
DO NOT FILE WITH PACER - Home - False Claim Act … NOT FILE WITH PACER i TABLE OF ALLEGATIONS I....
89
IN THE UNITED STATES DISTRICT COURT FOR THE EASTERN DISTRICT OF PENNSYLVANIA [UNDER SEAL] : CIVIL ACTION NO. : Plaintiff : : v. : FILED UNDER SEAL : : : [UNDER SEAL] : : Defendants. : FIRST AMENDED QUI TAM COMPLAINT FILED UNDER SEAL DO NOT FILE WITH PACER
Transcript of DO NOT FILE WITH PACER - Home - False Claim Act … NOT FILE WITH PACER i TABLE OF ALLEGATIONS I....

IN THE UNITED STATES DISTRICT COURT
FOR THE EASTERN DISTRICT OF PENNSYLVANIA
[UNDER SEAL] : CIVIL ACTION NO.
:
Plaintiff :
:
v. : FILED UNDER SEAL
:
:
:
[UNDER SEAL] :
:
Defendants. :
FIRST AMENDED QUI TAM COMPLAINT
FILED UNDER SEAL
DO NOT FILE
WITH PACER

i
TABLE OF ALLEGATIONS
I. INTRODUCTION ................................................................................................................... 1
II. THE PARTIES ........................................................................................................................ 4
A. Relator/Plaintiff................................................................................................................... 4
B. Defendants .......................................................................................................................... 6
1. Defendant CVS Caremark Corporation .......................................................................... 6
2. CVS Caremark Entities Participating in Medicare Part D Program ............................... 8
3. Defendant CVS Caremark’s PBM Subsidiary, Caremark Rx ........................................ 9
a. Caremark Rx Provides Its Part D PBM Services Through A Subsidiary
SilverScript, LLC .............................................................................................................. 11
b. Other CVS Caremark Entities Providing Part D PBM Services............................. 12
4. Defendant CVS Caremark’s Medicare Part D Plan (PDP) Sponsor, SilverScript
Insurance Company ............................................................................................................... 12
5. CVS Caremark Revenues Related to Medicare Part D Services .................................. 13
C. The "Medical Card System" Entities ................................................................................ 14
1. Medical Card System, Inc. ............................................................................................ 14
2. MCS Life Insurance Company ..................................................................................... 15
III. JURISDICTION AND VENUE ............................................................................................ 16
IV. APPLICABLE LAW ............................................................................................................. 17
A. The Medicare Part D Program: Prescription Drug Coverage .......................................... 17
B. Entities Operating in the Medicare Part D System ........................................................... 18
1. Part D Sponsor .............................................................................................................. 18
2. First Tier, Downstream, and Related Entities ............................................................... 23
C. Summary of the Part D Process - Adjudicating Prescriptions ......................................... 24
D. CMS Part D Payments Based on PDE Claims Data Submitted to CMS .......................... 26
E. Medicare Part D Payments to Part D Sponsors Are Expressly Conditioned Upon
Submission of Accurate, Complete and True PDE Data .......................................................... 28
1. Required Data Elements for PDE Records ................................................................... 28
2. Part D Claims – Certification of Truth and Accuracy .................................................. 30

ii
a. PDE Data on Gender, Prescriber, NDC .................................................................. 32
(i) Sponsors or PBMs Must Report the Patient’s Gender to CMS .......................... 33
(ii) Sponsors or PBMs Must Report the Prescriber ID Number to CMS .................. 34
(iii) Sponsors or Their PBMs Must Submit NDC Codes to CMS ............................. 35
b. Part D Sponsors or Their PBMs Must Submit Drug Cost Data to CMS ............... 35
F. Part D Requirements for Dispensing "Covered Drugs" .................................................... 36
1. Part D Drugs – National Drug Codes (NDC) ............................................................... 37
2. Part D Requires Compliance with All State Pharmacy Laws ....................................... 38
G. Part D Requirements of Sponsors Are Impacted When Services Performed by the PBM
Are Not in Compliance with Part D Requirements ................................................................... 42
1. Part D Sponsors and Their PBMs Are Required to Comply with All Applicable State
Laws....................................................................................................................................... 42
2. Part D Sponsors and Their PBMs Must Deny Claims for Any Expired Drugs ............ 43
3. Part D Sponsors or PBMs Must Deny Claims for Drugs Prescribed by Excluded
Providers ................................................................................................................................ 45
4. Part D Sponsors Must Conduct Concurrent DURs, Including Gender Contraindications
....................................................................................................................................... 45
5. Part D Sponsors Must Have a Comprehensive Fraud, Waste and Abuse Plan............. 47
H. CMS Identifies Areas Susceptible to Fraud by Part D Stakeholders ................................ 48
1. Part D Sponsor and PBM Fraud, Waste and Abuse...................................................... 48
2. Fraud, Waste and Abuse by Downstream Entities........................................................ 49
I. Requirements of Part D First Tier, Downstream, and Related Entities: All Part D
Downstream Entities Must Comply with all Applicable Federal and State Laws and
Regulations, and CMS Instructions ........................................................................................... 49
VII. FRAUD ALLEGATIONS: .................................................................................................... 50
A. Background: Contracts for Medicare Part D PBM Services Between Caremark and MCS
Life ........................................................................................................................................... 50
B. The Part D Audit by Pharm/DUR Inc. Reveals that the Caremark Defendants Unlawfully
and Intentionally Failed to Comply with the Fundamental Requirements of the Medicare Part
D Program ................................................................................................................................. 55
1. The Audit ...................................................................................................................... 55

iii
2. Pharm/DUR’s Audit Findings....................................................................................... 58
C. Defendants Have Illegally Submitted False Medicare Part D PDE Claims Data to CMS
Resulting in False Part D Payments to MCS and/or MCS Life ................................................ 59
1. False Prescriber Identifiers (DEA Numbers) ................................................................ 60
a. The Caremark Defendants Fraudulently Do Not Edit for Unidentified Prescribers ...
................................................................................................................................. 61
b. Invalid Prescriber Date Undermines Appropriateness of Part D Claim ................ 62
2. Gender-Specific Deviations .......................................................................................... 63
3. Drugs with Expired or Obsolete NDCs ........................................................................ 64
4. No Prior Authorization ................................................................................................. 66
5. Drugs Dispensed Over Approved Limit ....................................................................... 67
6. Improper MAC Pricing ................................................................................................. 69
D. Defendants Failed to Perform Appropriate Concurrent Drug Utilization Reviews .......... 69
E. The CVS Caremark Defendants Thwarted MCS’s Ability to Have in Place a Plan to
Detect, Correct, and Prevent Part D Fraud, Waste and Abuse ................................................. 70
F. Defendants Caused CMS to Make Inflated Part D Subsidy Payments to MCS Life ...... 71
G. Defendants Have Illegally Caused CMS to Make Inflated Medicare Part D Subsidy
Payments to CVS Caremark’s Customers Other than MCS Life.............................................. 73
1. Caremark's System-Wide Part D Claims Processing Failures ...................................... 73
H. CMS Improperly Paid Part D Retiree Drug Subsidies...................................................... 74
1. Improper Part D Retiree Drug Subsidies to Employer Plans Offered by MCS ............ 74
2. CMS Has Improperly Paid Part D Retiree Drug Subsidies to Defendant CVS
Caremark's Other Customers ................................................................................................. 75
COUNT I - Violations of the Federal False Claims Act 31 U.S.C. § 3729(a)(1)(A), (2) and (3)
and (7) ........................................................................................................................................... 76
Demand for Jury Trial ................................................................................................................... 82
EXHIBIT "A" - CVS CAREMARK ORGANIZATIONAL CHART PART D
EXHIBIT "B" - PBM AGREEMENT BETWEEN MCS AND SILVERSCRIPT
EXHIBIT "C" - PART D CLAIMS DATA

IN THE UNITED STATES DISTRICT COURT
FOR THE EASTERN DISTRICT OF PENNSYLVANIA
UNITED STATES OF AMERICA, EX REL.
ANTHONY R. SPAY
Plaintiffs,
v.
CVS CAREMARK CORPORATION,
CAREMARK Rx, LLC (f/k/a CAREMARK
Rx, INC.),
CAREMARK, LLC (f/k/a/ CAREMARK,
INC.)
SILVERSCRIPT, LLC (f/k/a SILVERSCRIPT
INC.),
Defendants.
:
:
: CIVIL ACTION NO. : 09-4672
:
:
:
: FIRST AMENDED
: QUI TAM COMPLAINT
:
: JURY TRIAL DEMANDED
:
: FILED IN CAMERA AND
: UNDER SEAL PURSUANT
: TO 31 U.S.C. § 3730(b)(2)
:
: HON. RONALD L. BUCKWALTER
_______________________________________ :
I. INTRODUCTION
Qui Tam Plaintiff/Relator Anthony R. Spay, through his counsel, Pietragallo Gordon
Alfano Bosick & Raspanti, LLP, on behalf of the United States of America, brings his First
Amended Complaint against Defendant CVS Caremark Corporation, Defendant Caremark Rx,
LLC (f/k/a Caremark Rx, Inc.), Defendant Caremark LLC (f/k/a Caremark, Inc.), Defendant
SilverScript, LLC (f/k/a SilverScript, Inc.), and alleges based upon his own direct and
independent knowledge:
1. This is an action to recover damages and civil penalties on behalf of the
United States of America, arising from false and/or fraudulent records, statements and claims
made, used and caused to be made, used, or presented by Defendants CVS Caremark
Corporation, Caremark Rx, LLC (f/k/a Caremark Rx, Inc., Caremark LLC (f/k/a Caremark, Inc.),
SilverScript, LLC (f/k/a SilverScript, Inc.) (collectively referred to as the "Defendants"), and/or
2
their agents, predecessors, successors, and employees in violation of the Federal Civil False
Claims Act, 31 U.S.C. § 3729 et seq., as amended (“the FCA” or “the Act”).
2. Defendants, in their role as Pharmacy Benefits Manager ("PBM") for Medicare
Part D Sponsors throughout the United States and in the Commonwealth of Puerto Rico have
intentionally, systematically, recklessly and illegally provided false or fraudulent Medicare Part
D claims and prescription drug event (“PDE”) data to the Centers for Medicare and Medicaid
Services (“CMS”) since 2006.
3. As a direct result of Defendants’ fraudulent, improper and illegal practices,
Federal health insurance programs including, but not limited to, Medicare Part D, have been
caused and continue to:
A. pay false or fraudulent claims related to Part D prescription drugs that would
not have been paid but for the Defendants’ intentional, illegal, improper, and
reckless business practices;
B. pay increased subsidies to Medicare Part D Plan Sponsors, including
Medical Card System, Inc. and/or MCS Life Insurance Company, through:
direct advance monthly payments; reinsurance subsidies; low-income cost-
sharing subsidies (or grants for low-income Part D individuals received in lieu
of low-income subsidies); risk-sharing arrangements; year-end retroactive
adjustments and reconciliations; and/or reinsurance payments made for private
fee-for-service plans;
C. based on the Defendants’ false representations of compliance with Federal
laws and regulations related to the Part D program, enter into contracts with
the Defendants as providers of Part D services, whether as a Sponsor, PBM, or

3
other downstream entity, including but not limited to, CMS’s Electronic Data
Interchange (“EDI”) Agreement, and/or other agreements which are necessary
for Part D providers to submit claims or data to CMS and/or to receive
payments related to the Medicare Part D program.
4. Defendants utilize an automated nationwide claims adjudication system in all
States, as well as the Commonwealth of Puerto Rico, where the Defendants provide PBM
services, and, as a result, the Defendants’ illegal and improper practices have also caused the
Federal government to pay false or fraudulent claims in Federal health insurance programs, in
addition to Part D, which provide prescription drug benefits to their beneficiaries, including, but
not limited to CHAMPUS/TRICARE, CHAMPVA, and the Federal Employee Health Benefits
Program.
5. As a direct and foreseeable result of the Defendants’ improper and illegal
practices, Federal and state health insurance programs, including but not limited to, Medicare
and Medicaid, have been impacted by Defendants' adjudication of Part D claims by virtue of the
States' contributions to low income cost subsidies.
6. Plaintiff seeks through this action to recover on behalf of the United States
damages and civil penalties arising from Defendants’ making or causing to be made false or
fraudulent records, statements and/or claims in connection with its knowing violations of the
Medicare Part D Program reporting requirements and claims submissions for Part D benefits.
7. Pursuant to 31 U.S.C. § 3730(c)(3), if the Government elects not to intervene in a
qui tam action, the Relator has the right to proceed against the Defendant on behalf of the
Government. The Court may later permit the Government to intervene upon a showing of good
cause. In a non-intervened matter, the Government, and, therefore, the American taxpayer, still

4
receives at least 70% of any recovery obtained through the qui tam Relator’s efforts pursuant to
31 U.S.C. § 3730(d)(2).
II. THE PARTIES
A. Relator/Plaintiff
8. Plaintiff/Relator Anthony R. Spay is a resident of the State of New Jersey and a
citizen of the United States.
9. Relator Spay is a duly licensed pharmacist under the laws of Pennsylvania, with
37 years of diversified experience within the pharmacy industry. He is uniquely qualified to
bring this action on behalf of the United States.
10. Relator’s knowledge of the pharmacy industry emanates from three decades of
experience since becoming a licensed pharmacist encompassing retail practice, benefits
management, long-term care, behavioral health, executive management, prescription drug
fraud/abuse detection, auditing and recovery for many of the nation’s largest payers and
pharmacy claims processors.
11. After receiving his pharmacy degree, Relator Spay spent over seven years as retail
Pharmacy Manager with Eckerd Drugs (1967-74). Drawing on this knowledge and experience,
Mr. Spay later owned and operated his own chain of retail pharmacies for twenty years
(1974 to 1994).
12. Following his successful career as a retail pharmacist, Mr. Spay founded and
served as President of Managed Care Consultants (1994 to the present), where he has continued
his involvement with community mental health issues. Mr. Spay is also a consultant and board
member for a behavioral health organization.
13. In addition to operating two retail pharmacies, Relator served as President of

5
Squire Medical Services (1995-1999), a long term care supplier with seven locations.
14. For over 17 years, Relator dedicated himself to co-founding, developing, and
managing Pharm/DUR Inc., a corporation headquartered in Philadelphia, PA.
15. Mr. Spay co-founded Pharm/DUR Inc. in 1992 to administer many aspects of
pharmaceutical management programs for insurers, employer groups, and commercial and
government-sponsored health plans. Under Relator’s leadership as President and Chief Executive
Officer, Pharm/DUR Inc. became one of the largest providers of pharmacy prescription benefit
audit and recovery services in the United States with auditors across the country.
16. Relator has extensive experience designing and implementing drug auditing
protocols, fraud detection methods, software, and supporting training systems for the
identification and investigation of prescription drug fraud, waste and abuse – both retrospectively
and prospectively.
17. Under Relator’s guidance, Pharm/DUR and its successor companies’ clients have
included some of the largest pharmaceutical benefit management firms, HMOs and private
insurance firms in the United States. Pharm/DUR Inc. has conducted in excess of 100,000 in-
store audits nationwide, in addition to numerous desk audits, program reviews and retrospective
forensic electronic data analyses and audits. Annually, the Company has conducted
approximately 15,000 in-store audits in a minimum of 35 states.
18. Pharm/DUR Inc. and its successor companies have used a proprietary system
application, AUDITRAC Automated Healthcare System (“AUDITRAC”), which utilizes the
paid claims data from Pharm/DUR’s clients to develop targeted pharmacy audits.
19. Relator is a current and former member of many local and national professional
scientific societies. He is a current and former Fellow of the American College of Apothecaries
6
and of the Compounding Pharmacists of America, a Board Member of Crisis Management
Services, Inc., a member of the National Association of Retail Druggists, an Executive Board
Member of the Philadelphia Association of Retail Druggists, and an Education Committee
Member of the Pharmacist Association.
20. On or about July 1, 2009, Affiliated Computer Services (“ACS”) acquired
Pharm/DUR Inc. Following the ACS acquisition, Pharm/DUR’s audit operations continued to be
operated by Pharm/DUR’s existing management team, including the Relator, who stayed with
the new company as a Managing Director.
21. ACS was acquired by The Xerox Corporation in February of 2010. Relator Spay
retired from ACS in May of 2011.
B. Defendants
1. Defendant CVS Caremark Corporation
22. Defendant CVS Caremark Corporation (hereafter “CVS Caremark”), the largest
provider of prescriptions and related healthcare services in the United States, is incorporated
under the laws of the state of Delaware, and headquartered at One CVS Drive,
Woonsocket, Rhode Island 02895.
23. CVS Caremark was formed on March 22, 2007, as the result of a merger between
CVS Corporation and Defendant Caremark, Rx, Inc. At that time, Defendant Caremark Rx, Inc.
was merged with CVS Corporation and into a newly-formed subsidiary of CVS Corporation,
Caremark Rx, LLC, with the CVS subsidiary continuing as the surviving entity. Following the
merger, the merged company changed its name to “CVS Caremark Corporation.”
24. CVS Caremark has reported to the public that since at least 2007, it has been the
largest provider of prescription and related healthcare services in the United States, having filled
7
or managed more than one billion prescriptions since that time.
25. CVS Caremark operates two business segments: retail pharmacy and pharmacy
services. In 2010, Defendant CVS Caremark’s PBM filled or managed approximately 585
million prescriptions. That same year, its retail pharmacy segment filled approximately 636
million retail prescriptions, which accounted for 18% of the entire U.S. pharmacy market.
26. In its retail pharmacy segment, CVS Caremark operates a national retail pharmacy
network with over 60,000 participating pharmacies, including more than 6,000 retail CVS
pharmacy stores. CVS Caremark also operates an on-line pharmacy, CVS.com®, and mail order
and specialty pharmacies.
27. CVS Caremark’s Pennsylvania operations include 384 retail stores, one specialty
pharmacy store, and two specialty mail order facilities.
28. In its pharmacy services business, CVS Caremark offers a full range of pharmacy
benefit management (“PBM”) services. The PBM business generates revenues for CVS
Caremark primarily from dispensing prescription drugs and performing related services for
which it receives certain fees. These PBM services include mail order pharmacy services,
specialty pharmacy services, plan design and administration, formulary management, and claims
processing. For calendar year 2007, CVS Caremark’s largest customer was the Federal
Employees Health Benefits Program (“FEHBP”). It continues to be one of its largest customers.
29. CVS Caremark has been administering the retail pharmacy benefit program for
the largest FEHBP Plan, the Blue Cross and Blue Shield Government-wide Service Benefit Plan,
(also known as the Federal Employee Program (“FEP”)) since 1993.
30. In late 2009, Defendant CVS Caremark’s contract with FEP was extended
through the end of 2011. A new agreement, announced in May of 2011, further extends CVS
8
Caremark’s contract with the FEP through 2014, and includes mail-order pharmacy and specialty
pharmacy services on top of retail pharmacy benefit services, including network contracting and
management of customized clinical programs.
31. All prescriptions managed by CVS Caremark, whether filled at one of its own
mail service pharmacies or through its own retail pharmacy, are uniformly and systematically
analyzed, processed and documented by CVS Caremark’s nationwide proprietary prescription
management systems.
32. According to CVS Caremark’s own financial reports, these uniform computerized
prescription management systems assist staff and network pharmacists in the processing of
prescriptions by automating tests for various items, including plan eligibility, early refills,
duplicate dispensing, appropriateness of dosage, drug interactions or allergies, over-utilization
and potential fraud issues.
2. CVS Caremark Entities Participating in Medicare Part D Program
33. Currently, Defendant CVS Caremark participates in the Medicare Part D
prescription drug program in several significant ways. Attached as Exhibit “A” is an
organizational chart describing the CVS Caremark entities involved in its Medicare Part D
business. Since 2006, CVS Caremark has provided Part D PBM services to CVS Caremark’s
clients’ Part D Plans through the following subsidiaries: SilverScript, Inc; Caremark LLC;
CaremarkPCS; CVS Caremark Part D Services, LLC; and RxAmerica, LLC.
34. Since 2006, CVS Caremark has served as a Medicare Prescription Drug Plan
(“PDP”) Sponsor that contracts with Medicare to provide prescription drug benefits in all 50
states, the District of Columbia, and Puerto Rico, through SilverScript Insurance Company
(“SSIC”) and Accendo Insurance Company (“Accendo”).

9
35. CVS Caremark acquired Accendo. Effective January 1, 2009, Accendo replaced
RxAmerica® as the Medicare-approved prescription drug plan for the RxAmerica Medicare Part
D drug benefit plans.
36. In addition, CVS Caremark operates thousands of retail pharmacies, as well as
mail order and specialty pharmacies that process Part D prescriptions and dispense Part D drugs
to Medicare beneficiaries.
37. Since 2006, through its subsidiary, SSIC, a Medicare Part D Prescription Drug
Plan (“PDP”) Sponsor, CVS Caremark has provided Medicare Part D drug benefits to eligible
beneficiaries.
38. SSIC and Accendo are PDPs that contract with Medicare to provide prescription
drug plans in all 50 states, the District of Columbia, and Puerto Rico.
39. In December 2010, CVS Caremark announced an agreement to acquire the
Medicare Part D business of Universal American Corp. (“UAM Medicare Part D business”) for
approximately $1.25 billion. This acquisition was completed on April 29, 2011. Through its
UAM Medicare Part D business, CVS Caremark provides Medicare prescription drug benefits to
more than three million beneficiaries though the Community CCRxSM prescription drug plan.
3. Defendant CVS Caremark’s PBM Subsidiary, Caremark Rx
40. Defendant Caremark Rx, LLC (f/k/a Caremark Rx, Inc.) (hereafter “Caremark
Rx”) is one of the largest pharmaceutical services companies in the United States. It is
incorporated under the laws of the state of Delaware, with its principal executive offices located
at 211 Commerce Street, Suite 800, Nashville, Tennessee, 37201. Caremark Rx is the parent of
CVS Caremark’s pharmacy services subsidiaries.
41. In 2006, and prior to the March 2007 merger, Caremark Rx, was one of the largest
10
pharmaceutical services companies in the United States with net revenues exceeding $36 billion.
As of December 31, 2006, Caremark Rx employed more than 13,000 people.
42. Caremark Rx’s pharmaceutical services are referred to as pharmacy benefit
management (“PBM”) services, and include both the facilitation of dispensing prescription drugs
to eligible participants in benefit plans maintained by its customers, as well as the provision of
drug benefits to eligible beneficiaries under the Federal government’s Medicare Part D Program.
43. In short, Caremark Rx, through its subsidiaries, operates mail order, specialty
mail order and retail specialty pharmacy subsidiaries, all of which conduct business throughout
the United States and/or its legal territories.
44. The pharmacy services segment of CVS Caremark’s business includes the
provision of products and services to managed care entities that provide services to beneficiaries
of Medicare, Medicaid, and other government-sponsored healthcare programs, as well as
employers who qualify for the retiree drug subsidy.
45. CVS Caremark participates in the administration of Medicare (Part D) Drug
Benefit through Caremark Rx. Caremark Rx’s PBM services are provided to its health plan
clients and other clients that have qualified as Medicare Part D drug Plans, or PDPs. Caremark
Rx’s customers are primarily sponsors of health benefit plans (employers, unions, government
employee groups, insurance companies, and managed care organizations).
46. CVS Caremark also participates extensively in the Medicare Part D Program by
assisting employer, union, and other health plan clients that qualify for the Medicare Part D
retiree drug subsidy by collecting and submitting eligibility and/or drug cost data to CMS as
required under Part D in order for these employer, union, and other health plan clients to obtain
Part D retiree drug subsidies.

11
a. Caremark Rx Provides Its Part D PBM Services Through A
Subsidiary SilverScript, LLC
47. Defendant SilverScript, LLC (f/k/a SilverScript, Inc.) (hereafter “SilverScript”) is
a Delaware limited liability company with its principal place of business at 2211 Sanders Road,
Northbrook, IL 60062.
48. From before January 1, 2006 through March 22, 2007, SilverScript was a wholly-
owned subsidiary of Caremark Rx. SilverScript is now a wholly-owned subsidiary of Defendant
CVS Caremark.
49. Since 2006, Defendant Caremark Rx, through SilverScript, has provided PBM
services to Part D Plan Sponsors throughout the country. These Part D Plan Sponsors include, at
times relevant to this matter, Medical Card System, Inc. (hereafter “MCS”) and its affiliated PDP
Sponsor, MCS Life. MCS is a for profit corporation registered in the Commonwealth of Puerto
Rico. See paragraphs 65-78, infra.
50. During 2006 alone, Caremark Rx managed more than 516 million prescriptions
for individuals from more than 2,000 organizations, including its largest customer, the FEHBP,
which accounted for more than 16% of Defendant Caremark Rx’s net revenue.
51. During 2006, Caremark Rx derived substantially all of its net revenue from
dispensing prescription drugs to eligible participants in benefit plans maintained by its health
plan sponsor customers and to individuals throughout the United States.
52. SilverScript provides managed PBM services to Part D Plan Sponsors throughout
the country, including, at times relevant to this matter, to MCS Life. Following the March 2007
merger, Caremark Rx continued to provide these same services through its subsidiaries, which
then operated as subsidiaries of the newly-formed entity, CVS Caremark.
53. From 2006 until sometime just prior to 2009, CVS Caremark provided Part D
12
PBM services through its subsidiary SilverScript. Sometime before 2009, CVS Caremark’s Part
D PBM was known as and doing business as "CVS Caremark Part D Services, LLC.” CVS Part
D Services, LLC, is a Delaware limited liability corporation with a registered agent located at
Corporation Trust Center, 1209 Orange Street, Wilmington, DE 19801.
b. Other CVS Caremark Entities Providing Part D PBM Services
54. Defendant Caremark, LLC (f/k/a Caremark, Inc.) (hereafter “Caremark”) is a
California limited liability company which has its principal place of business at 2211 Sanders
Road, Northbrook, IL 60062. Caremark is a wholly-owned subsidiary of CVS Caremark.
55. In 2006 and before the March 2007 CVS-Caremark merger, Defendant Caremark
Rx conducted its pharmaceutical services operations through its subsidiaries, including but not
limited to, Caremark, Inc. (now Defendant Caremark LLC) and CaremarkPCS (f/k/a
AdvancePCS).
4. Defendant CVS Caremark’s Medicare Part D Plan (PDP) Sponsor,
SilverScript Insurance Company _____ _
56. CVS Caremark additionally participates in the Medicare Part D Program through
the offering of Medicare Part D benefits by its subsidiary, SilverScript Insurance Company, a
subsidiary of SilverScript.
57. In 2005, Defendant Caremark Rx through its subsidiaries Caremark and
SilverScript, formed SilverScript Insurance Company to participate as a Part D Plan (PDP) under
the Medicare Drug Benefit. In 2006, SilverScript Insurance Company obtained a license from
the State of Tennessee to operate as a health insurance company.
58. Since 2006, Defendant CVS Caremark has participated in Medicare Part D
prescription program through the offering of Medicare Part D pharmacy benefits by its
subsidiary, SilverScript Insurance Company, which has been approved by CMS as a prescription

13
drug plan (PDP) Sponsor under Medicare Part D in all regions of the United States.
59. SilverScript Insurance Company, a direct wholly-owned subsidiary of CVS
Caremark Corporation, now offers Part D Plans in all 50 states, Washington D.C. and
Puerto Rico. For the year ended 2008, SilverScript Insurance Company was licensed in
Pennsylvania, which represented $47.8 million in direct written business for Part D Plans,
SilverScript's second-highest market next to New York state.
60. SilverScript Insurance Company, a national Part D Sponsor, and SilverScript,
Inc., a Medicare Part D pharmacy benefit management company (PBM), are both subsidiaries of
CVS Caremark.
5. CVS Caremark Revenues Related to Medicare Part D Services
61. CVS Caremark Defendants participate in the Federal government’s Medicare Part
D program as a PDP and as a PBM. CVS Caremark’s net revenues include both Part D payments
received from CMS, as well as payments received from Part D Sponsors related to CVS
Caremark’s subsidiaries’ Part D PBM services.
62. CVS Caremark’s Part D insurance premiums earned by its PDPs, are set based on
the PDP’s annual bid and related contractual arrangements with the Centers for Medicare and
Medicaid Services (“CMS”). The Part D insurance premiums include a direct premium paid by
CMS to CVS Caremark’s subsidiary and a beneficiary premium, which is the responsibility of
the PDP member. The Part D beneficiary premium is subsidized by CMS in the case of low-
income members. CVS Caremark collects Part D insurance premiums from beneficiaries and
CMS then recognizes them ratably as revenue over the period in which members are entitled to
receive benefits.
63. In addition to the Part D insurance premiums, CVS Caremark’s net revenues

14
include co-payments, deductibles and co-insurance (collectively, the “Member Co-Payments”)
related to PDP members’ actual prescription claims. CMS subsidizes a portion of these Member
Co-Payments by paying CVS Caremark an estimated prospective Member Co-Payment subsidy
each month. The prospective Member Co-Payment subsidy amounts received from CMS are also
included in CVS Caremark’s net revenues, and represented 2.6%, 3.5% and 1.3% of CVS
Caremark’s consolidated net revenues in 2010, 2009 and 2008, respectively. If the prospective
Member Co-Payment subsidies received differ from the amounts based on actual prescription
claims, CVS Caremark records the difference as either accounts receivable or accrued expenses.
64. The Medicare Prescription Drug, Improvement, and Modernization Act of 2003
(“MMA”) created a drug subsidy program available to certain employer, union and other group
plans that provide retiree coverage to Medicare Part D eligible individuals that is at least
equivalent to Medicare Part D coverage. The Part D retiree drug subsidy is equal to 28% of drug
costs, and is currently (until 2013) tax-free. CVS Caremark’s net revenues also include these
retiree drug subsidies paid by CMS.
C. The "Medical Card System" Entities
1. Medical Card System, Inc.
65. Medical Card System, Inc. (hereafter, “MCS”) is a for profit corporation
registered in the Commonwealth of Puerto Rico, whose principal place of business is located at
225 Ponsce de Leon Avenue, Hato Rey, Puerto Rico.
66. MCS is the second largest health administration and health insurance company in
Puerto Rico with more than 725,000 commercial, Medicare, and Puerto Rico Medicaid
(“Reforma”) insured lives. MCS provides health plans to more than 1,000 companies and covers
over 150,000 employees and family members. MCS has been operating in Puerto Rico for over

15
26 years and employs more than 500 people.
67. Among other health services, MCS provides medical plans in Puerto Rico,
Medicare Part D coverage through both PDPs and Medicare Advantage Part D Plans (“MA-
PDs”) which are offered through MCS's subsidiary, MCS Life Insurance Company. MCS also
provides Part D coverage to employers who offer Part D benefits through employer plans to
whom Part D retiree drug subsidies would apply.
68. In addition, MCS, through its affiliate, MCS Advantage, Inc., also provides
managed Medicare coverage. MCS Classicare healthcare plans provide MA-PD coverage to
beneficiaries receiving Medicare Part C (managed care) coverage through MCS Advantage, Inc.
69. MCS provides pharmacy benefits to dual eligible Medicare Part D and Medicaid
beneficiaries, including members impacted by Low Income Subsidy grants available to Medicare
Part D beneficiaries living in the United States territories.
2. MCS Life Insurance Company
70. MCS Life Insurance Company (hereafter “MCS Life”) is a for profit corporation
registered in the Commonwealth of Puerto Rico, whose principal place of business is located at
225 Ponsce de Leon Avenue, Hato Rey, Puerto Rico.
71. MCS Life is a subsidiary of MCS. At all times relevant hereto, MCS Life
provided Medicare Part D coverage to plans offered by MCS.
72. In November 2004, CMS approved MCS Life’s request to offer managed care
coverage to Medicare beneficiaries in the San Juan, Puerto Rico metro area and in 50 other
municipalities in Puerto Rico, where approximately 325,000 Medicare beneficiaries lived.
73. Since January 1, 2006, MCS Life has participated with CMS as a Medicare Part D
Plan Sponsor, providing Medicare Part D coverage to plans offered by MCS.

16
74. From January 1, 2006 through at least September 2007, pursuant to the terms of a
contract executed between them (“the Part D Contract”), CVS Caremark and SilverScript
provided Medicare Part D PBM services to MCS Life for health insurance plans offered by
MCS.
75. At the time of the Part D Contract in early 2006, MCS Life offered Part D
benefits through a number of PDPs and MA-PDs, including: MCS Classicare Rx (PDP); MCS
Classicare Rx2 (PDP); Classicare (MA-PD); Platino MAPD; and Platino SNP.
76. MCS Life developed formularies for the following Part D Plans: MCS Classicare
Rx (PDP); MCS Classicare Rx2 (PDP); and MCS Classicare PFFS (Premium MA-PD); MCS
Classicare Rx Standard (PDP).
77. At the time of the Part D Contract in early 2006, MCS Life also offered Part D
benefits to employer plans providing prescription coverage to their retirees. These retiree Plans
include: Ela 9.3 (MA-PD); Ela Rx (PDP), Ela Rx2 (PDP), BPPR (MA-PD), BPPR Premium
((MA-PD), Avon (MA-PD), BASF (MA-PD), Island Finance (MA-PD), Prossam Rx (PDP).
78. In or about February 2007, MCS retained Relator Spay’s company, Pharm/DUR,
to perform a comprehensive audit of the Medicare Part D PBM services provided for MCS Life
by SilverScript.
III. JURISDICTION AND VENUE
79. This Court has jurisdiction over the subject matter of this action pursuant to
28 U.S.C. § 1331, 28 U.S. C. § 1367 and 31 U.S.C. § 3732.
80. This Court has personal jurisdiction and venue over Defendants pursuant to
28 U.S.C. §§ 1391(b) and 31 U.S.C. § 3732(a) because that section authorizes nationwide service
of process and because the Defendants have minimum contacts with the United States.

17
Moreover, the Defendants can be found in, and reside and transact business in, this District.
81. Venue is also proper in this District pursuant to 31 U.S.C. § 3731(a) because
Defendant CVS Caremark can be found in, and conducts business in this District. At all times
relevant to this Complaint, Defendant CVS Caremark regularly conducted substantial business
within the Eastern District of Pennsylvania, maintained employees and offices in Pennsylvania,
and made significant sales within Pennsylvania, where its facilities include hundreds of retail
stores, one specialty pharmacy store, and two specialty mail order facilities.
82. In addition, the statutory violations as alleged herein, occurred within this District.
IV. APPLICABLE LAW
A. The Medicare Part D Program: Prescription Drug Coverage
83. The Medicare Part D Program provides beneficiaries with assistance in paying for
out-patient prescription drugs. This massive out-patient prescription drug benefit was added to
Medicare by the Medicare Prescription Drug, Improvement, and Modernization Act of 2003,
(“MMA”), Pub. L. 108-173 (Dec. 8, 2003), 42 U.S.C. § 1395w-101 et seq. (2004 supplement),
42 C.F.R. § 423.506.
84. The MMA provides that Medicare beneficiaries entitled to Medicare benefits
under Part A or enrolled in Part B are eligible for Medicare Drug benefits under Part D. Section
1860D-2 of the Social Security Act, 42 U.S.C. 1395w-102, provides for out-patient prescription
drugs to be provided to Medicare beneficiaries to be called “Medicare Part D” benefits which
began in January 2006.
85. If a drug, as prescribed and dispensed or administered to an individual, is covered
for that individual under Medicare Part A or Part B, then the drug is not covered under
Part D. 42 U.S.C. § 1396w-102(e)(2)(B), Section 1860D-2(e)(2)(B) of the Social Security Act.
18
86. The MMA also created a subsidy available to certain employer, union, and other
group Plans that provide retiree coverage to Part D eligible individuals that is at least equivalent
to Part D coverage (the “retiree drug subsidy”). Section 1860D-22 of the Social Security Act, 42
U.S.C. § 1395w-132. Thus, the Federal government pays a Part D retirement subsidy to
employers whose Plans provide prescription drug benefits similar to Part D Plans for their retired
employees.
B. Entities Operating in the Medicare Part D System
1. Part D Sponsor
87. Unlike coverage in Medicare Parts A and B, Part D coverage is not provided
within the traditional Medicare program. Instead, Medicare beneficiaries must affirmatively
enroll in one of many hundreds of Part D Plans offered by private companies such as the
Caremark Defendants. See, MMA, Sections 1102, 1860D-1 through 1860D-42, and 1871 of the
Social Security Act; 42 U.S.C. §§ 1302, 1395w-101 through 1395w-152, and 1395hh.
88. A Medicare Part D Plan Sponsor ("Part D Sponsor"), whether it be a Part D Plan
or PDP, or a Medicare Advantage Prescription Drug Plan or MA-PD, is an entity that is certified
as meeting the requirements of Part D and that contracted with CMS to provide Part D benefits.
Section 1860D-41, 42 U.S.C. § 1395w-151(a)(13) and (14)(B). The term "Part D Sponsor" also
includes employer and union-sponsored plans which offer qualified Part D prescription coverage.
42 C.F.R. § 423.4.
89. Under Part D, the process begins with the health insurance company submitting a
certified application to CMS to participate as a Part D Plan Sponsor to provide prescription drug
coverage to qualifying Part D Plans. 42 C.F.R. §§ 423.502, 423.265 and 423.272. That
application is a prerequisite for contracting with CMS as a Part D Plan Sponsor. 42 C.F.R. §

19
423.504(b). CMS is authorized to deny an application to qualify as a Part D Sponsor based on
the applicant’s failure to comply with the terms of a previous year’s contract with CMS, even if
the applicant is currently meeting all of the requirements for Part D participation. 42 C.F.R.
423.503(b).
90. The Part D Plan Sponsor must also agree to comply with the requirements and
standards of Part D and all the terms and conditions of payment. Section 1860D-12, 42 U.S.C. §
1395w-112(b)(1).
91. The contract between the Part D Plan Sponsor and CMS must include the
elements listed in 42 C.F.R. § 423.505(b), including compliance with the reporting requirements
as set forth in § 423.514 and the requirements set forth in § 423.329(b) for submitting drug
claims and related information to CMS for its use in risk adjustment calculations. The Part D
Plan Sponsor must also expressly agree to provide CMS with the information CMS determines is
necessary to carry out payment provisions. 42 C.F.R. § 423.505(b)(8) and (9).
92. A Part D Plan Sponsor, in contracting with CMS, also expressly “agrees to
comply with Federal laws and regulations designed to prevent fraud, waste, and abuse, including,
but not limited to, applicable provisions of Federal criminal law [and] the False Claims Act (32
U.S.C. §§ 3729 et seq.).” 42 C.F.R. 423.505(h)(1).
93. To qualify for Part D payments from CMS, before each plan year, each approved
Part D Plan Sponsor must submit a bid, certified by an actuary, for each Part D Plan it will offer.
42 C.F.R. § 423.265. The bid contains a per member per month (“PMPM”) cost estimate to
provide Part D benefits to an average Medicare beneficiary in a particular geographic area. CMS
considers both the tiered formulary structure and utilization management program components of
the Part D Plan Sponsor’s bid. 42 C.F.R. § 423.272(a)(2). From those Part D Plan bids, CMS

20
calculates nationwide and regional benchmarks which represent an average PMPM cost. If the
Part D Plan Sponsor’s bid exceeds the benchmark, the Plan Member must pay the difference.
94. Once approved, the Part D Plan Sponsor may market its Plans to eligible
Medicare Part D beneficiaries, but CMS sets restrictions on marketing and enrollment. 42
C.F.R. § 423.50.
95. During each benefit year, CMS pays the Part D Plan Sponsors estimated
payments on a monthly basis. In turn, Part D Plan Sponsors provide CMS with documentation
of their actual costs. One required method for Part D Plan Sponsors to provide actual cost
information to CMS is by submitting a Prescription Drug Event (“PDE”) record for every
prescription that is filled for a Plan Member.
96. Once enrolled, each Part D Plan participant pays a monthly premium to the Part D
Plan, as determined under the Part D Regulations. 42 C.F.R. §§ 423.153 and 423.293.
97. In the year following each benefit year, CMS reconciles a PDP Sponsor’s actual
prescription drug costs as derived from its PDE records against the Sponsor’s bid. If a PDP
sponsor’s actual costs exceed the estimated costs, the Sponsor may be able to recoup some of its
losses through a risk-sharing arrangement with CMS. Conversely, if a Part D Plan Sponsor’s
estimated costs exceed its actual costs, the Sponsor may have to pay back some of its estimated
payments to CMS.
98. Thus, CMS pays the Part D Sponsor under Medicare Part D. The Part D Sponsor
then pays the Part D Plan pharmacies for prescriptions, less the Medicare beneficiary’s co-pay.
99. The Part D Sponsor is required to make several significant and material express
certifications to CMS regarding its submission of Part D data used for payment:
21
1. Certification of Data that Determines Payment: “As a condition for
receiving a monthly payment … the Part D Plan sponsor agrees that its
chief executive officer (CEO), chief financial officer (CFO), or an
individual delegated the authority to sign on behalf of one of these
officers, and who reports directly to the officer, must request payment
under the contract on a document that certifies (based on best knowledge,
information, and belief) the accuracy, completeness, and truthfulness of all
data related to payment. The data may include specified enrollment
information, claims data, bid submission data, and other data that CMS
specifies.” 42 C.F.R. § 423.505(k)(1).
2. Certification of Enrollment and Payment Information: “The CEO, CFO, or
an individual delegated the authority to sign on behalf of one of these
officers, and who reports directly to the officer, must certify (based on best
knowledge, information, and belief) that each enrollee for whom the
organization is requesting payment is validly enrolled in a program offered
by the organization and the information CMS relies on in determining
payment is accurate, complete, and truthful and acknowledge that this
information will be used for the purposes of obtaining Federal
reimbursement.” 42 C.F.R. § 423.505(k)(2).
3. Part D Sponsor Certification of Claims Data: “The CEO, CFO, or an
individual delegated with the authority to sign on behalf of one of these
officers, and who reports directly to the officer, must certify (based on best
knowledge, information, and belief) that the claims data it submits under §

22
423.329(b)(3) (or for fallback entities, under § 423.871(f)) are accurate,
complete, and truthful and acknowledge that the claims data will be used
for the purpose of obtaining Federal reimbursement.” 42 C.F.R. §
423.505(k)(3).
4. Certification of Bid Submission Information. The CEO, CFO, or an
individual delegated the authority to sign on behalf of one of these
officers, and who reports directly to the officer, must certify (based on best
knowledge, information, and belief) that the information in its bid
submission and assumptions related to projected reinsurance and low
income cost sharing subsidies is accurate, complete, and truthful and fully
conforms to the requirements in § 423.265.” See, 42 C.F.R. §
423.505(k)(4).
100. The Part D Sponsor is required to expressly certify to the accuracy and
completeness of allowable costs for risk corridor and reinsurance information and of data for
price comparison that it submits to CMS. 42 C.F.R. § 423.505(k)(5) and (6).
101. Particularly relevant here, the entity submitting the Part D payment data, the Part
D Sponsor or PBM, must also make express certifications to CMS regarding Part D data used for
payment. The Federal regulations provide that the entity submitting Part D claims data, the Part
D Sponsor or the PBM, must execute the following certification:
“If the claims data are generated by a related entity,
contractor, or subcontractor of a Part D plan sponsor, the
entity, contractor, or subcontractor must similarly certify
(based on best knowledge, information, and belief) the
accuracy, completeness, and truthfulness of the data and
acknowledge that the claims data will be used for the purposes
of obtaining Federal reimbursement.”

23
42 C.F.R. § 423.505(k)(3), (emphasis added).
2. First Tier, Downstream, and Related Entities
102. The regulations governing Part D benefits define major entities with which a
Part D Sponsor may contract. 42 C.F.R. § 423.505(i). See also CMS Prescription Drug Manual
Chapter 9 - Part D Program to Control Fraud, Waste and Abuse, 40 – Part D Sponsor
Accountability and oversight, p. 12. CMS has described these entities as “pharmacies or other
providers, related entities, contractors, subcontractors, first tier and downstream entities.”
103. A “First Tier Entity” is a party with whom the Part D Sponsor has a written
contract “acceptable to CMS with a Sponsor or applicant to provide administrative services or
health care services for a Medicare eligible individual under Part D." 42 C.F.R. § 423.501.
104. In most cases, the “First Tier Entity” will be a pharmacy benefits manager, PBM.
CMS Prescription Drug Manual Chapter 9 - Part D Program to Control Fraud, Waste and Abuse,
40 – Part D Sponsor Accountability and oversight, p. 12.
105. A “Downstream Entity” is any entity with a written contract with the Part D
Sponsor “below the level of the arrangement between a Sponsor and a first-tier entity.” 423.501.
Downstream entities include the ultimate service providers of health and administrative services,
i.e., pharmacies and further downstream below the pharmacy, the pharmacist. CMS Prescription
Drug Manual Chapter 9 - Part D Program to Control Fraud, Waste and Abuse, 40 – Part D
Sponsor Accountability and oversight, p. 12.
106. By way of simple illustration, the Part D Sponsor (here, Defendant MCS Life)
enters into a contract with PBM (here, the CVS Caremark Defendants). The PBM is the First
Tier Entity. The PBM then contracts with participating pharmacies to provide the dispensing
services. The pharmacies are Downstream Entities. If the pharmacies then contract with
24
pharmacists, the pharmacists would also be Downstream Entities. CMS Prescription Drug
Manual Chapter 9 - Part D Program to Control Fraud, Waste and Abuse, 40 – Part D Sponsor
Accountability and oversight, p. 12.
107. A Related Part D entity is “an entity that is related to the Part D Sponsor by
common ownership or control and either performs some of the Sponsor’s management functions
under contract or delegation, furnishes services to Medicare enrollees under oral or written
agreements, or certain lease arrangements with the Sponsor. This includes, for example, where a
Sponsor is the parent company of its own in-house PBM.” 42 C.F.R. § 423.501; CMS
Prescription Drug Manual Chapter 9- Part D Program to Control Fraud, Waste and Abuse, 40 –
Part D Sponsor Accountability and oversight, p. 13.
C. Summary of the Part D Process - Adjudicating Prescriptions
108. Most Medicare beneficiaries who elect Part D coverage are responsible for certain
costs, which may include a monthly premium, an annual deductible, and/or co-pays.
109. After receiving a prescription from his or her doctor, the Part D Plan beneficiary
goes to a retail pharmacy and presents the prescription to the pharmacist (or submits a
prescription to a mail order pharmacy).
110. The pharmacy receives the prescription and participant’s information, and then
submits required data elements to the Plan or its PBM to confirm Medicare Part D enrollment
and identify co-pays. This typically takes place via real-time data transmissions between the
pharmacy and the PBM.
111. The pharmacy must also perform pharmacy services, as required by state law.
For example, in Pennsylvania, pharmacy services include verifying the prescription being
prepared, performing checks for allergic reactions and drug interactions, and retaining the

25
prescription on file which identifies the prescriber.
112. Where the Part D Plan Sponsor uses a PBM, the PBM reviews the pharmacy's
initial data submission to conduct pre-dispensing/point-of-sale reviews of the Part D claim as
required by Federal law and regulations and pursuant to the contract between the Plan Sponsor
and the PBM.
113. If the claim for the prescription is not rejected by the Sponsor or PBM, the
pharmacy receives payment authorization and co-pay information and dispenses the prescription
to the Part D beneficiary. The beneficiary pays the co-pay to the pharmacy and receives the
prescription. At the time of the initial data submission, the pharmacy transmits to the Plan
Sponsor or PBM certain data elements specified by contract between the pharmacy and the Plan
Sponsor or PBM. These data elements would include, among other things, the beneficiary
information, prescriber information, and drug information.
114. Once the PBM or Plan receives that data from the pharmacy, the PBM or Plan
Sponsor submits the claim data to CMS via a Prescription Drug Event (“PDE”) record.
115. The Part D Plan or its PBM is required to also submit other data to CMS, i.e.,
enrollment information, bid submission data, costs for risk corridor and reinsurance information,
and data for price comparison. 42 C.F.R. 423.505 (k).
116. Part D Sponsors are also required to submit other information to CMS regarding
costs of providing Part D coverage, i.e., administrative costs, rebates, and other information.
117. Sections 1860D-15(c) (1)(C) and (d)(2) of the MMA require Sponsors to submit
data and information necessary for CMS to carry out payment provisions. For every prescription
filled, the Part D Sponsor or its PBM prepares and submits a PDE record to CMS.
118. The PDE record contains prescription drug cost and payment data that enables

26
CMS to make payments to Plans and otherwise administer the Part D benefit.
D. CMS Part D Payments Based on PDE Claims Data Submitted to CMS
119. Sections 1860D-14 and 15 of the MMA provide that CMS pay Plans for Part D
benefits through subsidies and risk sharing.
120. CMS pays a direct subsidy (a capitated payment) to the Part D Plan (PDP) in the
form of advance monthly payments equal to the Part D Plan's standardized bid, risk adjusted for
health status as provided in § 423.329(b), minus a monthly beneficiary premium as determined in
§ 423.286. 42 C.F.R. § 423.315(b). In other words, CMS pays a monthly sum to the Part D Plan
Sponsor for each Part D beneficiary enrolled in the Plan.
121. In addition to the direct subsidy, through low-income subsidies, CMS makes
payments to the Part D Plan for premium and cost sharing subsidies on behalf of certain subsidy-
eligible individuals as provided in § 423.780 and § 423.782. These types of premium and cost-
sharing subsidies for qualifying low-income individuals are called "Low-Income Cost Sharing
Subsidies" (LICS), and are documented and reconciled using PDE data submitted to CMS. CMS
“Updated Instructions: Requirements for Submitting Prescription Drug Event Data (PDE),”
4.27.2006, page 41, Section 10.1. In the United States Territories, CMS issues grants in lieu
of LICS.
122. Through retroactive adjustments and reconciliations, CMS also reconciles
payment year disbursements with updated enrollment and health status data, actual low-income
cost-sharing costs and actual allowable reinsurance costs as provided in § 423.343.
See 42 C.F.R. § 423.315(f). In other words, CMS reconciles payments received by Part D Plans
at the end of the year to determine whether additional funds are due to or from the Part D Plan
Sponsor.

27
123. For private fee-for-service plans (as defined by § 422.4(a)(3)) that offer qualified
prescription drug coverage, CMS determines the amount of reinsurance payments to be made to
them as provided under § 423.329(c)(3). See 42 C.F.R. § 423.315(g).
124. Thus, throughout the year, CMS makes prospective payments to Part D Sponsors
for three subsidies based on the Sponsors’ approved bids: (1) the direct subsidy (a monthly
capitated payment) designed to cover the Sponsor’s cost of providing the benefits; (2) the low-
income cost-sharing subsidy (the Federal government’s portion of cost-sharing payment for
certain low-income beneficiaries); and (3) the reinsurance subsidy (the Federal government’s
share of drug costs for beneficiaries who have reached catastrophic coverage).
125. A Part D Sponsor may also receive other payments from CMS resulting from
year-end reconciliations and adjustments.
126. Pursuant to 42 C.F.R. § 423.343, after the close of the plan year, CMS is
responsible for reconciling the prospective payments to the Part D Sponsor’s actual allowable
costs to calculate final payments and risk sharing amounts. CMS determines the Plan’s actual
allowable costs by relying upon certain data elements submitted by Sponsors in their PDE
records.
127. CMS specifically relies upon and uses the following PDE cost and payment fields
in its year end reconciliation: gross drug cost above out-of-pocket threshold, gross drug cost
below out-of-pocket threshold, low-income cost-sharing subsidy, and covered D Plan paid
amount (the four PDE data elements). The Sponsor, or its PBM, calculates the four data elements
from the point-of-sale claims data submitted by the pharmacy using instructions provided by
CMS.
128. In order to receive Part D funds from CMS, Part D Sponsors, their authorized
28
agents, employees, and contractors (including pharmacies) are required to comply with all
applicable Federal laws, regulations, as well as CMS instructions. 42 U.S.C. § 1860D-12(b)(1);
42 C.F.R. § 505(i)(4)(iv).
E. Medicare Part D Payments to Part D Sponsors Are Expressly Conditioned
Upon Submission of Accurate, Complete and True PDE Data
129. As an express condition of payment by CMS, all Part D Sponsors must submit
data and information necessary for CMS to carry out the payment provisions found in § 1860D-
15(c)(1)(C) and (d)(2) of the Social Security Act. Thus, CMS payments to a Part D Sponsor are
expressly conditioned upon the Sponsor providing “information to CMS that is necessary to
carry out this subpart, or as required by law.” 42 C.F.R. § 423.322 (a).
130. Accordingly, all contracts between Part D Sponsors and CMS must contain the
following term: the Part D Sponsor must agree to: “provide CMS with the information CMS
determines is necessary to carry out payment provisions in subpart G of this Part (or for fallback
entities, the information necessary to carry out the payment provisions in subpart Q of this
Part).” 42 C.F.R. § 423.505(b)(9).
131. In order to carry out these payment provisions, (42 C.F.R. § 423.329
determination of payments”), CMS mandatorily requires Part D Sponsors to submit data
regarding drug claims that can be linked at the individual level to Part A and Part B and other
information as CMS determines necessary. 42 C.F.R. § 423.329(b)(3)(i) (data collection).
1. Required Data Elements for PDE Records
132. On April 27, 2006, CMS issued “Updated Instructions: Requirements for
Submitting Prescription Drug Event Data (PDE)”, in which CMS identified a set of data
elements, Prescription Drug Event (“PDE”) data, which are necessary to determine payments to
Medicare Part D PDP Sponsors. The Part D Plan must submit a PDE record for each and every

29
dispensing event. “Updated Instructions: Requirements for Submitting Prescription Drug Event
Data (PDE),” 4.27.2006, page 9.
133. The PDE record is a summary record that documents the final adjudication of a
dispensing event by a PBM based upon claims received from pharmacies.
“Updated Instructions: Requirements for Submitting Prescription Drug Event Data (PDE),”
4.27.2006, page 9.
134. There are 37 set data elements in the required data set for all PDE records:
15 elements for the National Council for Prescription Drug Program ("NCPDP") billing
transaction, 5 data elements for the NCPDP billing response transaction, and 17 data elements
identified by CMS for purposes of administering Part D. “Updated Instructions: Requirements
for Submitting Prescription Drug Event Data (PDE),” 4.27.2006, page 9.
135. Most of the Medicare Part D PDE data elements are the same elements developed
by the NCPDP, which have been used for decades by PBMs, pharmacies, and other providers
when submitting Medicare and Medicaid claims for prescription drugs to CMS for payment. In
its “Instructions for Submitting Prescription Drug Event Data,” dated 4/27/2006, at page 11,
CMS stated: “Most data elements represent existing NCPDP fields where we employ the same
definition and field values that are currently in use per the NCPDP version 5.1 drug claim
standard.” NCPDP version 5.1 was approved in September of 1999.
136. When CMS identified “Data Elements for PDE Records,” it clearly stated, and all
parties were on notice, that submission of PDE data is an express condition of payment: “In this
section, we list the required data elements that must be submitted on PDE records for payment ...
This Section defines each data element and its specific potential use for CMS’s payment
process.” CMS “Updated Instructions: Requirements for Submitting Prescription Drug Event
30
Data (PDE),” 4.27.2006, page 11, Sec. 2.
137. CMS further described the purpose of the various PDE data elements as follows:
“Much of the data, especially dollar fields, will be used primarily for payment. However, some
of the other data elements such as pharmacy and prescriber identifiers will be used for validation
of the claims as well as for other legislated functions such as quality monitoring, program
integrity, and oversight.” CMS “Updated Instructions: Requirements for Submitting Prescription
Drug Event Data (PDE),” 4.27.2006, pages 5-6, Section 1.4.
138. CMS provided that the reporting “requirements apply to all Part D Plans.”
“Updated Instructions: Requirements for Submitting Prescription Drug Event Data (PDE),”
4.27.2006, page 5. Thus, CMS data reporting requirements and instructions apply to all Part D
Plans (PDPs), Medicare Advantage Part Plans (MA-PDs), and any other entity providing Part D
benefits.
2. Part D Claims – Certification of Truth and Accuracy
139. Sponsors and their subcontractors, i.e., PBMs, when submitting Part D PDE data
to CMS, must certify that all claims are true and accurate. CMS Prescription Drug Benefit
Manual, Chapter 9 – Part D Program to Control Fraud, Waste, and Abuse, Section 80.1, p.67,
citing 42 C.F.R. § 423.505(k)(3).
140. Thus, CMS’s Regulations for the submission of Part D PDE data place the legal
risk of submitting invalid Part D claims data squarely with the submitting or generating entity:
“CMS requires that any entity that generates [Part D] claims data on behalf of a Sponsor”
must both: “certify to CMS the accuracy, completeness, and truthfulness of that data;” and
“acknowledge that the data will be used for purposes of obtaining Federal
reimbursement.” See “Prescription Drug Benefit Manual, Chapter 9 – Part D Program to

31
Control Fraud, Waste, and Abuse,” page 16, Section 40-2; citing 42 C.F.R. § 423.505(k)(3))
(emphasis added).
141. In keeping with the requirements of 42 C.F.R. § 423.505(k)(3) and CMS
Prescription Drug Benefit Manual, Chapter 9 – Part D Program to Control Fraud, Waste, and
Abuse, Section 80.1, p.67, Sponsors and their subcontractors who submit Part D PDE data to
CMS must certify that it is true and accurate.
142. Since January 2006, this express certification of Part D PDE data has been
included in CMS’s Electronic Data Interchange (EDI) Agreement (or a similar document). The
EDI Agreement must be executed in order for an eligible organization to submit PDE data
electronically to CMS. The EDI is executed by Medicare Plans offering Part D prescription drug
benefit and/or the Part D PMBs who submit PDE data on behalf of Part D Sponsors. The
certification on the Part D EDI Agreement contains the following (or similar) language:
“By signing below, the eligible organization certifies that each
submission of PDE data pursuant to this Agreement will be
accurate and complete to the eligible organization's best
knowledge, information and belief.”
143. Defendants, through subsidiary Part D sponsors and/or PBMs, have made such
explicit certifications of PDE data from 2006 to the present. They continue to make these
certifications on an ongoing basis to the Government.
144. CMS also requires, through the EDI Agreement, that the Part D Sponsor both:
“ensure that every electronic entry can be readily associated and identified with an original
source document (e.g., an original drug claim) …,” and “retain all original source documentation
pertaining to any such particular Medicare prescription drug event for a period of at least 10
years after the prescription drug event is received and processed.”
145. CMS recognizes that the submission of “inaccurate or incomplete prescription

32
drug event (PDE) data” constitutes Part D fraud, waste, or abuse. CMS Prescription Drug Benefit
Manual, Chapter 9 – Part D Program to Control Fraud, Waste, and Abuse,” page 56.
146. Moreover, in addition to being legally obligated to submit and certify accurate
PDE data in the first instance, Part D Sponsors are also explicitly required to correct all
previously submitted PDE data if the data was erroneous when initially submitted. CMS 2007
Part D Reporting Requirements page 4.
147. Part D Sponsors are required to make PDE data submissions to CMS at the end of
the coverage year (or no later than 5 months after the close of the year) including PDE records,
adjustments, and deletions. See, 42 C.F.R. § 423.308. Part D Sponsors also submit cost reports
at the end of the year. 42 C.F.R. § 423.343. For 2006, however, CMS collected cost data on
LICS via PDE records instead of cost reports. “Updated Instructions: Requirements for
Submitting Prescription Drug Event Data (PDE),” 4.27.2006, page 10.
a. PDE Data on Gender, Prescriber, NDC
148. The 37 elements comprising a Medicare Part D PDE electronic data submission
include: the patient gender (field 7); the prescriber’s identification (fields 12 and 13); the
product/service ID (National Drug Code, “NDC” numbers (field 15).
149. A National Drug Code or “NDC” is an eleven-digit number which the
pharmaceutical manufacturer or labeler assigns to a pharmaceutical product and attaches to the
product container at the time of packaging. The NDC identifies the product manufacturer, dose
form and strength, and package size. NDCs must be assigned pursuant to Federal drug law. See,
21 C.F.R. 210.25(c)(1).
150. In addition, the PDE record alerts CMS if the data being submitted is for purposes
of correcting an earlier submission through adjustment and deletion codes (field 23)

33
(distinguishing original from adjusted or deleted PDE records). CMS "Updated Instructions:
Requirements for Submitting Prescription Drug Event Data (PDE),” 4.27.2006, page 9, Sec. 1.
151. The PDE data elements for gender, prescriber information, and product/service ID
(NDC) are not optional. CMS "Updated Instructions: Requirements for Submitting Prescription
Drug Event Data (PDE),” 4.27.2006, page 11, Section 2. Indeed, referenced above, the
prescriber identifiers are actually used and relied upon by CMS to validate the submitted claims.
Id. at pages 5-6, Section 1-4.
(i) Sponsors or PBMs Must Report the Patient’s Gender to
CMS
152. The PDE data element that identifies the patient’s true gender is contained in
Field 7 of the submitted PDE electronic data record.
153. Together with the health insurance claim number (HICN) at Field 4, and the
patient’s date of birth at Field 6, the gender patient identifier assists in confirming the identity of
the beneficiary. “Updated Instructions: Requirements for Submitting Prescription Drug Event
Data (PDE),” 4.27.2006, page 12, Section 2.
154. The patient's gender identification also impacts directly another significant Part D
requirement because Part D Plan Sponsors must conduct concurrent DURs including gender-
related contraindications. See also 42 C.F.R. § 423.153(c)(2)(ii).
155. When the PBM conducts appropriate concurrent DURs for gender-specific drugs,
this allows the PBM (and Sponsor) to confirm the accuracy of the patient's gender as reported by
the pharmacy and included by the PBM as part of the PDE electronic claim record submitted to
CMS.
156. In addition, appropriate collection and reporting of patient gender data not only
impacts patient safety by avoiding inappropriate use of gender-specific drugs, but also supports

34
the required programs to avoid fraud, waste and abuse related to theft or misuse of member
identification cards. For example, where a male may attempt to use the identification card of a
female in order to improperly obtain medications.
(ii) Sponsors or PBMs Must Report the Prescriber ID
Number to CMS
157. The PDE data elements that identify the prescriber are contained in fields 12 and
13 of the electronic PDE record. Field 12 contains the “Prescriber ID Qualifier,” the field that
indicates the type of identifier used in the Prescriber ID field. Field 13 contains the Prescriber ID
itself, meaning the prescriber’s own unique identification number, i.e., DEA number. CMS
“Updated Instructions: Requirements for Submitting Prescription Drug Event Data (PDE),”
4.27.2006, page 13, Section 2 (emphasis added).
158. CMS noted the following regarding the required PDE data on physician
identification numbers: “CMS requires use of a DEA number whenever it uniquely identifies the
prescriber and is allowed by state law. In other cases, the prescriber’s state license number or
Unique Provider Identification Number (UPIN#) shall be used.” CMS “Updated Instructions:
Requirements for Submitting Prescription Drug Event Data (PDE),” 4.27.2006, page 12,
Section 2 (emphasis added).
159. Thus, Part D Sponsors or their PBMs must report Part D claims data that
"uniquely identifies" the prescriber, either through a DEA number, or the prescriber’s State
license number, or through his unique Provider Identification Number (“UPIN”), when reporting
PDE data.
160. The vast majority of Part D claims submitted to CMS originate from electronic
data transmitted by the pharmacy to the Plan Sponsor or PBM at the point of sale (POS), in other
words, while the Part D beneficiary is at the pharmacy counter or while a mail order is being
35
processed after receipt at a mail order pharmacy.
(iii) Sponsors or Their PBMs Must Submit NDC Codes to
CMS
161. The PDE data elements that identify the dispensed drug are contained in
Field 15, “Product/Service ID,” which identifies the dispensed drug using an 11-digit NDC
number. “Updated Instructions: Requirements for Submitting Prescription Drug Event Data
(PDE),” 4.27.2006, page 13, Section 2.
b. Part D Sponsors or Their PBMs Must Submit Drug Cost Data
to CMS
162. When Part D Sponsors or their PBMs report PDE data to CMS, these data
elements include the costs associated with each dispensing event. CMS uses these PDE data
elements, in part, to determine the capitated payments (monthly subsidy) paid for each Medicare
Part D beneficiary. 42 C.F.R. § 423.505(k). The Part D Sponsor or PBM is required to submit
the cost of the drug actually dispensed to the Part D beneficiary.
163. CMS requires accurate reporting by the Part D Sponsor or PBM of the following
three data elements from PDE records to determine costs that qualify for payment under the
Medicare benefit: Field 27 (Ingredient Cost Paid), the amount paid to the pharmacy for the drug
itself, not including dispensing fees or other costs; Field 28 (Dispensing Fee Paid), the amount
paid to the pharmacy for dispensing the medication, including only “activities related to the
transfer of possession the drug from the pharmacy to the beneficiary, including charges
associated with mixing drugs, delivery, and overhead as delineated in the final rule § 423.100
and the preamble to the rule, which fee may be negotiated with pharmacies at the plan or PBM
level;” Field 29 (Sales Tax), all amounts paid to the pharmacy to cover sales tax. “Updated
Instructions: Requirements for Submitting Prescription Drug Event Data (PDE),” 4.27.2006,

36
pages 14-15.
164. Based upon these three data elements, CMS determines the costs associated with
each prescribing event that qualifies for Medicare Part D payment. Not only is it mandatory, but
it is crucial, that the Part D Sponsor or submitting PBM accurately reports to CMS the NDC for
the drug actually dispensed, as the cost the pharmacy paid for the particular drug is based upon
the NDC.
165. If the Part D Sponsor submits an NDC to CMS for a drug other than the drug
actually dispensed, then the data submitted in the Cost Fields (27 through 29) which is tied to a
particular NDC is false.
F. Part D Requirements for Dispensing "Covered Drugs"
166. Pursuant to Section 1860D-2(e)(1)(A) of the Social Security Act, a “covered
Part D drug” is defined as a drug that is “dispensed only upon prescription and that is described
in subparagraph (A)(i), (A)(ii), or (A)(iii) of section 1927(k)(2).” 42 U.S.C. 1395w-102(e).
Part D allows payment for any use of a covered Part D drug for a medically accepted indication.
§ 1395w-102(e)(1)(B).
167. The term “covered outpatient drug” is defined in Section 1927(k)(2)(A) of the
Social Security Act, 42 U.S.C. 1396r-8, to mean, “of those drugs which are treated as prescribed
drugs for purposes of section 1905(a)(12) [the Medicaid statute], a drug which may be dispensed
only upon prescription,” except as provided in paragraph (5), and subject to the exceptions in
paragraph (3). See also 42 C.F.R. 423.100.
168. Although Medicare Part D drugs must meet all Medicaid requirements, all drugs
covered under the Medicaid drug program are not necessarily covered under Part D.
Section 1860D-2(e) of the Social Security Act, 42 U.S.C. 1395w-102(e)(2).

37
169. Under Medicare Part D, CMS can pay only for drugs that both meet the definition
of “covered Part D drug” and are approved for coverage under the Sponsor's specific Plan.
Section 1860D-2(e) of the Social Security Act. See also 4/26/06 CMS Requirements for
Submitting Prescription Drug Event Data, p. 20.
170. Federal regulations also specifically require that each Part D Sponsor have an
established drug utilization management and quality assurance programs. 42 C.F.R. §
423.153(a). A drug utilization management program includes “policies and systems to prevent
over-utilization … of prescribed medications.” 42 C.F.R. 423.153(b)(2).
171. Quality assurance programs include compliance by network pharmacies with
State pharmacy practice and concurrent Drug Utilization Review (“DUR”). The purpose of
concurrent DUR, is to ensure that a review of the prescribed therapy is performed before each
prescription is dispensed to a Part D beneficiary. Concurrent DUR must include age and gender
contraindications, over-utilization, and incorrect dosage or duration of drug therapy. 42 C.F.R. §
423.153(c).
1. Part D Drugs – National Drug Codes (NDC)
172. Pursuant to Section 1927(k)(3) of the Social Security Act, 42 U.S.C. 1396r-8, the
term “covered outpatient drug” includes only those drugs for which a National Drug Code
number is required by the Food and Drug Administration, and specifically excludes “a drug or
biological used for a medical indication which is not a medically accepted indication.”
173. For obvious safety reasons, Federal Regulations further require drug
manufacturers or labelers to assign an expiration date to each pharmaceutical product, which
must appear on the label. 21 C.F.R. 201.17. 21 C.F.R. 211.137(a) and (d) (expiration dating).
174. Thus, the container received by the pharmacist from the manufacturer or labeler

38
bears the NDC, including the expiration date, as required by Federal Regulations.
175. Therefore, the Federal government will only pay for drugs under Medicare Part D
that are identified by NDC number when used for medically accepted indications, which are
listed in the labeling approved by the FDA, or use of which is supported by one of the drug
compendia identified in the Medicaid statute. See, Section 1927(g)(1)(B)(i) of the Social
Security Act.
2. Part D Requires Compliance with All State Pharmacy Laws
176. In addition to meeting the Medicaid statute’s definition of “prescribed drug,”
covered Part D drugs must be dispensed in accordance with State pharmacy laws and
regulations. 42 C.F.R. § 423.505(i)(4)(iv) (requiring compliance with Federal laws, Regulations,
and CMS instructions); 42 C.F.R. § 423.504(b)(iv)(A)(requiring compliance with applicable
Federal and state standards); 42 C.F.R. § 423.153(c)(1) (Sponsors must represent that that
network providers are required to comply with state pharmacy standards).
177. The Defendants here, as network providers for the Part D Plan Sponsors, were
required to comply with CMS Part D laws and all regulations mandating adherence to state
pharmacy laws.
178. States have enacted stringent laws regulating the practice of pharmacy and the
practice of medicine to protect patients from harm resulting from the use of unsafe or
inappropriate drugs and from the improper practice of medicine and pharmacy.
179. Under these State laws, for the patient to receive a prescription drug, a licensed
health care practitioner who determines the appropriate treatment, and issues a prescription for
an FDA-approved drug, must examine the patient. The prescription may also authorize refills.
The patient then has the prescription filled by a registered pharmacist working in a licensed

39
pharmacy that meets all State law requirements.
180. For example, Pennsylvania law requires that the pharmacist perform prospective
drug reviews ("PDR") before filling, delivering or sending a new retail or out-patient
prescription. See, Section 27.19 of the Pennsylvania Pharmacy Code. This PDR includes a
review of the patient profile and offer to counsel the patient or caregiver. Id. at § 27.19(b).
181. Pennsylvania law also requires that the prescription drug label contain the drug's
name, manufacturer, strength, manufacturer control number, and expiration date. See § 27.18(k).
Pennsylvania pharmacies must keep file records, including patient name and prescriber
identifiers, date of issue, etc., and also the original prescriptions for two years.
Id. at § 27.18(b).
182. The Pennsylvania Pharmacy Code specifically requires the removal from stock
and the disposal of expired drugs, and expressly prohibits the pharmacist from selling or giving
away expired drugs. Id. at § 27.14(b).
183. Here, as MCS provided Part D prescription drug coverage in Puerto Rico, a
“prescription drug or medication” is “[a]ny drug that is required under the Puerto Rico or the
United States laws to be dispensed by prescription, which shall be dispensed by a pharmacist in a
pharmacy duly authorized and registered by the Secretary of Health.” Puerto Rico Laws (P.R.L.)
Title 20 (Examining Boards and Professional Colleges), Chapter 20 (Pharmacy), Subchapter V
(Manufacture, Distribution, Dispensation of Medications) (hereafter, "P.R.L. Chapter 20"),
Section 400(kk).
184. Under Illinois law, a prescription must be issued by a licensed professional and
contain the prescriber's name, address, and signature; and DEA number where required for
controlled substances. 225 ILCS 85/3(e).

40
185. Illinois law also requires the pharmacist perform a DUR, including an offer to
counsel the patient, before any prescription is filled or refilled. See § 1330.700 of the Illinois
Pharmacy Practice Act, Title 68, Illinois Administrative Code.
186. Illinois law also requires that the prescription drug label contains the name and
address of the dispensing pharmacy, the name or initials of the person authorized to practice
pharmacy, the date on which such prescription was filled, the name of the patient, the serial
number of the prescription as filed, the prescriber’s last name, the directions for use, and the drug
name, dosage, and quantity. 225 ILCS 85/22.
187. Illinois pharmacies which move drugs from the manufacturer’s original container
to another container for dispensing must affix a label to the dispensing container which contains
“the name and strength of the drug, the name of manufacturer or distributor, beyond use date,
and lot number.” The “beyond use date” is the expiration date. Title 68, Illinois Administrative
Code § 1330.10. Under Illinois law, the expiration date for prepackaged drugs is the
manufacturer's expiration date or 12 months, whichever is less. Id. at § 1330.730; see also Title
77, Illinois Administrative Code, Section 725.20 (expired drugs are unfit for human
consumption).
188. Illinois pharmacies must keep file records, including patient name and prescriber
identifiers, date of issue, etc., and original prescriptions for five years. Id. at § 1330.500(c).
189. Under the Illinois Food Drug and Cosmetic Act states, “[d]rug products …
containing expiration dates or beyond use dates which have expired shall be considered non-
salvageable merchandise,” which includes drugs unfit for human consumption.
190. Likewise, under Puerto Rico law, pharmaceutical services required of the
pharmacist when dispensing drugs by prescription include: receiving, evaluating, and
41
interpreting the prescription; completing the patient's pharmaceutical records; labeling drugs in
compliance with all applicable Federal and State laws and regulations; verifying the prescription
against the medication and the patient's pharmacy record in order to identify, prevent, or solve
drug-related problems; and documenting this process. P.R.L. Chapter 20, § 407b(a) through (c).
191. Likewise, under Florida law, a pharmacist dispensing a prescription drug must
perform a DUR, including an offer to counsel the patient, before any prescription is filled or
refilled. Chapter 456 Florida Statutes Section 465.003(6). In addition, Florida law requires that a
prescription “contain the name of the prescribing practitioner, the name and strength of the drug
prescribed, the quantity of the drug prescribed, and the directions for use of the drug; must be
dated; and must be signed by the prescribing practitioner on the day when issued. A written
prescription for a controlled substance … must have the quantity of the drug prescribed … and
must be dated with the abbreviated month written out on the face of the prescription.” Chapter
456 Florida Statutes Section 456.42.
192. Under Florida law, the prescription label must include the name of the dispenser,
the date filled, the prescriber’s name, the patient’s name, and the directions for use. Chapter 499
Florida Statues 499.007.
193. Florida law also requires that the “manufacturer, repackager, or other distributor
of any medicinal drug shall display the expiration date of each drug … on the container and on
its packaging” and that the pharmacist or “practitioner dispensing medicinal drugs on an
outpatient basis shall display on the outside of the container of each medicinal drug dispensed, or
in other written form delivered to the purchaser either the expiration date when provided by the
manufacturer, repackager, or other distributor of the drug or an earlier beyond-use date for
expiration, which may be up to 1 year after the date of dispensing.” Chapter 456 Florida Statutes

42
Section 465.0255.
G. Part D Requirements of Sponsors Are Impacted When Services Performed
by the PBM Are Not in Compliance with Part D Requirements
194. Part D Sponsors often contract with PBMs for the adjudication of Part D claims
and the submission to CMS of Part D data necessary to receive payment. Federal Regulations
specifically require that Part D PBMs agree to perform all services in compliance “with all
Federal laws, regulations and CMS instructions.” 42 C.F.R. 423.504 (i)(4)(iv).
195. Thus, any Part D PBM who contracts with a Part D Sponsor to adjudicate
prescription drug benefit claims and submit Part D data to CMS must meet all compliance
standards established for Part D Sponsors.
1. Part D Sponsors and Their PBMs Are Required to Comply with All
Applicable State Laws
196. Federal Regulations also require that, in order to contract with CMS, a Part D
Sponsor must agree to comply with applicable State laws requirements and preemption by
Federal law requirements “described in subpart I of this part.” 42 C.F.R. 423.505(b)(15).
197. The importance of adhering to applicable State laws in the provision of Medicare
Part D prescription drug coverage is clear from Federal Regulations that require, as a condition
precedent to contract as a Part D Sponsor, “Any entity seeking to contract as a Part D Plan
Sponsor must [h]ave administrative and management arrangements satisfactory to CMS, as
demonstrated by at least … [a] compliance plan that consists of … [w]ritten policies, procedures,
and standards of conduct articulating the organization’s commitment to comply with all
applicable Federal and State standards. 42 C.F.R. 423.504(b)(iv)(A).
198. In addition, Part D Sponsors “must have established quality assurance measures
and systems to reduce medication errors and adverse drug interactions and improve medication

43
use that include a … [r]epresentation that network providers are required to comply with
minimum standards for pharmacy practice as established by the States.” 42 C.F.R.
423.153(c)(1).
2. Part D Sponsors and Their PBMs Must Deny Claims for Any Expired
Drugs
199. As discussed above, one of the data elements which the Sponsor, directly or
through a PBM, must report to CMS in the electronic PDE record is the “Product/Service ID,”
which “identifies the dispensed drug using a National Drug Code (NDC).”
200. As also discussed above, Federal Regulations require that drug manufacturers or
labelers assign an expiration date to each pharmaceutical product. 21 C.F.R. § 211.137(a) and
(d) (expiration dating). That is the expiration date that is communicated to CMS.
201. Once the manufacturer or labeler assigns the expiration date to a pharmaceutical
product, CMS uses the expiration date supplied by the manufacturer or labeler and maintains a
“First Data Bank” file or a similar compendium that identifies drugs that are outdated or have
been removed from the marketplace.
202. The First Data Bank date is the shelf life expiration date of the last batch of
product produced based upon federally mandated drug labeling requirements. The First Data
Bank file contains the NDC and corresponding expiration date for all drugs covered under the
Medicare Part D program.
203. Expired drugs are also sometimes referred to as “terminated drugs.”
A terminated drug product is one whose shelf life expiration date has been met, per
manufacturer notification. An obsolete NDC, on the other hand, is a national drug code
which has been replaced or discontinued by the manufacturer or labeler. See, e.g.,
http://medicaidprovider.hhs.mt.gov/providerpages/definitions.shtml.
44
204. Pharmacists cannot, nor should they ever, dispense expired drugs to beneficiaries.
Many State pharmacy codes expressly prohibit the dispensing of expired drugs. See, e.g., §
27.14(b) of the Pennsylvania Pharmacy Code; Ohio Revised Code, 3715.521(A); 21 C.F.R. §
211.137; Illinois Code § 725.20.
205. As an indication of the importance of the expiration date of prescription drugs
dispensed, the pharmacy laws of Puerto Rico governing the dispensing of prescription drugs also
require that the prescription label include the “date of expiration and lot number of the
medication.” Section 410(d).
206. A Part D Sponsor or PBM who reports an expired NDC to CMS is making a
claim for a drug that was not covered by Part D when dispensed and for which the Sponsor is not
entitled to receive any reimbursement. In fact, CMS has cited as an example of fraud by
downstream pharmacies the dispensing by pharmacists of expired drugs. Ch.9. Fraud, Waste and
Abuse at Section 70.1.3., page 58.
207. There are also serious health risks associated with using an expired drug or an
inaccurate NDC. For example, an expired drug may not be effective for the disease or condition
for which it was prescribed. If the pharmacy is using an NDC for an old lot number, but
dispensing a drug with an NDC that is current, the pharmacy is not complying with State
pharmacy laws that require that prescription labels include the proper expiration date for the drug
dispensed. Importantly, a Medicare beneficiary cannot tell whether his prescriptions are affected
by drug recalls or other safety concerns tied to a particular NDC.
208. Also, the pharmacy is then also able to take advantage of price differentials
between the NDC billed for and the NDC of the drug actually dispensed. In addition, under
Medicaid, rebates are lost when an expired NDC is billed.

45
3. Part D Sponsors or PBMs Must Deny Claims for Drugs Prescribed by
Excluded Providers
209. Part D Sponsors “shall not pay for drugs prescribed or provided by a provider
excluded either by HHA-OIG or GSA.” CMS Ch. 9, Part D Program to Control Fraud, Waste
and Abuse, 4.25.06, Section 50.2.6.3.3, page 45.
210. The Part D Sponsor or submitting PBM is required to report to CMS the
prescribing physician's identifier as part of the submitted PDE data record (PDE Field 12) to
receive payment from CMS.
211. In order to determine whether a provider is excluded, the Part D Sponsor or PBM
must first identify the provider and then compare the identified provider against the list of
excluded persons on the OIG or GSA exclusion list.
212. The Part D Sponsor or PBM is required to determine the prescriber's identity in
order to comply with CMS's mandate against payment for claims by excluded providers.
213. A Part D provider (whether a first tier or downstream entity) that fails to
accurately identify the prescribing physician in its PDE submission prevents the Part D Sponsor
from meeting CMS's strict requirement that Part D Sponsors refuse paying for prescriptions
written by excluded providers.
4. Part D Sponsors Must Conduct Concurrent DURs, Including Gender
Contraindications
214. Medicare Part D Regulations require that Part D Sponsors have in place
established quality assurance measures and systems to reduce medication errors and adverse drug
interactions and improve medication use. These Regulations require Concurrent Drug
Utilization Review (“Concurrent DUR”) systems, policies, and procedures. 42 C.F.R. § 423.153.
215. Concurrent DUR systems, policies, and procedures must be designed to ensure

46
that a review of the prescribed drug therapy is performed before each prescription is dispensed to
an enrollee in a Sponsor's Part D Plan. 42 C.F.R. § 423.153 (c)(2). It is too late to conduct DUR
after the prescription has already been dispensed.
216. The Medicare Part D Sponsor’s Concurrent DUR must include, at a minimum:
(i) Screening for potential drug therapy problems due to therapeutic duplication; (ii) Age/gender-
related contraindications; (iii) Over-utilization and under-utilization; (iv) Drug-drug interactions;
(v) Incorrect drug dosage or duration of drug therapy. (vi) Drug-allergy contraindications; and
(vii) Clinical abuse/misuse. 42 C.F.R. § 423.153 (c)(2).
217. CMS has specifically identified the use of claims processing systems as "an
effective tool for plans to monitor the delivery of the prescription drug benefit." CMS has
identified as examples of claims systems edits used to deny or suspend payments, "edits to
prevent payment of statutorily excluded drugs, real time contraindications (i.e., drug-drug
interactions) … sex and age edits compared to the drug prescribed.” CMS Prescription Drug
Manual Chapter 9 – Part D Program to Control Fraud, Waste and Abuse, Section 50.2.6.3.1,
p. 44.
218. Gender edits are part of necessary required safety edits. They must be performed
as part of the Part D Sponsor's Concurrent DUR, at the point-of-sale, and they assist the
pharmacist in identifying and/or preventing inappropriate drug therapy. 42 C.F.R. § 423.153
(c)(2)(ii).
219. Pharmacies and PBMs, including Defendants here, have been extremely familiar
with gender edits since long before the implementation of Medicare Part D. Indeed, the National
Council of Prescription Drug Programs, Inc. (NCPDP) Rejection Code 61, “Product/Service Not
Covered For Patient Gender,” has been in use since at least 2002.
47
220. In addition, since 1993, the Section 1927(g)(2)(A) of the Social Security Act has
required that State Medicaid providers perform prospective DUR (before the drug is filled and
delivered to the Medicaid beneficiary) to screen for potential drug therapy problems, including
“therapeutic duplication, drug-disease contraindications, drug-drug interactions (including
serious interactions with nonprescription or over-the-counter drugs), incorrect drug dosage or
duration of drug treatment, drug-allergy interactions, and clinical abuse/misuse.” Medicaid
programs have also limited access to certain drugs based on the gender of the beneficiary since at
least 2005.
221. Like the prescriber identifier data, gender edits are another key way to avoid
Fraud, Waste and Abuse in the Part D Program. The drug-beneficiary gender edit required under
Medicare Part D provides an important safeguard against drug diversion by confirming that the
person receiving the drug is the Medicare Part D beneficiary, and that the drug is not being
diverted to an inappropriate person or to illegal street sales.
222. Where the Part D Plan has failed to perform obligatory concurrent DUR,
including drug-to-gender edits, the Sponsor or PBM has submitted Part D claims for payment
that were not properly indicated as required by Federal Regulations. They also have submitted
PDE gender data that is false because they cannot make a true certification that the gender data
submitted is true or accurate.
5. Part D Sponsors Must Have a Comprehensive Fraud, Waste and
Abuse Plan
223. As referenced above, any authorized Part D Sponsor is required to have in place a
“comprehensive fraud, waste and abuse plan to detect, correct, and prevent fraud, waste, and
abuse as an element of their compliance plan." 42 C.F.R. § 423.504(b)(4)(vi)(H). This is a
cornerstone of CMS’s efforts to protect the Federal government and beneficiaries from fraud
48
related to the delivery of the Medicare prescription drug benefit.
224. In the Part D provider contract, the Part D Plan Sponsor must agree to
“comply with Federal laws and regulations designed to prevent fraud, waste, and abuse,
including, but not limited to applicable provisions of Federal criminal law, the False Claims Act,
32 U.S.C. Sec. 3729 et seq., and the anti-kickback statute, section 1128B(b) of the Act.”
42 C.F.R. § 423.505(h)(1).
H. CMS Identifies Areas Susceptible to Fraud by Part D Stakeholders
225. CMS has identified specific risk areas of vulnerability for fraud, waste and abuse
by specific key Part D stakeholders that are instrumental in the delivery of Part D benefits.
1. Part D Sponsor and PBM Fraud, Waste and Abuse
226. Sponsor and PBM fraud, waste and abuse occurs where the Part D Sponsor fails
to provide medically necessary services to Part D enrollees where this failure is likely to
adversely affect the enrollee. CMS Prescription Drug Manual, Chapter 9, Section 70.1.1, pages
54-55.
227. The failure to ensure that the drug was prescribed by a licensed professional, the
failure to deny claims for expired or obsolete drugs, and the failure to reject claims based on
gender contraindications are all examples of Sponsor and PBM fraud, waste and abuse that
adversely affect the enrollee.
228. Another area of Sponsor and PBM fraud, waste and abuse includes payments for
excluded drugs in violation of the Sponsor's obligation to ensure that they only provide coverage
for “covered Part D drugs,” under 42 C.F.R. § 423.100, as listed in the Sponsor’s approved
formularies, and in accordance with Section 1860D-2(e)(2) of the Social Security Act.
229. In addition, where a Part D Plan or PBM “misrepresents or falsifies information it

49
furnishes to CMS or to an individual under the Part D drug benefit program;” and when the PBM
or "Sponsor submits inaccurate or incomplete prescription drug event (PDE) data or Part D Plan
quarterly data," these are also examples of Sponsor fraud waste and abuse. CMS Prescription
Drug Manual, Chapter 9, Section 70.1.1, page 56.
230. Fraud, waste and abuse by a Part D PBM, as identified by CMS, includes most of
the same examples listed for Part D Plans, but also includes failure to offer a beneficiary the
negotiated price of a Part D drug. CMS Prescription Drug Manual, Chapter 9, Section 70.1.2,
pgs. 57-58.
2. Fraud, Waste and Abuse by Downstream Entities
231. Examples of pharmacy fraud, waste and abuse as identified by CMS include:
billing practices (billing for non-covered prescriptions as covered items, drug diversion, etc.);
bait and switch pricing; dispensing expired or adulterated prescription drugs; and failure to offer
negotiated prices. CMS Prescription Drugs Manual, Chapter 9, Section 70.1.3, page 58.
I. Requirements of Part D First Tier, Downstream, and Related Entities: All
Part D Downstream Entities Must Comply with all Applicable Federal and
State Laws and Regulations, and CMS Instructions
232. As described above, Federal Regulations require that Part D Sponsors follow
applicable State pharmacy laws. This requirement also applies to any first tier, downstream, or
related entity under contract to perform any of the Part D Sponsor’s activities or responsibilities
under the Part D contract with CMS. 42 C.F.R. § 423.505(i)(4)(iv) provides that “If any of the
Part D Plan Sponsors’ activities or responsibilities under its contract with CMS is delegated to
other parties, the following requirements apply to any related entity, contractor, subcontractor, or
pharmacy: … [a]ll contracts or written arrangements must specify that the related entity,
contractor, or subcontractor must comply with all applicable Federal laws, regulations, and

50
CMS instructions.”
233. Federal Regulations specifically require that Part D Sponsors establish quality
assurance measures and systems that require the Sponsor’s network providers “to comply
with minimum standards for pharmacy practice as established by the States.”
42 C.F.R. § 423.153(c)(1). A “network” provider is described as a pharmacy where enrollees
may be expected to obtain covered Part D drugs. See 42 C.F.R. § 423.128(b)(5) and (6).
234. In addition, Federal Regulations also require that Part D Sponsors comply with
State law requirements as described in 42 C.F.R. § 423.505(b)(15) (Part D Sponsors qualification
under state law as insurers) and meet all applicable Federal and State standards. 42 C.F.R. §
423.504(b)(iv)(A).
VII. FRAUD ALLEGATIONS:
A. Background: Contracts for Medicare Part D PBM Services Between
Caremark and MCS Life
235. In June 2003, Defendant Caremark Rx entered into a Prescription Benefit
Management ("PBM") Agreement with MCS, pursuant to which Caremark, Inc. provided PBM
services to health insurance Plans offered by MCS. The MCS-Caremark PBM Agreement was
amended in 2004 and again in 2006. Attached as Exhibit “B” is a true and correct copy of the
MCS-Caremark PBM Agreement.
236. MCS Life was approved by CMS to provide Medicare Part D coverage to health
insurance Plans offered by MCS.
237. In early 2006, MCS Life and Defendant SilverScript entered into a
Managed Pharmacy Benefit Services Agreement – Medicare Part D, which was effective January
1, 2006, pursuant to which SilverScript provided PBM services to support MCS Life’s
participation with CMS as a Part D Plan (PDP) Sponsor (the "MCS-SilverScript PBM

51
Agreement").
238. According to the terms of the MCS-SilverScript PBM Agreement, SilverScript
agreed “to participate, as a subcontractor to [MCS], in the management of [MCS's] Part D Plan,
and [SilverScript] understands that its activities must, to the extent these are communicated to
SilverScript, be consistent and comply with [MCS's] contractual obligations to CMS as a Part D
Plan Sponsor.” MCS-SilverScript PBM Agreement contract dated 1/1/06 at Section 1.1, p. 1.
239. MCS and SilverScript each agreed to “comply with applicable CMS Laws and
Regulations without the need for further notice to and approval from the other party.”
MCS-SilverScript PBM Agreement 1/1/06 at Section 1.1, p. 1.
240. According to the terms of the MCS-SilverScript PBM Agreement, the Medicare
Part D PBM services to be provided to MCS Life by Caremark Rx’s subsidiary included, but
were not limited to:
A. pharmacy services, whereby SilverScript would contract with a network of
participating pharmacies (retail, mail order and specialty) to perform
pharmacy services (i.e., to dispense prescriptions) for plan participants. MCS-
SilverScript PBM contract dated 1/1/06 at Section 1.2, p. 1. SilverScript
agreed that "its agreements with Participating Pharmacies and non-retail
pharmacies will be consistent and comply with [MCS's] contractual
obligations to CMS that [MCS] has communicated to SilverScript, and the
template agreement SilverScript has submitted to MCS. Each party agrees
that it shall comply with CMS Laws and Regulations without the need for
further notice to and approval from the other party." MCS-SilverScript
PBM Agreement at Section 1.2, p. 1-2. (emphasis added);
B. claims processing, meaning the PBM would adjudicate both provider
(pharmacy) point of sale ("POS") claims (a/k/a “real time claims”), which are
processed through SilverScript’s automated electronic on-line claims
adjudication system, as well as claims submitted directly to SilverScript by
plan participants on SilverScript’s standard claim form (a/k/a paper claims).
Defendants' PBM services also included the administration of mail order
prescriptions. The Caremark Defendants agreed to process both
electronic and paper claims in keeping with CMS standards as specified
in Section 3.17.A-5-10 of the Part D Application and the applicable State
or Federal Law. MCS-SilverScript PBM Agreement at Section 1.4.d., p. 4.
52
(emphasis added);
C. collect and report to CMS Claims data as specified in Section 3.13,
subsections 4 and 5 of the Part D Application, and such additional
information for purposes of reconciliation of risk factors, low income
subsidy payments, reinsurance payments, and risk corridor as required
by CMS as communicated by [MCS] to SilverScript, and via the Medicare
Data Communications Network ("MDCN"). SilverScript agreed to send MCS
copies of the reports submitted to CMS. MCS-SilverScript PBM Agreement
at Section 1.10.b., p. 12. (emphasis added); and
D. compliance with its [MCS Life’s] Fraud and Abuse Program which MCS
established to monitor Part D services “to the extent such program does
not conflict with SilverScript’s processes.” MCS-SilverScript PBM
Agreement at Section 1.16.c., p. 6 (emphasis added).
241. With regard to the submission of Part D claims data, SilverScript and MCS
expressly agreed that "SilverScript shall perform data edit and quality control procedures
designed to ensure accurate and complete prescription drug data." MCS-SilverScript PBM
Agreement at Section 1.10.a., p. 12 (emphasis added).
242. Pursuant to the MCS-SilverScript PBM Agreement, the Caremark Defendants
have significant financial incentives for adjudicating Part D claims and dispensing Part D drugs.
First, the Caremark Defendants received administrative (processing) fees of $0.20 per paid retail
or mail order claim (and $.80 per on-line claim). MCS-SilverScript PBM Agreement at p. 34
(emphasis added). The Caremark Defendants do not receive the processing fee where the claim
is rejected. These fees are significant in light of the fact that the Caremark Defendants’ PBMs
process hundreds of millions of prescriptions each year.
243. The Caremark Defendants were also incentivized to process (not reject) Part D
claims because, under the MCS-SilverScript PBM Agreement, they collected a dispensing fee of
$3.00 per retail prescription ($1.48 for mail order prescriptions) only if the prescription was
billed and “dispensed to the Part D participant through Caremark’s retail pharmacy network.”

53
MCS-SilverScript PBM Agreement at p. 34 (emphasis added). Again, the dispensing fee is
earned only for those prescriptions “dispensed.”
244. The Caremark Defendants had additional incentives through their Caremark and
CVS-owned mail order and retail pharmacies, because they earned additional funds paid to the
dispensing pharmacy (including drug costs and the pharmacy’s share of the dispensing fee).
None of these are paid unless the Part D claim is paid. Again, these incentives are significant in
light of the hundreds of millions of prescriptions dispensed through CVS Caremark pharmacies
each year.
245. According to the terms of the MCS-SilverScript PBM Agreement, the Medicare
Part D PBM services to be provided by Defendant’s subsidiary also included, at paragraph 1.8.a.,
Concurrent Drug Utilization Review (DUR) services for retail or point of sale (POS) claims.
246. According to the contract’s terms, when a claim was rejected by Caremark’s
system, but actually represented appropriate therapy in the judgment of the physician or
pharmacist, the pharmacist could either dispense the drug at the plan participant’s expense or call
[MCS Life] or Silver Script to override the denial edit.
247. However, under Caremark’s System, only those claims processing edits provided
by the PBM and selected by the Part D Plan as triggering a denial edit would require further
action by the pharmacist to either contact MCS or SilverScript to override the denial or to have
the plan participant obtain the prescription outside Part D at their own expense.
248. The language of the PBM Agreement regarding concurrent DUR services states
as follows:
A. clinical and quality of care issues detected by some DUR edits do not affect
the claim payment but result in transmission of a warning or alert message
transmitted at the time of dispensing to the pharmacist as part of the paid
claim response from SilverScript. Participating pharmacies are directed to
54
review the messages and to use their professional judgment as to whether
action is required. SilverScript also agreed to provide to MCS Life, as the
customer’s expense, a monthly report of concurrent DUR services rendered.
MCS-SilverScript Agreement at 1.8.a., p.7;
B. except as set forth in paragraph (b) [sic] above, in performing DUR Services,
SilverScript will not, and is not required by this Agreement to, deny any
claims or require physicians, pharmacist, or patient compliance with any norm
or suggested drug regimen, or in any way substitute SilverScript’s judgment
for the professional judgment or responsibility of the physician or pharmacist.
MCS-SilverScript Agreement at p. 7, paragraph 1.8.b.; and
C. SilverScript’s DUR services are highly automated ... and ... necessarily limited
by the amount, type and accuracy of Plan Participant information
made available to SilverScript ... SilverScript [has] no obligation to acquire
information concerning any Plan Participant beyond the information that is
included in SilverScript’s eligibility file or the Claims submitted by
Participating Pharmacies in connection with the Plan. MCS-SilverScript
Agreement, Section 1.18.b., p. 8.
249. The MCS-SilverScript PBM Agreement was in effect from January 1, 2006 until
January 1, 2008 when Catalyst Rx took over as PBM for MCS’s Medicare Part D Program.
250. From approximately January 1, 2006 through approximately January 2008, for
each of the MCS health Plans, MCS Life provided Part D coverage and the Caremark
Defendants’ subsidiary, SilverScript, provided PBM services. In other words, the Defendant
SilverScript provided Medicare Part D PBM services to MCS Life for health insurance plans
offered by MCS from January 1, 2006 until January 2008.
251. For each health insurance benefit Plan offered by MCS, MCS Life provided
Medicare Part D prescription drug coverage (MCS Life was the Part D Sponsor) and the
Caremark Defendants (through SilverScript, the Part D PBM) provided PBM services according
to the terms and conditions of the PBM Agreement that operated in conjunction for each of MCS
plans with either a 2006 Medicare Part D Client Plan Design Document or a 2007 New Business
form.

55
252. The MCS-SilverScript PBM Agreement required that SilverScript adhere to all
requirements of the Medicare Part D Program, both those contained in CMS’s Laws and
Regulations, as well as those contained in the contract between the Sponsor, MCS and CMS.
253. From January 1, 2006 until approximately January 2008, these Medicare Part D
PBM services described above were provided by Defendant Caremark Rx and its subsidiaries.
Following the March 22, 2007 CVS-Caremark merger, these PBM services were performed by
Defendant CVS Caremark through its subsidiaries.
B. The Part D Audit by Pharm/DUR Inc. Reveals that the Caremark
Defendants Unlawfully and Intentionally Failed to Comply with the
Fundamental Requirements of the Medicare Part D Program
1. The Audit
254. In early 2007, MCS retained Relator’s company, Pharm/DUR Inc.
("Pharm/DUR"), to conduct an audit of all the Medicare Part D retail and mail order
pharmacy claims paid by MCS for MCS Life's Part D participants from January 1 through
December 31, 2006.
255. Pharm/DUR’s audit was supposed to include desk audits of both retail and mail
order pharmacies and (field) on-site audits as needed so as to be as comprehensive as possible.
256. The Pharm/DUR desk audit program was utilized in instances where the Part D
data analysis system identified a specific submission or data trend that was fraudulent or abusive,
or where the claim volume of a specific pharmacy was not sufficient to be included for an on-site
audit. After using pre-determined edits to identify the pharmacies and specific claims for desk
review, Pharm/DUR made written requests directly to selected pharmacies for documentation of
specific components of the Part D claims as a basis for extended or investigational audits.
257. In February 2007, Pharm/DUR informed the Caremark Defendants that MCS had
56
retained Pharm/DUR to conduct its audit. At the same time, Pharm/DUR obtained from the
Caremark Defendants the paid Part D claims data for the MCS Life Part D participants.
258. The PDE data elements themselves are collected and initially generated by the
dispensing entity (retail or mail order pharmacy) to the PBM, which then submits the data in
PDE report format to CMS. The claims data provided by Defendant Caremark to Pharm/DUR,
whether the raw data initially provided to the Caremark Defendants, or the PDE report submitted
by the Caremark Defendants to CMS, is identical for each affected field.
259. The MCS-SilverScript PBM Agreement specifically required Caremark to submit
to CMS, on behalf of MCS, data reflecting Part D claims paid by MCS. Thus, all paid claims
data Caremark provided to Pharm/DUR was presented by Defendants to CMS for payment under
Part D.
260. The pharmacies in the CVS Caremark network serving MCS members were
throughout the United States and Puerto Rico. For example, the CVS Caremark Defendants
adjudicated claims for Part D prescriptions for MCS beneficiaries that originated from CVS
Caremark’s mail order facilities located in Miramar, Florida and Mt. Prospect, Illinois, as well as
from CVS and other retail pharmacies across the United States, including in Pennsylvania.
261. Pharm/DUR conducted an analysis of all Part D paid claims data for both retail
and mail order pharmacy prescriptions submitted by pharmacies to be adjudicated by Defendant
Caremark/Silverscript from January 1, 2006 through December 31, 2006.
262. Following the Part D paid claims data analysis, the next step in the Pharm/DUR
audit process was to perform on-site and desk audits of retail pharmacies and on-site audits of
mail order pharmacies.
263. Pharm/DUR’s on-site audits involved auditors visiting the pharmacies to obtain

57
copies of documents purportedly supporting the claims information submitted by the pharmacies
and processed by the PBM for specific prescriptions in the review claims dataset. The on-site
auditor would compare the original hard copy of the prescriptions with the information submitted
for payment.
264. Pharm/DUR sent notices to the Caremark network retail pharmacies selected for
desk and/or on-site audits. Thereafter, on August 23, 2007, the Caremark Defendants sent a
facsimile on Caremark letterhead to the pharmacies serving MCS members directing them not to
cooperate with Pharm/DUR’s Part D audit. The facsimile read:
Attention
Pharmacies serving MCS members
You may have received information from Pharm/DUR Inc.
regarding an audit on behalf of MCS concerning MCS’s MAPD
business. Please, DO NOT release any information to this
company or to MCS. Pharm/DUR does not have the right or
privilege to contact any pharmacy on behalf of MCS, and therefore
should not receive any claims, pricing, personal health
information, or any confidential proprietary information from you
concerning MCS. [The fax bore an image of a MCS Life Insurance
Company identification card.] (Below the image of the MCS
identification card, the fax continued.) If you have any questions
or concerns, please contact Mildred Muniz at 787-287-2201.
Thank you for participating in Caremark pharmacy networks.
265. This intentional disruption by the CVS Caremark Defendants of the Part D audit
process conducted on behalf of MCS, the CVS Caremark affiliated Part D Sponsor, directly
conflicts with what the CVS Caremark Defendants described in their Part D Compliance/Fraud,
Waste & Abuse training manual as network pharmacies’ “responsibilities” to cooperate with Part
D audits by CVS Caremark, its subsidiaries, or “affiliates.”
266. Due to a series of obstructive actions of the Caremark Defendants, Pharm/DUR
was unable to fully complete the desk or the on-site audits of many of the MCS retail

58
pharmacies, or to conduct the audits of the mail order facilities as requested by MCS, the Part D
Sponsor.
2. Pharm/DUR’s Audit Findings
267. Pharm/DUR communicated the results of its audit analysis of paid claims data
from MCS’s retail and mail order pharmacies (CVS Network Providers) to both MCS and to the
Caremark Defendants through a series of communications, which culminated in Pharm/DUR
issuing a December 2007 report.
268. Pharm/DUR’s December 2007 report documented the six areas where
Pharm/DUR concluded that the Defendants had illegally and fraudulently adjudicated, paid, and
submitted to CMS claims for Medicare Part D drugs. These six areas and the findings for each
category were in sum:
1) Gender Specific Deviations: fraudulently dispensing of gender-specific drugs:
507 claims, causing improper payments by MCS and reported to CMS totaling $53,608;
2) MAC Pricing: fraudulently failing to apply Maximum Allowable Cost
(“MAC”) pricing to all of the MAC drugs: 3,658 claims causing improperly paid by MCS and
reported by MCS to CMS totaling $105,141.80;
3) Expired Drugs: fraudulent payment for expired drugs (with an outdated NDC)
on 11,286 claims causing improperly paid claims by MCS and reported to CMS by Defendant
Caremark totaling $399,794;
4) False Prescriber Identifiers: fraudulent payment for claims where Defendant
Caremark as the PBM adjudicated claims even though its network pharmacies failed to report
accurate physician identifiers, and instead used "push" numbers on 15,903 claims causing
improper payments by MCS and Part D claims reported to CMS totaling $673,494.58;

59
5) No Prior Authorization: Caremark fraudulently adjudicated claims where drugs
were dispensed and claims were paid without prior authorization:
Tier 2 drugs: 633 claims improperly paid by MCS and reported by Caremark to
CMS totaling $45,951.77;
Tier 4 drugs: 14,840 claims improperly paid by MCS and reported by Caremark
to CMS totaling $2,796,346.32;
6) Over Limits: Caremark fraudulently adjudicated claims processed for
quantities of drugs or days supply over the approved limit on 1,875 improper claims paid by
MCS and reported by Caremark to CMS totaling $209,209.66.
269. Pharm/DUR's conclusions were based upon the Part D claims data analysis of
mail order and retail pharmacies as well as desk audits of some of the retail pharmacies. Based
upon an analysis of Part D claims paid data, Pharm/DUR identified 48,702 Medicare Part D
claims which Defendant Caremark had adjudicated and fraudulently paid, with a total cost of
$4,283,546.13 to MCS, all of which were submitted to CMS for payment.
C. Defendants Have Illegally Submitted False Medicare Part D PDE Claims
Data to CMS Resulting in False Part D Payments to MCS and/or MCS Life_
270. In their Medicare Part D Compliance/Fraud, Waste & Abuse training manual for
pharmacies, CVS Caremark itself recognized accurately that the False Claims Act “makes it
illegal for anyone to knowingly file, or make someone else file, a false claim for payment with
the Federal government. This includes submitting wrong or fraudulent claims for
prescription drugs dispensed to beneficiaries in a Federal government program such as
Medicare Part D.” (Emphasis in the original.) In that same document, Defendant CVS
Caremark also emphasized the importance of understanding that Part D Plans will be sanctioned
for “providing false information to CMS.”

60
1. False Prescriber Identifiers (DEA Numbers)
271. Pharm/DUR’s analysis demonstrated that the Caremark Defendants fraudulently
paid claims where fictitious physician identifiers (including “Physician Push Numbers" or other
obviously incorrect numbers) were used to populate PDE Fields 12 and 13 to adjudicate the Part
D claim.
272. Physician “push” numbers are fictitious physician identifiers created by inserting
a random alpha-numeric data of the appropriate number of characters where PDE data element
No. 13 belonged on the electronic PDE record. The most commonly used "push number" or
false physician identifier used was "AA00000000," which Defendant Caremark fraudulently,
knowingly and recklessly permitted to occupy Field 13 on 4,360 claims involving 993 members.
273. The creation of these false physician identifier numbers also caused PDE claims,
particularly Field No. 12, the “Prescriber ID Qualifier,” which describes the type of identifier
(for example, DEA number or state license number), to contain false data.
274. The Caremark Defendants adjudicated 15,903 claims using obviously fictitious
physician identifiers - - just during the time period covered by the audit. The Caremark
Defendants submitted or caused to be submitted to CMS at least 31,806 false PDE data items (2
data items, Fields 12 and 13, associated with each false prescriber) in the PDE data records for
the affected Part D claims in a fraudulent attempt to obtain payment from CMS. Attached as
Exhibit “C” is a table containing representative Part D claims adjudicated by the Defendants
using obviously fictitious physician identifiers.
275. None of these claims involved paper or non-standard claims which would have
permitted the use of a default DEA identifier.
276. Significantly, of the claims involving physician push numbers, many originated at

61
Defendant CVS Caremark's own facilities. For example, Caremark Miramar Pharmacy, LLC, a
mail order pharmacy located in Miramar, Florida, was the source of at least 330 claims (and
likely thousands more) with physician push numbers involving total payments of $43,152.52.
These claims accounted for nearly 15% of prescriptions processed and 16% of the total dollars
paid for all claims processed by the Caremark Miramar Pharmacy for the Pharm/DUR audit
period. Moreover, Caremark’s Miramar, Florida facility processes Part D claims for many Part
D Plans in addition to MCS.
277. Thus, because Caremark utilized the same process for adjudicating claims and
submitting them for payment, the Miramar facility alone was the site for tens of thousands of
additional false Part D claims across other Part D Plans.
278. In addition, Defendant CVS Caremark’s mail order facility in Mt. Prospect,
Illinois and its retail pharmacies in Allentown, Bethlehem, and Lebanon, Pennsylvania also
fraudulently processed prescriptions with invalid prescribed identifiers in the same manner as
described above.
a. The Caremark Defendants Fraudulently Do Not Edit for
Unidentified Prescribers
279. Pharm/DUR communicated to the Caremark Defendants that “the processing of
claims with fictitious physician identifiers “make[s] it impossible to identify terminated or un-
licensed [sic] physicians as mandated by CMS Fraud, Waste and Abuse Guidelines.”
280. The Caremark Defendants admitted that “An edit to reject claims for unidentified
prescribers is not a system edit that Caremark provides its customers.” Thus, incredibly, the
Caremark Defendants essentially conceded that it had been engaging in systemic Part D fraud
across all of its plans nationwide in connection with its submission of PDE data.
281. Caremark/SilverScript was required to ensure that an edit to reject claims for

62
unidentified prescribers was in place. Federal Regulations both mandate that the Part D Sponsor
and First Tier Entities (here, Caremark/SilverScript) submit accurate PDE Data, and prohibit
Part D Sponsors from paying claims for prescriptions by excluded or unlicensed providers.
Excluded providers can only be identified by through accurate physician data.
282. In addition, Part D Sponsors and First Tier Entities (here, Caremark/SilverScript)
are responsible for compliance with all State pharmacy laws. Both Federal Regulations and the
Caremark Defendant's PBM Agreement obligates them to adhere to all Federal and State
standards.
283. CVS Caremark fraudulently failed to ensure that Part D prescriptions were
processed in keeping with minimum requirements of State pharmacy codes, all of which require
a licensed prescriber to issue a prescription.
b. Invalid Prescriber Date Undermines Appropriateness of Part
D Claim
284. The Caremark Defendants stated, in their response to Pharm/DUR's findings, that
their nationwide claims adjudication system does not deny Part D claims which even when they
contain false and fraudulent physician identifiers. Thus, the Caremark Defendants have conceded
that, in all of their Part D PBM contracts (their total pharmacy services involved a billion
prescriptions in 2007), they do not: 1) deny claims containing false physician identifiers; and 2)
have a system to identify false prescriber identifiers. In sum, the Caremark Defendants
intentionally have no way to determine whether a billion or more prescriptions with false
physician identifiers involve drugs prescribed by an excluded or unlicensed provider.
285. The Caremark Defendants’ Part D PBM services have failed to fulfill the Part D
Sponsor’s absolute duty under the Part D Regulations to submit only claims with accurate
prescriber data and to deny claims for drugs prescribed by excluded or unlicensed providers.

63
286. The Caremark Defendants intentionally and fraudulently did not make any effort
to ensure that claims submitted for payment to CMS even included a properly identified
prescriber. Accordingly, the Caremark Defendants intentionally and fraudulently made no effort
to determine that either the prescriber was licensed or that the prescriber was on a list of
excluded prescribers. Thus, the Caremark Defendants could not, and did not, truthfully certify
that the PDE data was accurate and complete.
287. With regard to just the MCS contract alone, during the period audited by
Pharm/DUR, the Caremark Defendants fraudulently adjudicated nearly 16,000 claims with false
physician identifiers, causing improper payments by MCS and reported to CMS totaling
$673,494.58.
288. CVS Caremark utilizes a nationwide claims adjudication system and has admitted
that they intentionally make no effort to ensure that prescribers are identified or to deny claims
for excluded or unlicensed providers, the total damage to the Federal Government from this
knowing and intentional Part D fraud is extraordinarily significant. This is particularly true
when considered in light of the fact that Caremark has been adjudicating and submitting Part D
claims for thousands of other Plans, including Federal Government Plans.
2. Gender-Specific Deviations
289. Pharm/DUR found that the Caremark Defendants adjudicated Part D claims
without editing for gender-specific deviations (that is, drugs used exclusively in males but
prescribed for females and vice versa). With regard to the MCS contract alone, the Caremark
Defendants fraudulently adjudicated 507 claims with gender-specific deviations, resulting in the
submission by Caremark to CMS of false and fraudulent Part D claims totaling $53,608.
Attached as Exhibit “C” is a table containing representative Part D claims adjudicated by the
64
Defendants without editing for gender-specific.
290. In response to these findings, Caremark admitted that its nationwide system does
not even reject claims for drug/gender deviations.
291. The CVS Caremark Defendants were knowingly and intentionally reckless as to
the accuracy of gender data they submitted to CMS in Field 7 of the Part D PDE claim data.
292. Federal Part D Regulations require that a Part D Sponsor conduct a Concurrent
DUR for age and gender contraindications. 42 C.F.R. § 423.153 (c)(2)(ii).
293. Although the Caremark Defendants were contractually bound to follow CMS’s
statutory, regulatory and contractual mandates, Caremark intentionally and fraudulently failed to
conduct a Concurrent DUR on their Part D claims for gender contraindications.
294. The Caremark Defendants have admitted that their nationwide system is
intentionally designed not to conduct concurrent DUR for gender contraindications (will not
deny claims based on drug-sex edits). The total damage to the Federal government from this
knowing and intentional Part D fraud is extraordinarily significant, particularly when considered
in light of the fact that Caremark has been adjudicating and submitting Part D claims for
thousands of other Plans, including Federal Government Plans.
3. Drugs with Expired or Obsolete NDCs
295. Pharm/DUR further concluded that the Caremark Defendants paid Medicare Part
D claims for drugs with NDC numbers that were “outdated, stale and/or obsolete ... and that [t]he
payment of these claims should be rejected ... payment of these claims leaves the client
potentially at risk of legal action should a patient have a serious adverse reaction.”
296. With respect to the SilverScript/MCS Agreement, the drugs for which the
Defendants fraudulently approved and submitted Part D claims to CMS for payment where the
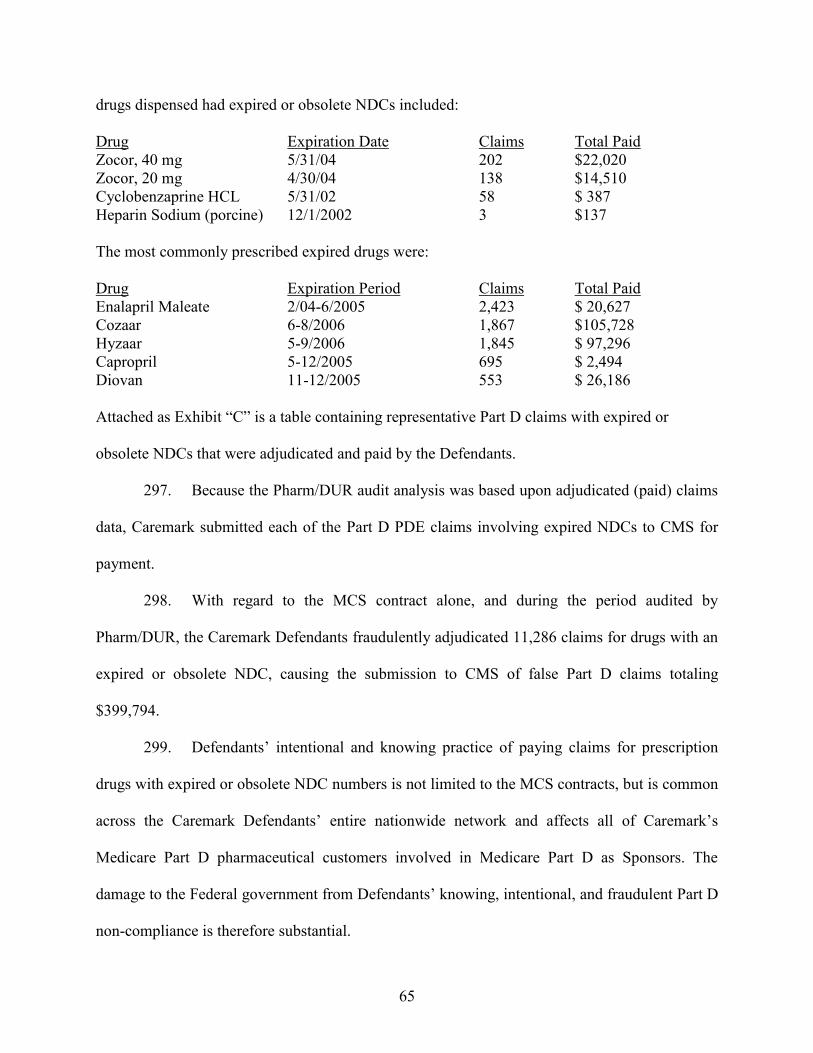
65
drugs dispensed had expired or obsolete NDCs included:
Drug Expiration Date Claims Total Paid
Zocor, 40 mg 5/31/04 202 $22,020
Zocor, 20 mg 4/30/04 138 $14,510
Cyclobenzaprine HCL 5/31/02 58 $ 387
Heparin Sodium (porcine) 12/1/2002 3 $137
The most commonly prescribed expired drugs were:
Drug Expiration Period Claims Total Paid
Enalapril Maleate 2/04-6/2005 2,423 $ 20,627
Cozaar 6-8/2006 1,867 $105,728
Hyzaar 5-9/2006 1,845 $ 97,296
Capropril 5-12/2005 695 $ 2,494
Diovan 11-12/2005 553 $ 26,186
Attached as Exhibit “C” is a table containing representative Part D claims with expired or
obsolete NDCs that were adjudicated and paid by the Defendants.
297. Because the Pharm/DUR audit analysis was based upon adjudicated (paid) claims
data, Caremark submitted each of the Part D PDE claims involving expired NDCs to CMS for
payment.
298. With regard to the MCS contract alone, and during the period audited by
Pharm/DUR, the Caremark Defendants fraudulently adjudicated 11,286 claims for drugs with an
expired or obsolete NDC, causing the submission to CMS of false Part D claims totaling
$399,794.
299. Defendants’ intentional and knowing practice of paying claims for prescription
drugs with expired or obsolete NDC numbers is not limited to the MCS contracts, but is common
across the Caremark Defendants’ entire nationwide network and affects all of Caremark’s
Medicare Part D pharmaceutical customers involved in Medicare Part D as Sponsors. The
damage to the Federal government from Defendants’ knowing, intentional, and fraudulent Part D
non-compliance is therefore substantial.

66
4. No Prior Authorization
300. Pursuant to Section 1860D of the Social Security Act, CMS only pays for Part D
drugs approved for coverage under the Sponsor’s specific Plan. According to 42 C.F.R. §
423.100, covered Part D drugs include only those Part D drugs included in the Plan's formulary.
The Plan’s formulary includes the designation of certain drugs provided on a preferred or tiered
cost-sharing status. In addition, the CVS Caremark PBM was required to conduct concurrent
DUR for over-utilization 42 C.F.R. § 423.153(c)(2).
301. Pharm/DUR obtained the MCS formularies at issue, which required prior
authorization before dispensing certain Tier 2 and Tier 4 drugs.
302. Pharm/DUR’s analysis of the MCS/Caremark paid claims data led to the
conclusion that the Caremark Defendants illegally and fraudulently permitted participating
pharmacies to dispense drugs, without required Part D formulary prior authorizations, and
illegally paid these claims. Pharm/DUR found that the Tier 2 and Tier 4 drugs involved “were
listed on the MCS formularies as requiring an authorization.” Attached as Exhibit “C” is a table
containing representative Part D claims for Tier 2 and Tier 4 drugs that were adjudicated and
submitted without required prior authorization.
303. The Caremark Defendants fraudulently adjudicated and paid 633 Part D claims
totaling $45,951.77 for Tier 2 drugs without required authorizations causing improper Part D
claims to be paid by MCS and false and fraudulent Part D PDE data to be submitted by
Caremark to CMS. In addition, the Caremark Defendants’ knowing and intentional fraudulent
refusal to require prior authorization before dispensing Tier 4 drugs involved another 14,840
claims inappropriately adjudicated by the CVS Caremark Defendants, paid by MCS, and falsely
reported by CVS Caremark as valid Part D claims. These false and fraudulent Tier 4 claims

67
totaled $2,796,346.32.
304. Defendants' intentional and fraudulent failure to require prior authorizations
before dispensing the Tier 2 and Tier 4 drugs caused over-utilization which affected both MCS's
bid and CMS’s payments to MCS (for both subsidy payments and reconciliations). Claims for
Part D prescriptions which required prior authorizations, but did not go through the authorization
process, were falsely and fraudulently included in the Defendants' data submissions to CMS.
305. Drugs dispensed fraudulently or illegally as Part D benefits can put enrollees into
or out of “donut hole,” thereby affecting both the enrollee’s co-pay and (once catastrophic limit
reached) the Sponsor's and the government’s obligation to provide catastrophic coverage for the
entire prescription. The Caremark Defendants fraudulently submitted these inappropriate Part D
claims and associated costs to CMS. MCS, as the Part D Sponsor, received inflated capitation
payments and reconciliations based upon these invalid Part D costs.
5. Drugs Dispensed Over Approved Limit
306. Pharm/DUR’s analysis of Part D paid claims data also led to the conclusion that
the Caremark Defendants fraudulently processed 1,875 claims for quantities of drugs or days
supply over the approved limit. Pharm/DUR initially identified over-limit dispensing affecting
both Tier 2 and Tier 4 drugs, based upon listed quantities and/or days supply in the
Tier 2 and Tier 4 formularies. However, after removing any drugs where the correct quantity was
dispensed, regardless of the supply that had been processed (per MCS approval), and following
the related removal of claims for Tier 2 drugs, there were still 1,875 claims for Tier 4 drugs
fraudulently dispensed over the limit approved by MCS or exceeding the maximum dose as
listed by the manufacturers.
307. Exceeding the maximum dose poses an obvious risk to Patient Safety.

68
308. Caremark was required to conduct concurrent DUR for over-utilization. 42
C.F.R. § 423.153(c)(2). Caremark’s inappropriate adjudication of Part D claims for over-limit
Part D drugs caused MCS to make improper payments and Caremark's false submission to CMS
of improper Part D claims totaling $209,209.66. Attached as Exhibit “C” is a table containing
representative Part D claims that were adjudicated and submitted to CMS which contain
quantities over the approved limits.
309. Neither MCS as the Plan Sponsor, nor the Caremark Defendants as a PBM (first
tier entity), submitted corrected PDE data or otherwise notified CMS of these claims for Tier 4
drugs dispensed for quantities over the approved limit.
310. Caremark's adjudication of Part D prescription claims over approved limits
caused over-utilization which affected both the MCS bid and Part D payments by CMS.
311. Over-utilization of Part D drugs resulting from lack of prior authorization and
dispensing over approved limits has a substantial impact for an individual Part D enrollee, but
more importantly for the entire pool of Part D participants.
312. Inappropriately dispensed drugs can put enrollees into or out of a donut hole.
These improperly adjudicated claims affect both the enrollee’s co-pay and, once catastrophic
limit reached, the Part D Plan Sponsor's obligation to provide coverage for the entire prescription
cost.
313. On the MCS Plan alone, over-utilization caused CMS to improperly cover more
than $3 million in Part D claims where drugs were fraudulently dispensed without a prior
authorization or in quantities exceeding approved limits.

69
314. As the Part D Sponsor's costs are reported to CMS in the Part D PDE data and
other cost submissions, over-utilization inflates in subsequent years the payments CMS made to
the Part D Sponsors, including capitation payments.
6. Improper MAC Pricing
315. "Maximum Allowable Cost" ("MAC") pricing means the unit price established by
Defendant SilverScript for a generic drug included in Defendant SilverScript's MAC list.
According to the terms of the MCS-SilverScript PBM Agreement, SilverScript was obligated to
provide the MAC list to MCS. See MCS-SilverScript PBM Agreement at p. 28.
316. Pharm/DUR found that SilverScript fraudulently failed to apply MAC pricing to
all of the MAC drugs (3,658 claims/ $105,141.80 total).
317. With regard to the MCS contract alone, during the time period audited by
Pharm/DUR, the Caremark Defendants fraudulently adjudicated 3,658 claims with pricing which
deviated from the MAC pricing provided on the Caremark Defendants’ MAC list, causing
improper Part D payments by MCS and improper submission of Part D claims to CMS totaling
$105,141.80. Attached as Exhibit “C” is a table containing representative Part D claims
adjudicated by the Defendants and submitted to CMS where the pricing deviated from the
Defendants’ MAC list.
318. The Caremark Defendants' intentional and fraudulent failure to apply MAC
pricing alone caused both the Part D beneficiary to pay a higher co-pay and the Plan to report
higher Part D costs to CMS.
D. Defendants Failed to Perform Appropriate Concurrent Drug Utilization
Reviews
319. The Caremark Defendants nationwide Part D claims adjudication system failed to
have the required concurrent DUR, including gender contraindications and review for over-

70
utilization. The Part D customers of the Caremark Defendants, which include hundreds of PDPs
and MA-PDs throughout the United States, including MCS and MCS Life, were thus illegally
permitted to illegally reject the performance of drug-to-sex edits at point of sale or point of
distribution (when the concurrent DUR was to be conducted).
320. In all instances where the Caremark Defendants failed to conduct drug-to-sex
edits, either because they permitted their Part D Sponsor customers, including MCS and MCS
Life, to illegally reject the performance of drug-to-sex edits as part of the concurrent DUR at the
point of sale or point of distribution, or because the PDP Sponsor failed to perform a review of
the prescribed drug therapy for gender-related contraindications “before the prescription was
dispensed to an enrollee in a Sponsor's Part D Plan, ” they failed to perform concurrent DUR, as
required by 42 C.F.R. § 423.153 (c)(2)(ii).
321. PDP Sponsors are not entitled to receive Medicare Part D payment for
claims based on drugs dispensed without appropriate concurrent DURs, including for
gender-related contraindications and over-utilization.
322. From January 1, 2006 to December 31, 2006, the Caremark Defendants
fraudulently adjudicated 507 claims on behalf of MCS where there were gender-specific
deviations, causing improper payments by MCS and reported to CMS totaling $53,608.
Attached as Exhibit “C” is a table containing representative Part D claims adjudicated and
submitted to CMS where the Defendants failed to perform concurrent DUR.
E. The CVS Caremark Defendants Thwarted MCS’s Ability to Have in Place a
Plan to Detect, Correct, and Prevent Part D Fraud, Waste and Abuse
323. During the time period relevant to this Complaint, the Caremark Defendants
regularly and knowingly submitted false or fraudulent PDE data items to CMS. Upon
information and belief, the CVS Caremark Defendants continue to submit false or fraudulent
71
PDE data to CMS in the very same manner as described herein.
324. In addition, as described above, the CVS Caremark Defendants intentionally and
fraudulently thwarted the Sponsor’s (MCS’s) efforts to conduct an appropriate Part D fraud,
waste, and abuse program as required by 42 C.F.R. § 505(h)(1).
325. Because CVS Caremark Defendants’ efforts to submit false or fraudulent PDE
data items were designed to generate claims for prescription drugs in situations in which the
prescribing physician could not be identified, or the drugs dispensed had expired NDC codes, or
the Defendants intentionally failed to conduct appropriate concurrent DUR for drug-to-sex edits
or for over-utilization, the Defendants were unable to establish that the drugs dispensed were
medically necessary for treatment of patients’ specific medical conditions. In addition, the CVS
Caremark Defendants interfered with MCS’s efforts, through Pharm/DUR, to complete a Part D
audit.
326. The Caremark Defendants’ customers should not have submitted Part D claims
data to CMS related to Part D drugs dispensed as a result of the Caremark Defendants’
intentional company-wide failure to perform the Part D claims adjudication process as required
for compliance with Medicare Part D program requirements.
327. The Caremark Defendants’ efforts to interfere with MCS’s Part D fraud, waste
and abuse program resulted in MCS neither reporting the overpayment to CMS nor returning any
overpaid funds to CMS.
F. Defendants Caused CMS to Make Inflated Part D Subsidy
Payments to MCS Life
328. The paid claims data provided by the Caremark Defendants to Pharm/DUR
represents the value of Part D claims adjudicated and reported to CMS between January 1, 2006
and December 31, 2006.

72
329. Each of the fraudulently adjudicated Part D claims identified in the Pharm/DUR
report represented a Part D prescription drug event adjudicated by the Caremark Defendants' and
a PDE claim submitted to CMS for coverage under the Medicare Part D Program by Defendant
Caremark, as the PBM for MCS.
330. MCS Life and/or the Caremark Defendants included in submissions to CMS
(other than the PDE data records i.e., the Sponsor’s costs of providing Part D coverage), the costs
related to each of the inappropriately paid Part D claims identified as a result of the Pharm/DUR
audit and/or included in the Pharm/DUR December 2007 report.
331. The Pharm/DUR audit report was based on the Caremark Defendants' claims paid
data for retail and mail order pharmacies. The Pharm/DUR analysis of the retail pharmacy
claims data also included some desk audits and on-site audits. Pharm/DUR's analysis revealed
that the Caremark Defendants fraudulently submitted (on behalf of MCS) $4,283,546.13 in costs
for Part D drugs which should not have been either covered under Medicare Part D or submitted
to CMS.
332. PDE data includes, at Fields 27 (Ingredient Cost Paid), 28 (Dispensing Fee Paid),
and 29 (Sales Tax), the costs incurred by the Part D Sponsor for each Part D prescription drug
claim paid by the Part D Plan (including MA-PDs), here, MCS.
333. CMS makes payments to Part D Plan Sponsors based on PDE data submitted by
or on behalf of the Part D Sponsor. Here the Part D PDE data was submitted by the Caremark
Defendants on behalf of MCS.
334. The PDE data fraudulently submitted by the CVS Caremark Defendants on behalf
of MCS, together with other information required by CMS, was an express condition of payment
of Part D benefits by CMS. Each fraudulent Part D PDE claim submitted by the CVS Caremark

73
Defendants on behalf of MCS beneficiaries contained the CVS Caremark Defendants’ express
certification to CMS of “the accuracy, completeness, and truthfulness of that data;” and the CVS
Caremark Defendants’ acknowledgment “that the data will be used for purposes of obtaining
Federal reimbursement.”
335. The payments made to MCS by CMS reflect that more than $4 million in Part D
claims which should not have been submitted to CMS. By virtue of these false claims, MCS
illegally received an overpayment.
336. The Caremark Defendants fraudulently adjudicated and submitted these claims on
behalf of MCS. The Caremark Defendants also illegally interfered with MCS’s efforts to
conduct an effective fraud, waste, and abuse program related to Part D Plans.
337. The Caremark Defendants fraudulently submitted or caused the submission of
Part D claims data (PDE data) and other required payment data on behalf of MCS from January
1, 2006 and until 2008 to CMS, which included costs related to Part D prescription claims where
the Defendants intentionally failed to adhere to Federal laws and Regulations, state pharmacy
codes, CMS instructions, and/or contractual obligations to which the Government required
compliance in order to make payments under the Medicare Part D program.
338. As a result of Defendants’ intentional and fraudulent conduct, CMS has made
payments (including monthly subsidies, risk adjustments, etc.) to MCS which take into account
these false or fraudulent Part D claims and their related costs.
G. Defendants Have Illegally Caused CMS to Make Inflated Medicare Part D
Subsidy Payments to CVS Caremark’s Customers Other than MCS Life
1. Caremark's System-Wide Part D Claims Processing Failures
339. Caremark (now CVS Caremark) uniformly and systemically analyses, processes
and documents all prescriptions managed by CVS Caremark using CVS Caremark’s nationwide

74
proprietary prescription management system.
340. CVS Caremark has admitted that its nationwide system does not conduct gender
edits, check for false physician identifiers, or reject claims with expired NDCs.
341. The following Part D claims processing failures detected by Pharm/DUR involve
company-wide or system-wide non-compliance with Part D requirements by the Caremark
Defendants: fraudulent failure to conduct gender edits as part of Concurrent DUR and the
adjudication of claims containing gender deviations; fraudulent failure to reject claims for false
physician identifiers and submission of physician push numbers; the fraudulent failure to exclude
expired drugs and the adjudication claims with expired NDCs for three years past the inactive
dates.
342. These intentional company-wide Part D claims adjudication failures involve false
claims submissions to CMS and increased payments in terms of monthly Part D subsidies and
other payments, and to the CVS Caremark Defendants’ customers nationwide who participate in
the Part D program. This includes, but is not limited to, the Part D Plans operated by CVS
Caremark subsidiaries, as well as non-CVS Caremark based Part D Plans.
343. The resulting damages to the Federal government are significant and continuing.
H. CMS Improperly Paid Part D Retiree Drug Subsidies
1. Improper Part D Retiree Drug Subsidies to Employer Plans Offered
by MCS ______
344. At times relevant to this Complaint, MCS also offered, in addition to its Plans
offering standard Medicare Part D benefits, at least 10 employer Plans providing prescription
coverage to their retirees.
345. As MCS provides health plans to more than 1,000 companies and covers over
150,000 employees and family members, MCS has applied for Part D Retiree Drug Subsidies

75
("RDS") with regard to those employer plans which offer prescription drug benefits similar to
Part D Plans to Medicare-eligible retirees.
346. The claims by MCS for these RDS benefits were plagued by the CVS Caremark
Defendants' intentional system-wide claims adjudication fraud and non-compliance with state
and Federal laws and Regulations described above with regard to the traditional Part D program.
Therefore, any claims for RDS payments made by MCS health plans based upon prescription
claims which failed to adhere to applicable Part D requirements led to illegal and unwarranted
Part D RDS payments to MCS health plans by CMS.
2. CMS Has Improperly Paid Part D Retiree Drug Subsidies to
Defendant CVS Caremark's Other Customers
347. Defendant CVS Caremark’s nationwide claims adjudication practices, as
described above, directly resulted in company-wide non-conformance with Federal statutes,
Regulations, and CMS instructions regarding the Medicare Part D Program.
348. Defendant CVS Caremark administers claims for other Part D customers
nationwide and has processed claims which were included in the costs reported by its other
customers with employer Plans in support of requests to CMS for RDS.
349. Defendant Caremark’s largest customer during the year ending December 2007
was the Federal Employee Health Benefits Program, whose FEHBP qualifies as a group health
plan eligible for RDS subsidies. 42 C.F.R. § 423.884; 42 C.F.R. § 423.882.
350. Defendant CVS Caremark had other customers, including FEHBP, who submitted
requests to CMS for Part D RDS payments.
351. Therefore, any claims submitted by Defendant Caremark’s other customers’
health plans, including FEHBP, which included prescription drug claims which failed to adhere
to Part D requirements (particularly those lacking physician identifiers, those where expired or

76
obsolete drugs were dispensed, and Part D drugs dispensed without required concurrent DUR,
including gender edits) caused illegal and unwarranted Medicare Part D RDS payments by CMS
to these Plans.
COUNT I
Violations of the Federal False Claims Act
31 U.S.C. § 3729(a)(1)(A), (2) and (3) and (7)
352. Relator realleges and incorporates by reference the allegations contained in
paragraphs 1 through 351 of this Complaint.
353. This is a claim for treble damages and penalties under the False Claims Act,
31 U.S.C. § 3729, et seq., as amended.
354. As a prerequisite to participating in Federally-funded health care programs,
including Medicare Part D, Defendants expressly certified (or, through their participation in a
Federally funded program, impliedly certified) their compliance with applicable statutes
and regulations.
355. The above-described Part D claims of MCS and/or MCS Life that included false
PDE data submitted by the Caremark Defendants to CMS were not eligible for reimbursement
from Medicare Part D because complete, accurate, and true PDE submissions were an express
condition of payment under the Medicare Part D statute and applicable regulations.
356. During the time period relevant to this Complaint, the Part D claims submitted by
the CVS Caremark Defendants and/or MCS did not qualify for reimbursement under any of the
various Federal health care programs because the CVS Caremark Defendants intentionally and
fraudulently failed to adhere to Part D requirements by adjudicating prescription claims, failed to
perform concurrent DURs, and reporting false Part D claims data to CMS as more fully
described above.

77
357. The CVS Caremark Defendants also fraudulently induced CMS to contract with
them as a Part D Plan and/or as a Part D PBM knowing that they could not comply with Federal
Part D requirements that their PDE data be accurate, complete, and true. The CVS Caremark
Defendants’ nationwide claims adjudication process intentionally contained no edits to detect
invalid physician identifiers, or drugs with expired or obsolete NDCs. The CVS Caremark
Defendants also intentionally and fraudulently failed to ensure that their nationwide claims
adjudication system conducted required concurrent DUR (including gender contraindications), or
prevented the submission of claims without prior authorization in keeping with the Part D
Sponsor’s Plan and formulary.
358. Based upon the paid claims data of the Medicare Part D prescriptions adjudicated
by the CVS Caremark Defendants for MCS and obtained by Pharm/DUR Inc., the CVS
Caremark Defendants improperly adjudicated claims which did not qualify for reimbursement
under any of the various Federal health care programs, including Medicare Part D, because there
was no approval or support for such drugs to be eligible for reimbursement and/or because
Defendants’ unlawful activity created overutilization of such drugs in situations where they were
not medically necessary for treatment of patients’ specific medical conditions.
359. Defendants' unlawful practices caused false claims for Medicare Part D benefits
to be submitted to CMS which affected both the benefits of the individual Part D member and,
the payments made by CMS, including calculation of periodic Part D reconciliations and future
capitation payments CMS paid or would be paying to the Part D Sponsors involved, including
MCS.
360. By virtue of the acts described above, Defendants knowingly presented or caused
to be presented, false or fraudulent claims to the United States Government for payment

78
or approval.
361. Defendants violated the Federal False Claims Act by submitting prescription drug
claims or causing them to be submitted for reimbursement from Federal health care programs,
including Medicare Part D, knowing that they were ineligible for the payments demanded.
362. Claims submitted by the CVS Caremark Defendants on behalf of MCS to
Federally-funded health care programs, including Medicare Part D, related to improperly
adjudicated Part D drug claims, constituted violations of the Federal False Claims Act, 31 U.S.C.
§ 3729(a)(1)(A).
363. In light of CVS Caremark’s nation-wide claims adjudication system and attendant
Part D violations, claims adjudicated by the Defendants and submitted by or on behalf of
customers other than MCS to Federally-funded health care programs, including Medicare Part D,
related to improperly adjudicated Part D drug claims, constituted violations of the Federal False
Claims Act, 31 U.S.C. § 3729(a)(1)(A).
364. By virtue of the acts described above, Defendants knowingly made, used, or
caused to be made or used false records and statements, and omitted material facts, to induce the
government to approve and pay such false and fraudulent claims.
365. Each element of the Part D PDE claim record that was created as a result of the
Defendants’ illegal prescription adjudication and claims submission practices represents a false
or fraudulent record or statement. The Defendants knowingly submitted or caused to be
submitted to CMS Part D claims via PDE data reports which included false data elements.
366. The Defendants knowingly made, used or caused to be made or used false records
and statements, including: the false certifications and representations of compliance with Federal
statutes and regulations for Medicare Part D which the CVS Caremark Defendants or MCS

79
submitted to CMS with the false claims for payment, the Medicare Part D PDE data; the cost
reports submitted by or on behalf of the MCS entities or on behalf of CVS Caremark’s Part D
subsidiaries, and the express or implied certifications that the CVS Caremark Defendants made
in order to participate as a Medicare Part D provider, all of which were made or used to get false
or fraudulent claims paid or approved and constituted violations of the Federal False Claims Act,
31 U.S.C. § 3729(a)(1)(B).
367. Each Part D claim related to these false Part D PDE records represents a false or
fraudulent claim for payment.
368. Each data element or record submitted to CMS in order to receive payment under
Medicare Part D, which incorporated or referenced these false Part D PDE records represents a
false or fraudulent claim for payment.
369. Defendants submitted or caused the submission to CMS of false PDE data and/or
false records or statements of certifications and representations of compliance with Federal
statutes and regulations in order for MCS to receive payment under Medicare Part D.
370. MCS was not entitled to receive payments from CMS for Medicare Part D
benefits based on claims containing false PDE data or false certification and/or representations of
compliance with Federal statutes and regulations for Medicare Part D.
371. During the Medicare Part D annual reconciliation, overpayments by CMS to
Part D Plans or Sponsors, including MCS, must be returned.
372. MCS and/or the CVS Caremark Defendants have submitted annual reconciliations
since 2006 without revealing the thousands of improperly adjudicated Medicare Part D claims
which, therefore, contained false PDE data and constituted false claims.
373. At the time of their periodic Medicare Part D reconciliation, the Caremark

80
Defendants and/or MCS failed to report their submission of false PDE data to CMS, and MCS
also failed to return payments received from CMS based upon false Part D claims.
374. As a result of Defendants’ failure to make accurate Medicare Part D annual
reconciliations, Defendants submitted false claims in order to avoid returning overpayments
to CMS.
375. Medicare Part D overpayments made to the Caremark Defendants’ own Part D
subsidiaries and other Part D customers, in addition to MCS, must be returned to CMS.
376. The Patient Protection and Affordable Care Act (“PPACA”), 42 U.S.C. §
1128J(d), which the Defendants violated, requires that Defendant CVS Caremark self-report and
return to Medicare overpayments within 60 days of identification of the overpayment.
377. The Caremark Defendants knowingly caused to be made or used false records or
false statements, i.e., the false certifications caused to be made by the MCS entities when the cost
reports and other records submitted for Part D reconciliations were submitted to conceal, avoid,
or decrease an obligation to pay or transmit money or property to the United States, in violation
of the Federal False Claims Act, 31 U.S.C. § 3729(a)(1)(G).
378. Relator cannot at this time identify every false claim for Federal prescription
health care program payment, including Part D, that were caused by Defendants’ conduct,
particularly the Caremark Defendants' nationwide claims adjudication system, which violates
Medicare Part D requirements. These false claims were presented by the Caremark Defendants
on behalf of thousands of separate entities, across the United States, and over several years. The
records supporting those additional false claims are in the possession and control of the
Defendants.

81
379. Federal health insurance programs, including Medicare Part D, have paid many
thousands of claims, amounting to many hundreds of millions of dollars, for drugs dispensed in
violation of the Part D program requirements for prescription coverage and for corresponding
costs reported by the Part D Sponsors whose Part D claims were adjudicated using the Caremark
Defendants’ nationwide claims adjudication system related to the costs of these inappropriately
dispensed drugs.
380. At all times relevant hereto, Defendants’ acted knowingly as that term is defined
in the Federal False Claims Act, 31 U.S.C. § 3729(b)(1), in that the Defendants acted with actual
knowledge, or in deliberate disregard of the truth or falsity of the information, or in reckless
disregard of the truth or falsity of the information provided in support of the Part D drug claims
and payments and other Part D records submitted in support thereof as detailed above.
381. The Government, unaware of the falsity of the records, statements and claims
made or caused to be made by Defendants, paid and continues to pay the claims that would not
be paid but for Defendants' illegal failure to comply with the requirements of Medicare Part D.
382. By reason of the Defendants’ acts, the United States has been damaged, and
continues to be damaged, in substantial amount to be determined at trial.
WHEREFORE, Relator requests the following relief:
A. Judgment against Defendants for three times the amount of damages the
United States has sustained because of their actions, plus a civil penalty of $11,000 for each
violation of the Federal False Claims Act.
B. 25% of the proceeds of this action if the United States elects to intervene, and
30% if it does not.
C. His attorneys’ fees, costs and expenses.

82
D. Such other relief as the Court deems just and appropriate.
Demand for Jury Trial
Pursuant to Rule 38 of the Federal Rules of Civil Procedure, Qui Tam Plaintiff hereby
demand a trial by jury.
Respectfully submitted,
Dated: ____________________ PIETRAGALLO GORDON ALFANO
BOSICK & RASPANTI, LLP
By: _________________________________
Marc S. Raspanti, Esquire
Michael A. Morse, Esquire
Pamela C. Brecht, Esquire
I.D. Nos.: 41350; 80507; 62249
1818 Market Street, Suite 3402
Philadelphia, PA 19103
(215) 320-6200
www.Pietragallo.com
Attorneys for Qui Tam Plaintiff
Anthony R. Spay 2056443v1

EXHIBIT “A”
EXHIBIT “B”

EXHIBIT “C”


















