Heparin-Induced Thrombocytopenia · Heparin-induced thrombocytopenia • Thrombocytopenia •


• DOACS
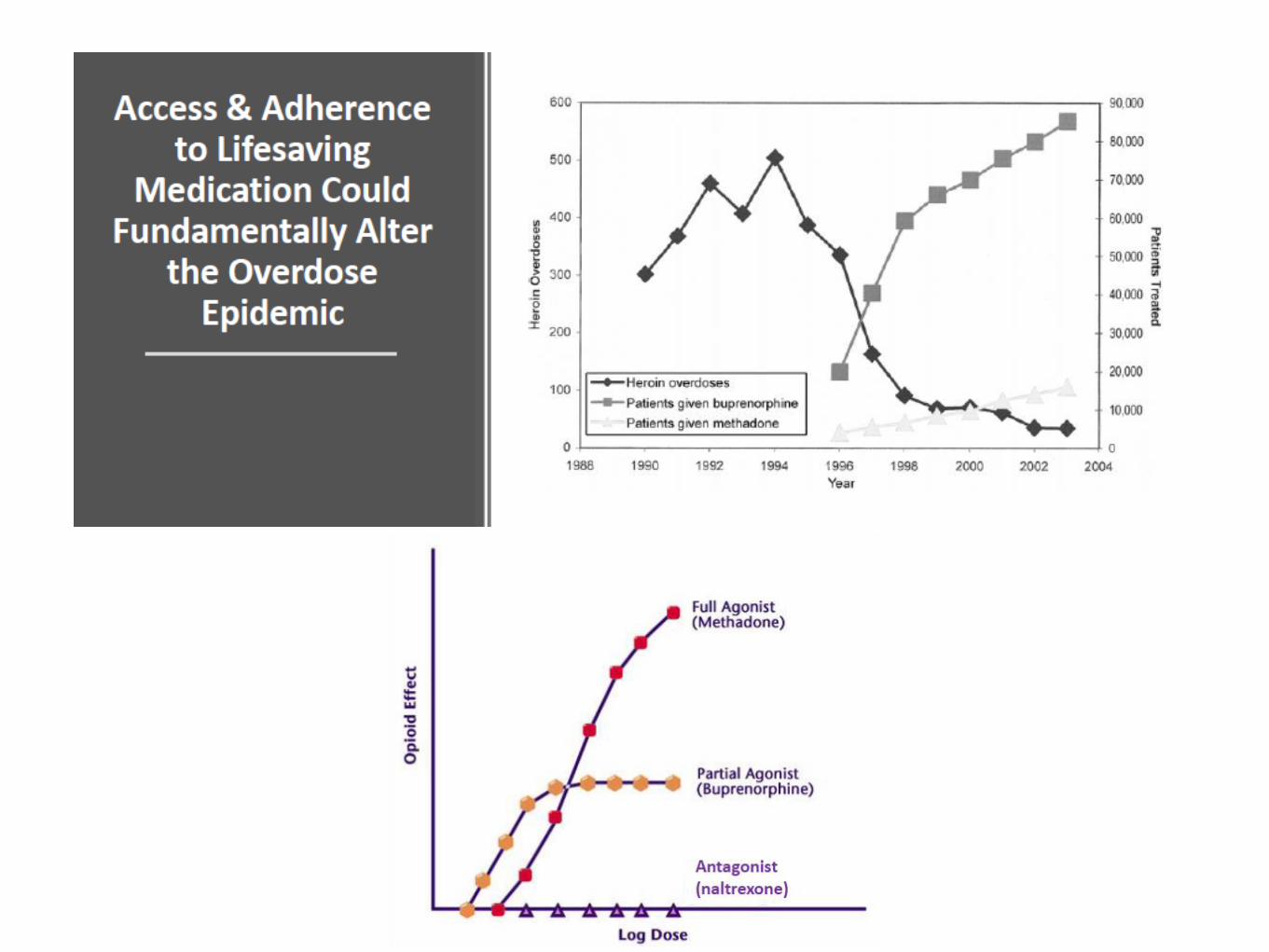
• opiate addiction
• Thrombocytopenia
• COPD, O2 suppl.
• viral prodromes
• ACS
• C difficile
• pulmonary embolism
• sepsis
• pneumonia

A 78yr old woman presents with
dizziness. ECG shows AF however it
reverts to SR in ED.
Background hypertension, diabetes and
renal impairment, with eGFR 20 ml/min.
She is stable for d/c.
What is the optimal approach approach
regarding the AF ?

• Nothing, she is in SR and stable
• enoxaparin 1 mg/kg bd until INR therapeutic on warfarin
• apixaban 5mg bd x7 days then 2.5mg bd
• dabigatran 110mg bd
• rivaroxaban 15mg bd x3wk then 20mg daily
• Nothing, she is in SR and stable
• enoxaparin 1 mg/kg bd until INR therapeutic on warfarin
• apixaban 5mg bd x7 days then 2.5mg bd
• dabigatran 110mg bd
• rivaroxaban 15mg bd x3wk then 20mg daily







She has done well, with paroxysmal AF
that is controlled.
2 years later she is diagnosed with PE
and found to have breast cancer
eGFR is now 40 ml/min
What is the optimal anticoagulation now?

• enoxaparin until INR therapeutic on warfarin
• enoxaparin
• apixaban 10mg bd x7 days then 5mg bd
• dabigatran 110mg bd
• rivaroxaban 15mg bd x3wk then 20mg daily

• enoxaparin until INR therapeutic on warfarin
• enoxaparin
• apixaban 10mg bd x7 days then 5mg bd
• dabigatran 110mg bd
• rivaroxaban 15mg bd x3wk then 20mg daily




A 36yr man is brought in by police because of concern for his
agitated behaviour. He has abdominal cramping and is
agitated.
It is clear he is in opiate withdrawal.
What is the best approach?

• Let him suffer, he deserves it and it will teach him a lesson
• Load him with endone and give a script for discharge as
well as a fentanyl patch if he runs out of tablets
• symptomatic management including benzodiazepines,
antiemetic, clonidine; then admit for supervised detox.
• symptomatic management as above, then commence
buprenorphine

• Let him suffer, he deserves it and it will teach him a lesson
• Load him with endone and give a script for discharge as
well as a fentanyl patch if he runs out of tablets
• symptomatic management including benzodiazepines,
antiemetic, clonidine; then admit for supervised detox.
• symptomatic management as above, then commence
buprenorphine




A 35 yr woman with no medical history of note presents with
a petechial rash following a mild viral RTI.
She is otherwise stable, exam is normal
Platelet count 2; no other abnormality
You diagnose ITP
What is the initial treatment?

• prednisone 50mg daily with haematology follow up
• dexamethasone 40mg daily x4 days
• plasmapheresis
• platelet transfusion

• prednisone 50mg daily with haematology follow up
• dexamethasone 40mg daily x4 days
• plasmapheresis
• platelet transfusion



ie mucosal involvement
Increased risk ICH


Her friend also mentions that she has a similar rash, and feels
unwell. She also has no medical history of note
You say “can’t you see we’re busy”
Triage wonders why she can’t see her GP for a rash, and sends
her to the waiting room
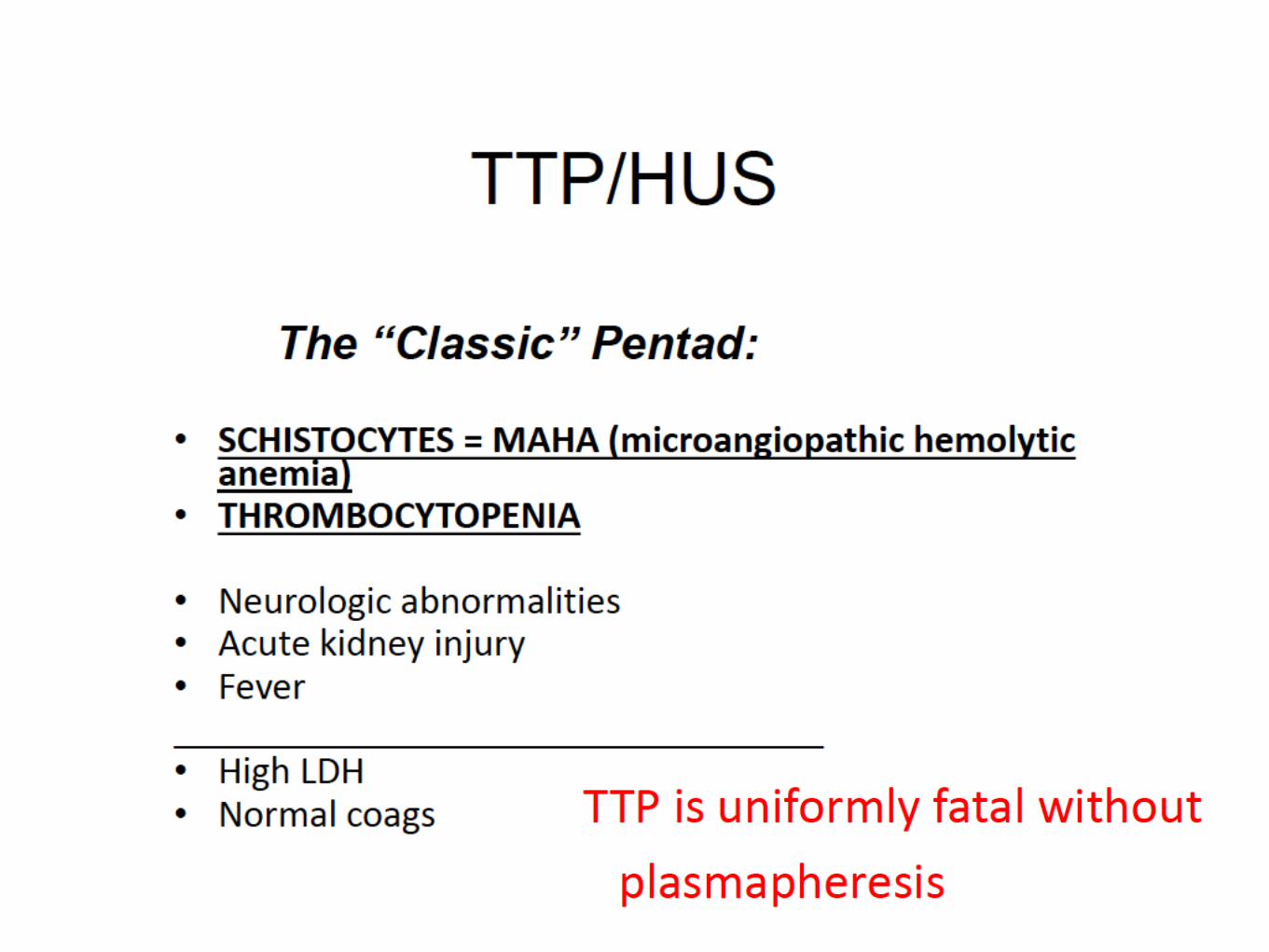
Further history reveals she has been intermittently confused
Temp 38.4, vital signs stable, exam shows petechial rash
The lab phones her results:

• Hb 86
• platelets 35
• bilirubin 46
• LDH 640
• creatinine 325
• INR/APTT normal
Next step
• dexamethasone 40mg/day x4 days
• urgent referral for plasmapheresis; insert vas cath
• admit medicine and refer haematology for bone marrow
biopsy
• treat for sepsis

Next step
• dexamethasone 40mg/day x4 days
• urgent referral for plasmapheresis; insert vas cath
• admit medicine and refer haematology for bone marrow
biopsy
• treat for sepsis








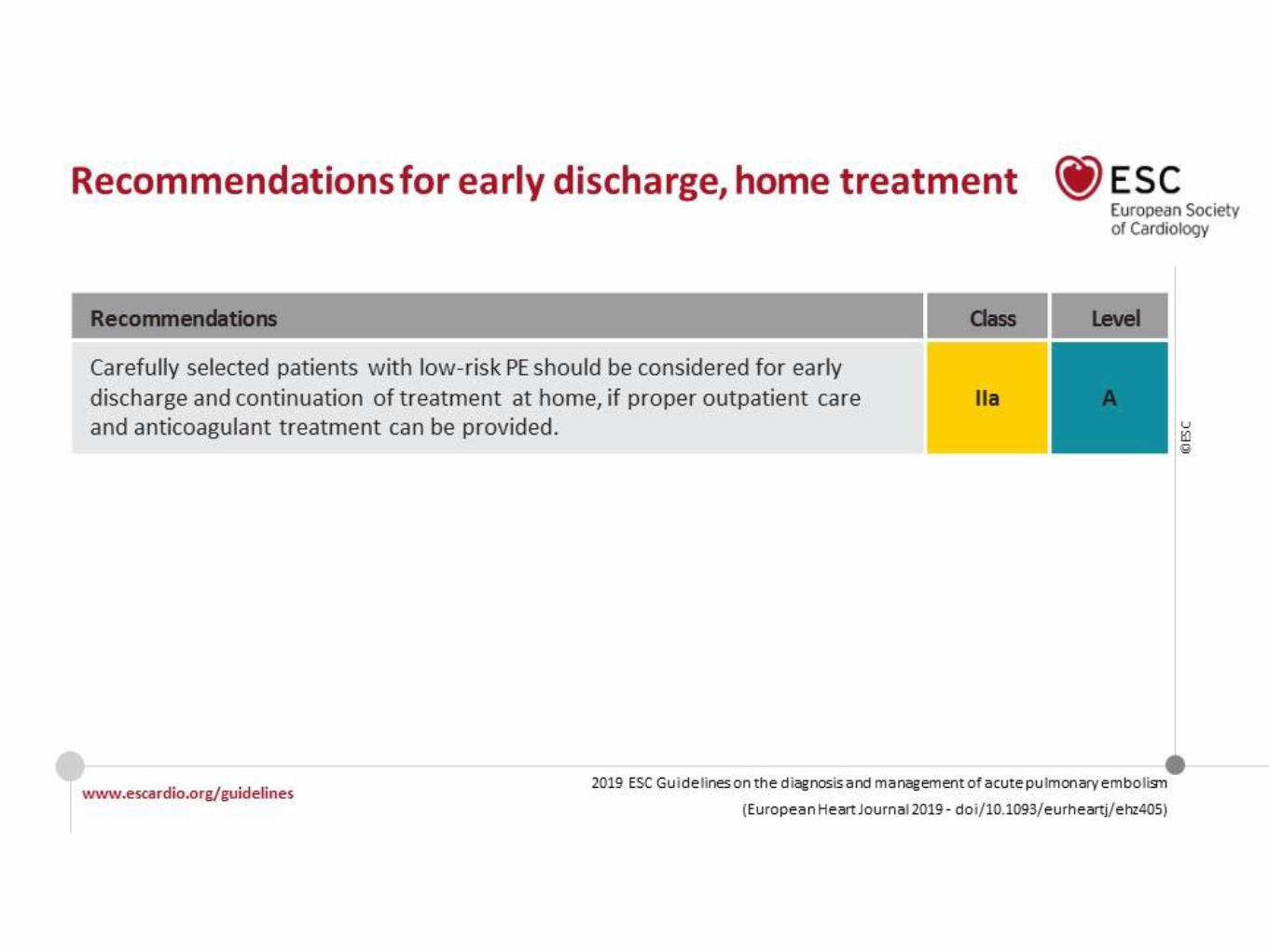
?? exertion symptoms with acceptable O2 sats



Anything more ?




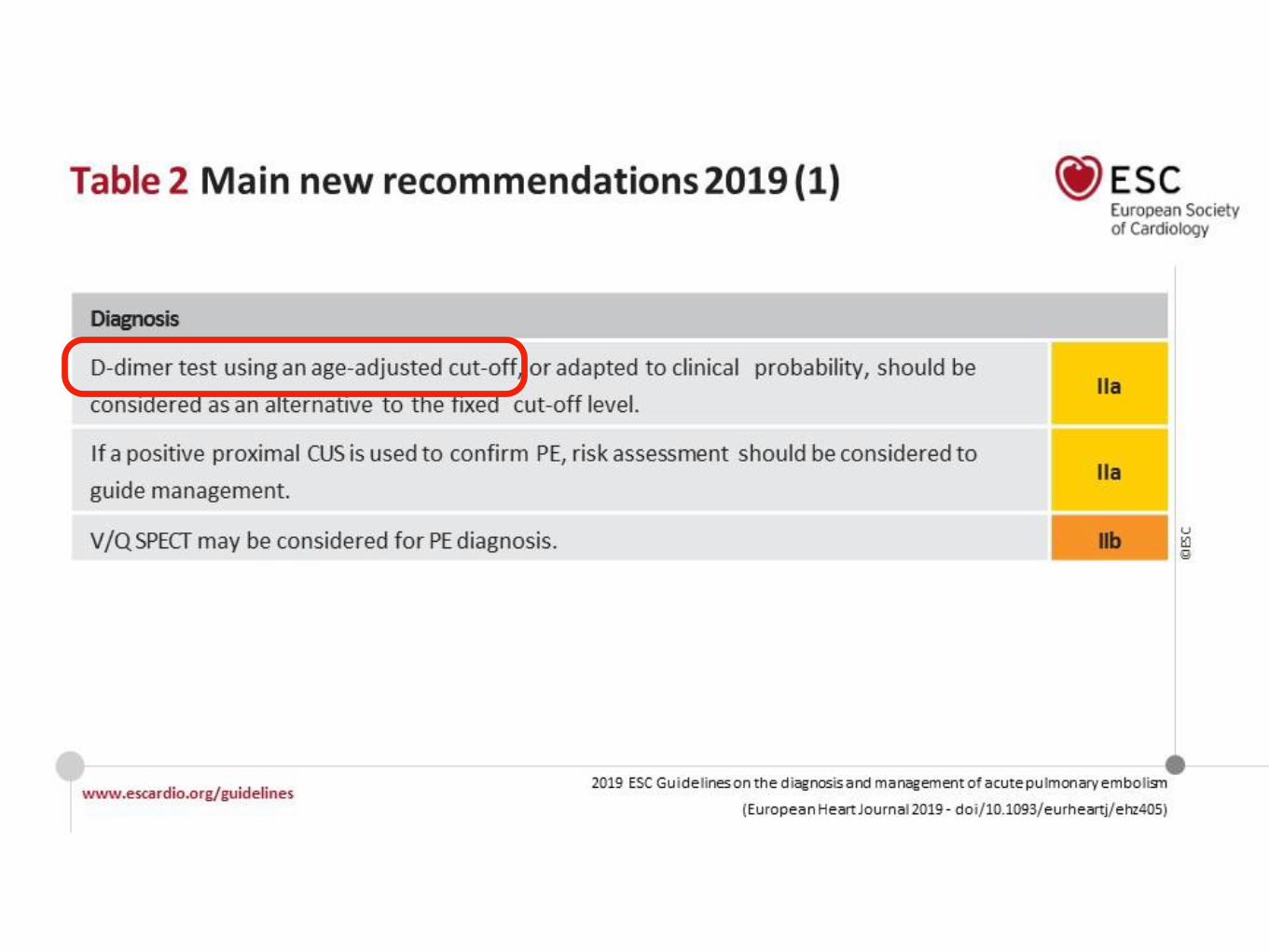
Most false +ve if
testing low risk groups


What is best way to monitor
response of HIV to ART?
• viral load
• CD4 count
• both

What is best way to monitor
response of HIV to ART?
• viral load
• CD4 count
• both

What is best way to monitor
response of HIV to ART?
• viral load
• CD4 count
• effective treatment prevents low CD4
• can drop transiently <200 in acute illness
• both









A 64yr- man develops C difficile diarrhoea after antibiotics
given for pneumonia. He is clinically stable with eGFR 55
What is the preferred treatment?
• oral metronidazole 500mg tds
• IV metronidazole 500mg tds
• oral vancomycin 125mg QID
• IV vancomycin 1g bd

A 64yr- man develops C difficile diarrhoea after antibiotics
given for pneumonia. He is clinically stable with eGFR 55
What is the preferred treatment?
• oral metronidazole 500mg tds
• IV metronidazole 500mg tds
• oral vancomycin 125mg QID
• IV vancomycin 1g bd







Low risk
Well’s score 0-4.0
Moderate risk
Well’s score 4.5-6.0


Safely reduced imaging from 52 to 34 %












Case: 68yr-F presents with cough, productive sputum and
fever. HR is 95 bpm, BP 115/80, RR 22, O2 sats on air 93%,
lactate 2.4. There is patchy inflammatory changes on CXR,
and she is admitted for IV benzylpenicillin and oral
doxycycline.
The respiratory physician contacts the ED Director to
express concern that antibiotics were not given until 5 hours
after arrival.
• How would you respond?




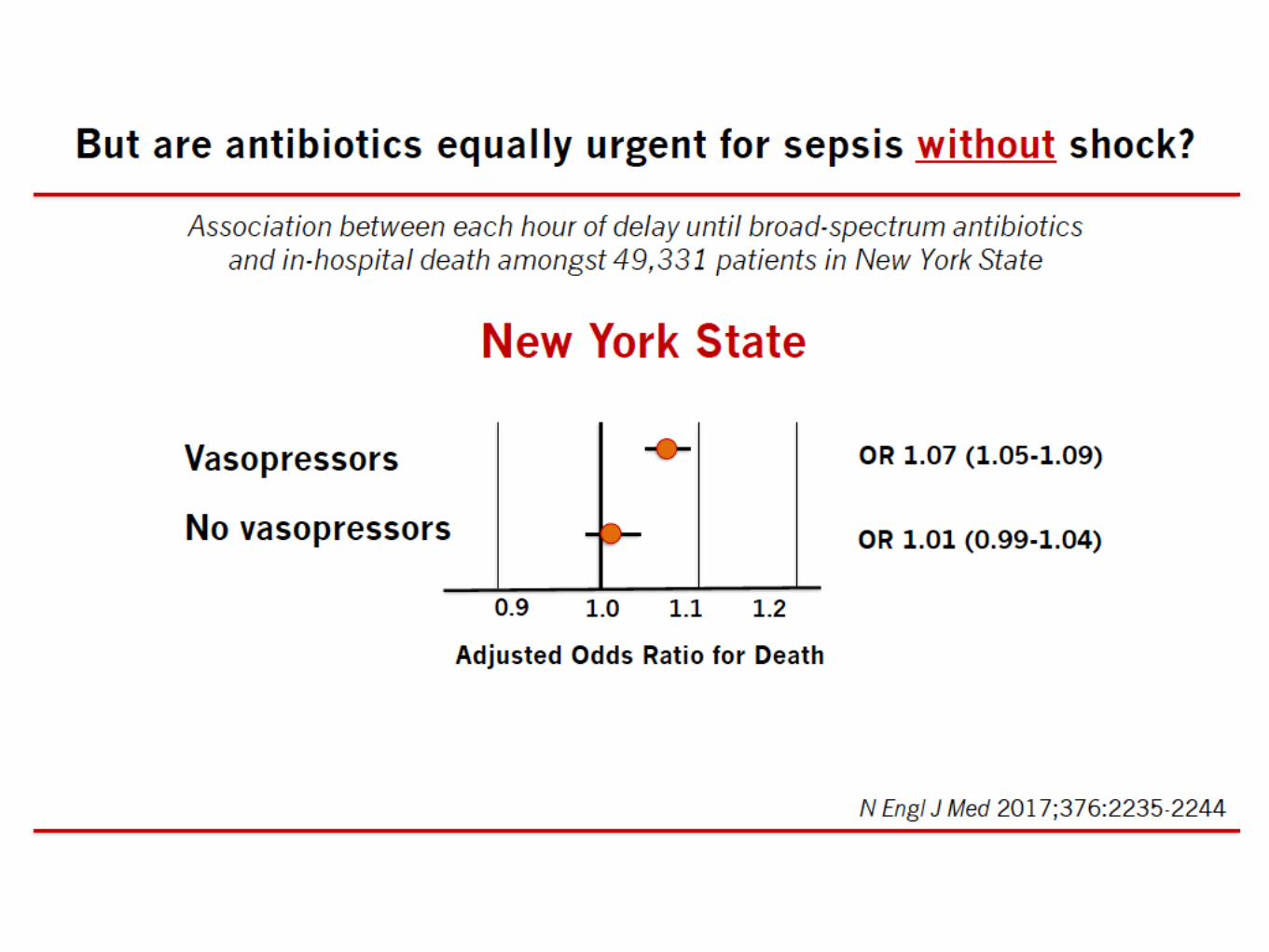



Time to clinical stability