Dobutamine stress echo in myocardial viability assessment
39
Role of Dobutamine Stress Echo (DSE) in myocardial viability assessment
-
Upload
please-hit-like-if-you-really-liked-my-ppts -
Category
Health & Medicine
-
view
572 -
download
4
Transcript of Dobutamine stress echo in myocardial viability assessment

Role of Dobutamine Stress Echo (DSE) in myocardial viability
assessment

Understanding Basic Concepts

Ischemia CascadeThe answer to the Question “Why Echo”

Wall Motion
More Specific
Requires Ischemia
Perfusion Changes
More Sensitive
May occur without producing Ischemia

Low cost
Environment friendly
No ionizing radiation
Equally accurate
Why Echo in comparison to SPECT, PET etc.

Coronary Flow Reserve
Angina with ST-T changes
WITHOUT Wall Motion
Abnormalities
Microvascular Ischemia
• Syndrome X• LV Hypertrophy

Stressors in Stress Testing


Exercise Stress Testing
Treadmill
Most potent
Bicycle
Imaging at Peak Stress and during
each stage of stress
Avoids problem of early resolution of
ischemia
Can accurately measure the time of
onset of ischemia
Prognostically important

Situations where Pharmacological Stress is preferred to Exercise Stress


Dipyridamol
Less myocardial dysfunction
More blood flow heterogeneity• Sometimes even
without wall motion abnormalities
• Still supply is sufficient for the demand
More myocardial dysfunction
Less blood flow
heterogeneity
Dobutamine

Adverse Effects and Complications


Protocols



Interpretation of Pharmacological and Exercise Stress Echo

Stress induced myocardial ischemia – Hallmarks
• Worsening of wall motion abnormalities• Development of new wall motion abnormalities
Specific
• Lack of hyperdynamic motion• Beta Blockers• THR not attained
Non-Specific
• Akinetic segment becoming dyskinetic
No meaning

Adjunctive Diagnostic Criteria
LV cavity dilatation
Decreased Global LV systolic function
TVD or Left Main disease
Differential responses to Exercise and Dobutamine Stress Echo

Diagnostic End Points
• Max dose of pharmacological agent
• Achievement of THR
• Akinesis of ≥ 2 LV segements
• Severe Chest pain• Obvious ECG
positivity• ≥ 2mm ST shift
Submaximal Non-diagnostic End Points
• Non tolerable symptoms
• Limiting Asymptomatic side effects• Hypertention (BP
> 220/120)• Hypotension (BP
drop > 40mm Hg)• Supraventricular
Arrythmias• Complex
Ventricular Arrythmias
• VT• Frequent
polymorphic VPC

Dipyridamol Stress Preferred• Hypertension• Atrial and Ventricular Arrhythmias
Dobutamine Stress Preferred• Conduction disturbances • Bronchospastic diseases• On Xanthine medications• Caffeine containing drinks
• Tea• Coffee• Cola

Contents of Stress Echo Report

Statistics, StudiesThe Comparison

Exercise Stress Echo
Dobutamine Stress Echo
VT 1.4% 4%
VF 1 2
SVT and AF are more common than VT/VF
Single Centre Analysis ( >50,000 studies ) – Mayo Clinic

Ischemic Threshold Event Rate< 60% THR 43%≥ 60% THR 9%No Ischemia 0%
Dobutamine Stress Echo in Preop Evaluation and Prognostication
A Mayo clinic study of 530 patients

Accuracy of different approaches for diagnosis of CAD with Stress Echo
Hoffmann R, Lethen H, Marwick T, et al. Standardized guidelines for the interpretation of dobutamine echocardiography reduce interinstitutional variance in interpretation. Am J Cardiol. 1998;82:1520–1524.

Safety Data

Safety of Pharmacological Stress Echo

Physical stress with exercise is probably safer than
pharmacological testing
Lattanzi F, Picano E, Adamo E, Varga A. Dobutamine stress echocardiography: safety in diagnosing coronary artery disease. Drug Saf 2000; 22:251–62.Varga A, Garcia MA, Picano E. International Stress Echo Complication Registry. Safety of stress echocardiography (from the International Stress Echo Complication Registry). Am J Cardiol 2006;98:541–3
Safety of Pharmacological Stress Echo

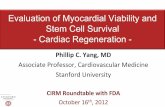
Special SubsetsMyocardial Viability Assessment

Viable
Thickness ≥ 6mm
Scarred
Thinned Echodense

Hibernating Myocardium
• Viable but underperfused myocardial tissue that regains functionality after revascularization
• Rescue of hibernating myocardium via revascularization manifests as improved left ventricular function
• DSE has emerged as a noninvasive tool for detecting hibernating myocardium and thus identifying patients most like to benefit from revascularization
Gilstrap et al . Dobutamine stress echocardiography: a review and update. Research Reports in Clinical Cardiology 2014:5 69–81

Biphasic wall motion response• At low doses: hibernating myocardium will augment due to
inotropic stimulation
• At higher doses: hibernating segment may exhibit abnormal wall motion
• This biphasic response appears to be most predictive of post-revascularization viability
• ASE guidelines recommend that viability assessment includes improvement in at least 2 echocardiographic left ventricular segments
Gilstrap et al . Dobutamine stress echocardiography: a review and update. Research Reports in Clinical Cardiology 2014:5 69–81

van der Sijde JN et al. Diabetes Care. 2012 Mar;35(3):634-9
Abnormal DSE

DSE after MI
• Has a sensitivity of 82% and a specificity of 80% for detecting a residual stenosis subtending an area of hibernating myocardium
• Myocardial viability early after MI: – Single best predictor of recurrent in-hospital
ischemia and unstable angina after discharge – Associated with better left ventricular function
recovery and lower long-term mortality
Gilstrap et al . Dobutamine stress echocardiography: a review and update. Research Reports in Clinical Cardiology 2014:5 69–81

DSE in CAD and ischemic cardiomyopathy
• Helps to identify patients most likely to have improved survival
• In ischemic cardiomyopathy: Identifies patients with highest chances of survival post-procedure
• In CAD: Useful in predicting ultimate post-revascularization left ventricular recovery
Gilstrap et al . Dobutamine stress echocardiography: a review and update. Research Reports in Clinical Cardiology 2014:5 69–81

Diagnostic Accuracy comparison for Myocardial Viability AssessmentMetanalysisBax et al. 2001
Bax JJ, Poldermans D, Elhendy A, et al. Sensitivity, specificity, and predictive accuracies of various noninvasive techniques for detecting hibernating myocardium. Curr Probl Cardiol. 2001;26:142–186

THANK YOU