. (2009) Knowledge gaps and research needs for understanding and treating neonatal hypoglycemia: workshop report from Eunice Kennedy Shriver National Institute of Child Health and Human Development. Journal of Pediatrics, 155 (5) 612-7. Koh, T. H. H. G., Aynsley-Green, A., Tarbit, M. et al. (1998) Neural dysfunction during hypoglycaemia. Archives of Disease in Childhood (63)1353-1358. Lucas, A., Morley, R., Cole, T. J. (1988) Adverse neurodevelopmental outcome of moderate neonatal hypoglycaemia. British Medical Journal, 297 (6659):1304-8. National Institute for Health and Clinical Excellence (2008) Diabetes in pregnancy. Management of diabetes and its complications from pre-conception to the postnatal period London: NICE. [Available on-line at: www.nice.org.uk] Royal College of Anaesthetists, Royal College of Midwives, Royal College of Obstetricians and Gynaecologists, Royal College of Paediatrics and Child Health. (2007) Safer Childbirth: Minimum Standards for the Organisation and Delivery of Care in Labour. London RCOG Press [Available on-line at: www.rcog.org.uk] Rozance, P. J. and Hay, W. W. (2010) Neonatal Hyperglycaemia. American Academy of Pediatrics. 11 (11) 632-640. Stenninger, E., Flink, R., Eriksson, B. and Sahlen, C. (1998) Long-term neurological dysfunction and neonatal hypoglycaemia after diabetic pregnancy. Archives of Disease in Children and Foetal and Neonatal Education, 79 (3) 174-9.
Hypoglycaemia Management and Prevention in Neonates Guideline
Hypoglycaemia Management and Prevention in Neonates Guideline v2.1 Page 17 of 17
UNICEF UK Baby Friendly Initiative (2007). Guidance on the development of policies and guidelines for the prevention and management of Hypoglycaemia of the Newborn. UNICEF. [Available on-line at www.babyfriendly.org.uk]
14. Associated Documentation
NDHT Newborn Infant Feeding policy and guidelines
NDHT Care of the Newborn Immediately After Birth guideline
NDHT Thermal Care of the Neonate guideline


















