Document
6
OPEN PEDIATRIC REVIEW Musculoskeletal pain in overweight and obese children SM Smith 1,2 , B Sumar 1 and KA Dixon 1 This review seeks to provide a current overview of musculoskeletal pain in overweight and obese children. Databases searched were Academic Search Complete, CINAHL, Medline, Proquest Health and Medical Complete, Scopus, Google Scholar, SPORTDiscuss and Trove for studies published between 1 January 2000 and 30 December 2012. We used a broad definition of children within a 3- to 18-year age range. The search strategy included the following terms: obesity, morbid obesity, overweight, pain, musculoskeletal pain, child, adolescent, chronic pain, back pain, lower back pain, knee pain, hip pain, foot pain and pelvic pain. Two authors independently assessed each record, and any disagreement was resolved by the third author. Data were analysed using a narrative thematic approach owing to the heterogeneity of reported outcome measures. Ninety-seven records were initially identified using a variety of terms associated with children, obesity and musculoskeletal pain. Ten studies were included for thematic analysis when predetermined inclusion criteria were applied. Bone deformity and dysfunction, pain reporting and the impact of children being overweight or obese on physical activity, exercise and quality of life were the three themes identified from the literature. Chronic pain, obesity and a reduction in physical functioning and activity may contribute to a cycle of weight gain that affects a child’s quality of life. Future studies are required to examine the sequela of overweight and obese children experiencing chronic musculoskeletal pain. International Journal of Obesity (2014) 38, 11–15; doi:10.1038/ijo.2013.187 Keywords: adolescent; overweight; pain; musculoskeletal; disability; child health INTRODUCTION Worldwide childhood obesity has increased by 50% in the past 30 years, with B43 million children under the age of five being reported as overweight. 1 The WHO defines overweight and obesity as abnormal or excessive fat accumulation that may impair health. 1 In Australia, obesity, as defined by WHO, continues to be a major public health problem with over 20% of school children being either overweight or obese 2 and children from low socioeconomic areas being 70% more likely to be either overweight or obese. 3 Central obesity, as measured by waist circumference, is thought to be a more reliable indicator of health problems than total body mass for people with a body mass index (BMI) of less than 35. 4 Studies into obesity tend to report indices such as BMI and waist circumference. However, a definition of obesity and its clinical diagnosis is often difficult and remains controversial, with waist circumference, BMI and skin folds being the more common non-invasive measurements used. 5 A number of reports suggest that overweight and obese children have subsequently developed short- and long-term health problems that continue into adult life. 5,6 In particular, psychological co- morbidities associated with being overweight or obese during childhood and adolescence are well documented. 7,8 These health problems include social isolation, depression, loneliness and low self-esteem, and more recently depressive symptoms have been linked with cardiorespiratory fitness in obese adolescents. 9,10 Obesity in children is a significant public health problem, and it has the potential to have an impact on a child’s osteoarticular health, resulting in ongoing chronic pain. In adults, obesity is associated with physiological disability, in particular joint and chronic conditions such as cardiovascular disease, diabetes and some cancers. 1 Degenerative osteoarthritis and cartilage breakdown along with musculoskeletal pain have been reported as part of the disability spectrum related to obesity. 11 These conditions significantly reduce a person’s ability to exercise, and in addition chronic pain has been reported to negatively influence a person’s quality of life. 12 Given that being overweight or obese in adult life affects health and well-being, the potential for deleterious effects on the musculoskeletal system from being overweight or obese in childhood requires further attention. Chronic nonspecific musculoskeletal pain in children and adolescents has been reported as a common occurrence. 13–15 Children affected by chronic musculoskeletal pain have been found to have increased levels of anxiety and depression, as well as lower levels of activity. 16 Recent reviews on general musculoskeletal pain identified the most frequent site of nonspecific musculoskeletal pain in children in the lower limbs, with some estimates suggesting that this affects 24% of children aged between 6 and 10 years of age. 17,18 Interestingly, Tanamas and co-workers 19 found that an increase in adiposity and fat distribution across the body is related to foot pain, and yet this relationship is not evident with an increase in muscle mass. Although psychological wellness in children can be linked with increased levels of activity, an understanding of the role of musculoskeletal pain on the activity levels of overweight and obese children appears to be limited. The aim of this review was to provide a current overview of musculoskeletal pain in overweight and obese children with a focus on osteoarticular changes and joint health, reporting of musculoskeletal pain and the impact of pain on activity, exercise and quality-of-life indices. 1 Family and Community Health Research Group, School of Nursing and Midwifery, University of Western Sydney, Campbelltown, NSW, Australia and 2 Centre for Pharmacology and Therapeutics, Imperial College, Chelsea and Westminster Campus, London, UK. Correspondence: Professor SM Smith, Family and Community Health Research Group, School of Nursing and Midwifery, University of Western Sydney, Locked Bag 1797, Penrith, NSW 2751, Australia. E-mail: [email protected] Received 7 August 2012; revised 11 September 2013; accepted 21 September 2013; accepted article preview online 30 September 2013; advance online publication, 29 October 2013 International Journal of Obesity (2014) 38, 11–15 & 2014 Macmillan Publishers Limited All rights reserved 0307-0565/14 www.nature.com/ijo
-
Upload
nur-khairiyah -
Category
Documents
-
view
5 -
download
2
Transcript of Document
-
OPEN
PEDIATRIC REVIEW
Musculoskeletal pain in overweight and obese childrenSM Smith1,2, B Sumar1 and KA Dixon1
This review seeks to provide a current overview of musculoskeletal pain in overweight and obese children. Databases searchedwere Academic Search Complete, CINAHL, Medline, Proquest Health and Medical Complete, Scopus, Google Scholar, SPORTDiscussand Trove for studies published between 1 January 2000 and 30 December 2012. We used a broad denition of children within a3- to 18-year age range. The search strategy included the following terms: obesity, morbid obesity, overweight, pain,musculoskeletal pain, child, adolescent, chronic pain, back pain, lower back pain, knee pain, hip pain, foot pain and pelvic pain.Two authors independently assessed each record, and any disagreement was resolved by the third author. Data were analysedusing a narrative thematic approach owing to the heterogeneity of reported outcome measures. Ninety-seven records were initiallyidentied using a variety of terms associated with children, obesity and musculoskeletal pain. Ten studies were included forthematic analysis when predetermined inclusion criteria were applied. Bone deformity and dysfunction, pain reporting and theimpact of children being overweight or obese on physical activity, exercise and quality of life were the three themes identied fromthe literature. Chronic pain, obesity and a reduction in physical functioning and activity may contribute to a cycle of weight gainthat affects a childs quality of life. Future studies are required to examine the sequela of overweight and obese childrenexperiencing chronic musculoskeletal pain.
International Journal of Obesity (2014) 38, 1115; doi:10.1038/ijo.2013.187
Keywords: adolescent; overweight; pain; musculoskeletal; disability; child health
INTRODUCTIONWorldwide childhood obesity has increased by 50% in the past 30years, with B43 million children under the age of ve beingreported as overweight.1 The WHO denes overweight andobesity as abnormal or excessive fat accumulation that mayimpair health.1 In Australia, obesity, as dened by WHO, continuesto be a major public health problem with over 20% of schoolchildren being either overweight or obese2 and children from lowsocioeconomic areas being 70% more likely to be eitheroverweight or obese.3 Central obesity, as measured by waistcircumference, is thought to be a more reliable indicator of healthproblems than total body mass for people with a body mass index(BMI) of less than 35.4 Studies into obesity tend to report indicessuch as BMI and waist circumference. However, a denition ofobesity and its clinical diagnosis is often difcult and remainscontroversial, with waist circumference, BMI and skin folds beingthe more common non-invasive measurements used.5 A numberof reports suggest that overweight and obese children havesubsequently developed short- and long-term health problemsthat continue into adult life.5,6 In particular, psychological co-morbidities associated with being overweight or obese duringchildhood and adolescence are well documented.7,8 These healthproblems include social isolation, depression, loneliness and lowself-esteem, and more recently depressive symptoms have beenlinked with cardiorespiratory tness in obese adolescents.9,10
Obesity in children is a signicant public health problem, and ithas the potential to have an impact on a childs osteoarticularhealth, resulting in ongoing chronic pain.
In adults, obesity is associated with physiological disability, inparticular joint and chronic conditions such as cardiovascular
disease, diabetes and some cancers.1 Degenerative osteoarthritisand cartilage breakdown along with musculoskeletal pain havebeen reported as part of the disability spectrum related toobesity.11 These conditions signicantly reduce a persons abilityto exercise, and in addition chronic pain has been reported tonegatively inuence a persons quality of life.12 Given that beingoverweight or obese in adult life affects health and well-being, thepotential for deleterious effects on the musculoskeletal systemfrom being overweight or obese in childhood requires furtherattention.
Chronic nonspecic musculoskeletal pain in children andadolescents has been reported as a common occurrence.1315
Children affected by chronic musculoskeletal pain have beenfound to have increased levels of anxiety and depression, as wellas lower levels of activity.16 Recent reviews on generalmusculoskeletal pain identied the most frequent site ofnonspecic musculoskeletal pain in children in the lower limbs,with some estimates suggesting that this affects 24% of childrenaged between 6 and 10 years of age.17,18 Interestingly, Tanamasand co-workers19 found that an increase in adiposity and fatdistribution across the body is related to foot pain, and yet thisrelationship is not evident with an increase in muscle mass.Although psychological wellness in children can be linked withincreased levels of activity, an understanding of the role ofmusculoskeletal pain on the activity levels of overweight andobese children appears to be limited. The aim of this review wasto provide a current overview of musculoskeletal pain inoverweight and obese children with a focus on osteoarticularchanges and joint health, reporting of musculoskeletal pain andthe impact of pain on activity, exercise and quality-of-life indices.
1Family and Community Health Research Group, School of Nursing and Midwifery, University of Western Sydney, Campbelltown, NSW, Australia and 2Centre for Pharmacologyand Therapeutics, Imperial College, Chelsea and Westminster Campus, London, UK. Correspondence: Professor SM Smith, Family and Community Health Research Group, Schoolof Nursing and Midwifery, University of Western Sydney, Locked Bag 1797, Penrith, NSW 2751, Australia.E-mail: [email protected] 7 August 2012; revised 11 September 2013; accepted 21 September 2013; accepted article preview online 30 September 2013; advance online publication, 29 October 2013
International Journal of Obesity (2014) 38, 1115& 2014 Macmillan Publishers Limited All rights reserved 0307-0565/14
www.nature.com/ijo
-
MATERIALS AND METHODSThis literature review was carried out using a systematic method20
described in the Preferred Reporting Items for Systematic Reviews andMeta-Analyses guideline. We developed a detailed protocol withprescribed inclusion and exclusion criteria to support the quality andconsistency within the literature review process. Studies associated withchildren who were dened as overweight or obese had to meet thefollowing criteria to be included: written in English, published after January2000; age range of 218 years; and report musculoskeletal pain. The typesof studies included in this review were randomised control trials, cohortstudies, quasi-experimental studies, controlled before and after studies andpatient reports. We excluded discussion papers, reviews, opinions andpolicy reports. A predened search strategy was used to examinedatabases for publications; after excluding records that did not meet theeligibility criteria, ten studies were included for synthesis, and themesassociated with musculoskeletal pain and overweight or obese childrenwere generated.
Search strategy and selection criteriaAcademic Search Complete, Cinahl, Google Scholar, Medline, ProquestHealth and Medical Complete, Scopus, SPORTDiscuss and Trove databaseswere searched for studies published between 1 January 2000 and 30December 2012. The literature review search strategy (Table 1) used acombination of MESH terms in the title/abstract for obesity and pain,limiting to children and teenagers, and used the following terms: obesity,morbid obesity, overweight, pain, musculoskeletal pain, child, adolescent,chronic pain, back pain, lower back pain, knee pain, hip pain, foot pain andpelvic pain.
Participants and denitionsFor this literature review, a broad denition of childhood to includechildren and adolescents within a range from 3 years to 18 years of agewas used. For musculoskeletal pain, terms such as joint pain and musclepain either objectively or subjectively reported were accepted. Forexample, joint pain may include shoulder pain, foot pain and knee pain.
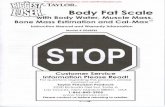
Search outcomeBy searching the electronic databases, 70 records were retrieved. Thereference list of each of the identied reports, reviews and originalresearch articles were manually searched for additional studies, with afurther 27 studies identied. Only manuscripts in English were consideredfor assessment. Three records were removed as duplicates. Abstracts foreach of the 94 records had the inclusion criteria applied separately by twoof the authors. The review owchart outlines the records identied orexcluded at each phase of the review process (Figure 1). Two authors
(BS and KD) independently assessed each abstract, and any disagreementwas resolved by the third author (SMS). Heterogeneity of reportedoutcome measures was identied, and subsequently a qualitative analyticprocess of thematic analysis was undertaken. Braun and Clarke21 (p 79)suggest that thematic analysis is a process for identifying, analysing andreporting patterns (themes) within data.
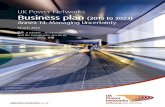
Data abstractionOn completion of the independent review of abstracts, full texts of theremaining ten manuscripts were sourced (Table 2). Each manuscript wascritically appraised by each individual author and the data weresummarised to develop the themes. Consensus on the themes wasachieved by the three authors. This review, however, did not assessinterventions for weight loss and/or general pain reduction; rather, itfocused specically on the ultimate goal of providing a current under-standing of musculoskeletal pain associated with overweight and obesechildren. Three central themes associated with musculoskeletal pain inoverweight and obese children were generated, and they comprisedmusculo-skeletal health, joint alignment and dysfunction, pain reportingand the impact of pain on physical activity, exercise and quality of life.
RESULTSImpact of being overweight or obese on musculoskeletal health,joint alignment and dysfunctionNumerous studies report the signicant impact of being over-weight or obese on bone and joint health in adults.2224 Key issuesare primarily bone demineralisation, deformity, dysfunction andthe associated pain due to these changes in body structures. Inthis review, we were able to identify three studies that reporteddysfunction and/or deformity of bone structure in overweightor obese children who report pain. The rst study examinedorthopaedic complications in overweight children andadolescents and found a signicantly higher prevalence ofskeletal fractures compared with non-overweight subjects.25
Similarly, a Dutch study identied that overweight and obesechildren self-reported ankle and foot problems26 and potentiallyimpacted on their ongoing joint health. More concerning was deSa Pintos study that reports the osteoarticular alterations in obesechildren who had a BMI above the 95th percentile withsignicantly higher reports of pain when compared with normal-weight children.27 The study also found a higher frequency ofgenu valgum, commonly called knock-knee, (55.1%) and a higherfrequency of genu recurvatum, which is an excessive extension of
Table 1. Strategies used to search the literature on musculoskeletal pain in overweight and obese children
Specific search elements Steps in search process Term combination
Characteristic 1 *Obesity/2 obes*.ab,ti.3 *Obesity, Morbid/4 *Overweight/5 overweight.ab,ti.
Combining characteristic terms 6 1 or 2 or 3 or 4 or 5Population 7 limit 6 to (child (6 to 12 years) or adolescent (13 to 18 years))Symptom 8 *Pain/
9 pain.ab,ti.10 *Chronic Pain/
Body region 11 *Back Pain/12 *Low Back Pain/13 (knee adj3 pain).ab,ti.14 (hip adj3 pain).ab,ti.15 (foot adj3 pain).ab,ti.16 (musculoskeletal adj3 pain).ab,ti.17 *Pelvic pain/18 (pelvi* adj3 pain).ab,ti.
Final search 19 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18
b, final search was limited to English text human subjects, age range and undertaken between 1 January 2000 and 30 December 2012. a, * before the MESH termmeans focused and not exploded. m, ab.ti limits search to abstract and title. j, indicates searching for term within three words of each other regardless of order.
Musculoskeletal pain in childrenSM Smith et al
12
International Journal of Obesity (2014) 11 15 & 2014 Macmillan Publishers Limited
-
the knee-joint, in obese children (24.2%) compared with thecontrol group of normal-weight children (2%). These studieshighlight a serious risk to the skeletal system of a child who iseither overweight or obese and the pain associated withmusculoskeletal dysfunction and deformity.
Musculoskeletal pain reporting in overweight and obese childrenPain reporting is central to this review, and we sought tounderstand from the literature the most common sites ofmusculoskeletal pain, how pain is reported and any differencesthat occur within the studied populations of overweight andobese children. Of the studies reviewed, musculoskeletal pain wasidentied through medical chart review and/or self-report byparents and/or children. Two retrospective medical chart reviewsof children and adolescents used musculoskeletal pain as theprimary inclusion criterion in two differing patient populations: apaediatric clinical trial unit and paediatric pain clinic.25,28 Sixprospective studies recorded pain from participating overweightand obese children and adolescents compared with normal-weight children in a variety of settings. Two of these studiesincluded participants from obesity clinics.27,29 One study was in aspecialised orthopaedic service30 and in primary care,26 and theremaining two studies assessed children31,32 in a primary schoolsetting.
The sites of pain in these overweight and obese paediatricpopulations differ in each study. Four studies reported musculo-skeletal pain sites, for example, lower back, knees, ankles andfeet,2527,31 and one study reported neck pain.26 However, threestudies reported nonspecic musculoskeletal pain withoutspecifying the pain site.28,30,32 Interestingly, children whoreported musculoskeletal pain in the back, hip, knee and/orankle were found to have a signicantly higher BMI than thosewithout pain, with the odds of having joint pain increased by 10%for every 10-kg increase of weight and an increase of 3% for everyunit increase in BMI.29 Recently, a study that sought to estimateoverall and age-specic associations between obesity andmusculoskeletal pain in children found a signicant increase inpain in the lower extremities of extremely obese children acrossthree age ranges encompassing children aged between 2 and 19years compared with normal-weight children.33
During this review, we identied only one scale (other than aquality-of-life tool) that was specically used to examine theimpact of pain in obese children. Podeszwa30 used the PediatricOutcomes Data Collection Instrument to determine obese
childrens overall health, pain and their ability to participate inactivities of daily life and vigorous exercise. They found that olderobese girls (age 411 and o18) had signicant reduction infunction, mobility and happiness, with a substantial increase inpain; however, obese boys had a greater reduction in mobilitywithout an increase in pain compared with normal-weight boys.This evidence highlights the potential for signicant disability inadult life, apart from chronic illnesses such as diabetes type 2 andheart disease, should these children continue to remainoverweight or obese.
Impact of pain on activity, exercise and quality of lifeHealth-related quality-of-life tools have been extensively used inadult obesity studies; however, very little research on overweightand obese children has been reported in terms of quality-of-lifeindices. Recently, a small number of studies have sought todescribe the impact of musculoskeletal dysfunction using thehealth-related quality-of-life tools. Taylor et al.25 identiedoverweight children through chart audit, dual X-rayabsorptiometry scans and data from the impact of weight onquality-of-life adolescent questionnaire as having moremusculoskeletal discomfort, impaired mobility and lower-extremity malalignment. These three health issues may have animpact on a childs quality of life and have been linked with areduction in the likelihood of physical activity when comparedwith non-overweight children. Hainsworth et al.28 studied thehealth impacts on children who experience chronic pain using thehealth-related quality-of-life tool and identied that 48% of obesechildren experience musculoskeletal pain more than other typesof pain such as headache or abdominal pain. The premise that acombination of chronic pain and obesity reduces physicalfunctioning was a signicant nding of Hainsworths study, aswas the nding that obesity and impaired physical functioningwas six times higher than obesity alone in this chronic painpaediatric population. This research suggests that there may be acyclic inter-relatedness between chronic pain, obesity and levelsof physical activity.
Wilson et al.34 conrm the association between physical activityand obesity as reported in Hainsworths study. Wilson et al. found,in a population of obese children who were receiving treatmentfor musculoskeletal pain, that the parents often reportedlimitations in the child being able to participate in exercise andsports. Specically, when parents are asked to report on theirchildrens activity, the parents relate the childs activity levels tothe childs weight, whereas children associate their activity levelwith their level of pain. Wilson et al. found that the relationshipbetween being overweight or obese and pain may be partiallymediated by physical activity levels. Both studies suggest aspiralling effect in which overweight and obese children withmusculoskeletal pain reduce their activity, potentially contributingto further weight gain. With few studies in this area, clearly moreresearch is required to develop a greater understanding of theimpact of activity and exercise on overweight and obese childrenwho cope with ongoing musculoskeletal pain and the effect ontheir short- and long-term quality of life.
DISCUSSIONThere is substantive evidence from many countries that anincreasing number of children are becoming overweight andobese.35 Most of the studies identied through this review werewithin specialist chronic pain or obesity paediatric clinicpopulations, and a small number of studies based in primarycare or used electronic health records addressed the issue ofobesity and musculoskeletal pain in children and adolescents.
The impact of being overweight or obese on a childs skeletalsystem has been reported in terms of joint health and dysfunction
Additional records identifiedthrough other sources
n=27
Records identified throughdatabase searching
n=70
Records after duplicates removedn=94
Records excludedwhen inclusion criteria
appliedn=70
Records screenedn=94
Full-text articlesexcluded with reason:
Adult populationReview articlePain notrecordedPain other than musculoskeletaln=14
Full-text articles assessed foreligibility
n=24
Studies included in synthesisn=10
Figure 1. Retrieval of published studies process flow diagram.
Musculoskeletal pain in childrenSM Smith et al
13
& 2014 Macmillan Publishers Limited International Journal of Obesity (2014) 11 15
-
resulting in more ankle, foot and knee problems than childrenwho are within a normal-weight range for their age.26 Obesity isassociated with pain, joint dysfunction27 and bone fractures.25 Theprogression of these osteoarticular changes into adult life, ifweight management is not achieved, could lead to the need forongoing orthopaedic treatment.33 Overweight and obese childrenreported musculoskeletal pain primarily due to changes withinarticulating joints such as knee and ankle, and as a result offractures.2527 Kesslers and other studies regarding bone fracturesreport signicantly higher rates of factures in overweight andobese children, yet pain in these studies is not reported.3639
From this review, it was found that children and their parentsmay report pain and activity differently. In the context of activity,children linked their pain with levels of activity, whereas parentsassociated activity with the childs weight.34 Therefore, the waypain is self-reported may require further validation from theperspectives of both parent and child. The relationship betweenincrease in BMI, weight and pain demonstrates a risk factor fordamage to the musculoskeletal structure, and this damage is oftenexpressed by the child as pain.25,26 Evidence is emerging to
suggest that a reduction in physical functioning of obese andoverweight children may occur and be evident through the childsexpression of pain, further impacting on their self-esteemresulting in a poorer quality of life.25,28,30 Changes to themusculoskeletal system in overweight and obese children havebeen shown to negatively inuence motor performance, includingmuscle strength, balance and walking, through changes in plantarexion during the swing phase of walking, resulting in a atterfoot.4044 Hip and knee exion is also affected in obese childrenowing to an increase in concentric contraction of hip exors,45
creating higher energy transfer and loads across hip joints,46
resulting in a change in gait to cope with the childs increasedbody mass. Therefore, the reporting of musculoskeletal pain byoverweight children may reect a signicant marker of a reductionin osteoarticular health and changes to skeletal structure. Inreviewing the literature associated with obese and overweightchildren, there appears to be links between bone health, pain,physical activity and quality of life, and these links may beimportant if the issue of musculoskeletal pain in this group ofchildren is to be addressed.
Table 2. Studies included in the review
First author Age (years) Country Year Sample size Type of study and measurement Results Determinant of overweight and obesity
Podeszwa, DA 218 USA 2006 50 Prospective PODCI validation study usingBMI, PODCI and life satisfaction question
Recorded impairment in sportsand pain in obese childrencompared with normative data.Data for this difference notprovided
BMI for age exceeding 95th percentile(based on growth charts developed bythe CDC that correct for genderdifferences)
Stovitz, S 318 USA 2008 135 Prospective descriptive cross-sectionalstudy using BMI and pain assessment. ORof pain for the knee and hip in obesechildren
Knee: OR 1.13 per 10 kg increasein weight, 95% CI: 1.01 1.29.OR 1.04 per unit increase in BMI,95% CI: 1.01 1.08Hip: OR 1.29 per 10 kg increase inweight, 95% CI: 1.05 1.60.OR 1.09 per unit increase in BMI,95% CI: 1.03 1.16
BMI for age exceeding 95th percentile(based on growth charts developed bythe CDC that correct for genderdifferences)
de Sa Pinto, AL 714 Brazil 2006 49 Prospective cross-sectional study usingBMI, limb flexibility, posture examination,clinic questionnaire, tender points andfibromyalgia criteria. Frequency of genuvalgum and genu recurvatum in obesechildren compared with normal-weightchildren
Genu valgum: 55.1% vs 2%;Po0.0001Genu recurvatum: 24.2% vs 2%;Po0.001
BMI for age exceeding 95th percentile (asdetermined by the National Health andNutrition Examination Survey)
Bell, LM 715 Australia 2011 283 Cohort study using BMI, structuredinterview, medical assessment,anthropometrics and fasting bloodinvestigations, including oral glucosetolerance test
Chi-square P 0.010OR compared with controlsFor overweight children: 1.53For obese: 4.09
Based on international age- and gender-specific BMI cutoffs
Taylor, ED 816 USA 2006 355 Retrospective medical chart review recordsusing BMI, IWQOL-A and DXA scans
OR: 4.45; 95% CI: 1.613.2;P 0.0053
BMI for age exceeding 95th percentile (asdetermined by the National Health andNutrition Examination Survey)
Bell, LM 613 Australia 2007 177 Cohort study using BMI, structuredinterview, medical assessment,anthropometric and fasting bloodinvestigations, including oral glucosetolerance test
For musculoskeletal pain:OR (with every increase of 1.0 inBMI z-score): 2.5495% CI of OR: 1.41 4.59Wald P-value (for BMI z-score):0.003
Children were classified as overweight orobese using the Cole et al.16 age- andgender-specific overweight and obesecutoffs of BMI for children
Hainsworth, KR 818 USA 2009 319 Retrospective review of medical recordsusing BMI, anthropometrics, clinical anddiagnostic data, self report of pain andHRQOL scores
Differences in musculoskeletal/orthopaedic pain characteristicsbetween the three weight groupswas substantial but not significantwith P 0.054
BMI was measured using the US Centrefor Disease Control and Prevention 2000growth charts for sex and age
Krul, M 217 Netherlands 2009 2,459 Retrospective review of Dutch NationalSurvey of Family Practice using Surveydatabase and face-to-face interview
OR: 1.92; 95% CI: 1.15 3.20;Pp0.05
A standard developed for age-specificoverweight and obesity BMI cutoff pointsin Dutch children was used to determinethe presence of overweight and obesityin the study population
Wilson, AC 818 USA 2011 118 Retrospective review of medical chartusing Clinic questionnaire, BMI and CALI-21for activity limitation
A significantly higher rate ofoverweight and obesity wasobserved among youth withchronic pain compared with anormative sample.
CDCs online paediatric BMI calculator,which was used to obtain BMI, BMIpercentile and BMI
Adams 211 (and 1219) USA 2012 913178 Cross-sectional study examinedassociations between weight class anddiagnosis of fractures, sprains, dislocationsand pain
Significant increase in pain of thelower extremities in extremelyobese children between 2 and 5years of age (OR 1.60, 95% CI1.16 2.20) compared with theirnormal weight counterparts andfor children 6 11 years extremelyobese (OR 1.31, 95% CI1.16 1.48), moderately obese(OR 1.24, 95% CI 1.13 1.35) andoverweight (OR 1.17, 95% CI1.07 1.28) compared with theirnormal weight counterparts
Definitions for overweight and obesitybased on sex-specific BMI-for-age growthcharts developed by CDC and WHO
Abbreviations: BMI, body mass index; CDC, Center for Disease Control; DXA, dual X-ray absorptiometry; HRQOL, health-related quality of life; IWQOL-A, impactof weight on quality-of-life adolescent questionnaire; PODCI, Paediatric Outcomes Data Collection Instrument.
Musculoskeletal pain in childrenSM Smith et al
14
International Journal of Obesity (2014) 11 15 & 2014 Macmillan Publishers Limited
-
CONCLUSIONThis review sought to identify the extent of musculoskeletal painin overweight and obese children as reported in literature. Theemerging evidence suggests that being overweight or obese has asignicant impact on the health and well-being of these youngpeople and may contribute to ongoing health problems such asmusculoskeletal pain and bone/joint dysfunction in later life. Thecumulative effect of children being overweight or obese andexperiencing musculoskeletal pain requires further investigation.
CONFLICT OF INTERESTThe authors declare no conict of interest.
ACKNOWLEDGEMENTSWe thank Geoff Lattimore, University of Western Sydneys medical research Librarian,for his assistance with the database searches and strategy.
REFERENCES1 World Health Organization. Obesity and Overweight Fact Sheet No. 311 2011;
http://www.who.int/mediacentre/factsheets/fs311/en/.2 Australian Bureau of Statistics. National Health Survey: Summary of Results,
2007-2008. Report No. 4364.0, Canberra, 2009b.3 Australian Institute of Health and Welfare. Headline indicators for childrens
health, development and wellbeing, 1-151, Canberra, 2011.4 Department of Health and Ageing. Measure Up. 2010; http://www.health.gov.au/
internet/abhi/publishing.nsf/Content/Weight,waist circumference andBMI-lp#overweight.
5 Kiess W, Galler A, Reich A, Muller G, Kapellen T, Deutscher J et al. Clinical aspectsof obesity in childhood and adolescence. Obes Rev 2001; 2: 2936.
6 Cruz ML, Shaibi GQ, Weigensberg MJ, Spruijt-Metz D, Ball GD, Goran MI. Pediatricobesity and insulin resistance: chronic disease risk and implications for treatmentand prevention beyond body weight modication. Rev Nutr 2005; 25: 435468.
7 Puder JJ, Munsch S. Psychological correlates of child obesity. Int J Obes 2010; 34:s37s43.
8 Hebebrand J, Herpertz-Dahlmann B. Psychological and psychiatric aspects ofpediatric obesity. Child Adolesc Psychiatry Clin N Am 2008; 18: 4965.
9 Puhl RM, Latner JD. Stigma, obesity and the health of the nations children.Psychol Bull 2007; 133: 557580.
10 Shomaker LB, Tanofsky-Kraff M, Zocca JM, Field SE, Drinkard B, Yanovski JA.Depressive symptoms and cardiorespiratory tness in obese adolescents.J Adolesc Health 2012; 50: 8792.
11 Mazzuca SA, Brandt KD, Lane KA, Chakr R. Malalignment and subchondrial boneturnover in contralateral knees of overweight/obese women with unilateralosteoarthritis: implications for bilateral disease. Arthritis Care Res 2011; 63:15281534.
12 Marcus D. Obesity and the impact of chronic pain. Clin J Pain 2004; 20: 186191.13 Hakala P, Rimpela A, Salminen JJ, Virtanen SM, Rimpela M. Back, neck and
shoulder pain in Finnish adolescents: national cross sectional surveys. Br Med J2002; 325: 743746.
14 El-Metwally A, Salminen JJ, Auvinen A, Kautiainen H, Mikkelsson M. Prognosis ofnon-specic musculoskeletal pain in preadolescents: a prospective 4 yearfollow-up study till adolescence. Pain 2004; 110: 550559.
15 Perquin CW, Hazebroek-Kampschreur AAJM, Huneld JAM, Bohnen AM,van Suijlekom-Smit LWA, Passchier J et al. Pain in children and adolescents:a common experience. Pain 2000; 87: 5158.
16 OSullivan P, Beales D, Jensen L, Murray K, Myers T. Characteristics of chronicnon-specic musculoskeletal pain in children and adolescents attendinga rheumatology outpatients clinic: a cross-sectional study. Pediatr Rheumatol2011; http://www.ped-rheum.com/content/9/1/3.
17 Al Khattat A, Campbell J. Recurrent Limb pain in childhood (growing pains). Foot2000; 10: 117123.
18 Kaspiris A, Zaropoulou C. Growing pains in children: epidemiological analysis in aMediterranean population. Jt Bone Spine 2009; 76: 486490.
19 Tanamas SK, Wluka AE, Berry B, Menz HB, Strauss BJ, Davies-Tuck M et al.The relationship between obesity and foot pain is related to fat mass and fatdistribution but not muscle mass. Arthritis Care Res 2012; 64: 262268.
20 Moher D, Liberati A, Tetzlaff J, Altman DG, Group TP. Preferred Reporting Items forSystematic Reviews and Meta-Analyses. PLoS Med 2009; 6: e1000097.
21 Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006; 3:77101.
22 Baker JF, George M, Baker DG, Toedter G, Von Feldt JM, Leonard MB. Associationsbetween body mass, radiographic joint damage, adipokines and risk factors forbone loss in rheumatoid arthritis. Rheumatology 2011; 50: 21002107.
23 Buchholz AL, Niesen MC, Gausden EB, Sterken DG, Hetzel SJ, Baum SZ et al.Metobolic acitivity of osteoarthritic knees correlates with BMI. Knee 2010; 17:161162.
24 Felson DT, Goggins J, Niu J, Zhang Y, Hunter DJ. The effect of body weight onprogression of knee osteoarthritis is dependent on alignment. Arthritis Rheumatol2004; 50: 39043909.
25 Taylor ED, Theim KR, Mirch MC, Ghorbani S. Orthopedic complications ofoverweight in children and adolescents. Pediatrics 2006; 117: 21672174.
26 Krul M, Van Der Wouden JC, Schellevis FG, Van Suijlekom-Smit LWA, Koes BW.Musculoskeletal problems in overweight and obese children. Ann Fam Med 2009;7: 352356.
27 de Sa Pinto AL, de Barros Holanda PM, Radu AS, Villares SMF, Lima FR.Musculoskeletal ndings in obese children. J Paediatr Child Health 2006; 42:341344.
28 Hainsworth KR, Davies WH, Khan KA, Weisman SJ. Co-occurring chronic pain andobesity in children and adolescents: the impact on health-related quality of life.Clin J Pain 2009; 25: 715721.
29 Stovitz SD, Pardee PE, Vazquez G, Duval S, Schwimmer JB. Musculoskeletal pain inobese children and adolescents. Acta Paediatr 2008; 97: 489493.
30 Podeszwa DA, Stanko KJ, Mooney 3rd JF, Cramer KE, Mendelow MJ. An analysis ofthe functional health of obese children and adolescents utilizing the PODCinstrument. J Pediatr Orthop 2006; 26: 140143.
31 Bell LM, Curran JA, Byrne S, Roby H, Suriano K, Jones TW et al. High incidence ofobesity co-morbidities in young children: a cross-sectional study. J Paediatr ChildHealth 2011; 47: 911917.
32 Bell LM, Byrne S, Thompson A, Ratnam N, Blair E, Bulsara M et al. Increasing bodymass index z-score is continuously associated with complications of overweightin children, even in the healthy weight range. J Clin Endocrinol Metab 2007; 92:517522.
33 MacFarlane GJ, de Silva V, Jones GT. The relationship between body mass indexacross the life course and knee pain in adulthood: results from the 1958 birthcohort study. Rheumatology 2011; 50: 22512256.
34 Wilson AC, Samuelson B, Palermo TM. Obesity in children and adolescents withchronic pain: associations with pain and activity limitations. Clin J Pain 2010; 26:705711.
35 Tsiros MD, Coates AM, Howe PRC, Grimshaw PN, Buckley JD. Obesity: the newchildhood disability? Obes Rev 2011; 12: 2636.
36 Pollack KM, Xie D, Arbogast KB, Durbin DR. Body mass index and injury riskamong US children 9 15 years old in motor vehicle crashes. Inj Prev 2008; 14:366371.
37 Pomerantz WJ, Timm NL, Gittelman MA. Injury patterns in obese versus nonobesechildren presenting to a pediatric emergency department. Pediatrics 2010; 125:681685.
38 Zonfrillo MR, Seiden JA, House EM, Shapiro ED, Dubrow R, Baker MD et al. Theassoication of overweight and ankle injuries in children. Ambul Pediatr 2008; 8:6669.
39 Kessler J, Koebnick C, Smith N, Adams A. Childhood obesity is associated withincreased risk of most lower extremity fractures. Clin Orthop Relat Res 2013; 471:11991207.
40 Wearing SC, Henning EM, Byrne NM, Steele JR, Hills AP. The impact of childhoodobesity on musculoskeletal form. Obes Rev 2006; 7: 209218.
41 Shultz SP, Browning RC, Schutz Y, Maffeis C, Hills AP. Childhoodobesity and walking: guidelines and challenges. Int J Pediatr Obes 2011; 6:332341.
42 Hills AP, Parker AW. Gait characteristics of obese children. Arch Phys Med Rehabil1991; 72: 403407.
43 Downing AM, Steele JR, Baur LA. What are the effects of obesity in childrenon plantar pressure distributions. Int J Obes Relat Metab Disord 2004; 28:15141519.
44 Downing AM, Steele JR, Baur LA. Does obesity inuence foot structure and plantarpressure patterns in prepubescent children? Int J Obes Relat Metab Disord 2001;25: 845852.
45 Nantel J, Brochu M, Prince F. Locomotor strategies in obese and non-obesechildren. Obesity 2006; 14: 17891794.
46 Shultz SP, Sitler MR, Tierney RT, Hillstrom HJ, Song J. Effects of paediatric obesityon joint kinematics and kinetics during 2 walking cadences. Arch Phys Med Rehabil2009; 90: 21492154.
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 3.0 Unported License. To view a copy of
this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
Musculoskeletal pain in childrenSM Smith et al
15
& 2014 Macmillan Publishers Limited International Journal of Obesity (2014) 11 15
-
Copyright of International Journal of Obesity is the property of Nature Publishing Group andits content may not be copied or emailed to multiple sites or posted to a listserv without thecopyright holder's express written permission. However, users may print, download, or emailarticles for individual use.
title_linkIntroductionMaterials and methodsSearch strategy and selection criteriaParticipants and definitionsSearch outcomeData abstraction
ResultsImpact of being overweight or obese on musculoskeletal health, joint alignment and dysfunction
Table 1 Musculoskeletal pain reporting in overweight and obese childrenImpact of pain on activity, exercise and quality of life
DiscussionFigure 1Retrieval of published studies process flow diagram.Table 2 ConclusionA6A7ACKNOWLEDGEMENTSA8