“Doctor, this patient is sick” From the ward to the PICU John Tsukahara MD Pediatric ICU...
57
“Doctor, this patient is sick” From the ward to the PICU John Tsukahara MD Pediatric ICU California Pacific Medical Center
-
Upload
audrey-watts -
Category
Documents
-
view
217 -
download
1
Transcript of “Doctor, this patient is sick” From the ward to the PICU John Tsukahara MD Pediatric ICU...

“Doctor, this patient is sick” From the ward to the PICU
John Tsukahara MDPediatric ICU
California Pacific Medical Center

I have no relevant financial relationships that might create any personal conflicts of
interest.

“Doctor, this patient is sick.” Important concepts
1. Recognize critically ill or deteriorating patients early.
2. Manage critically ill patients aggressively before they are transferred to the Pediatric ICU.

Ward patients are sicker and more complicated than they used to be

Procedures are just as difficult as they used to be

Pediatric ward nurses work hard.

Pediatric residents have less experience with critically ill patients

The line between the pediatric ward and the Pediatric ICU is not precise.

Subtle changes in patients can be difficult to detect and difficult to articulate

The decision to transfer a patient from the ward to the PICU can be difficult.

The pediatric hospitalist is key

From ward to PICU: the typical process• The ward team rounds in the morning, evaluates the patients and
develops plans for the day• During the day, a child has an acute event or deteriorates.• The bedside nurse is concerned• The nurse alerts the resident• The resident evaluates the patient and speaks with the hospitalist• The hospitalist evaluates the patient and decides that the child should
go to the PICU• The hospitalist contacts the PICU and speaks with the fellow or
pediatric intensivist• The PICU staff checks staffing and bed availablity• The PICU accepts the patient• The child is transferred from the ward to the PICU

“Doctor, this patient is sick.” Important concepts
1. Recognize critically ill or deteriorating patients early.
2. Manage critically ill patients aggressively before they are transferred to the Pediatric ICU.

PICU outcome: Does it make a difference where the patient came from?
• OdetolaFO. Do outcomes vary according to the source of admission to the pediatric intensive care unit? PedCritCareMed. 2008Jan;9(1):20
• University of Michigan, Ann Arbor • Tertiary care university children’s hospital. • 16 bed med-surg PICU and 15 bed cardiac
PICU• 6 years, 8,897 patients

PICU outcome: Does it make a difference where the patient came from?
• PRISM III: Pediatric Risk of Mortality score• A prognostic scoring system derived from 17
physiologic variables measured in the first 12 hours of PICU hospitalization– Vital signs– Laboratory results– Neurologic signs– Diagnoses
• Well-validated measure of severity of illness
Odetola, FO, et. al. Do outcomes vary according to the source of admission to the pediatric intensive care unit? PedCritCareMed. 2008Jan;9(1):20

PICU admission source and outcome:
EDED OROR Pediatric Pediatric WardWard
Transport, Transport, non PICUnon PICU
Un-adjusted Un-adjusted PICUPICU
MortalityMortality
Mean Mean PRISM III PRISM III scorescore
Adjusted Adjusted mortality riskmortality risk
Odetola FO. PedCritCareMed. 2008Jan;9(1):20

PICU admission source and outcome:
EDED OROR Pediatric Pediatric WardWard
Transport, Transport, non PICUnon PICU
Un-adjusted Un-adjusted PICUPICU
MortalityMortality2.2%2.2%
Mean Mean PRISM III PRISM III scorescore
Adjusted Adjusted mortality riskmortality risk
Odetola FO. PedCritCareMed. 2008Jan;9(1):20

PICU admission source and outcome:
EDED OROR Pediatric Pediatric WardWard
Transport, Transport, non PICUnon PICU
Un-adjusted Un-adjusted PICUPICU
MortalityMortality3.7%3.7% 2.2%2.2%
Mean Mean PRISM III PRISM III scorescore
Adjusted Adjusted mortality riskmortality risk
Odetola FO. PedCritCareMed. 2008Jan;9(1):20

PICU admission source and outcome:
EDED OROR Pediatric Pediatric WardWard
Transport, Transport, non PICUnon PICU
Un-adjusted Un-adjusted PICUPICU
MortalityMortality3.7%3.7% 2.2%2.2% 6.7%6.7%
Mean Mean PRISM III PRISM III scorescore
Adjusted Adjusted mortality riskmortality risk
Odetola FO. PedCritCareMed. 2008Jan;9(1):20

PICU admission source and outcome:
EDED OROR Pediatric Pediatric WardWard
Transport, Transport, non PICUnon PICU
Un-adjusted Un-adjusted PICUPICU
MortalityMortality3.7%3.7% 2.2%2.2% 9.8%9.8% 6.7%6.7%
Mean Mean PRISM III PRISM III scorescore
Adjusted Adjusted mortality riskmortality risk
Odetola FO. PedCritCareMed. 2008Jan;9(1):20

PICU admission source and outcome:
EDED OROR Pediatric Pediatric WardWard
Transport, Transport, non PICUnon PICU
Un-adjusted Un-adjusted PICUPICU
MortalityMortality3.7%3.7% 2.2%2.2% 9.8%9.8% 6.7%6.7%
Mean Mean PRISM III PRISM III scorescore
4.94.9 4.74.7 7.27.2 7.17.1
Adjusted Adjusted mortality riskmortality risk
Odetola FO. PedCritCareMed. 2008Jan;9(1):20

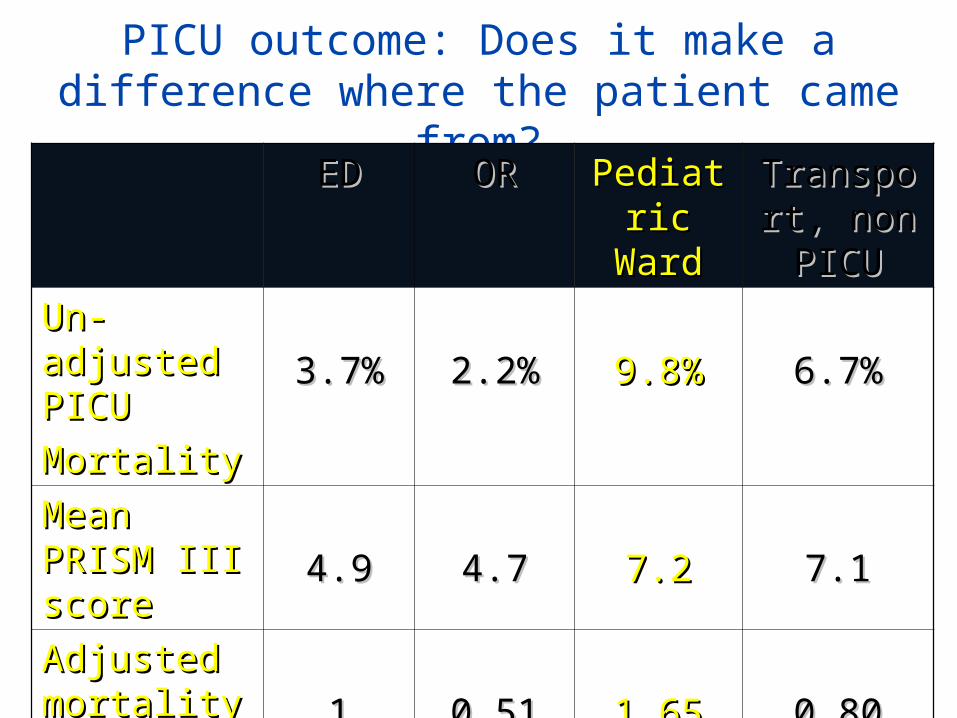
PICU admission source and outcome:
EDED OROR Pediatric Pediatric WardWard
Transport, Transport, non PICUnon PICU
Un-adjusted Un-adjusted PICUPICU
MortalityMortality3.7%3.7% 2.2%2.2% 9.8%9.8% 6.7%6.7%
Mean Mean PRISM III PRISM III scorescore
4.94.9 4.74.7 7.27.2 7.17.1
Adjusted Adjusted mortality riskmortality risk 11 0.510.51 1.651.65 0.800.80
Odetola FO. PedCritCareMed. 2008Jan;9(1):20

• Why are pediatric patients transferred to the PICU from the ward sicker than ED or OR admissions?
• Why is their mortality higher, even corrected for how sick they are?
• Is the same phenomenon seen in adults?

The adult experience• Escarce JJ, Admission source to the medical intensive care unit
predicts hospital death independent of APACHE II score. JAMA 1990;264(18):2389.
• APACHE: Acute Physiology and Chronic Health Evaluation Score
• “…an independent association between the MICU admission source and the risk of death.”
• Actual mortality rate was significantly higher than predicted for patients transferred to the MICU from the hospital ward.

The adult experience• Goldhill D, Outcome of intensive care patients in a group
of British intensive care units. CCM 1998;26(8):1337.
• 15 adult ICUs, 12,762 admissions• “Patients admitted from wards had a higher
mortality than patients from the operating room/recovery or the emergency department.”
• “Early identification of patients at risk…”

Pediatric rapid response teams
• Brilli RJ, et al, Implementation of a medical emergency team in a large pediatric teaching hospital prevents respiratory and cardiopulmonary arrests outside the intensive care unit. PCCM. 2007;8(3):236
• 50% of MET (Medical Emergency Team) calls resulted in transfer to the Pediatric ICU.

Pediatric rapid response teams
• Sharek PJ, et al, Effect of a rapid response team on hospital-wide mortality and code rates outside the ICU in a Children’s Hospital. JAMA. 2007 Nov21; 298(19):2267
• 57% of RRT calls resulted in transfer to the PICU, plus an additional 10% of the calls leading to transfer to the intermediate care unit.

Pediatric rapid response teams
• North Carolina Children’s Hospital (Chapel Hill, NC)
• Tina Schade Willis MD: “In cases where family concern was the reason for calling the Rapid Response Team, 70 percent of the pediatric patients were transferred to the ICU.”

What is happening in the PICU after transfer?
• Is the PICU staff managing ward transfer patients differently than patients from the OR or the ED?

What is happening on the ward?
• Are deteriorating patients unrecognized?• Prior to transfer to the PICU, are patients from
the ward managed differently than those from the OR or the ED?

Do sick ward patients go unrecognized?
• Tume L., The deterioration of children in ward areas in a specialist children’s hospital. 2007;12(1):12
• Most patients had significantly abnormal physiologic measures in the 24 hours prior to emergent transfer to the PICU

• In retrospective reviews, cardiopulmonary arrest is seldom sudden and unpredictable.
• Generally preceded by up to several hours of signs and symptoms predicting clinical deterioration.

Pediatric rapid response teams
• Also, “Medical Response Team” or “Medical Emergency Team”
• A multidisciplinary team of ICU-trained personnel
• Rapidly available for evaluation of patients outside the ICU who develop signs or symptoms of clinical deterioration

Pediatric rapid response teams
• Alters normal chain of command• An open system• “No false alarms”• A large fraction of the calls results in transfer
to the Pediatric ICU

Pediatric rapid response teams• Tibballs J. ArchDisChild 2005. 90(11):1148• Brilli RJ. PedCritCareMed 2007. 8(3):236• Sharek PJ. JAMA 2007. 298(19):2267• Hunt EA. ArchPedAdolMed 2008. 162(2):117
• Fewer respiratory arrests• Fewer cardiac arrests• Improved hospital survival

DEW line
DEW line

Pediatric Early Warning Score: PEWS
• A systematic method of identifying early physiologic deterioration.
• Vital signs, objective observations• Earlier recognition and earlier intervention for
deteriorating patients• Improved outcome

Pediatric Early Warning Score: PEWS
• Multiple scoring systems have been developed
• Some require as many as 20 items to score• Popular in Canada and England• Retrospective reviews reveal unrecognized
physiologic deterioration is common prior to acute events.

Pediatric Early Warning Systems• Akre M. Sensitivity of the Pediatric Early Warning Score to
Identify Patient Deterioration. Pediatrics 2010.125(4):e763
• Children’s Hospitals and Clinics of Minnesota• 325 beds• Retrospective review of 170 Rapid Response
Team events and 16 Code Blue Events on the pediatric ward
• Calculation of PEWS scores• “Critical PEWS” 4


Akre M. Sensitivity of the Pediatric Early Warning Score to Identify Patient Deterioration. Pediatrics.2010Apr;125(4):e763

Pediatric Early Warning Systems
• The overwhelming majority of the patients had elevated PEWS scores for hours prior to an emergency call.
• “The results of this study clearly demonstrate a prolonged period of patient change, affording the opportunity for consultation and intervention before a level of decompensation that requires an RRT or code blue event.”
Akre M. Pediatrics.2010Apr;125(4):e763

You’ve missed dinner and are headed to the ED to see another patient. A bedside nurse comes to you and says, “Doctor, this patient is sick.”

A nurse comes to you and says, “The baby’s blood glucose is low.”

Pediatric Early Warning Systems• “The definitive way to get doctors’ attention
and convince them to review patients is by presenting quantifiable evidence of deterioration.”
• “Quantifiable changes enable them to make judgments about how ill patients are and to prioritize care in terms of assessment and treatment.”
(Andrews T. Packaging: a grounded theory of how to report physiological deterioration effectively. JAdvNurs.2005;52(5):473)

Pediatric Early Warning Systems: the UK
• “Why Children Die—a pilot study”– Confidential Enquiry into Maternal and Child
Health (2008)
• “For paediatric care in hospital we recommend a standardised and rational monitoring system with imbedded early warning systems for children developing critical illness—an early warning score.”

“Doctor, this patient is sick.” Important concepts
1. Recognize critically ill or deteriorating patients early.
2. Manage critically ill patients aggressively before they are transferred to the Pediatric ICU.
PICU outcome: Does it make a difference where the patient came from?
EDED OROR Pediatric Pediatric WardWard
Transport, Transport, non PICUnon PICU
Un-adjusted Un-adjusted PICUPICU
MortalityMortality3.7%3.7% 2.2%2.2% 9.8%9.8% 6.7%6.7%
Mean Mean PRISM III PRISM III scorescore
4.94.9 4.74.7 7.27.2 7.17.1
Adjusted Adjusted mortality riskmortality risk 11 0.510.51 1.651.65 0.800.80

Why do equally ill patients transferred to the PICU from the ward do worse than patients transferred from the ED or the OR?

Early intervention makes a difference.

Sepsis and
septic shock

Pediatric asthma
Asthma mortality in children has dropped in the last few years. (CDC 2006)
However, “…a high percentage of deaths have resulted from under-recognition of asthma
severity and undertreatment…”

“Doctor, this patient is sick.” Important concepts
1. Recognize critically ill or deteriorating patients early.
2. Manage critically ill patients aggressively before they are transferred to the Pediatric ICU.

Careful transfer to the PICU
• Detailed communication• Written summary• Critical lines and tubes secured• Sick patients should be accompanied by a
physician, even if it is just down the hall

“Doctor, this patient is sick.” Concepts/Recommendations for Hospitalists
1. Recognize critically ill or deteriorating patients early. • Pediatric Rapid Response Team• Pediatric Early Warning System• Staff education
2. Manage critically ill patients aggressively before they are transferred to the Pediatric ICU.
• Begin aggressive treatment before transfer• Transfer expediently and safely
What about patients transported to the PICU from outlying hospitals?
• Gregory CJ. Comparison of Critically Ill and Injured Children Transferred From Referring Hospitals Versus In-House Admissions. Pediatrics. 2008;121:e906
• They tend to be sicker than patients transferred into the PICU from in-house sources.
• They have higher PRISM scores, greater utilization of PICU resources, and longer lengths of stay.