Do Community Health Worker Interventions Improve Rates of ... · Science of Cancer Health...
20
Review Do Community Health Worker Interventions Improve Rates of Screening Mammography in the United States? A Systematic Review Kristen J. Wells 1,2 , John S. Luque 2,3 , Branko Miladinovic 1 , Natalia Vargas 2 , Yasmin Asvat 1,2 , Richard G. Roetzheim 1,2 , and Ambuj Kumar 1,2 Abstract Background: Community health workers (CHW) are lay individuals who are trained to serve as liaisons between members of their communities and health care providers and services. Methods: A systematic review was conducted to synthesize evidence from all prospective controlled studies on effectiveness of CHW programs in improving screening mammography rates. Studies reported in English and conducted in the United States were included if they: (i) evaluated a CHW intervention designed to increase screening mammography rates in women 40 years of age or older without a history of breast cancer; (ii) were a randomized controlled trial (RCT), case–controlled study, or quasi-experimental study; and (iii) evaluated a CHW intervention outside of a hospital setting. Results: Participation in a CHW intervention was associated with a statistically significant increase in receipt of screening mammography [risk ratio (RR): 1.06 (favoring intervention); 95% CI: 1.02–1.11, P ¼ 0.003]. The effect remained when pooled data from only RCTs were included in meta-analysis (RR: 1.07; 95% CI: 1.03– 1.12, P ¼ 0.0005) but was not present using pooled data from only quasi-experimental studies (RR: 1.03; 95% CI: 0.89–1.18, P ¼ 0.71). In RCTs, participants recruited from medical settings (RR: 1.41; 95% CI: 1.09–1.82, P ¼ 0.008), programs conducted in urban settings (RR: 1.23; 95% CI: 1.09, 1.39, P ¼ 0.001), and programs where CHWs were matched to intervention participants on race or ethnicity (RR: 1.58, 95% CI: 1.29–1.93, P ¼ 0.0001) showed stronger effects on increasing mammography screening rates. Conclusions: CHW interventions are effective for increasing screening mammography in certain settings and populations. Impact: CHW interventions are especially associated with improvements in rate of screening mammo- graphy in medical settings, urban settings, and in participants who are racially or ethnically concordant with the CHW. Cancer Epidemiol Biomarkers Prev; 20(8); 1580–98. ’2011 AACR. Introduction In 2010, an estimated 207,090 women were diagnosed with breast cancer (BC) in the United States (1). The U.S. Preventive Services Task Force recommends screening mammography every 2 years for women aged 50 to 74 years and recommends screening for women aged 40 to 49 years be based on an individual’s risk factors (2). The American Cancer Society recommends yearly mammo- graphy beginning at age of 40 (3). Early detection of BC is associated with reductions in mortality and improve- ments in survival rates (4, 5). There are significant racial and socioeconomic dispa- rities in BC mortality, survival rates, and cancer stage at diagnosis in the United States (6–10). Women who are less likely to adhere to screening mammography guide- lines include those who belong to ethnic or racial mino- rities; lack comprehensive health insurance or a usual source of medical care; are non-English speakers; are immigrants; live in rural areas; or are socioeconomically disadvantaged (11–19). One model of BC screening promotion that has been implemented and evaluated frequently is the commu- nity health worker (CHW) model. CHWs are lay indi- viduals trained to serve as liaisons between members of their communities and health care providers and services (20). Historically, CHWs serve low-income, medically underserved, racial/ethnic minority, and hard-to-reach populations (21). Authors' Affiliations: 1 University of South Florida; 2 Moffitt Cancer Center, Tampa, Florida; and 3 Georgia Southern University, Statesboro, Georgia Note: This study was presented at the Third AACR Conference on The Science of Cancer Health Disparities in Racial/Ethnic Minorities and the Medically Underserved on October 1, 2010. Corresponding Author: Kristen J. Wells, University of South Florida, 12901 Bruce B. Downs Blvd., MDC 27, Tampa, FL 33612. Phone: 813- 396-2612; Fax: 813-905-8909; E-mail: [email protected] doi: 10.1158/1055-9965.EPI-11-0276 ’2011 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 1580 on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276
Transcript of Do Community Health Worker Interventions Improve Rates of ... · Science of Cancer Health...

Review
Do Community Health Worker Interventions ImproveRates of Screening Mammography in the United States?A Systematic Review
Kristen J. Wells1,2, John S. Luque2,3, Branko Miladinovic1, Natalia Vargas2, Yasmin Asvat1,2,Richard G. Roetzheim1,2, and Ambuj Kumar1,2
AbstractBackground: Community health workers (CHW) are lay individuals who are trained to serve as liaisons
between members of their communities and health care providers and services.
Methods: A systematic review was conducted to synthesize evidence from all prospective controlled
studies on effectiveness of CHW programs in improving screening mammography rates. Studies reported in
English and conducted in the United States were included if they: (i) evaluated a CHW intervention designed
to increase screening mammography rates in women 40 years of age or older without a history of breast
cancer; (ii) were a randomized controlled trial (RCT), case–controlled study, or quasi-experimental study; and
(iii) evaluated a CHW intervention outside of a hospital setting.
Results: Participation in a CHW intervention was associated with a statistically significant increase in
receipt of screening mammography [risk ratio (RR): 1.06 (favoring intervention); 95% CI: 1.02–1.11, P¼ 0.003].
The effect remainedwhen pooled data from only RCTswere included inmeta-analysis (RR: 1.07; 95%CI: 1.03–
1.12, P ¼ 0.0005) but was not present using pooled data from only quasi-experimental studies (RR: 1.03; 95%
CI: 0.89–1.18, P ¼ 0.71). In RCTs, participants recruited from medical settings (RR: 1.41; 95% CI: 1.09–1.82,
P¼ 0.008), programs conducted in urban settings (RR: 1.23; 95%CI: 1.09, 1.39, P¼ 0.001), and programswhere
CHWs were matched to intervention participants on race or ethnicity (RR: 1.58, 95% CI: 1.29–1.93, P¼ 0.0001)
showed stronger effects on increasing mammography screening rates.
Conclusions: CHW interventions are effective for increasing screening mammography in certain settings
and populations.
Impact: CHW interventions are especially associated with improvements in rate of screening mammo-
graphy in medical settings, urban settings, and in participants who are racially or ethnically concordant with
the CHW. Cancer Epidemiol Biomarkers Prev; 20(8); 1580–98. ’2011 AACR.
Introduction
In 2010, an estimated 207,090 women were diagnosedwith breast cancer (BC) in the United States (1). The U.S.Preventive Services Task Force recommends screeningmammography every 2 years for women aged 50 to 74years and recommends screening for women aged 40 to49 years be based on an individual’s risk factors (2). TheAmerican Cancer Society recommends yearly mammo-
graphy beginning at age of 40 (3). Early detection of BC isassociated with reductions in mortality and improve-ments in survival rates (4, 5).
There are significant racial and socioeconomic dispa-rities in BC mortality, survival rates, and cancer stage atdiagnosis in the United States (6–10). Women who areless likely to adhere to screening mammography guide-lines include those who belong to ethnic or racial mino-rities; lack comprehensive health insurance or a usualsource of medical care; are non-English speakers; areimmigrants; live in rural areas; or are socioeconomicallydisadvantaged (11–19).
One model of BC screening promotion that has beenimplemented and evaluated frequently is the commu-nity health worker (CHW) model. CHWs are lay indi-viduals trained to serve as liaisons between membersof their communities and health care providers andservices (20). Historically, CHWs serve low-income,medically underserved, racial/ethnic minority, andhard-to-reach populations (21).
Authors' Affiliations: 1University of South Florida; 2Moffitt Cancer Center,Tampa, Florida; and 3Georgia Southern University, Statesboro, Georgia
Note: This study was presented at the Third AACR Conference on TheScience of Cancer Health Disparities in Racial/Ethnic Minorities and theMedically Underserved on October 1, 2010.
Corresponding Author: Kristen J. Wells, University of South Florida,12901 Bruce B. Downs Blvd., MDC 27, Tampa, FL 33612. Phone: 813-396-2612; Fax: 813-905-8909; E-mail: [email protected]
doi: 10.1158/1055-9965.EPI-11-0276
’2011 American Association for Cancer Research.
CancerEpidemiology,
Biomarkers& Prevention
Cancer Epidemiol Biomarkers Prev; 20(8) August 20111580
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

Previous systematic reviews on the effectiveness ofCHWs on increasing screening mammography have sev-eral limitations. These reviews combined mammographywith other health behaviors (22), combined CHW inter-ventions with other mammography-enhancing interven-tion strategies (23–25), and combined between-groupstudies (comparing CHW interventions to comparisongroup) and within-group studies (comparing mammo-graphy rates over time in a CHW intervention group; ref.26), making it difficult to draw conclusions about effec-tiveness of CHW interventions in improving screeningmammography. To conclusively assess effect of CHWinterventions in increasing screening mammographyrates, we conducted a systematic review. The objectivewas to synthesize and critically appraise available evi-dence on effectiveness of CHW interventions in increas-ing screening mammography rates compared with acontrol group in any population.
Materials and Methods
A study protocol was developed clearly outlininga priori all stages of the systematic review process.
Search strategyWe conducted a comprehensive search of CINAHL,
Medline, PsychInfo, and Web of Science databases foryears 1980 through January 31, 2008. A broad searchstrategy was used to identify relevant articles andincluded 21 terms for CHW plus 5 BC terms to captureall studies evaluating CHW interventions to improvemammography screening. These terms included bothMeSH terms and other identified key words.Each search provided citations that were downloaded
into an Endnote database (27). After duplicate citationswere removed, all titles and abstracts were reviewed by 2study authors independently for their eligibility for inclu-sion. If a decision on inclusion was not made on initialreview, the full text article was obtained. Reference lists ofall eligible articles were also reviewed, and authors of thepresent article were asked to provide any additionalpublications not captured by the search.
Inclusion criteriaStudies published in English and conducted in the
United States were eligible for inclusion if they: (i) eval-uated a CHW intervention designed to increase screeningmammography rates in women 40 years of age or olderwithout a history of BC; (ii) were a randomized controlledtrial (RCT), case–controlled study, or quasi-experimentalstudy; and (iii) were studies in which the CHW interven-tion was delivered outside of a hospital. Studies werelimited to those conducted in the United States because ofvast differences between health systems in the UnitedStates and those in other English-speaking countries.Because CHW interventions are known by many terms,a definition of CHW was created to differentiate CHWstudies from other interventions: "any health care worker
who is involved with carrying out the intervention butwho does not necessarily have formal professional orparaprofessional education." This definition is similar toother definitions in previous reviews evaluating CHWresearch (22, 28).
Data abstractionThe primary outcome variable, receipt of mammogra-
phy, was abstracted from each article as it was reportedprior to the CHW intervention (baseline) and followingintervention (follow-up) for both participants whoreceived CHW as well as comparison groups. Data wereextracted for prespecified sensitivity analyses on samplesource (medical or community setting and urban orrural setting), description of intervention, componentsof intervention, and characteristics of CHWs. The follow-ing data were collected to assess methodologic quality ofresearch reported in each publication: generation of ran-domization sequence, matching of control to interventionparticipants in quasi-experimental studies, and use ofintent-to-treat (ITT) analysis.
Data extraction was conducted by 2 reviewers inde-pendently using a standardized data abstraction form.Any disagreements in data abstraction were resolved byconsensus in collaboration with a third author. Data wereentered into separate SPSS databases (29). Using Graph-Pad Software (30), Kappa coefficients were calculated toassess agreement between the 2 raters on 6 study vari-ables used in sensitivity analysis. Kappa coefficientscalculated for 6 variables indicated agreement rangedfrom "moderate" (0.410) to "almost perfect agreement"(0.885; ref. 31).
Statistical analysisDichotomous data (i.e., number of participants who
did and did not receive screening mammography in bothintervention and comparison groups at follow-up) wereused to calculate a risk ratio (RR), and summary results(RR) from each study were pooled under a random-effects model. A formal statistical test for heterogeneityusing an I2 test was conducted (32). The main studyanalyses were conducted using Review Manager (32).
Because cluster or group randomized trials (CRT) arefrequently used in research on efficacy of CHWs, weexplored the impact of various imputed values of intra-class correlation (ICC) on pooled estimates. ICC is the"similarity" of individuals within clusters, such asclinics or communities. A CONSORT guideline pertain-ing to CRTs explicitly recommends statistical adjust-ments for cluster randomization be used in powercalculations and analysis of primary outcomes, withreporting of ICC (33). Not accounting for clustering inanalysis of CRTs creates a "unit of analysis error" whenCRTs are combined with trials that randomized indivi-duals in a meta-analysis. Correcting for clusteringinflates variance of point estimates (RRs or ORs) inindividual CRTs, giving less weight to these studiesin random-effects meta-analysis.
Community Health Workers and Mammography
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 1581
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

A recent meta-analysis of enhanced care for depres-sion concluded that CRTs produced similar results toindividually randomized trials. However, the analysiswas based on relatively small values of ICC (ICC ¼ 0.02and 0.05; ref. 34). In contrast, a recent study reportedICC estimates in screening mammography CRTs to beas high as 0.2166 (35). A lack of adjustment for cluster-ing tends to inflate treatment effects (36). We alsoexplored the effect of cluster imbalance on pooledresults.
To conduct these analyses, similarities between indi-viduals within a cluster are measured by ICC. Given theaverage cluster size m, the design effect (DE), defined byDE ¼ 1 þ (m � 1) ICC, measures effect on variance of anestimate of treatment effect attributed to clustering. TheICC-adjusted random-effects meta-analysis was con-
ducted in the Bayesian setting due to ease of adjustingICCs for an empirical prior distribution. Using Winbugsversion 1.4.1. (37, 38), adjustment of cluster size imbal-ance was applied to DE minimum variance weightscorrected estimates, based on the Pareto principle inwhich 80% of participants belong to 20% of clusters(39). For each outcome, 5,000 burn-in simulations wereused, with the additional 45,000 simulations to obtain ORestimates. A flat uniform distribution on 0 to 1 range hasbeen recommended for priors of ICCs in case of absenceof prior knowledge (40). However, on the basis of a recentstudy of ICC estimates for cancer screening outcomes(35), unadjusted ICC estimates for mammographyscreening rates ranged from 0.0009 to 0.2166, so weadopted a conservative but informative empiricaluniform prior on (0, 0.5), for imputed values of ICC
Studies excluded Duplicate citations (n = 110)
Not relevant (n = 61)
Articles identified from database 1980–October 2008
(Total n = 265) PubMed/Medline (n = 115) PsycINFO (n = 17) CINAHL (n = 41) Web of Science (n = 92)
Potentially relevant studies identified andscreened for retrieval
(n = 128)
Articles identified in reference search or by
study authors
(Total n = 34)
Met inclusion criteria for systematic review
(n = 24)
Did not meet inclusion criteria (n = 104)
-30 did not describe CHW intervention -18 did not focus on BC screening - 8 had no comparison group - 33 did not report rates of screening mammography at follow-up - 10 were review articles - 5 reported studies outside of United States
Met inclusion criteria for meta-analysis
(n = 18)
Figure 1. Flow diagram ofliterature review process foridentifying studies evaluating useof community health workers toimprove screening mammographyrates.
Wells et al.
Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 Cancer Epidemiology, Biomarkers & Prevention1582
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

Tab
le1.
Sum
maryof
commun
ityhe
alth
worke
rinterven
tions
forBC
screen
ingbytarget
grou
p
Firstau
thor(ref.)
Target
population
CHW
number
and
charac
teristics
Leng
th;type
oftraining
Interven
tiondes
cription
Controld
escription
African
American
Earp(46)
Rural,African
American
wom
en50
þye
ars
170vo
luntee
rlay
health
adviso
rs3–
5se
ssions
,10
–12
hours
instruction;
role
playing
,BC,an
dsc
reen
ing
practices
.
2co
mmun
ityou
trea
chac
tivities
per
mon
thUC
inco
mparison
coun
ties
4pa
idco
mmun
ityou
trea
chsp
ecialists
(indige
nous
commun
itylead
ers)
Layhe
alth
adviso
rsco
nduc
ted2wee
kly
individua
lses
sion
s
Erw
in(47)
Rural,African
American
wom
en,Mississippi
River
Delta,AR
7African
American
BC
survivors
Training
provided
;interviewing
strategies
,brea
sthe
alth
educ
ation
Chu
rch-bas
edgrou
pab
outea
rlydetec
tion
andsc
reen
ing
UC
inco
mparison
coun
ties
Free
mam
mog
ram
vouc
hers
Pas
kett(55)
Predom
inatelyAfrican
-American
wom
en40
þye
ars,
low-inc
ome
hous
ing,
Winston
–Salem
,NC
(interven
tion)
and
Green
sboro,
NC
(con
trol)
ND
ND
Educ
ationa
lses
sion
sbylayhe
alth
educ
ators
Chu
rchprogram
cond
uctedbylay
health
educ
ator
UC
inco
mparison
city
Sun
g(60)
Low-inc
ome,
inne
rcity
African
American
wom
en
Layhe
alth
worke
rsrecruitedfrom
Nationa
lBlack
Wom
en's
Hea
lthProject
10wee
ks;interviewing
andhe
alth
educ
ation
Twoho
mevisits,
1boo
ster
session.
Educ
ationab
outbreas
tan
dce
rvical
canc
er,
Pap
test
andbreas
tex
amvideo
Can
cersc
reen
ing
educ
ationa
lmaterials
Rep
roduc
tivehe
alth
educ
ation
Wes
t(63)
Rural,low-inc
ome
African
American
wom
en50
–80
Indigen
ousAfrican
American
female
health
care
worke
rs.
Training
provided
;se
mi-structured
interview's
conten
t,co
unse
lingstyle
Perso
nalized
reminder
lettersfollo
wed
byintens
ivepho
neco
unse
ling
Elig
ible
forano
-cos
tmam
mog
ram;tailo
red
letter
desc
ribingris
kforBC
Pho
neca
llinclud
edse
mi-structured
interview
eliciting
barrie
rs,facilitators
tomam
mog
raphy
Problem
solvingto
overco
meba
rriers
Provided
phon
enu
mbers
forsc
heduling
mam
mog
raphy
(Con
tinue
don
thefollo
wingpag
e)
Community Health Workers and Mammography
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 1583
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

Tab
le1.
Sum
maryof
commun
ityhe
alth
worke
rinterven
tions
forBC
screen
ingbytarget
grou
p(Con
t'd)
Firstau
thor(ref.)
Target
population
CHW
number
and
charac
teristics
Leng
th;type
oftraining
Interven
tiondes
criptio
nControld
escriptio
n
Zhu
(64)
SingleAfrican
American
wom
en65
þ,livingin
pub
licho
using
African
American
wom
enfrom
same
hous
ingco
mplex
Four
3-ho
urse
ssions
;BC,
screen
ingpractices
,pos
sible
barriers
Hom
e-bas
edBC
screen
inged
ucation
Taug
htpartic
ipan
tsto
overco
mebarrie
rsBroch
ures
Pub
licho
usingco
mplexe
s,no
interven
tion
Hispan
ic/Latina
Fernan
dez
(48)
Hispan
icfarm
worke
rsLa
yhe
alth
worke
rsLa
yhe
alth
worke
rsgive
ntraining
curriculum
includ
ing
teac
hing
guide(12lesson
s)
Individua
land
grou
pinterven
tionse
ssions
with
layhe
alth
worke
r
Com
parison
clinics,
nointerven
tion
Educ
ationse
ssions
includ
edvideo
s,flip
charts,discu
ssions
ofbrea
stan
dce
rvical
screen
ing
Nav
arro
(53)
Low-inc
omeLa
tinas
,San
Diego
,CA
36co
nsejeras
Training
provided
;co
nduc
ting
smallg
roup
sessions
onhe
alth
topics
12-w
eek,
90-m
inute
grou
pse
ssionprogram
12-w
eekCom
mun
ityLiving
Skills
program
Con
sejerastaug
htca
ncer
prev
entio
nwith
cultu
rally-appropria
tematerials.
Nav
arro
(54)
Latin
as,San
Diego
,CA
36co
nsejeras
Training
provided
;follo
wing
cons
ejeraman
ualto
cond
uctwee
klyed
ucationa
lgrou
pse
ssions
12-w
eekgrou
pse
ssions
onbreas
tan
dce
rvical
canc
erea
rlydetec
tion
12-w
eekCom
mun
ityLiving
Skills
program
Nav
arro
(51)
Latin
as,San
Diego
,CA
36co
nsejeras
Training
provided
;co
nduc
ting
smallg
roup
sessions
onbreas
tan
dce
rvical
canc
ersc
reen
ing
12-w
eekgrou
pca
ncer
screen
inginterven
tion
follo
winged
ucationa
lmaterials
12-w
eekCom
mun
ityLiving
Skills
program
Nav
arro
(52)
Low-inc
ome,
low
accu
lturated
Latin
as,San
Diego
,CA
17co
nsejeras
Five
2-ho
urse
ssions
;14
program
sess
ions
,recruitm
entstrategies
,role
playing
tolead
sessions
Twelve
90-m
inutewee
kly
grou
pse
ssions
and
2mon
thly
sessions
focu
sing
onbrea
stan
dce
rvical
canc
er
Friend
san
d/orfamily
(learning
partners)
who
rece
ived
inform
ation
from
clas
spartic
ipan
ts
Sau
aia(57)
Latin
as,CO
"Pee
rco
unse
lors,"
4Catho
licch
urch
es,Den
ver,
CO
(Promotoras
)
Training
provided
Bim
onthly
mee
tings
after
mas
san
dothe
rch
urch
even
ts
209Catho
licch
urch
esse
nt:
(Con
tinue
don
thefollo
wingpag
e)
Wells et al.
Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 Cancer Epidemiology, Biomarkers & Prevention1584
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

Tab
le1.
Sum
maryof
commun
ityhe
alth
worke
rinterven
tions
forBC
screen
ingbytarget
grou
p(Con
t'd)
Firstau
thor(ref.)
Target
population
CHW
number
and
charac
teristics
Leng
th;type
oftraining
Interven
tiondes
criptio
nControld
escription
Res
pected
lead
erdelivered
homilies
addressingbrea
sthe
alth
atleas
ttw
ice
atea
chch
urch
1–3ho
me-bas
edhe
alth
grou
psper
church
Letter
desc
ribingproject
Biling
ualp
rintedmaterials
displayun
itsh
ortmes
sage
sforde
livery
atpulpitan
dch
urch
bulletin
New
sletter
Sua
rez(59)
Low-inc
omeMex
ican
American
wom
en40
þ,Te
xas
Mex
ican
-American
voluntee
rs,
Span
ishsp
eake
rs
ND
Verba
land
newsletter
canc
er-scree
ning
educ
ation
Com
parison
commun
ity,
nointerven
tion
Welsh
(62)
Latin
as,CO
"Pee
rco
unse
lors",
4Catho
licch
urch
es,
Den
ver,CO
Training
provided
;stan
dardized
curriculum
Mon
thly
visits
toea
chch
urch
Promotoras
approac
hed
pee
rsafterSun
day
mas
sesan
dduring
church
fairs
,othe
rch
urch
relatedac
tivities
Promotoras
facilitated
home-bas
edplatic
as(hea
lthgrou
ps)
abou
tbreas
the
alth
209ch
urch
esmailed:
introd
uctory
letter
NCIBC
screen
ing
educ
ationa
lmaterials
displayun
itmes
sage
sto
bede
livered
atpu
lpitor
church
bulletin
s
Asian
American
/Pac
ificIsland
erBird
(43)
Vietnam
ese-American
wom
en18
þ,Califo
rnia
16indigen
ouslay
health
worke
rne
ighb
orho
odlead
ers
68ne
ighb
orho
odas
sistan
ts
Training
provided
;de
liveryof
prev
entio
ned
ucation
Provided
training
man
ual
Small-grou
pho
me-bas
eded
ucationa
lses
sion
sFo
cuse
don
gene
ral
preve
ntion,
routine
chec
kups,
breas
tan
dce
rvical
canc
ersc
reen
ing
Flip
chartan
dfacilitated
discu
ssion
Com
parison
city,no
interven
tion
Gotay
(49)
NativeHaw
aiianwom
en,
18þ,
Oah
u,HI
Native-Haw
aiianlay
health
educ
ators
Training
provided
;brea
st,ce
rvical
canc
ersc
reen
ing.
Small-grou
p,trad
ition
alHaw
aiian"talk-story"
metho
ds
Com
parison
area
,no
interven
tion
(Con
tinue
don
thefollo
wingpag
e)
Community Health Workers and Mammography
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 1585
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

Tab
le1.
Sum
maryof
commun
ityhe
alth
worke
rinterven
tions
forBC
screen
ingbytarget
grou
p(Con
t'd)
Firstau
thor(ref.)
Target
population
CHW
number
and
charac
teristics
Leng
th;type
oftraining
Interven
tiondes
cription
Controld
escription
Free
mam
mog
ram
and
Pap
test
vouc
hers
Aud
iovisu
alaidsus
edOther
Populations
Allen(41)
Wom
enwho
workin
siteswith
Service
Employe
esInternationa
lUnion
represe
ntation
80femaleem
ploye
epee
rhe
alth
adviso
rs16
hours;
canc
ersc
reen
inggu
idelines
,ep
idem
iology
,ea
rlydetec
tion
metho
ds,
commun
ityreso
urce
s
16-m
onth
prog
ram,
6sm
allg
roup
discu
ssions
,role
mod
elingindividua
lou
trea
ch,co
unse
ling,
social
supportfocu
sed
onsc
reen
ing.
Works
hopat
stud
yco
nclusion
2works
ite-w
ideca
mpaign
sAnd
erse
n(42)
Wom
en50
–80
,rural
Was
hing
ton
Wom
enfrom
partic
ipating
commun
ities
Training
provided
Teleph
oneinterven
tion
usingba
rrier-sp
ecific
coun
selingto
promote
mam
mog
raphy
Con
trol
commun
ities
,no
interven
tion
Broch
ures
Calle
(44)
African
American
andWhite
wom
en40
þ
80ACSvo
luntee
rpee
red
ucators,
Jack
sonv
ille,
Orla
ndo,
FL
Half-day
;mam
mog
raphy
andmam
mog
raphy
facilities,
breas
the
alth
guidelines
,interven
tionproce
ss,
interven
tionpractice
sess
ions
,BC
fact
shee
t,reso
urce
guidefor
mam
mog
raphy
centers
Pho
neinterven
tion
emph
asized
importanc
eof
regu
larmam
mog
rams
Set
andco
nfirm
eddate
appointmen
twou
ldbe
sche
duled
andco
mpleted.
Nointerven
tion
Dua
n(45)
African
-American
,La
tina,
andWhite
wom
en50
–80
,ch
urch
esin
Los
Ang
eles
Cou
nty,
CA
Part-tim
epee
rco
unse
lors
ND
Pee
rco
unse
lors
prov
ided
telepho
neba
rrier-focu
sed
mam
mog
raphy
coun
seling
annu
ally
for2ye
ars
Chu
rche
s,no
interven
tion
Wom
enprov
ided
inform
ationab
outris
kstatus
,BC
preva
lenc
erates,
enco
urag
edto
askphy
sician
forreferral
(Con
tinue
don
thefollo
wingpag
e)
Wells et al.
Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 Cancer Epidemiology, Biomarkers & Prevention1586
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

Tab
le1.
Sum
maryof
commun
ityhe
alth
worke
rinterven
tions
forBC
screen
ingbytarget
grou
p(Con
t'd)
Firstau
thor(ref.)
Target
population
CHW
number
and
charac
teristics
Leng
th;type
oftraining
Interven
tiondes
cription
Controld
escription
Margo
lis(50)
African
American
,NativeAmerican
,an
dWhite
wom
en40
þ,no
n–prim
ary-ca
reou
tpatient
clinics
Low-inc
ome,
lay
femalese
nior
aides
(layhe
alth
adviso
rs)
One
mon
th;pee
red
ucation
tech
niqu
es,breas
the
alth,
commun
icationsk
ills,
cultu
rald
iversity,prin
ciples
ofrand
omization,
adhe
renc
eto
rese
arch
protoco
l
Appointmen
tssc
hedu
led
with
femalenu
rse
practition
erforthos
edue
forsc
reen
ing
Wom
enwho
declined
screen
ingen
courag
edto
follo
wup
with
health
care
provider
Wom
enwho
were
up-to-da
tewere
enco
urag
edto
get
regu
larsc
reen
ingan
dofferedmailedreminder
UC
Pas
kett(56)
African
-American
,NativeAmerican
,an
dWhite
wom
enfrom
rural
area
san
dlow-inc
ome
bac
kgroun
d.
2NativeAmerican
andAfrican
American
lay
health
adviso
rs
1wee
kplusfollo
w-up
sess
ions
;brea
sthe
alth,
practiceon
breas
tmod
els,
reso
urce
man
ual,prac
tice
interven
tionse
ssions
3in-perso
nindividua
lvisits,follo
w-uppho
neca
lls,mailings
over
9–12
mon
ths.
Educ
ationa
lmaterials
abou
tca
ncer
risk,
overco
mingba
rriers
tomam
mog
raphy
Discu
ssionof
mam
mog
raphy
,BC,breas
tse
lf-ex
am,
sche
dulingmam
mog
raphy
2pos
tcardmailings
addressingwom
en's
read
ines
sto
chan
ge
Letter
andNCIbroch
ure
abou
tce
rvical
canc
ersc
reen
ing;
afterfollo
wup
,letter
andNCI
broch
ureab
out
mam
mog
raphy
Slater(58)
Low-inc
omewom
en,
pub
licho
using
ACSan
dresiden
tvo
luntee
rsTraining
prov
ided
;vo
luntee
rsprovided
interven
tion
scrip
tsan
dprotoco
ls.
60minute"Frie
ndto
Friend
"program
with
health
professiona
lsp
eake
r,sm
allg
roup
discu
ssions
,as
sistan
cein
obtainingmam
mog
ram,
mam
mog
ram
reminder
Delay
edinterven
tion
Free
mam
mog
rams
Ass
istanc
ewith
appointmen
tsc
hedu
ling
Free
tran
sportatio
n
(Con
tinue
don
thefollo
wingpag
e)
Community Health Workers and Mammography
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 1587
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

(ICC ¼ 0.05, 0.1, 0.2). The pooled results are reported asORs with corresponding 95% credibility intervals.
Results
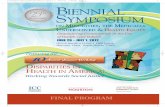
Study identificationThe initial database search yielded 265 articles (Fig. 1),
of which 24 met inclusion criteria (41–64). Of the 24articles included in the systematic review (Table 1), 18(75%; refs. 41–47, 50, 52, 55–63) had extractable data.Three articles (41, 42, 62) provided data enabling calcula-tion of multiple effect sizes. One study provided data onmultiple interventions (42), one study reported results in 2different strata based on age (41), and one study reportedresults separately by race and ethnicity (62). Of the 24included studies (Table 1), 14 were (58%) RCTs (41, 42, 44,45, 50, 51, 53, 54, 56, 58, 60, 61, 63, 64) and 10 were quasi-experimental studies (43, 46–49, 52, 55, 57, 59, 62).
Outcomes of CHW intervention on receipt ofscreening mammography
All trials. Most studies (75%) collected data onscreening mammography use via self-report interviewsor surveys (41–47, 49, 51–55, 58–60, 63, 64). Other studiescollected mammography data through chart reviews (56,61), health insurance claims data (57, 62), or through acombination of self-report and chart reviews (50). Themost common time frame in which screening mammo-graphywas collectedwas 1 year (45, 49–51, 54–56, 64) and2 years (41, 46, 49, 50, 55, 57, 59, 61, 62, 64), with 2 studiesreporting time frames in between 1 and 2 years (43, 58).Several studies evaluated the CHW intervention’s effecton lifetime receipt of screeningmammography (43, 47, 49,52, 53).
Of 18 studies with sufficient data to evaluate receipt ofscreening mammography in the meta-analysis, 10 (56%)were RCTs (41, 42, 44, 45, 50, 56, 58, 60, 61, 63) and 8 werequasi-experimental (43, 46, 47, 52, 55, 57, 59, 62). Thepooled RR of obtaining screening mammography basedon 28,836 mammography events (9,342 intervention;19,494 control) was 1.06 (95% CI: 1.02–1.11, P ¼ 0.003),indicating a statistically significant effect of CHW inter-ventions on improving rate of screening mammography(Fig. 2). However, there was a statistically significantheterogeneity among included studies (I2 ¼ 80%; P <0.00001).
Quasi-experimental studies. The pooled RR ofobtaining screening mammography based on 14,677mammography events (2,235 intervention; 12,442 con-trol) in 8 quasi-experimental studies (9 comparisons; refs.43, 46, 47, 52, 55, 57, 59, 62) was 1.03 (95% CI: 0.89–1.18,P ¼ 0.71; Fig. 2), indicating no effect of CHW interven-tions on rate of screening mammography. There was astatistically significant heterogeneity among includedstudies (I2 ¼ 84%; P < 0.00001).
RCT. The pooled RR of obtaining screening mammo-graphy based on 14,159 mammography events (7,107intervention; 7,052 control) in 10 RCTs (14 comparisons;
Tab
le1.
Sum
maryof
commun
ityhe
alth
worke
rinterven
tions
forBC
screen
ingbytarget
grou
p(Con
t'd)
Firstau
thor(ref.)
Target
population
CHW
number
and
charac
teristics
Leng
th;type
oftraining
Interven
tiondes
cription
Controld
escription
Web
er(61)
African
-American
,La
tina,
andWhite
low-inc
ome,
urban
wom
en52
–77
,6prim
aryca
refacilities
Roc
hester,NY
6wom
enfrom
loca
lco
mmun
ity(4
African
American
,1Hispa
nic,
1White)
ND
1perso
nalized
mam
mog
raphy
reminder
letter
from
physician
1low
literac
ymam
mog
raphy
reminder
letter
from
commun
ityhe
alth
educ
ator
1pe
rson
alized
mam
mog
raphy
reminder
letter
from
phy
sician
plusus
ualc
are
Patient
educ
ationan
dreminders
Iden
tificationan
dremov
alof
barrie
rs
Abbreviations
:ND,no
tdes
cribed
;UC,us
ualc
are.
Wells et al.
Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 Cancer Epidemiology, Biomarkers & Prevention1588
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

refs. 41, 42, 44, 45, 50, 56, 58, 60, 61, 63) was 1.07 (95% CI:1.03–1.12, P ¼ 0.0005; Fig. 2) indicating a statisticallysignificant effect of CHW interventions on improving
rate of screeningmammography. There was a statisticallysignificant heterogeneity among included trials (I2¼ 78%;P < 0.00001).
Study or subgroup
RCTs
Allen, 2001 a
Allen, 2001 b
Andersen, 2000 a
Andersen, 2000 b
Andersen, 2000 c
Andersen, 2000 d
Calle, 1994
Duan, 2000
Margolis, 1998
Paskett, 2006
Slater, 1998
Sung, 1997
Weber, 1997
West, 2004
Subtotal (95% CI)
Total events
Heterogeneity: τ2 = 0.00; χ2 = 60.35, df = 13 (P < 0.00001); I 2 = 78%
Test for overall effect: Z = 3.49 (P = 0.0005)
Quasi-experimantal studies
Bird, 1998
Earp, 2002
Erwin, 1999
Navarro, 2007
Paskett, 1999
Sauaia, 2007
Suarez, 1997
Welsh, 2005 a
Welsh, 2005 b
Subtotal (95% CI)
Total events
Heterogeneity: τ2 = 0.03; χ2 = 50.24, df = 8 (P < 0.00001); I 2 = 84%
Test for overall effect: Z = 0.37 (P = 0.71)
Total (95% CI)
Total events
Heterogeneity: τ2 = 0.00; χ2 = 111.43, df = 22 (P < 0.00001); I 2 = 80%
Test for overall effect: Z = 2.98 (P = 0.003)
Events
709
532
786
813
470
446
142
321
535
184
94
71
41
18
5,162
108
224
98
56
94
359
171
25
48
1,183
6,345
Total
817
573
856
855
776
745
289
416
772
433
151
163
142
119
7,107
197
387
152
80
168
590
450
84
127
2,235
9,342
Events
628
519
799
799
462
462
104
285
447
114
85
54
17
15
4,790
54
274
89
43
54
3,338
205
574
1,756
6,387
11,177
Total
731
560
867
867
800
800
305
397
711
418
163
158
157
118
7,052
193
409
140
63
134
5,708
473
1,323
3,999
12,442
19,494
IV, Random, 95% CI
1.01 (0.97–1.05)
1.00 (0.97–1.03)
1.00 (0.97–1.02)
1.03 (1.01–1.06)
1.05 (0.97–1.14)
1.04 (0.95–1.13)
1.44 (1.19–1.75)
1.07 (0.99–1.17)
1.10 (1.02–1.19)
1.56 (1.29–1.89)
1.19 (0.98–1.45)
1.27 (0.97–1.68)
2.67 (1.59–4.48)
1.19 (0.63–2.25)
1.07 (1.03–1.12)
1.96 (1.51–2.54)
0.86 (0.77–0.96)
1.01 (0.85–1.20)
1.03 (0.82–1.28)
1.39 (1.09–1.78)
1.04 (0.97–1.11)
0.88 (0.75–1.03)
0.69 (0.49–0.96)
0.86 (0.69–1.08)
1.03 (0.89–1.18)
1.06 (1.02–1.11)
Intervention Control RR RR
IV, Random, 95% CI
0.01 0.1 1 10 100
Favors control Favors intervention
Figure 2. Forest plot of comparison: intervention versus no intervention, outcome: receipt of mammography.
Community Health Workers and Mammography
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 1589
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

Sensitivity analysesTo assess robustness of our findings and account for
observed heterogeneity among included studies, we con-ducted additional analyses. Results from quasi-experi-mental studies varied both in magnitude and direction ofeffect. Therefore, quasi-experimental studies wereexcluded from further sensitivity analysis. Sensitivityanalysis focused on the following factors that may beassociated with success of CHW interventions in the 10RCTs: methodologic quality (cluster vs. individual ran-domization, ITT analysis), choice of control intervention,method ofmeasuring study outcome (self-report vs. chartreview), setting of participant recruitment (medical vs.community and rural vs. urban), number of CHW inter-vention components, and characteristics of CHWs.
Methodologic quality. A critical appraisal of metho-dologic quality of all studies was conducted, includinginformation about study design and analyses (Table 2).
Unit of randomization. Six RCTs (60%) randomizedindividual participants to either CHW intervention orcomparison group (44, 50, 56, 60, 61, 63), whereas in theother 4, unit of randomization was a cluster or group towhich participants belonged, such as a work site orchurch (41, 42, 45, 58). None of the CRTs reported powercalculations or whether they were adjusted for clusteringeffects. Three trials (41, 42, 45) incorporated clusteringeffects in the main statistical analysis but did not reportestimated ICC values. The fourth trial (58) reported thevalue of ICC (�0.0015), which was appropriatelyassumed to indicate no design effect for the primaryoutcome measure, and data were analyzed at individualrather than cluster level.
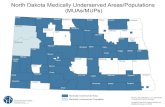
In RCTs that randomized individual participants,CHW intervention was associated with a statisticallysignificant increase in screening mammography (RR:1.39; 95% CI: 1.13–1.70, P ¼ 0.002). In RCTs that rando-mized groups to treatment condition, CHW interventionswere not associated with increases in screening mammo-graphy (RR: 1.02; 95% CI: 1.00–1.04, P ¼ 0.05). There wasstatistically significant heterogeneity among includedtrials that used individuals as unit of randomization(I2 ¼ 80%; P ¼ 0.0002). RCTs that used groups as unitof randomization did not show heterogeneity (I2 ¼ 27%;P ¼ 0.22). Compared with unadjusted estimates, ORestimates adjusted for ICC and imbalance were statisti-cally significant, indicating that CHWs improve rates ofscreening mammography. However, adjusted ORs werecloser to the point of no effect (Fig. 3).
ITT analysis. Pooled data from 3 RCTs which con-ducted ITT analysis (50, 61, 63) indicate that a CHWintervention was not associated with increases inscreening mammography (RR: 1.48; 95% CI: 0.85–2.59,P ¼ 0.17). In 7 studies (11 comparisons) that didnot conduct ITT analysis (41, 42, 44, 45, 56, 58, 60), aCHW intervention was associated with increases inscreening mammography (RR: 1.06; 95% CI: 1.02–1.10,P ¼ 0.004). Both studies that conducted ITT analysis(I2 ¼ 82%; P ¼ 0.004) and studies that did not conduct
ITT analysis (I2 ¼ 77%; P < 0.00001) showed significantheterogeneity.
Choice of control intervention. RCTs comparingCHW interventions to routine care (7 trials involving11 comparisons due to multiple intervention groups ordifferent comparisons by age; refs. 41, 42, 44, 45, 50, 58, 60)were associated with a statistically significant increasein screening mammography (RR: 1.04; 95% CI: 1.01–1.07,P ¼ 0.007). The only RCT employing health education ascontrol (56) compared with CHW also showed a statis-tically significant benefit with use of a CHW intervention(RR: 1.56; 95% CI: 1.29–1.89; P < 0.00001). The pooled RRfrom 2 RCTs that used mammography reminders ascontrol (61, 63) showed a statistically nonsignificant dif-ference comparedwith CHW (RR: 1.82; 95%CI: 0.83–4.01,P ¼ 0.14). However, there was statistically significantheterogeneity among included trials that used routinecare (I2 ¼ 65%; P ¼ 0.002) or mammography reminders(I2 ¼ 73%; P ¼ 0.05) as control.
Method of measuring study outcome. There was sig-nificant variation in measurement of study outcome,receipt of mammography, which limited sensitivity ana-lyses that could be conducted on length of time in whichmammography was measured (Table 2). The interval ofmeasurement reported in the RCTs ranged from receiptof mammography in the past 6 months to receipt ofmammography in the past 3 years. Seven of 10 RCTsmeasured screening mammography outcome using par-ticipant self-report (41, 42, 44, 45, 58, 60, 63). Two studiesmeasured screening mammography with chart review(56, 61) and one combined self-report and a review ofpatients’medical records (50). CHW interventions wereeffective at increasing screening mammography whenmammography was measured by chart review alone(RR: 1.93; 95% CI: 1.15–3.23, P ¼ 0.01) or by chart reviewplus self-report (RR: 1.10; 95% CI: 1.02–1.19, P ¼ 0.009).The pooled RR for the 7 RCTs (11 comparisons) whichmeasured mammography using self-report indicatedthat CHW interventions were not associated withincreases in screening mammography (RR: 1.03; 95%CI: 1.00–1.06, P ¼ 0.02). There was statistically signifi-cant heterogeneity among included trials that usedchart review alone (I2 ¼ 73%; P ¼ 0.06) and self-reportalone (I2 ¼ 59%; P ¼ 0.007) to measure the mammo-graphy outcome.
Study setting. Medical versus community setting. Fivestudies recruited participants from a medical setting (50,56, 60, 61, 63) and 4 (7 comparisons) recruited participantsfrom a community setting (e.g., church, neighborhood;refs. 42, 44, 45, 58). In one study, participants wererecruited from a work setting (41) which was not codedas either a community or medical setting and was there-fore excluded from sensitivity analysis. CHWs wereeffective in increasing rates of screening mammographyin RCTs recruiting participants from a medical setting(RR: 1.41; 95% CI: 1.09–1.82, P ¼ 0.008) or communitysetting (RR: 1.05; 95% CI: 1.01–1.10, P¼ 0.02). There was astatistically significant heterogeneity among included
Wells et al.
Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 Cancer Epidemiology, Biomarkers & Prevention1590
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

Tab
le2.
Ran
dom
ized
controlledtrialc
haracteristic
san
dstud
yqua
lity
First
author
(ref.)
Num
ber
of
partic
ipan
ts,
bas
eline
Mea
nag
eCHW
interven
tion
partic
ipan
ts,
y
Mea
nag
eco
ntrol
participan
ts,
y
Leng
thof
interven
tion,
mo
Tim
efrom
bas
elineto
follo
w-up,
mo
Gen
erationof
rand
omization
seque
nce
Power
analys
isDes
cribed
drop
outs
Participan
tsse
lected
bec
ause
oflack
of
adhe
renc
e
Definitionan
dmea
suremen
tof
mam
mography
outco
me
ITTan
alys
isco
nduc
ted
Allen(41)
2,94
3ND
ND
1630
Worksitesblock
edon
size
ofworks
itean
dtype
ofag
ency
tocrea
te4block
s.With
inea
chblock
rand
om-num
ber
gene
ratoras
sign
edworksitesto
each
cond
ition
.
ND
Yes
No
Pas
t12
–24
mo;
self-report
No
And
erso
n(42)
8,90
7ND
ND
2436
40co
mmun
ities
assign
edto
10block
sof
4co
mmun
ities
for
block
rand
omization.
Eac
hco
mmun
itywith
inon
eof
ten
block
srand
omly
assign
edto
astud
yarm
usingon
eof
24permutation
patternsof
4for
each
block
.
ND
Yes
No
With
in24
mo
offollo
wup
interview;
self-report
No
Calle
(44)
738
ND
ND
68
American
Can
cer
Soc
iety
voluntee
rsea
chge
neratedlist
of10
wom
en.Lists
collected
andwom
enrand
omized
toeither
interven
tionor
control
grou
ps.
ND
Yes
No
Bec
ause
start
ofinterven
tion;
self-report
No
(Con
tinue
don
thefollo
wingpag
e)
Community Health Workers and Mammography
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 1591
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

Tab
le2.
Ran
dom
ized
controlledtrialc
haracteristic
san
dstud
yqua
lity
(Con
t'd)
First
author
(ref.)
Num
ber
of
partic
ipan
ts,
bas
eline
Mea
nag
eCHW
interven
tion
partic
ipan
ts,
y
Mea
nag
eco
ntrol
participan
ts,
y
Leng
thof
interven
tion,
mo
Tim
efrom
bas
elineto
follo
w-up,
mo
Gen
erationof
rand
omization
seque
nce
Power
analys
isDes
cribed
drop
outs
Participan
tsse
lected
bec
ause
oflack
of
adhe
renc
e
Definitionan
dmea
suremen
tof
mam
mography
outco
me
ITTan
alys
isco
nduc
ted
Dua
n(45)
1,11
3ND
ND
2412
30ch
urch
esmatch
edto
12block
san
drand
omized
halfthe
church
esin
each
block
topee
rco
unse
lingan
dothe
rha
lfto
control.
Match
ingva
riables
includ
edrace
/ethnicity,
mem
bersh
ipsize
,reso
urce
s,an
dden
omination.
ND
Yes
No
Pas
t12
mo;
self-report
No
Margo
lis(50)
1,65
854
.555
.91da
yplus
mailed
reminders
12þ
Patientsas
sign
edto
interven
tionor
usua
lca
reac
cordingto
whe
ther
med
ical
reco
rdnu
mber
was
oddor
even
ND
Yes
No
12or
24mo
(dep
ending
onag
e);
self-reportplus
chartreview
Yes
Pas
kett
(56)
897
54.5
55.7
12–14
12–14
Stratified
selection,
block
edrand
omization
byrace
andclinic,
cond
uctedbystud
ystatistic
ian
Yes
Yes
Yes
Pas
t12
mon
ths;
chartreview
No
Slater(58)
427
68.9
67.4
2412
41pub
licho
usinghigh
risebu
ildings
rand
omized
totrea
tmen
tor
control
grou
ps.
Buildings
stratifiedbas
edon
number
ofwom
enper
buildingwho
were
40ye
arsan
dolde
r.
ND
Yes
No
With
in15
moof
interven
tion;
self-report
No
(Con
tinue
don
thefollo
wingpag
e)
Wells et al.
Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 Cancer Epidemiology, Biomarkers & Prevention1592
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

Tab
le2.
Ran
dom
ized
controlledtrialc
haracteristic
san
dstud
yqua
lity
(Con
t'd)
First
author
(ref.)
Num
ber
of
partic
ipan
ts,
bas
eline
Mea
nag
eCHW
interven
tion
partic
ipan
ts,
y
Mea
nag
eco
ntrol
partic
ipan
ts,
y
Leng
thof
interven
tion,
mo
Tim
efrom
bas
elineto
follo
w-up,
mo
Gen
erationof
rand
omization
seque
nce
Power
analys
isDes
cribed
drop
outs
Participan
tsse
lected
bec
ause
oflack
of
adhe
renc
e
Definitionan
dmea
suremen
tof
mam
mography
outco
me
ITTan
alys
isco
nduc
ted
Sun
g(60)
321
ND
ND
1117
Partic
ipan
tsrand
omly
assign
edto
interven
tion
orco
ntrolg
roup
s
ND
Yes
No
Dep
ended
onag
e(w
ithin
4y
if35
–39
;with
in3y
if40
–49
;ye
arly
ifolder
than
49);
self-report
No
Web
er(61)
376
6363
47
Patientsrand
omized
toon
eof
two
grou
ps.
Ran
dom
ization
stratified
bypracticesite
Yes
Yes
Yes
During
interven
tion
period;
chart
review
Yes
Wes
t(63)
320
ND
ND
1da
y6
Env
elop
eco
ntaining
rand
omization
grou
pop
ened
byCHW
after
completin
gtelepho
neinterview
ND
Yes
Yes
Pas
t6mo;
self-report
Yes
Community Health Workers and Mammography
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 1593
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

trials for both subgroups (medical setting: I2 ¼ 81%; P ¼0.0003; community setting: I2 ¼ 70%; P ¼ 0.003).
Urban versus rural setting. Six RCTswere conducted inan urban setting (44, 45, 50, 58, 60, 61), 3 (7 comparisons)in a rural setting (42, 56, 63), and 1 (ref. 41; 2 comparisons)did not report information on setting. Studies conductedin an urban area showed (RR: 1.23; 95% CI: 1.09–1.39, P¼0.001) a statistically significant benefit associated withCHW compared with control. Pooled results for studiesconducted in a rural setting (RR: 1.05; 95% CI: 1.00–1.11,P¼ 0.06) or unknown setting (RR: 1.01; 95% CI: 0.98–1.03,P ¼ 0.69) did not show a benefit associated withCHW compared with control. There was a statisticallysignificant heterogeneity among the subgroup of studiesconducted in an urban (I2 ¼ 74%; P ¼ 0.002) or ruralsetting (I2 ¼ 78%; P ¼ 0.0003) but not the 2 includedcomparisons for the study that did not report setting (I2¼0%; P ¼ 0.75).
Number of intervention components. The CHWswere described using several different terms, such asindigenous community leaders (46), consejeras (51–54),promotoras (57), lay health advisors (46, 50, 56), lay healtheducators (49, 55, 64), community health educators (61),lay health workers (43, 60), peer health advisors, (41) peercounselors (45), community health care workers (63), andvolunteers (42, 44, 58, 59). The most commonly reportedcomponents of CHW interventions included health edu-cation (41–43, 45–49, 51–54, 56, 57, 59–64), referrals tohealth care (42, 43, 45, 47, 48, 50, 58, 59, 63), appointmentscheduling (48, 50, 56, 61), and vouchers, free mammo-grams, or lower cost mammograms (46–49, 63). Lesscommon intervention components included emotionalor social support (41, 61), financial paperwork (48, 61),communication with the health care team (61), mailedreminders (50, 61), and child care (61). Sensitivity analysis
showed a statistically significant increase in receipt ofscreening mammography associated with increase innumber of interventions. RCTs where CHW interven-tions included 1 intervention component (refs. 44, 45, 60;RR: 1.23; 95% CI: 1.00–1.52, P ¼ 0.05) or 2 interventioncomponents (refs. 41, 42, 56, 58; RR: 1.03; 95% CI: 1.00–1.07; P ¼ 0.06) were associated with a statistically non-significant increase in rates of screening mammography.Interventions that included 3 intervention components(refs. 50, 63; RR: 1.10; 95%CI: 1.03–1.19,P¼ 0.008) ormorethan 3 intervention components (ref. 61; RR: 2.67; 95% CI:1.59–4.48, P ¼ 0.0002) were associated with a statisticallysignificant increase in rates of mammography. There wasa statistically significant heterogeneity among includedRCTs in subgroups where CHW used 1 (I2 ¼ 75%; P ¼0.02) or 2 intervention components (I2¼ 74%; P¼ 0.0004).There was a statistically nonsignificant heterogeneityamong included RCTs in the subgroup with 3 CHWintervention components (I2 ¼ 0%; P ¼ 0.81).
Racial or ethnic concordance of CHW and target popu-lation. The studies reviewed targeted a number ofdifferent populations. Ninety-two percent of the studiesincluded ethnic or racial minority participants or focusedon low-incomepopulations. Pooled results fromRCTs thatreportedmatching CHWand target population by race orethnicity (refs. 44, 56, 61, 63; RR: 1.58; 95%CI: 1.29–1.93,P <0.0001) and that did not report matching CHW and targetpopulation by race or ethnicity (refs. 41, 42, 45, 50, 58, 60;RR: 1.03; 95%CI: 1.01–1.05,P¼ 0.02) showed a statisticallysignificant improvement in adherence to screening mam-mography; however, the effect was stronger for the RCTsthat matched CHWs to participants by race and ethnicity.There was not statistically significant heterogeneityamong either subgroup of studies (concordant: I2 ¼45%; P ¼ 0.14; not concordant: I2 ¼ 45%; P ¼ 0.06).
Effect of ICC adjustment on OR estimates
Method
Unadjusted 1.36 (1.18–1.57)
1.34 (1.22–1.49)
1.32 (1.21–1.43)
1.32 (1.21–1.44)
1.31 (1.21–1.42)
1.32 (1.21–1.43)
1.31 (1.21–1.44)
ICC = 0.05, balanced
ICC = 0.1, balanced
ICC = 0.2, balanced
ICC = 0.05, pareto imbalance
ICC = 0.1, pareto imbalance
ICC = 0.2, pareto imbalance
OR (95% Cl)
0 OR = 1 2
Favors control Favors intervention
Figure 3. Effect of ICC adjustmenton OR estimates.
Wells et al.
Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 Cancer Epidemiology, Biomarkers & Prevention1594
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

Discussion
The result from this meta-analysis of 18 studies enrol-ling a total of 26,660 participants indicates that CHWinterventions are associated with a statistically significantincrease in rates of screening mammography but tend tohave stronger effects in specific settings and studydesigns and when participants and CHWs were similarethnically or racially. When RCTs were compared withquasi-experimental studies, the significant increase inscreening mammography rates due to CHW interven-tionswas observed in RCTs but not in quasi-experimentalstudies. In RCTs, all studies showed either a neutral(intervention neither increased nor decreased mammo-graphy rates) or positive intervention effect (interventionincreased mammography rates), indicating that CHWswere more effective than control in improving screeningmammography rates. In quasi-experimental studies,direction of intervention effects was both positive andnegative. These findings point out to inherent biasesassociated with observational study designs. Overall,there was a significant heterogeneity in studies, withvarying populations, varying lengths of intervention,varying lengths of follow-up after intervention, and vary-ing time frames for the mammography outcome. Imput-ing different values of ICC had minimal effect on thedistribution of point estimates of ORs or credibility inter-vals. So, there was little impact of similarity of differentclusters (e.g., clinics) as a result of using a CRT design onoverall effectiveness of CHW interventions on screeningmammography.Overall, our findings are similar to results of previous
studies (21, 65). Results of the present study are alsosimilar to findings of a recent systematic review (26)which found that a subset of CHW interventions wasassociated with significantly greater screening mammo-graphy utilization rates when compared with controls orother interventions (mail, print, minimal CHW). Ourstudy improves on this recent review by providing ameta-analysis of all studies evaluating impact of CHWson screening mammography. In addition, through sensi-tivity analyses of data from RCTs, the present studyprovides information about specific situations whereCHW interventions are most likely to be beneficial (inter-ventions conducted in urban settings, recruitment ofparticipants from medical settings, measuring mammo-graphy outcome using a chart review, CHW interven-tions with 3 or more components, and interventionswhere CHW and patients are racially or ethnically con-cordant). The findings of our study differ from those ofLewin and colleagues (22), who found no beneficial effect(RR: 1.05; 95% CI: 0.99–1.12, P ¼ 0.10) of CHW interven-tions on screening mammography based on a meta-ana-lysis of 4 RCTs conducted internationally. While ouranalysis includes 3 of the 4 studies reported by Lewinand colleagues (22), our analysis also includes twice asmany RCTs as well as quasi-experimental studies. Thus,our results came from a larger pool of data that may not
be as strongly influenced by results of an individualstudy.
A lack of information reported in articles did not allowfor detailed sensitivity analysis of methodologic studyquality. Sensitivity analysis comparing unit of randomi-zation indicates CRTs of CHW interventions did not leadto increased mammography rates, whereas studies thatrandomized individuals were associated with a signifi-cant increase inmammography. In addition, there was nosignificant increase in mammography screening in 3studies that utilized ITT analysis to evaluate a CHWintervention (50, 61, 63), but there was a significantincrease in studies without ITT analysis. This lack ofintervention effect may be related to smaller pooledsample size of the 3 studies (n ¼ 2,019) or may suggestpossible biases favoring intervention effect in studies thatused per-protocol analyses, rather than ITT (66).
CHW interventions were associated with increases inrates of screening mammography in studies with routinecare or health education but not in studies with mammo-graphy reminders. Screening reminders may exert astrong effect on mammography rates, as noted by others(67, 68). Most RCTs reviewed included mammographyreferrals, reminders, or appointment scheduling as 1CHW intervention component (42, 44, 45, 50, 56, 58, 61,63). This finding points to the need to determine compo-nents of CHW interventions most strongly associatedwith increases in screening mammography to improveefficiency of CHW programs.
Both community and medical settings of recruitmentwere associated with increases in screening mammogra-phy related to a CHW intervention, but the effect wasstronger in participants recruited from a medical setting.Connecting patients to a medical setting is important indesigning a CHW program as establishing a usual sourceof care is a known predictor of mammography screening(16, 69). In addition, CHW interventions that took place inan urban settingwere associatedwith screeningmammo-graphy increases, whereas CHW interventions conductedin rural settings were not. These differences may reflectdifficulties in obtaining amammogram in a rural area (19).
RCTs that delivered at least 3 types of interventionswere associated with increases in screening mammogra-phy. These findings concur with previous findings (24)indicating that interventions with multiple interventioncomponents were associated with stronger increases inscreening mammography rates. While the studiesreviewed tended to focus or include historically or medi-cally underserved populations, the RCTs that reportedconcordance between participants and CHWs on race orethnicity indicated a stronger CHW intervention effect onscreening mammography than studies where race andethnic concordance was not described or conducted. Incontrast, a previous systematic review found concor-dance between physicians’ and patients’ race or ethnicitywas not associated with improved health outcomes orpatients’ utilization of health care (70). Sensitivity ana-lyses could not be conducted to evaluate differences in
Community Health Workers and Mammography
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 1595
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

effectiveness of CHW interventions by different popula-tion groups because the majority of the RCTs targetedmultiple underserved populations. Thus, there was noway to categorize them in a meaningful way for compar-isons.
There are several limitations to this systematic reviewand meta-analysis. The study may be biased as itincluded only published peer-reviewed articles.Although unpublished works were eligible for inclusionin the review, none met inclusion criteria. This reviewwas limited to studies published in English and imple-mented in the United States. Thus, meta-analysis resultsmay not generalize to countries providing better or worseaccess to mammography screening services. In addition,sensitivity analyses were based on a small number ofRCTs and should be interpreted with caution. The sys-tematic review is also limited by reporting of data inoriginal articles. Several sensitivity analyses could not beconducted because of significant variability in popula-tions, interventions, and study designs reported. Thisvariability is expected in the context of conductingresearch on interventions designed to meet local needsof various populations and under different breast screen-ing guidelines in place throughout the years, but varia-bility makes it difficult to combine data into meaningfulcategories.
The findings have significant implications for publichealth practice by indicating that CHW interventions areassociated with improvements in rate of 1 time screeningmammography, especially in medical settings, urban set-tings, and in participants who are racially or ethnicallyconcordantwith theCHW.However, asmammography isa behavior that must be repeated multiple times, there isstill much that is unknown about efficacy of CHW inter-ventions in increasing repeated BC screening. A recent
systematic review and meta-analysis of the effectivenessof various types of interventions designed to promoterepeat BC screening found studies that utilized screeningreminders only and studies that used more intensiveinterventions (including CHWs) were both associatedwith increases in repeat mammography (68). Futureresearch should evaluate whether CHW interventionsare associated with repeat mammography screeningand initiation of mammography screening. Futuresystematic reviews are necessary to compare CHW inter-ventions to othermammographypromoting interventionssuch as media interventions (71). In addition, future sys-tematic reviews should evaluate whether CHW interven-tions are associatedwithother cancer screeningbehaviors.Finally, future research should be conducted to defini-tively determinewhich participants and populations ben-efit most from CHW interventions and why.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Grant Support
This work was supported by a training grant from the National CancerInstitute (NCI) at the NIH (R25CA090314; Paul Jacobsen, Principal Inves-tigator) and by a grant from the NCI, through its Center to Reduce CancerHealth Disparities, NIH, Department of Health and Human Services(UO1 CA 117281-01; R.G. Roetzheim, Principal Investigator).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received March 18, 2011; revised April 27, 2011; accepted June 1, 2011;published OnlineFirst June 8, 2011.
References1. American Cancer Society. Cancer facts and figures 2010. Atlanta, GA:
American Cancer Society, Inc; 2010.2. US Preventive Services Task Force. Screening for breast cancer: U.S.
Preventive Services Task Force recommendation statement. AnnIntern Med 2009;151:716–26.
3. American Cancer Society. American Cancer Society guidelines for theearly detection of cancer. 2010 [cited 2010 Jan 23]. Available from:http://www.cancer.org/docroot/PED/content/ped_2_3x_ACS_Cancer_Detection_Guidelines_36.asp.
4. Boyer-Chammard A, Taylor TH, Anton-Culver H. Survival differencesin breast cancer among racial/ethnic groups: a population-basedstudy. Cancer Detect Prevent 1999;23:463–73.
5. Kerlikowske K, Grady D, Rubin SM, Sandrock C, Ernster VL. Efficacyof screening mammography. A meta-analysis. JAMA 1995;273:149–54.
6. Albano JD, Ward E, Jemal A, Anderson R, Cokkinides VE, Murray T,et al. Cancer mortality in the United States by education level andrace. J Natl Can Inst 2007;99:1384–94.
7. Chu KC, Lamar CA, Freeman HP. Racial disparities in breast carci-noma survival rates: separating factors that affect diagnosis fromfactors that affect treatment. Cancer 2003;97:2853–60.
8. Clegg LX, Reichman ME, Miller BA, Hankey BF, Singh GK, Lin YD,et al. Impact of socioeconomic status on cancer incidence and stage
at diagnosis: selected findings from the surveillance, epidemiology,and end results: National Longitudinal Mortality Study. CancerCauses Control 2009;20:417–35.
9. Lantz PM, Mujahid M, Schwartz K, Janz NK, Fagerlin A, Salem B, et al.The influence of race, ethnicity, and individual socioeconomic factorson breast cancer stage at diagnosis. Am J Public Health2006;96:2173–8.
10. Vona-Davis L, Rose DP. The influence of socioeconomic disparitieson breast cancer tumor biology and prognosis: a review. J WomensHealth 2009;18:883–93.
11. Echeverria SE, Carrasquillo O. The roles of citizenship status, accul-turation, and health insurance in breast and cervical cancer screeningamong immigrant women. Med Care 2006;44:788–92.
12. Goel MS, Wee CC, McCarthy EP, Davis RB, Ngo-Metzger Q, PhillipsRS. Racial and ethnic disparities in cancer screening: the importance offoreign birth as a barrier to care. J Gen Intern Med 2003;18:1028–35.
13. Jacobs EA, Karavolos K, Rathouz PJ, Ferris TG, Powell LH. LimitedEnglish proficiency and breast and cervical cancer screening in amultiethnic population. Am J Public Health 2005;95:1410–6.
14. Kandula NR, Wen M, Jacobs EA, Lauderdale DS. Low rates of color-ectal, cervical, and breast cancer screening in Asian Americanscompared with non-Hispanic whites: cultural influences or accessto care? Cancer 2006;107:184–92.
Wells et al.
Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 Cancer Epidemiology, Biomarkers & Prevention1596
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

15. Kim J, Soong-Nang J. Socioeconomic disparities in breast cancerscreening among US women: trends from 2000 to 2005. J Prev MedPublic Health 2008;41:186–94.
16. Peek ME, Han JH. Disparities in screening mammography. Currentstatus,interventionsandimplications.JGenInternMed2004;19:184–94.
17. Sabatino SA, Coates RJ, Uhler RJ, Breen N, Tangka F, Shaw KM.Disparities in mammography use among US women aged 40–64years, by race, ethnicity, income, and health insurance status, 1993and 2005. Med Care 2008;46:692–700.
18. Wells KJ, Roetzheim RG. Health disparities in receipt of screeningmammography in Latinas: a critical review of recent literature. CancerControl 2007;14:369–79.
19. Doescher MP, Jackson JE. Trends in cervical and breast cancerscreening practices among women in rural and urban areas of theUnited States. J Public Health Manag Pract 2009;15:200–9.
20. Witmer A, Seifer SD, Finocchio L, Leslie J, O’Neil EH. Communityhealth workers: integral members of the health care work force. Am JPublic Health 1995;85:1055–8.
21. Swider SM. Outcome effectiveness of community health workers: anintegrative literature review. Public Health Nurs 2002;19:11–20.
22. Lewin S, Dick J, Pond P, Zwarenstein M, Aja G, van Wyk B, et al. Layhealth workers in primary and community health care. CochraneDatabase of Syst Rev 2005;CD004015.
23. Legler J, Meissner HI, Coyne C, Breen N, Chollette V, Rimer BK. Theeffectiveness of interventions to promote mammography amongwomen with historically lower rates of screening. Cancer EpidemiolBiomarkers Prev 2002;11:59–71.
24. Yabroff KR, Mandelblatt JS. Interventions targeted toward patients toincrease mammography use. Cancer Epidemiol Biomarkers Prev1999;8:749–57.
25. Spadea T, Bellini S, Kunst A, Stirbu I, Costa G. The impact ofinterventions to improve attendance in female cancer screeningamong lower socioeconomic groups: a review. Prev Med 2010;50:159–64.
26. Viswanathan M, Kraschnewski J, Nishikawa B, Morgan LC, Thieda P,Honeycutt A, et al. Outcomes of community health worker interven-tions. Rockville, MD: Agency for Healthcare Research and Quality;2009. Report No.: 09-E014.
27. Endnote X. Stamford, CT: Thompson ResearchSoft; 2006.28. Lehmann U, Sanders D. Community health workers: what do we know
about them? 2007 [cited 2010 Nov 23]. Available from: http://www.who.int/hrh/documents/community_health_workers.pdf.
29. SPSS I. SPSS statistics 17.0. 17.0 ed. Chicago, IL: SPSS Inc.; 2010.30. Graphpad Software. Quickcalcs: online calculators for sciences. La
Jolla, CA: GraphPad Software Inc.; 2010.31. Landis JR, Koch GG. The measurement of observer agreement for
categorical data. Biometrics 1977;33:159–74.32. Higgins J, Green S. Cochrane handbook for systematic reviews of
interventions. Version 5.0.0 [updated 2008 Feb]. Oxford, UK: TheCochrane Collaboration; 2008.
33. Campbell MK, Elbourne DR, Altman DG. CONSORT statement: exten-sion to cluster randomised trials. BMJ 2004;328:702–8.
34. Gilbody S, Bower P, Torgerson D, Richards D. Cluster randomizedtrials produced similar results to individually randomized trials in ameta-analysis of enhanced care for depression. J Clin Epidemiol2008;61:160–8.
35. Hade EM, Murray DM, Pennell ML, Rhoda D, Paskett ED, ChampionVL, et al. Intraclass correlation estimates for cancer screening out-comes: estimates and applications in the design of group-randomizedcancer screening studies. J Natl Cancer Inst Monogr 2010;2010:97–103.
36. Donner A, Klar N, Zou G. Methods for the statistical analysis of binarydata in split-cluster designs. Biometrics 2004;60:919–25.
37. MRC Biostatistics Unit. The BUGS project-Bayesian inference usingGibbs sampling. Cambridge, UK: Cambridge University; 2010.
38. Ntzoufras I. Bayesian modeling using WinBUGS. Hoboken, NJ: JohnWiley & Sons; 2009.
39. Guittet L, Ravaud P, Giraudeau B. Planning a cluster randomized trialwith unequal cluster sizes: practical issues involving continuous out-comes. BMC Med Res Methodol 2006;6:17.
40. Turner RM, Omar RZ, Thompson SG. Bayesian methods of analysisfor cluster randomized trials with binary outcome data. Stat Med2001;20:453–72.
41. Allen J, Stoddard A, Mays J, Sorensen G. Promoting breast andcervical cancer screening at the workplace: results from the Womanto Woman Study. Am J Public Health 2001;91:584–90.
42. Andersen MR, Yasui Y, Meischke H, Kuniyuki A, Etzioni R, Urban N.The effectiveness of mammography promotion by volunteers in ruralcommunities. Am J Prev Med 2000;18:199–208.
43. Bird JA, McPhee SJ, Ha NT, Le B, Davis T, Jenkins CN. Openingpathways to cancer screening for Vietnamese-American women: layhealth workers hold a key. Prev Med 1998;27:821–9.
44. Calle EE, Miracle-McMahill HL, Moss RE, Heath CW Jr. Personalcontact from friends to increase mammography usage. Am J PrevMed 1994;10:361–6.
45. Duan N, Fox SA, Derose KP, Carson S. Maintaining mammographyadherence through telephone counseling in a church-based trial. Am JPublic Health 2000;90:1468–71.
46. Earp J, Eng E. Increasing use of mammography among older, ruralAfrican American women: results from a community trial. Am J PublicHealth 2002;92:646–54.
47. Erwin DO, Spatz T, Scotts C, Hollenberg J. Increasing mammographypractice by African American women. Cancer Pract 1999;7:78–85.
48. Fern�andez ME, Gonzales A, Tortolero-Luna G, Partida S, Bartholo-mew LK. Using intervention mapping to develop a breast and cervicalcancer screening program for Hispanic farmworkers: Cultivando LaSalud. Health Promot Pract 2005;6:394–404.
49. Gotay C, Banner R, Matsunaga D, Hedlund N, Enos R, Issell B, et al.Impact of a culturally appropriate intervention on breast and cervicalscreening among native Hawaiian women. PrevMed 2000;31:529–37.
50. Margolis KL, Lurie N, McGovern PG, Tyrrell M, Slater JS. Increasingbreast and cervical cancer screening in low-income women. J GenIntern Med 1998;13:515–21.
51. Navarro AM, McNicholas LJ, Senn KL, Kaplan RM, Campo MC,Ropp�e B. Use of cancer screening tests among Latinas one andtwo years after participation in the Por La Vida Darnos Cuentaprogram. Women Cancer J 2000;2:23–30.
52. Navarro AM, Raman R, McNicholas LJ, Loza O. Diffusion of cancereducation information through a Latino community health advisorprogram. Prev Med 2007;45:135–8.
53. Navarro AM, Senn KL, Kaplan RM, McNicholas L, Campo MC, RoppeB. Por La Vida intervention model for cancer prevention in Latinas. JNatl Cancer Inst Monogr 1995:137–45.
54. Navarro AM, Senn KL, McNicholas LJ, Kaplan RM, Ropp�e B, CampoMC. Por La Vidamodel intervention enhances use of cancer screeningtests among Latinas. Am J Prev Med 1998;15:32–41.
55. Paskett E, TatumCM,D’Agostino Jr. R,Rushing J, VelezR,MichielutteR, et al. Community-based interventions to improvebreast andcervicalcancer screening: results of the Forsyth County Cancer Screening(FoCaS) Project. Cancer Epidemiol Biomarkers Prev 1999;8:453–59.
56. Paskett E, Tatum C, Rushing J, Michielutte R, Bell R, Foley KL, et al.Randomized trial of an intervention to improve mammography utiliza-tion among a triracial rural population of women. J Natl Cancer Inst2006;98:1226–37.
57. Sauaia A, Min SJ, Lack D, Apodaca C, Osuna D, Stowe A, et al.Church-based breast cancer screening education: impact of twoapproaches on Latinas enrolled in public and private health insuranceplans. Prev Chronic Dis 2007;4:A99.
58. Slater J, Ha CN, Malone ME, McGovern P, Madigan SD, Finnegan JR,et al. A randomized community trial to increase mammographyutilization among low-income women living in public housing. PrevMed 1998;27:862–70.
59. Suarez L, Roche R, Pulley L, Weiss N, Goldman D, Simpson D. Why apeer intervention program for Mexican-American women failed tomodify the secular trend in cancer screening. Am J Prev Med1997;13:411–7.
60. Sung JF, Blumenthal DS, Coates RJ, Williams JE, Alema-Mensah E,Liff JM. Effect of a cancer screening intervention conducted by layhealth workers among inner-city women. Am J Prev Med 1997;13:51–7.
Community Health Workers and Mammography
www.aacrjournals.org Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 1597
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

61. Weber BE, Reilly BM. Enhancing mammography use in the inner city.A randomized trial of intensive case management. Arch Intern Med1997 10;157:2345–9.
62. Welsh AL, Sauaia A, Jacobellis J, Min SJ, Byers T. The effect of twochurch-based interventions on breast cancer screening ratesamong Medicaid-insured Latinas. Prev Chronic Dis 2005;2:A07.
63. West DS, Greene P, Pulley L, Polly K, Gore S, Weiss H, et al. Stepped-care, community clinic interventions to promote mammography useamong low-income rural African American women. Health EducBehav 2004;31:29S–44.
64. Zhu K, Hunter S, Bernard LJ, Payne-Wilks K, Roland CL, Elam LC,et al. An intervention study on screening for breast cancer amongsingle African-American women aged 65 and older. Prev Med2002;34:536–45.
65. Gibbons MC, Tyus NC. Systematic review of U.S.-based randomizedcontrolled trials using community health workers. Prog CommunityHealth Partnersh 2007;1:371–81.
66. Montori VM, Guyatt GH. Intention-to-treat principle. CMAJ 2001;165:1339–41.
67. Wagner TH. The effectiveness of mailed patient reminders onmammography screening: a meta-analysis. Am J Prev Med 1998;14:64–70.
68. Vernon SW, McQueen A, Tiro JA, del Junco DJ. Interventions topromote repeat breast cancer screening with mammography: a sys-tematic review and meta-analysis. J Natl Cancer Inst 2010;102:1023–39.
69. Swan J, Breen N, Graubard BI, McNeel TS, Blackman D, Tangka FK,et al. Data and trends in cancer screening in the United States: resultsfrom the 2005 National Health Interview Survey. Cancer 2010;116:4872–81.
70. Meghani SH, Brooks JM, Gipson-Jones T, Waite R, Whitfield-Harris L,Deatrick JA. Patient-provider race-concordance: does it matter inimproving minority patients’ health outcomes? Ethn Health 2009;14:107–30.
71. Baron RC, Rimer BK, Breslow RA, Coates RJ, Kerner J, Melillo S, et al.Client-directed interventions to increase community demand forbreast, cervical, and colorectal cancer screening a systematic review.Am J Prev Med 2008;351 Suppl:S34–55.
Wells et al.
Cancer Epidemiol Biomarkers Prev; 20(8) August 2011 Cancer Epidemiology, Biomarkers & Prevention1598
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276

2011;20:1580-1598. Published OnlineFirst June 8, 2011.Cancer Epidemiol Biomarkers Prev Kristen J. Wells, John S. Luque, Branko Miladinovic, et al. ReviewScreening Mammography in the United States? A Systematic Do Community Health Worker Interventions Improve Rates of
Updated version
10.1158/1055-9965.EPI-11-0276doi:
Access the most recent version of this article at:
Cited articles
http://cebp.aacrjournals.org/content/20/8/1580.full#ref-list-1
This article cites 59 articles, 5 of which you can access for free at:
Citing articles
http://cebp.aacrjournals.org/content/20/8/1580.full#related-urls
This article has been cited by 6 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/20/8/1580To request permission to re-use all or part of this article, use this link
on November 6, 2020. © 2011 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Published OnlineFirst June 8, 2011; DOI: 10.1158/1055-9965.EPI-11-0276